Suicide and Suicidal Behaviour in Women - Issues and Prevention - A Discussion Paper
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Suicide and Suicidal
Behaviour in Women –
Issues and Prevention
A Discussion Paper
July 2015© 2015 Suicide Prevention Australia For more information contact Suicide Prevention Australia GPO Box 219, Sydney NSW 2001 P: 02 9262 1130 E: admin@suicidepreventionaust.org W: www.suicidepreventionaust.org Suicide Prevention Australia acknowledges the funding provided under the Australian Government National Suicide Prevention Program. Suggested citation: Suicide Prevention Australia (2015). Suicide and Suicidal Behaviour in Women – Issues and Prevention. A Discussion Paper. Sydney: Suicide Prevention Australia.
Suicide Prevention Australia Position Statements
Suicide Prevention Australia (SPA) is the national organisation for suicide prevention and works with
organisations, agencies, communities and individuals to prevent suicide across Australia. SPA publishes
position statements on priority areas of suicide prevention, intervention and postvention in Australia.
These foundation documents provide a basis for understanding, dialogue, teaching, service delivery,
strategy and policy development as well as research, and reflect the diversity of voices within the sector.
Position statements are not intended to be specific to or limited to policy makers alone, but are instead
written with a general cross section of the educated lay public in mind (i.e. broader community, media,
and other non-government organisations). Suicide Prevention Australia Position Statements therefore
represent a starting point for policy and strategy development, while supporting ongoing collaborative
programs and services.
These statements are developed in consultation with community and specialist reference groups and are
ratified by the Suicide Prevention Australia Board. This current Discussion Paper has been designed as
a catalyst for dialogue, to inspire and guide consultation and inform the development of a final Position
Statement and policy document on the topic.
SPA Position Statements can be downloaded from the Suicide Prevention Australia website:
www.suicidepreventionaust.org
Acknowledgments Disclaimer
This paper is designed
Suicide Prevention Australia This material has been prepared
as a catalyst for
acknowledges the advice, for information purposes only,
dialogue, to inspire
support and involvement of and represents the views of
and guide consultation
individuals and groups that have Suicide Prevention Australia,
and to inform policy
contributed to the development based on the best available
development.
of this Discussion Paper. evidence accessed at the
Appreciation is particularly time of publication. While all
expressed to those who, reasonable care has been
through their participation, taken in its preparation, Suicide
provided invaluable knowledge, Prevention Australia makes no
expertise and experience, representation or warranty of
including representatives any kind, express or implied, as
from organisations supporting to the completeness, reliability
women in a range of settings. or accuracy of the information.
Suicide Prevention Australia also This Discussion Paper is subject
acknowledges Susan Beaton to change without notice at
Consulting for assistance in the discretion of SPA, and as
preparing and drafting this additional developments occurs.
Discussion Paper. Any links to third party websites
do not necessarily represent
Suicide Prevention Australia
endorsement.
acknowledges the funding
provided under the Australian
Government National Suicide
Prevention Program.
Suicide and Suicidal Behaviour in Women – Issues and Prevention | 3Contents
Snapshot of Key Findings . ..................................................................... 6
Introduction ............................................................................................. 8
Why focus on suicide and suicidal behaviour in women? ................ 8
Background ............................................................................................. 9
Suicide in Australia ............................................................................ 9
Relevant Data and Statistics ................................................................ 10
Suicide . ............................................................................................ 10
Non-fatal suicidal behaviour ........................................................... 13
Trends in hospitalisation ................................................................. 15
Attitudes and beliefs about women’s suicide and suicidal
behaviours................................................................................................ 17
Factors impacting and influencing suicidal behaviour in women .. 18
Risk Factors .......................................................................................... 19
Mental Illness .................................................................................. 19
Pregnancy ........................................................................................ 20
Alcohol and substance abuse . ........................................................ 20
Intimate partner violence ................................................................ 21
Bullying ............................................................................................ 21
Non-suicidal-self-injury. .................................................................. 22
Population Groups at Higher Risk ....................................................... 23
Aboriginal & Torres Strait Islander People ..................................... 24
Bereaved by suicide ......................................................................... 25
Protective Factors ................................................................................ 26
Policy Context ....................................................................................... 26
International .................................................................................... 26
National . .......................................................................................... 27
Recommendations Framework ........................................................... 28
Recommendations for Dialogue and Change ..................................... 31
References ............................................................................................ 33
4 | Suicide and Suicidal Behaviour in Women – Issues and PreventionSuicide and Suicidal Behaviour in Women – Issues and Prevention | 5
Snapshot of the Key Findings
• Women have higher rates • Whereas young men’s Risk Factors
of suicidal behaviour, i.e. suicides have reduced in
ideation, planning and suicide number and rate since the • Women with a history of
attempts compared to men 1997 global peak, young mental illness diagnoses,
and when suicide mortality women’s have not. in particular depression,
and morbidity are combined and anxiety disorders have
it has a large impact on a greater risk of suicidal
• Women are more highly
public health in Australia and behaviours. However not all
represented in non-fatal
internationally. women experiencing mental
suicidal behaviours but are
illness become suicidal,
far less visible in suicide
in fact the greater majority
• In 2013, 637 women died prevention programs and
do not.
by suicide, a rate of 5.5 per research.
100,000 accounting for 21,608 • Depression is a major issue
years of potential life lost. • The number of women aged for a significant number
15 - 24 years who injured of middle-aged and older
• Suicide is a disproportionate themselves so severely women; peri menopause
cause of death among that they require hospital is a complex time of life
younger women. The treatment has increased by for women with a 16 fold
proportion of 15-19 and 20- more than 50 per cent since increase in diagnoses of
24 year old female suicides 2000. depression. This age group
(25%) compared to older of women also have a higher
women (less than 5%). rate and numbers of suicides
• Self-injury is not well
The majority of these 2013 than women of all other ages,
understood across the
adolescent suicides were by including youth.
community, even amongst
hanging. health professionals, which • One in 10 women develop
can lead to stigmatisation and depression during pregnancy
• Hanging is the most social exclusion. Considering and 1 in 7 women develop
commonly used method of the strong association postnatal depression; roughly
suicide for women (as it is for between self-injury and 30% of pregnant women
men) with poisoning by drugs suicidality for women, it is with depression experience
being second most common. imperative that the issue suicidal ideation.
The number of women using of self-injury in women is
• Alcohol was detected in
poisoning by drugs has addressed, especially for
nearly 28% of women and
remained relatively stable younger women.
36% of men who suicided.
across the past 10 years,
while hanging has increased • A review of 664 relevant
by 10% for both men and studies demonstrated
women. a strong, unequivocal
relationship between
intimate partner violence
and suicidality.
• There is a complex
relationship between
bullying and risk of suicidal
behaviours. Bullying and
peer victimisation puts
adolescents at increased
6 | Suicide and Suicidal Behaviour in Women – Issues and Preventionrisk of suicidal ideation and young people with cross- Recommendation 3:
behaviour, especially when gender appearance, traits, or Increase consistent and
other psychopathology is behaviours. systematic demographic
present (e.g. depression). categories to include
• ABS data for 2013 showed
It is not necessarily the sexuality, relationships,
the suicide rate for Aboriginal
bullying per se; there are gender experience / identity /
and Torres Strait Islander
many important mediating expression, and intersex
women has increased to
variables. Suicidal ideation characteristics in suicide and
12.9 per 100,000 compared
and behaviour is usually not suicidal behaviour.
with 5.4 for non-Indigenous
attributed to just one event
women. Recommendation 4:
or factor.
• Suicide rates (per 100,000) Develop well-articulated
• Overall, adolescents are in 2013 for young Aboriginal policies and strategies to
at greater risk for suicidal and Torres Strait Islander address the risk factors for
thoughts and behaviours if women aged 15-24 years was suicide and suicidal behaviour
they have been both bullies 22.7 compared to 5.0 for non- in women.
and victims. For women, Indigenous women.
Recommendation 5:
any involvement in bullying • From 2004-05 to 2012-13, Introduce mental health literacy
is associated with adverse the hospitalisation rate programs and resources which
outcomes. For males it is for intentional self-harm are gender and culturally
frequent involvement that increased for Aboriginal sensitive.
is associated with adverse and Torres Strait Islander
outcomes. Women are less people by 48.1 per cent, while Recommendation 6:
likely to be bullies but when the rate for non-Indigenous Increase gender sensitive
they are, they have a more people remained relatively service provision to meet the
severe impairment than their stable. needs of women at risk.
male counterparts.
• Evidence shows us that of Recommendation 7:
all the relationships to the Mandatory procedures for
Population Groups at deceased, partners and the treatment of women
Increased Risk mothers of people who die seeking medical care following
by suicide are the groups attempted suicide.
• In a national survey 38%
most at increased risk of
of same-gender attracted Recommendation 8:
suicide.
women aged 22-27
Work in collaboration with
years had experienced
depression compared to
Recommendations key Australian Women’s
Health organisations to
19% of heterosexual women SPA endorses and amplifies
host a Roundtable dialogue
respondents. many of the recommendations
on women’s suicide and
developed by Women’s Health
• Non-heterosexual women suicidal behaviour to develop
Victoria (2011).
of various sexualities were sustainable prevention,
almost four times more likely Recommendation 1: intervention and postvention
to have tried to harm or kill Increase accuracy in the strategies and policy.
themselves in the previous recording of suicidal behaviour
six months. by developing standardised data
• The relationship between classification and recording
bullying and suicide risk systems nationally.
was stronger for lesbian Recommendation 2:
and bisexual youth than for
Increase consistent and
heterosexual youth. Nineteen
systematic reporting of gender-
studies showed links
disaggregated data on suicide
between suicidal behaviour
and suicidal behaviour.
in lesbian and bisexual
adolescents and bullying at
school, especially among
Suicide and Suicidal Behaviour in Women – Issues and Prevention | 7Introduction
Why focus on suicide and suicidal behaviour in women?
Suicide research consistently behaviour among women of differences in help-seeking
demonstrates that women trans experience, women and help-acceptance rates for
have higher rates of suicidal with intersex characteristics, distress and mental illness
behaviour, i.e. ideation, planning feminine spectrum people who between women and men (Stack
and suicide attempts compared do not identify as women or 2000; Smalley et al 2005; McKay
to men; however men are more men, and those with culturally et al 2014). In addition, some of
likely to die by suicide (WHO specific genders beyond the these reported differences may
2014). This is referred to as the woman/man binary. vary across cultural contexts
“Gender Paradox in Suicide” rather than functioning as
The substantial attention on
(Canetto & Sakinofsky 1998). universal constants.
suicide prevention for men
Gender plays a significant role in reflects the high importance This discussion paper focuses
suicide and suicidal behaviours. of this pressing global issue. on women’s suicidality because
Gender differences have been However, given the large swing it is an important public
reported in relation to suicide in the size of the health burden health issue. The paper will
methods, risk and protective towards women when suicide discuss the available data and
factors, causal factors, the very mortality and morbidity are statistics relating to suicide
nature of suicidal behaviour combined (Chaudron & Caine and suicidal behaviour in
and how it is manifested. 2004), it would seem both women, the most relevant risk
However, our knowledge of reasonable and sensible to factors for women, the sub-
these differences remains focus also on understanding population groups more at-risk,
incomplete, particularly so for and preventing women’s suicidal the impact of cultural beliefs
reported gender differences in behaviour. Taken together, the and attitudes about gender,
those who attempt suicide, and numbers of women who think and the policy environment.
also within different age groups. about suicide, plan their suicide, The paper will conclude with
The relevant knowledge already attempt suicide and die by recommendations for dialogue
acquired from research to suicide is considerable and has and change for the prevention
date (e.g. Stefanello et al 2010; a large impact on public health of suicide and suicidal
Freitas 2008; Pietro & Tavares in Australia and internationally. behaviour in women.
2005; Qin et al 2000; Roy & Janal
There are many theories and
2006) has rarely been used to
explanations for differences in
inform gender specific suicide
suicide and suicidal behaviour
prevention and treatment “One reason for the lack of
between women and men
responses. investment in female suicidal
and (Schrijvers et al., 2012;
behaviour may be that
Further, despite growth and Hawton 2000; Canetto 2008;
there has been a tendency
advancements in the suicide Jaworski 2007). Some of these
to view suicidal behaviour
prevention field over the past include: gender equality/
in women as manipulative
twenty years, more of the focus inclusion issues, differences
and non-serious (despite
has been on understanding and in socially acceptable methods
evidence of intent, lethality,
preventing suicide mortality for dealing with stress and
and hospitalization), to
rather than non-fatal suicidal conflict for women and men,
describe their attempts as
behaviours. Research has differences in vulnerability to
“unsuccessful,” “failed,”
not contributed much to our psychopathology, biological and
or attention-seeking, and
understanding of suicide and neurobiological differences,
generally to imply that
suicidal behaviour in women availability of and preference
women’s suicidal behaviour
nor consciously informed for different means of suicide,
is inept or incompetent”
prevention of suicide in this cultural role differences,
(Beautrais 2006)
population. There is also very availability and patterns of
limited research on suicidal alcohol/drug consumption, and
8 | Suicide and Suicidal Behaviour in Women – Issues and PreventionBackground
Suicide in Australia
The impact of suicide and are more likely than the general At a global level, in response to
suicidal behaviours has far population to also experience difficulties in capturing the full
reaching effects on Australian suicidality. For this reason NSSI extent and accurate calculation
families and communities. will be discussed in the Risk of non-fatal suicidal behaviour,
Official Australian Bureau of Factors section of this paper. the World Health Organisation
Statistics (ABS) figures put the recently published a resource
Suicide data has been under
lives lost from suicide at about booklet “Preventing suicide: A
scrutiny for the past seven
2,500 people in Australia each resource for non-fatal suicidal
years in Australia following
year (ABS 2014), however this behaviour case registration”
notification of the discrepancies
is believed to be an under- (WHO, 2014).
between Australian Bureau
estimate of the true numbers
of Statistics (ABS) data and The purpose of the booklet is to
(De Leo 2007, 2010). The
the data obtained from the guide national governments and
preliminary ABS data for 2013
Queensland Suicide Register policy makers in defining the
states men’s suicides numbered
(QSR) (De Leo, 2007; Williams topic and establishing national
1,885 (rate of 16.4 per 100,000)
et al., 2010). In 2009 the ABS registries or surveillance
and women’s suicides at 637 (5.5
acknowledged the possibility systems for non-fatal suicidal
per 100,000). Each death has a
of poor suicide data ‘quality’, behaviour. The current lack
devastating impact on biological
which they reported may of national data registration
and chosen families, friends,
have been a consequence of and classification systems
colleagues and communities.
increased numbers of open for suicidal behaviours
‘Suicidal behaviour’ or coroners’ cases at the time of creates a massive gap in our
‘suicidality’ is a broad term releasing their statistics (ABS, knowledge about suicidality
that includes suicide attempts 2009). Consequently, the ABS and in particular women’s
(non-fatal, self-injurious acts instigated a revision process non-fatal suicidal behaviour.
done with an intention to die), of their data in 2009 whereby Nevertheless, and in light of the
suicide planning (taking action retrospective reconciliation constraints of variability in data
in preparation for suicide) of suicide cases from 2007 collection and classification
and suicide ideation (thoughts onwards would take place. systems of non-fatal suicidal
about taking one’s own life). The revision process, which behaviour, some existing
People who experience suicidal is currently completed for data may provide estimated
ideation and make suicide data up until 2011, involves prevalence (albeit conservative)
plans are at increased risk of re-examination of all coroner information on this phenomena
suicide attempts, and people certified deaths at 12 and 24 in Australia.
who experience all forms of months after the original data
suicidality are at greater risk entry and processing, resulting
of death by suicide, though a in “three sets of suicide data
suicide attempt is the most for each reference year:
significant predictor of future Preliminary, revised and final”
suicide. (Kõlves et al, 2013:11). This
revision process and reform
Non-suicidal self-injury (NSSI),
to improve suicide data is
i.e. injury to oneself without
welcomed by researchers and
intent to die, is prevalent
suicide preventionists alike,
amongst women and can be
and is supported particularly
extremely distressing and
by the National Committee for
complex. For most people, this
Standardised Reporting on
behaviour is not about ending
Suicide (see SPA website).
their life, however those who
deliberately injure themselves
Suicide and Suicidal Behaviour in Women – Issues and Prevention | 9Relevant Data & Statistics
1. Suicide Global
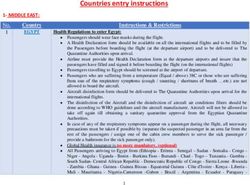
Evidence across many decades As portrayed in Figure 1, Globally men’s suicide rates
reveals that for many so-called globally women’s suicides have predominate over women’s
‘developed’ countries of the been much more stable across suicide rates with a ratio of 3.2:1
world the suicide rate of men the past 65 years and across in 1950, 3.6:1 in 1995 and 3.9:1
exceeds that of women between age groups than men’s, though in 2020; with only one exception
three to fourfold, with the there is considerable variation (China), where suicide rates
exception only of China where by region, and some age groups in women are consistently
(up until just recently) women’s of women have higher numbers, higher than suicide rates in
suicide rates exceeded men’s rates or proportion of total men, particularly in rural areas
rates (Kõlves, Kumpula & De deaths (Callanan & Davis, 2012). (Phillips, Li & Zhang 2002).
Leo, 2013). Recent research has More recently however, in the This cross-cultural variability
shown that the rate of men’s period from 2000 to 2012, the is important to consider, as the
suicide in China has surpassed global age-standardised suicide comparative findings suggest
the women’s rate (Chen et al., rate for women has fallen by that suicide rates are influenced
2012). In countries like India, 32% (with variations by region) by local gender ideology.
Singapore, Hong Kong, Kuwait (WHO 2014).
and Japan, men’s and women’s
suicide rates are relatively the
same (Cheng & Lee, 2000).
Figure 1: Global suicide rates since 1950 and projected trends until 2020
35
Males
30
25
20
15
10 Females
5
0
1950 1995 2020
900,000 1.53 MILLION
DEATHS REPORTED DEATHS ESTIMATED
Source: Bertolote & Fleischmann (2002)
10 | Suicide and Suicidal Behaviour in Women – Issues and PreventionThere were an estimated 804,000 Globally, suicides account for transgender and 2.5% were not
suicide deaths worldwide in 56% of all violent deaths (50% sure of their gender. This means
2012, which equates to a global in men and 71% in women) 3.7% or more of that population
suicide rate of 11.4 per 100, 000 (WHO 2014). could be misclassified. It is
population (8.0 for women and therefore important to be aware
A point of consideration is that
15.0 for men). of the proportion of culturally
many people of trans experience
specific non-binary gender
A method of assessing the are misclassified in a way that
groups and the potential impact
importance of suicide as a public does not reflect how they live
on our understanding of gender
health problem is to assess and identify their own gender.
based analysis; consider, for
its relative contribution to all A recent New Zealand study
example, the ‘sistagirls’ in
intentional deaths, which include (Clark et al 2014) found 1.2%
Aboriginal communities and
deaths from interpersonal of a nationally representative
fa’affafine in Samoa.
violence, armed conflict and adolescent population sample
suicide (i.e. violent deaths). reported identifying as
National
Similar to global trends, data, 637 women died by
Australian women’s suicide suicide, a rate of 5.5 per
rates have been relatively stable 100,000, though rates fluctuate
and constant across the past across age groups (see Figure
thirty years, at approximately 5 3, next page); accounting for
deaths per 100,000 (see Figure 21,608 years of potential life lost
2 below). According to the 2013 (ABS 2015).
preliminary ABS
Figure 2: ABS suicide rates 1989 – 2013 by sex (incl. revision process)
50
45
40 Male Preliminary
Suicide Rate (per 100,000)
Male Revised
35
Female Preliminary
30
Female Revised
25
20
15
10
5
0
89
90
91
92
93
94
95
96
97
98
99
00
01
02
03
04
05
06
07
08
09
10
11
12
13
19
19
19
19
19
19
19
19
19
19
19
20
20
20
20
20
20
20
20
20
20
20
20
20
20
YEAR
Source: Hunter Institute for Mental Health
Suicide and Suicidal Behaviour in Women – Issues and Prevention | 11Figure 3: Age-standardised suicide rates per 100,000 by sex and age group,
Australia, 2013
40.0
35.0
Males..... 16.4
Females... 5.5
30.0
25.0
20.0
15.0
10.0
5.0
0.0
s
s
s
s
s
s
s
s
s
s
s
s
s
s
s
er
yr
yr
yr
yr
yr
yr
yr
yr
yr
yr
yr
yr
yr
yr
yr
ov
14
9
4
9
4
9
4
9
4
9
4
9
4
9
4
-1
-2
-2
-3
-3
-4
-4
-5
-5
-6
-6
-7
-7
-8
d
0-
an
15
20
25
30
35
40
45
50
55
60
65
70
75
80
85
Source: ABS (2015)
In 2013, suicide accounted using poisoning by drugs has the difficulties attending to
for 0.9% of all women’s remained relatively stable adjustments within the broader
deaths. Of note, suicide is a across the past 10 years, community environment and
disproportionate cause of hanging has increased by 10% more research is needed to
death among younger women, for both men and women (in better understand the recent
compared to older women, 2003 hanging represented rise in the choice of this method
as shown in Figure 4, next 37% of all women’s suicides; (Biddle et al 2012).
page. Of particular concern in 2012 it was 47%). Hanging is
is the proportion of 15-19 and an increasing and predominant
20-24 year old girls’ suicides method of suicide. Only a
compared to older women. small proportion, 10% of
The majority of these 2013 hangings occur in controlled
adolescent suicides were by environments (such as prisons,
hanging. hospitals), the remainder occur
in the community (Gunnell et al
Whereas young men’s suicides
2005).
have reduced in number and
rate since the 1997 global peak, Hanging is potentially lethal
young women’s have not. and the means (rope, belt,
cord etc.) highly accessible,
Hanging is the most commonly
yet prevention within the
used method of suicide for
community environment is
women (as it is for men)
a challenge. The prevention
with poisoning by drugs
of hanging deaths is in fact a
being second most common.
global challenge because of
Whereas the number of women
12 | Suicide and Suicidal Behaviour in Women – Issues and PreventionFigure 4: S
uicide as proportion of total deaths by sex & age group, 2013
35.0
30.0
Males.... 2.5%
Females 0.9%
25.0
20.0
15.0
10.0
5.0
0.0
s
s
s
s
s
s
s
s
s
s
s
s
s
s
s
er
s
yr
yr
yr
yr
yr
yr
yr
yr
yr
yr
yr
yr
yr
yr
yr
ge
ov
la
14
9
4
9
4
9
4
9
4
9
4
9
4
9
4
-1
-2
-2
-3
-3
-4
-4
-5
-5
-6
-6
-7
-7
-8
&
Al
0-
15
20
25
30
35
40
45
50
55
60
65
70
75
80
85
Source: ABS (2015)
2. Non-fatal suicidal behaviour
Evidence suggests that people making it impossible to identify prevalence of a suicide attempt
who engage in non-fatal an accurate number of suicide in a large population study
suicidal behaviour and attempt attempts in Australia. conducted in Queensland
suicide are likely to do so again revealed women’s numbers
Accessing accurate, valid
unless they receive appropriate were higher than those of men,
and reliable data on suicide
help (Australian Government 5.0 compared to 3.3 (De Leo et
attempts is problematic;
Department of Health & Ageing al 2005).
however there are some
2007). The Australian Bureau
sources that provide an Researchers, policy makers
of Statistics (ABS) categorises
approximate picture. A and clinicians are confronted
suicide attempts under
comparison between two by many challenges when
‘intentional self-harm’. The
data collection points of trying to define and classify
ABS defines ‘intentional self-
Australia’s National Survey of suicidal behaviours, including
harm’ as ‘a range of behaviours
Mental Health and Wellbeing adopting a standard vocabulary,
including cutting, poisoning
(NSMHW), 1997 and 2007, dealing with the issue of data
and attempted suicide (ABS
showed an increase in the 12 reliability, data linkage, and
2008). The numbers of people
month prevalence rates of service usage versus self-
who injure themselves without
women’s suicide attempts from reporting of non-fatal suicidal
the intention of suicide and
0.4% to 0.5% respectively for behaviour. Most data on the
those who engage in non-fatal
the age group 16 – 85 years prevalence of suicide attempts
suicidal behaviour cannot be
(ABS 2008). From another is derived from hospital
separated within the existing
source, the estimate of lifetime data, which unfortunately
data collection systems,
Suicide and Suicidal Behaviour in Women – Issues and Prevention | 13One international example 2007 National Survey of
“The objective of this booklet of achieving improvements Mental Health and Wellbeing
is to advocate for taking to the classification of non- (NSMHW), approximately 2.1
non-fatal suicidal behaviour fatal suicidal behaviour can million adults in Australia have
more seriously and to put it be observed in the United had serious thoughts about
on the agenda, as it has been Kingdom where the Republic killing themselves. According
overshadowed by death from of Ireland has developed a to the same survey 600,000
suicide or forgotten about National Register of Deliberate adults have made a plan to
altogether.” Self-Harm, operating since suicide and 500,000 adults
2006 (Perry et al 2012). The have made a suicide attempt
“Preventing Suicide –
focus here has been on the during their lifetime (Slade
A resource for non-fatal
design of standardised data et al 2008). Table 1 below
suicidal behaviour case
collection procedures for presents 12-month prevalence
registration”, WHO 2014
documenting, observing, of men and women’s suicidality
measuring and analysing obtained from the NSMHW
non-fatal behaviour across survey, plus ABS suicide data.
suffers from a myriad of case time to subsequently inform
The proportion of women
classification issues. Further, prevention and intervention
who experienced some form
there are no standardised strategies. Another example
of suicidality (being ideation,
terms used across jurisdictions comes from the Multicentre
plans and/or attempts) is
(states/territories) or health Study of Self-Harm in England
nearly 1% higher than their
facilities and institutions, with which is a large collaboration
men counterparts. This is a
‘intentional self-harm’ (ISH) between Derbyshire, Oxford
public health problem in an
being the terminology most and Manchester health trusts
order of magnitude far greater
commonly used in the hospital (Kapur et al 2013). It involves
than just suicide mortality
setting. However there are use of shared standard
numbers. Presentation to a
variable behaviours which can protocols for investigating
hospital after a suicidal attempt
be registered as ISH, including the epidemiology, causes,
is low, with less than 30% of
suicide attempts as well as clinical management, outcome
a large Queensland survey
non-suicidal self-injury, without and prevention of self-harm
acknowledging attendance
an intention to die (WHO 2014). behaviour. According to the
after their attempt (De Leo et al
Table 1: Prevalence, 12-month suicidality by gender, Australia, 2007 & 2013 suicides
Women % Women No. Men % Men No. All Persons All Persons
% No
Suicidal ideation 2.7 221,300 1.9 146,700 2.3 370,000
Suicide plans 0.7 57,500 0.4 33,500 0.6 91,000
Suicide attempts 0.5 42,700 0.3 22,600 0.4 65,000
Any suicidality 2.8 N/A 1.9 N/A 2.4 380,000
Suicides (ABS 2013 data) 25 637 75 1,885 100 2,522
I Note: Any suicidality is lower than the sum as people may have reported more than one
type of suicidality.
II Note: Using most recently available suicide data 2013
N/A Note: Not easily derived from the ABS data spreadsheet
Source: ABS (2008 & 2015)
14 | Suicide and Suicidal Behaviour in Women – Issues and Prevention“Population-based data on
Trends in rates of hospitalisation due to
hospital-treated intentional category of ‘intentional self-harm’
self-harm represents an
important index of the
burden of mental illness As previously mentioned, and 2% respectively (AIHW
and suicide risk in the hospital data gives us only an 2014).The number of women
community.” approximate picture of non-fatal aged 15 - 24 years who injured
suicidal behaviour since the themselves so severely that they
(Perry et al 2012) term “intentional self-harm” require hospital treatment has
(ISH) clusters together suicide increased by more than 50 per
attempts and non-suicidal cent since 2000 (see Figure 5
2005). Women were 2.3 times self-injury”. Be that as it may, below). In 2010-11, more than
more likely than men to attend hospital attendance trends are 26,000 people were hospitalised
hospital after a suicidal act with useful to further illuminate the for “intentional self-harm”;
each of these presentations picture. nearly one in five were women
creating an opportunity for aged 15-24 years (AIHW 2013).
The rates for women
compassionate care, psycho- hospitalised as a result of ISH While it cannot be determined
education, treatment, and were at least 40% higher than how many of these cases were
linkage to ongoing support men’s rates over the period non-fatal suicidal behaviours
in the community. Increased from 1999–00 to 2011–12, with or self-injury without intention
accuracy in the recording of the number of women’s cases to die, the dramatic increase is
reported non-fatal suicidal exceeding men’s cases most concerning.
behaviour is vital to suicide noticeably in the adolescent
prevention efforts and can Figure 6 (next page) indicates
years (AIHW 2014).
be used to determine the the recent age distribution by
prevalence and correlates of Poisons (including prescription sex of those hospitalised for
non-fatal suicidal behaviour, and non-prescription, but “intentional self-harm”. Clearly
the efficacy of interventions excluding gas) accounted the prevalence of this behaviour
and informs government for almost 82% of all in younger women requires
funding allocations for suicide hospitalisations due to ISH urgent attention.
prevention and mental health over the period from 1999–00
The suicide methods used
support programs to meet the to 2011–12. Contact with
by women and men have
needs of women and at risk sharp objects and hanging
contributed (amongst other
people. accounted for a further 12%
Figure 5: T
rends in hospitalised injury, Australia 1999–00 to 2010–11
Cases of self-harm among women aged 15 to 24
5278
5000
4500
4000
3407
1999/2000 2001/02 2003/04 2005/06 2007/08 2010/11
Source: AIHW (2013)
Suicide and Suicidal Behaviour in Women – Issues and Prevention | 15factors) to the difference in and masculinity and gender
suicide rates (Callanan & roles in Australian society
Davis, 2012). Historically, it have affected method choices,
has been debated that women however more research is
have chosen methods of required to fully understand,
variable effectiveness e.g. and address the change to more
poisoning (overdose) whereas lethal methods and how this
men have chosen more violent varies within minority groups
methods e.g. firearms, hanging. (Women’s Health Victoria 2011).
Nevertheless, research shows
Women may have the same
that women and men with equal
intent to die, however the
intent to die use methods for
resulting suicide attempt status
suicide which differ in lethality,
is less recognised as a social
with men typically choosing
issue, and is not well recorded
more lethal methods (Denning
in data collection and reporting.
et al 2000).
As a result, while women are
Trends have been changing, more highly represented in
however, and women are non-fatal suicidal behaviours
adopting more lethal methods they are far less visible in
(Byard et al 2004; Austin et al suicide prevention dialogue
2011). It has been posited that and research.
the changing ideas of femininity
Figure 6: A
ge-specific rates of hospitalisation as a result of intentional self-harm,
by sex, Australia, 2010–11
500
Hospitalisations per 100,000 population
Males
400 Females
300
200
100
0
s
s
s
s
s
s
s
s
s
s
s
s
s
s
s
s
s
er
yr
yr
yr
yr
yr
yr
yr
yr
yr
yr
yr
yr
yr
yr
yr
yr
yr
ov
4
9
4
9
4
9
4
9
4
9
4
9
4
9
4
9
4
0-
5-
-1
-1
-2
-2
-3
-3
-4
-4
-5
-5
-6
-6
-7
-7
-8
&
10
15
20
25
30
35
40
45
50
55
60
65
70
75
80
85
AGE GROUP
Note: Rates for ages 0–4 and 5–9 not reported.
16 | Suicide and Suicidal Behaviour in Women – Issues and PreventionAttitudes and beliefs about women’s
suicide and suicidal behaviours
guilty or responsible (Canetto is in healthcare settings. Some
“The gender & Sakinofsky, 1998; Jaworski, healthcare staff continue to lack
differential in suicide 2003). This portrayal is implicit, understanding and compassion,
has been one of the pervasive and subtle and can and in their time-poor, stressful
most perplexing and insidiously influence the way work environments, often
controversial issues in which women’s suicidal deem suicidal behaviour as
in the study of suicidal behaviours are misunderstood “attention-seeking”. This
behaviour, largely and unsupported by families, greatly compromises the quality
because of gender the community and service of care provided to women
biases, which have providers. and potentially adds to their
influenced both theory At a global level, in response to
risk (Scourfield et al 2011).
and research”. difficulties in capturing the full
Despite the development and
implementation of guidelines
extent and accurate calculation
and standards relating to the
of non-fatal suicidal behaviour,
treatment of suicidal patients,
the World Health Organisation
There are ubiquitous cultural staff may not always adhere
recently published a resource
stereotypes that impede the to these guidelines (Dyson
booklet “Preventing suicide: A
level and kind of support 2007). Women are generally
resource for non-fatal suicidal
provided to women exhibiting more likely than men to come
behaviour case registration”
suicidal behaviours. While forward to share their personal
(WHO, 2014).
stigmatisation of suicide exists experience of having been
for both genders, women’s The purpose of the booklet is to hospitalised for self-harm and
suicidal behaviours are often guide national governments and report feeling dissatisfied with
viewed differently (Canetto policy makers in defining the emergency and psychiatric
1997). topic and establishing national services due to perceived
registries or surveillance negative attitudes directed
Suicidal behaviour, in particular,
systems for non-fatal suicidal towards them (Walker 2009;
suicide attempts and NSSI,
behaviour. The current lack NMHC Report Card 2013).
is more common in women,
of national data registration
and these behaviours are A systems approach to
and classification systems
regarded as more ‘feminine’ compassionate and humanistic
for suicidal behaviours
than acts of suicide by men. care for suicidal women
creates a massive gap in our
Women who attempt suicide is imperative if we are to
knowledge about suicidality
are often portrayed in classic encourage women to access
and in particular women’s
literature and popular culture support (Youngson 2012;
non-fatal suicidal behaviour.
as engaging in a form of US Suicide Care in Systems
Nevertheless, and in light of the
‘manipulative femininity’ (Dyson Framework, 2012; Ballat &
constraints of variability in data
et al 2003; Canetto 2008; Campling, 2010). Training
collection and classification
Scourfield 2011). The view of of healthcare staff needs to
systems of non-fatal suicidal
men’s suicide however is seen address underlying, entrenched
behaviour, some existing
as masculine, decisive, lethal, beliefs and attitudes not just
data may provide estimated
violent, aggressive and serious. suicide risk assessment.
prevalence (albeit conservative)
Women’s suicide is often
information on this phenomena
conceptualised as non-lethal,
in Australia.
non-violent and passive and
women who attempt suicide are One domain where judgemental
often described as ‘attention- beliefs and attitudes about
seeking’, aiming to manipulate women’s suicidal behaviours are
their loved ones into feeling highly visible and problematic
Suicide and Suicidal Behaviour in Women – Issues and Prevention | 17Factors impacting and societal stereotypes, cultural Life experience and
influencing suicidal norms, and limited role relationships:
behaviour in women definitions can also contribute to • current relationship/marital
the wellbeing of women. turmoil
Suicide is complex and there is
usually an interplay of multiple A wide range of risk factors • intimate partner violence and
factors that contribute to have been recognised as domestic violence
someone taking their own life. influencing suicide and some
are illustrated below. For • childhood sexual abuse
Although the experience of
suicidal behaviour is unique and simplicity, they have been • exposure to poor parenting
individual in nature, a number grouped into areas reflective of or violent parental conflict;
of bio psychosocial and cultural the Ecological Model (Dahlberg fractured family structures
factors have been found to & Krug 2002; WHO 2014)
across systemic, societal, • family of origin history of
influence the risk of suicide
community, relationship (social violence or suicide
in women (though the level of
research on differences in risk connectedness to immediate • financial, work stress, under
factors between genders is family and friends) and or unemployed
scant). individual risk factors.
Community level:
Risk factors can be defined as Individual factors: • social or geographical
either distal or background • mental health diagnoses isolation
factors, such as genetic factors, and related symptoms
or proximal, more immediate (depression, eating disorders, • bullying and hate crimes
factors, such as a recent life schizophrenia, borderline • high unemployment
events. These factors interact personality disorder, post-
• poverty and low income
with a confluence of social traumatic stress responses,
determinants, for example NSSI) • cultural scripts about
intimate partner violence, women’s suicidal behaviour
• harmful use of alcohol and
culture, geographic location,
substance use
and discrimination, to influence
patterns of women’s suicidality. • post-natal depression,
Not having autonomy, choices unwanted pregnancy
and agency in one’s life
• chronic illness/pain
adversely affects women’s
experience. Constraints • previous non-fatal suicidal
including financial, economic behaviour
equity, health, marriage and
• genetic and biological factors
relationship recognition, fertility
and assisted reproduction • access to lethal means
options, geographic mobility, • feelings of hopelessness
employment equality issues,
18 | Suicide and Suicidal Behaviour in Women – Issues and PreventionRisk Factors
from interpersonal violence,
Discussed below are risk factors that have some reproductive rights, freedom
from discrimination and racism,
research evidence documenting their specific gender equality, and access to
influence on women’s suicidal behaviour and suicide. education, healthcare. A positive
social environment can support
wellbeing through protective
Mental illness become suicidal, in fact the
greater majority do not. factors that mitigate risk.
Research reveals that women
There is also an important Depression remains a major
with a history of mental illness
body of literature on the issue for a significant number of
diagnoses, in particular
medicalisation of women’s middle-aged and older women;
depression, and anxiety
misery and the problem of peri menopause is a complex
disorders have a greater risk of
women receiving a diagnosis of time of life for women with a 16
suicidal behaviours (Chaudron &
depression (Ussher 2010). fold increase in diagnoses of
Caine 2004; Cougle et al 2009).
depression (Cohen et al 2006).
Depression appears to have Mental health symptoms This age group of women also
a higher prevalence among experienced more by women have a higher rate and numbers
women with an earlier age of that carry increased suicide risk of suicides than women of all
first onset (Ferguson et al, 2000; include depression, particularly other ages, including youth
Kessler 2003), and depression during the perinatal period, (Lawrence et al 2000). In
diagnoses are ubiquitous among and eating disorders (both Australia approximately 100,000
women who die by suicide bulimia and anorexia nervosa). women over 50 years of age
(Chaudron & Caine 2006). Borderline personality disorder will be diagnosed with a major
Co-occurring conditions, e.g. (BPD) is a severe and persistent affective disorder during any
affective disorders, anxiety mental illness, prevalent one year (ABS 2007-2008).
disorders and substance use amongst women. Among One contributing factor for
disorders, are particularly patients with BPD, 69% - 80% worsening depression in
common among those who engage in suicidal behaviour, vulnerable women appears to
take their own life. One study with a suicide mortality rate of be menopause (Freeman et al
revealed that 74% of women, up to 9% (Linehan et al 2006). 2006). There is debate amongst
who had attempted suicide at
Women’s greater vulnerability health professionals whether
some stage in their life, had also
to non-fatal suicidal behaviour this is new depression because
received a prior diagnosis of
can also be associated with of the menopause or is pre-
depression or PTSD (Cougle et
gender-related vulnerability existing depression exacerbated
al 2009). While having a mental
to psychopathology and at this time. Nevertheless,
health diagnosis is strongly
to psychosocial stresses women in their middle years
associated with suicidality,
(Beautrais 2006). Biological have increased rates and
an acute situational crisis of
factors may include: personality numbers of suicides and the
deep despair, hopelessness
traits, genetic susceptibility, management of increased
and unbearable suffering can
and family history, while social depression at this time in life
also precipitate suicidality. It
determinants include: lack of will improve their quality of life
is also true that not all women
access to resources, resilience, and wellbeing.
experiencing mental illness
connectedness, freedom
Suicide and Suicidal Behaviour in Women – Issues and Prevention | 19Pregnancy 2007). Contributing factors also suggesting a higher rate
include that 1 in 10 women of suicide among these women
The relationship between develop depression during (Reardon et al, 2002).
pregnancy and suicidality is pregnancy and 1 in 7 women
complex, with motherhood The menstrual cycle implications
develop postnatal depression;
generally providing a protective for women are that non-fatal
roughly 30% of pregnant
effect. However there has suicidal behaviour occurs most
women with depression
been significant difficulty often when oestrogen and
experience suicidal ideation
collecting accurate data about serotonin levels are lowest
(Gold et al, 2012; Melville et
the prevalence of suicide and (Villeneuve et al, 2006).
al 2010). Factors associated
suicidal behaviour among with suicidal ideation during A recent article on this topic
mothers in Australia. the antenatal period include helps us to understand the
depression, perceived stress, complex association between
smoking, and common mental pregnancy and suicide. “Thus
“It has been argued that if disorders (Gavin et al., 2011; pregnancy (and other cardinal
all women were given the Huang et al., 2012). Austin et al., life events) can increase,
right to self-determination (2007) identified a risk profile decrease, or be unrelated to
and were able to control that is unique to childbearing the risk of suicide, dependent
their own fertility, there women – women with previous on the psychological valence
would be fewer unwanted psychiatric hospitalisation of pregnancy, on the types of
pregnancies and therefore without their baby and severe support networks provided
fewer suicides”. mental illness with early onset for pregnant women, and on
(Boama & Arulkumaran, following childbirth (postpartum the coincident presence of
2009; WHO, 2008) psychosis). In women with post- underlying risk factors for
partum psychosis the suicide suicide (eg, previous suicide
risk increased 7-fold in the year attempt, mental illness, or
after childbirth and 17- fold over substance abuse) (Phillips,
Despite pregnancy and the long term (Appleby et al 2014)”.
parenthood being a protective 1998).
factor for women against suicide Alcohol and substance
Intimate partner violence (IPV)
and suicidal behaviour, suicide abuse
also peaks during pregnancy
is a leading cause of death for for a wide range of psychosocial See SPA’s 2011 Position
women during pregnancy and reasons (Martin et al 2004), Statement “Alcohol, drugs &
in the year after giving birth strengthening the combined Suicide Prevention” for further
and a significant contributor risk of pregnancy (particularly information on this topic.
to indirect maternal mortality unplanned), IPV and suicidality.
(Austin et al., 2007; Palladino et Substance abuse appears to be
al., 2011; Humphry, 2011). The The protective effect of a strong identifier for detecting
Australian Institute of Health pregnancy may be lessened in women at risk for suicide.
and Welfare (AIHW) in 2008 mothers aged less than twenty Alcohol abuse is considered a
reported that the numbers years or in cases where the distal risk factor for suicide,
increased through to the end of pregnancy ends in stillbirth, with individuals with alcohol
the first postnatal year. Women miscarriage, the loss of a child, abuse having higher rates
tend to use more violent means or is unwanted (Qin et al., 2000; of suicide than the general
in the perinatal period than non- Qin & Mortenson, 2003). There population (Rossow et al, 2007;
childbearing women (Austin et is a long-standing association Potash et al., 2000). Alcohol use
al 2007). between depression/suicidal is also considered a proximal
behaviour and unwanted risk factor, in that alcohol use
While rates of suicide mortality pregnancy (Bunevicius et al., lowers inhibitions that may
appear to be lower among 2009; Newport et al., 2007). normally prevent suicidal
pregnant women than women Rates of suicide ideation and behaviour in individuals who
without pregnancy, there is mental health problems are are not alcoholics (Moscicki,
a close correlation between increased among women 1995). A review of studies found
maternal suicide and severe who have undergone induced alcohol involved in 10% to 69%
postnatal mental illness (Oates, abortions, with some studies of suicides (Cherpitel et al.,
2003; Austin, Kildea, & Sullivan,
20 | Suicide and Suicidal Behaviour in Women – Issues and Prevention2004). According to a recent (Oquendo et al 2007; Curtis Bullying
study, alcohol was detected in 2006).Women who are severely
nearly 28% of women and 36% injured in incidents of domestic Bullying is defined as the
of men who suicided (Kaplan et violence are more likely to ongoing physical or emotional
al., 2014). report depression, anxiety, victimisation of a person.
alcohol abuse, eating disorders The emerging problem of
Less is known about alcohol cyberbullying occurs when
and suicide ideation (Curtis
involvement in nonfatal suicidal people use new communication
2006).
behaviour. Some studies technologies, such as social
suggest that perhaps 30% Women who have been abused media and texting, to harass and
to 50% of hospital-admitted by their intimate partners cause emotional harm to others.
suicide acts involved alcohol are almost four times more Much of the research on this
(Borges et al., 2004; Cherpitel et likely to have suicidal ideation issue has involved adolescents
al., 2004). compared to non-abused in the school setting, however
women (Taft 2006), and are bullying can occur across all
Women’s self-inflicted injuries
at increased risk of suicide ages and social environments.
involved alcohol significantly
attempts (Coker et al., 2002). A
less often than men’s however There is a complex relationship
recent systematic review of 664
men also drink more than between bullying and risk of
relevant studies (McLaughlin
women. Although women suicidal behaviours (Gould et
et al., 2012) demonstrated a
more frequently attempt al. 2003). Bullying and peer
strong, unequivocal relationship
suicide, European emergency victimisation puts adolescents
between intimate partner
department data suggest that at increased risk of suicidal
violence and suicidality.
women are less likely to have ideation and behaviour,
used alcohol immediately prior For women who have especially when other
to a poisoning or other suicidal experienced IPV, suicide is psychopathology is present (e.g.
act then men (Prkacin et al., elevated (Guggisberg 2006 depression) (Van Geel 2014). It is
2001). & 2008). A VicHealth report not necessarily the bullying per
stated that IPV was a leading se; there are many important
Women’s nonfatal poisoning
contributor to the death of mediating variables (Arseneault
suicidal behaviour involved
Victorian women aged between et al., 2010; Wang et al., 2011).
alcohol 21.9% of the time,
15-44 years, accounting for 10% Suicidal ideation and behaviour
compared to 34.3% for men.
of deaths, with more than half is usually not attributed to just
Alcohol and substance use
being suicides (VicHealth 2005). one event or factor.
by women increases their
likelihood of dying by suicide Exposure to childhood sexual Bullying others, and not only
(Conner et al., 2007). abuse can result in increased being victimised, is associated
vulnerability to subsequent with depression, suicidal
Intimate partner violence psychopathology and adverse ideation and attempts (Kaltiala-
(IPV) and sexual abuse life events. The risk of suicide Heino et al. 2000; Roland 2002).
ideation and attempts increases The strongest association
Reducing violence against
with the extent of the abuse. between involvement in
women and children is a
burgeoning issue in Australia, Suicidal ideation is more bullying and depression/
as it is around the world. common among women who suicidal ideation/attempts is
According to the Australian have been sexually assaulted found among those who are
Longitudinal Study on Women’s than the general population both bullies and victims (bully-
Health, 1 in 5 women report (Stepakoff 1998). Younger victims) (Kim & Leventhal, 2008;
having experienced domestic survivors may be at particular Klomek et al., 2007).
violence in the past year. In risk of attempting suicide
2012, more than 130,000 women following rape (Petrak 2002).
were abused by their partners
(ABS 2014).
Women constitute the majority
of victims of sexual abuse and
IPV and these experiences are
linked to suicidal behaviours
Suicide and Suicidal Behaviour in Women – Issues and Prevention | 21You can also read