UNDERNUTRITION AND WEIGHT LOSS IN THE ELDERLY
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

UNDERNUTRITION AND WEIGHT LOSS IN THE ELDERLY NAUSHIRA PANDYA M.D.,C.M.D. Chair and Associate Professor Department of Geriatrics Director, Geriatric Education Center, NSU COM CECILIA ROKUSEK Ed.D., R.D. Professor of Family Medicine and Public Health Executive Director, Geriatric Education Center, NSU COM
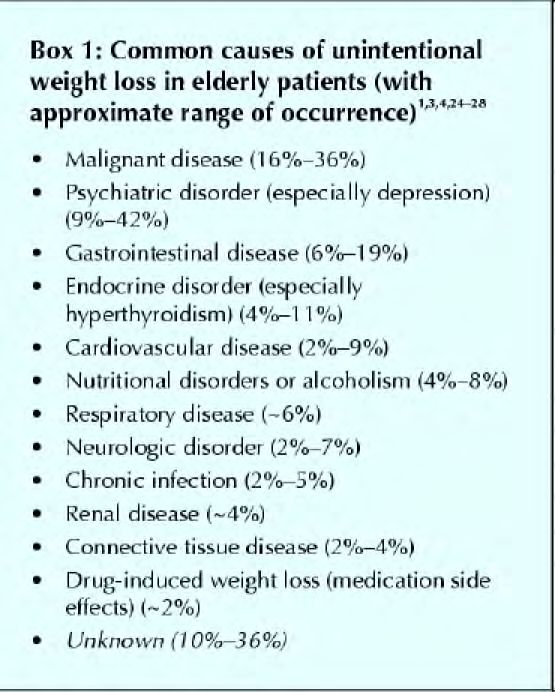
The scope of the problem
Mode of living Prevalence(%) References
Free-living 5 Dept of Health and Social
Sec, UK
7 Dept of Health and Social
Sec, UK
5 Blondel-Cynober et al.
2 Lowink et al.
1-4 Cederholm et al.
Hospital 39 Cederholm et al.
59 Rapin et al.
50 Alix.
22 Volkert et al.
Nursing home 30-60 Rudman et al.
10-85 Kerstetter et al.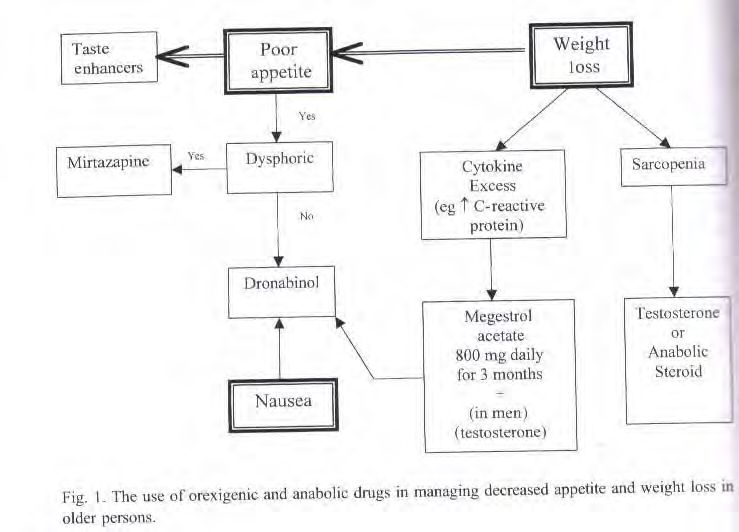
Change in food intake over the life span-
NHANES III
3500 52
3000 51
2500 50
(% of energy)
2000 49 Kcal Men
(Kcal)
Kcal Women
1500 48 Carbs
1000 47
500 46
0 45
20-29 30-39 40-49 50-59 60-69 70-79 >80
Age(y)
NHANES 111 DATA
4% of persons between 60-69 yr were unable to
prepare their meals or walk around
23% of persons over 80 yr were unable to
prepare their meals and 17% were unable to
walk
GFR < 30ml/min/1.72m2 major risk factor for
malnutrition in older adults
30-40% of patients on dialysis were malnourished
Marwick C. JAMA 1997;227
Normal aging changes, physical,
psychological and social precipitants
Anorexia
Weight loss
Malnutrition
Depression
Cognitive dysfunction
Social withdrawal
Isolation
Giving up DEATH Egbert
Barriers to adequate nutritional management of
older patients by physicians
Inadequate training in recognizing protein calorie
undernutrition
Unawareness that protein calorie undernutrition
may be the presenting feature of many treatable
diseases in the elderly
Unawareness of currently available treatment
options
Morley
Conditions associated with protein-energy undernutrition in the elderly Immune deficiency, increased infection, pneumonia Pressure ulcers Poor wound healing Anemia Falls Cognitive deficits, increased delirium Osteopenia, hip fractures Altered drug metabolism Sarcopenia, weakness, fatigue Orthostatic hypotension and dehydration Non-thyroidal illness Decreased maximal breathing capacity Decreased cardiac output

Predictors of nutritional disorders and disability
Katz ADL index score
Serum albumin level
Patient’s current weight as percentage of usual weight
Number of prescribed medications taken
Presence of renal disease (BUN level > 30)
Individual’s income
Presence of one or more decubiti (grade II or higher)
Dysphagia
Mid-arm muscle circumference
Sullivan DHNutrition and immunity in the elderly Infections are more common in the undernourished - especially pulmonary Cell-mediated immunity and delayed hypersensitivity declines Total lymphocyte count ↓ (< 800/mm3 reflects undernutrition) T cell proliferation ↓ B lymphocyte proliferation È Cytokine release ↓ (IL2 and IL1) - fever often absent, and inflammatory syndromes have prolonged evolution periods È CD4:CD8 ratio in undernourished patients who are HIV - Micronutrient supplementation has been showed to restore T cell deficiency (zinc-thymulin, Vit E -?antioxidant)
Usual aging is associated with decrease in skeletal and visceral lean body mass (LBM), bone density, total body water, and increase in total fat SARCOPENIA wasting of CACHEXIA is loss of skeletal muscle both muscle and fat LBM declines 19% in men Not physiologic and 12% in women (25- Occurs in malignancies 75y) and HIV disease Due to aging, inactivity, Systemic inflammatory malnutrition, catabolic response diseases (CHF, COPD, cancer, hyperthyroidism)
Outcomes of Severe Weight Loss in Older Persons Increased hospitalization Increased length of hospital stay Increased hospital costs Delayed recovery from surgery Increased mortality (weight loss in 6 mths in NH pts associated with 2 fold increase in likelihood of death- Yamashita et al. 2002) Increased NH placement in older women (BMI < 21.4 Kg/m2 )
The assessment
Case 1 A 73 yr old woman is noted to have a 10 lb involuntary weight loss at her annual physical Food just does not appeal to her and she can’t be bothered with meals; she lives alone She has HTN, osteoarthritis, glaucoma, and T2 diabetes Medications: captopril, metformin, naproxen Exam: unkempt, apathetic, R knee effusion
What further questions would you ask? What would you look for in the physical exam?
Important points in the history Anorexia? Early satiety? Nausea? Change in bowel habits? Fatigue or apathy? Memory loss? Depression? Food availability? Poverty? Social history
Physical signs of Undernutrition Loss of subcutaneous fat - interossei and palmar creases - loss of fullness in arms, chest wall - squared-off appearance of shoulders Muscle wasting (sarcopenia) - loss of tone and bulk in quadriceps, deltoids - reduced strength Edema of ankles, sacrum, and even ascites - absence of weight loss misleading Dysphoria, decreased cognition Poor wound healing, pressure ulcers
Parameters Used in Identifying Undernutrition
Body weight loss (>5% in 30 days or 10% in 180 days)
Body mass index < 19 kg/m2 (may be spuriously elevated)
Severe if BMI < 16
Dietary food intake of less than 75% of meals for 3 days
Serum albumin value of less than 3.5 or 3.0 g/dl (decreases
by 0.8 per decade after age 60) Influenced by
posture, CHF, dialysis, cytokines, dialysis, nephrosis,
paraproteinemias
Serum cholesterol value of less than 160 mg/dl (occurs late,
limited use for screening)
Associated with hospitalizations, LOS, complications, mortalityScreening and Assessments Tools
SCALES - outpatient screening tool
DETERMINE - a low specificity tool, increases public
awareness, and easily performed by the patient
- developed by the Nutrition Screening Initiative (AAFP,
Am Diet.Assoc, Nat Council of the Aging)
- Level I Screen separates those who need evaluation and
intervention from those who need other medical and
community services
- Level II Screen by physician or other primary provider
(includes anthropometrics, labs, social and functional
testing
MNA - Mini Nutritional Assessment.
Malnutrition Inflammation Score (dialysis patients)SCALES Protocol for evaluating risk of malnutrition in the elderly (scores > 3 indicates patient at clear risk) Morley 1991 Item evaluated Criterion for 1 point Criterion for 2 points Sadness GDS 10-14 > 15 Cholesterol < 160 mg/dl -- Albumin 3.5 - 4.0 g/dl < 3.5 g/dl Loss of weight 1 kg (or ¼” in MAC 3 kg (or 1/2”) (MAC 1 month) in 6 months) Eating problems Patient needs -- assistance Shopping and food Patient needs -- prep problems assistance
Why does caloric intake decrease in the elderly?
ALTERATIONS IN THE HEDONIC QUALITIES OF
FOOD WITH AGING
Food enjoyment depends on taste, odor, temperature,
texture, masticatory sounds, all of which are altered
Smell declines progressively; hence monotonous diets
Alzheimer’s, Parkinsonism, laryngectomy, B12
deficiency, hypothyroidism, RF, cirrhosis, diltiazem,
streptomycin
Reduction in sensory-specific satiety
Increase in taste thresholds; sweet least affected modality;
flavor enhanced foods better consumed
Difficulty recognizing taste mixtures
Social isolationAnorexia of aging- Physiological reduction in food intake with advanced age Food intake is lower in healthy older persons, especially of fat rather than carbohydrates È BMR due to loss of muscle Immobility Greater satiation after a standard meal than younger people Reduced fundic nitric oxide leads to a decrease in adaptive relaxation and earlier satiation (È by leptin, Ç by NPY) Opiod feeding drive (for fats) is less efficient Refeeding can reset appetite
Elderly demented patients often eat enough for their diminished energy
requirements
Hoffer, L J. BMJ 2006;333:1214-1215
Copyright ©2006 BMJ Publishing Group Ltd.Some postulated factors involved in the pathogenesis of physiologic anorexia
ÀTaste and smell
CYTOKINES
OVARIES TNF α
Àestrogen
Interleukin-1
Interleukin-6
CENTRAL NERVOUS
SYSTEM
ADIPOCYTES ÀDynorphin
¿leptin STOMACH
ÀNeuropeptide Y Àadaptive relaxn
¿CART ¿ Antral stretch
TESTIS
Àtestosterone
DUODENUM
ANOREXIA ¿cholecysto-
Àmuscle mass kinin
WEIGHT
LOSSNeurotransmitters and Hormones Involved in the
Control of Food Intake (ÈÇ changes with aging)
Stimulate Inhibit
Peripheral motilin Cholecystokinin
ghrelin Glucagon-like peptide 1
ÇAmylin
Leptin (males only)
cytokines
È Estrogen (females
Hormones Thyroid Cortisol
È Testosterone Progestagens only)
Central Dynorphin Dopamine CRH
neuropeptide Y Norepi Serotonin
orexinA Histamine Isatin
Melanin-conc H ÈNO Dopamine
Ç CARTStress,
Infection
Burns, Trauma
Increase in Inc macrophage
Glucocorticoids proliferation
Mineralocorticoids Inc release of IL1, TNF
ADH Colony stim factor
Decreased IGF1 Gamma interferon
Gluconeogenesis Inc ESR
Protein Energy
Protein catabolism Leukocytosis
Malnutrition
Lipolysis Anorexia
Hypoalbuminemia
Fluid, electrolyte Protein
Liver dysfunction
shifts catabolism
Decreased host defenses
Weight loss
Inc requirement for
Cals + protein
Pathophysiology of protein-energy malnutrition.“Meals on Wheels”: causes of weight loss
M: medications (dig, theophylline, fluoxetine)
E: emotional (depression)
A: alcohol, anorexia tardive, or elder abuse
L: late life paranoia
S: swallowing problems (dysphagia, candidiasis, webs)
O: oral or dental problems (xerostomia)
N: nosocomial infections (TB, C.Diff, H Pylori)
W: wandering, dementia problems
H: hyperthyroidism, hypercalcemia, hypoadrenalism
E: enteric problems (gluten entropathy, pancreatic insufficiency)
E: eating problems
L: low salt, low fat diets (ADA and other therapeutic diets)
S: shopping and food preparation problems MorleyCauses of weight loss - MEDICAL Dysgeusia (antibiotics, captopril, tegretol, allopurinol, L dopa, lithium, baclofen, antihistamines, Vit A, zinc deficiency) Anorexia (Addison’s disease, dyspepsia*,H. Pylori infection, hypercalcemia) Oral and swallowing problems, dry mouth, poorly fitting dentures, web stricture, esophageal candidiasis Malabsorption (Celiac disease, intestinal ischemia) Increased metabolism (hyperthyroidism, pheochromocytoma) Metabolic (diabetes, hepatic, renal, cardiac failure) Chronic infections, TB Mixed causes (cancer*, Parkinsonism, COPD, cardiac cachexia)
Causes of weight loss - SOCIAL Poverty, fixed income Functional impairment limiting ADL’S, dependancy Social Isolation Elder abuse, caregiver fatigue Poor nutritional knowledge Finicky eaters Alcohol Institutional factors- inadequate assistance Ethnic food preferences Monotony of institutionalized food
Causes of weight loss -PSYCHOLOGIC Dementia Depression* Bereavement Alcoholism Late-life mania or paranoia Anorexia tardive or nervosa Sociopathy (loss of locus of control) Excessive burden of life Phobias (cholesterol or choking) Globus hystericus
Drug Therapy That May Contribute to Nutritional Disorders Cardiac glycosides (digoxin) Diuretics Anti-inflammatory drugs Antacids (overuse) Psychotropic drugs Antidepressants (SSRI’s) Antineoplastic drugs Anticonvulsants Phenothiazines Oral hypoglycemics Anti-parkinsonian Anticholinergic
Alibhai, CMAJ. 2005 March
So What is Frailty? A physiologic state of increase vulnerability to stressors that results from decreased physiologic reserves and even dysregulation, of multiple physiologic systems Evidence indicates that Frailty may be a result of alterations in metabolic activity, that then leads to derangement of normal physiology Cytokine over expression Hormonal imbalances
Frailty vs. Disability vs. Co morbidity Fried, LP, et al. Journal of Gerontology 2001 M146 – M156
Consequences of Frailty Disability Difficulty with Activities of Daily living Dependency Falls Need for Long – Term Care Mortality
Phenotype of Frailty
SHRINKING
Unintentional weight loss
Sarcopenia
WEAKNESS
POOR ENDURANCE & ENERGY
SLOWNESS
LOW ACTIVITY
FRAILTY: 3 or more criteria
PREFRAILTY: 1 or 2 criteria
Fried, LP, et al. Journal of Gerontology 2001 M146 – M156Frailty Syndrome Criteria
WEAKNESS
Grip strength in the lowest 20% at baseline; adjust
for gender
MEN and BMI Cutoff for Grip Strength
(Kg) criterion for frailty
BMIAging & Frailty Revised schematic of homeostenosis: The older person employs or consumes physiologic reserves just to maintain homeostasis, and therefore there are fewer reserves available for meeting new challenges Copyright © 2003 Spring-Verlag New York, Inc. All rights reserved.
Cycle of Frailty
Cytokine Over Expression
IL-6, IL-1, TNF-a, IL-2, Hsp70
atherosclerosis
anemia
PAD, CAD,
Cerebrovascular
Falls, Heart
disease failure…
Osteoporosis or
osteopenia
Cognitive decline Sarcopenia
Dementia Fractures Falls
Impairments in Function, mobility, and/or endurance
FRAILTYCytokines & Frailty
Interleukin -6 (IL-6), TNF-alpha, Heat Shock protein
70:
Found to be elevated in older adults who complain of
fatigue and found to have poor mobility and poor muscle
endurance
Bautmans et al. JAGS. 56:3, pgs 389-396
IL-6 found to be elevated in older people with
cachexia
Hubbard et al. JAGS. 56:2, pgs 279-284
That subclinical anemia may be a related to chronic
inflammatory state marked by serum IL-6 elevation
Leng et al. JAGS. 50:7, pgs 1268-1271Hormones & Frailty
Hormone Deficient states may lead to the
following
Growth Hormone, IGF-1 Sarcopenia, Osteoporosis
Testosterone Cognitive decline, Depression,
Osteoporosis
Estrogen * Osteoporosis, Cognitive decline
Vitamin D Osteoporosis, Sarcopenia, poor
mobility
* Replacement not recommendedPrevention of Frailty Address Nutrition, Function & Co-morbidities Diabetes Control Stroke prevention CAD, PAD treatment Fall prevention, Physical therapy interventions Exercise Nutritional evaluations Immunizations, Vaccinations
F. R. A. I. L. T. Y. Food intake: Maintain nutrition, protein intake, fiber intake In between meal supplements Appetite enhancers such as marinol and megestrol Supplement for any nutritional deficiencies B12, B6, Folate
F. R. A. I. L. T. Y. Resistance exercise 3x/ week Resistance with weights or bands builds muscles and helps reduce joint stiffness and pain Exercise has been shown to Increase muscle strength Increase muscle size Increase gait velocity Increase mobility
Case 2 A 68 yr old retired accountant is noted to have a 12 lb weight loss at his clinic visit for a diabetic foot ulcer, complicated by chronic osteomyelitis Meal intake reduced by 50%, but he has adequate resources and lives with his wife who is his caregiver. More fatigued and slow. Exam: CBG 209, cheerful, sarcopenia in UE and LE, draining heel wound,
How would you manage this patients weight loss?
Treatment Strategies Identify cause/causes and initiate targeted dental, medical, psychological, social, or community intervention Thorough evaluation of all prescription and OTC medications Nutrition counseling of patient and caregivers Nutritional supplementation Increased staff at mealtimes, food presentation, taste enhancement, change meal times (not 8-5 PM) Orexigenic drugs
Useful non-invasive screening tests
Complete blood count
Liver function tests (including alkaline
phosphatase and bilirubin), measurement of LDH
Chest radiography
Patients with iron-deficiency anemia or
symptoms likely to originate in the
gastrointestinal tract, and patients with elevated
liver enzyme levels on initial screening, should
undergo
either endoscopy or UGI series
or abdominal ultrasoundIdentify and treat Improved prognosis
the cause + quality of life
Despite therapy no No cause identified or Weight gain
increase in weight no treatable condition
NUTRITIONAL SUPPORT
Frequent small meals high in
protein and fat
Supplements, night snacks Consider enteral
PHYSICAL THERAPY No weight Hyperalimentation
Exercise gain No terminal illlness
OCCUPATIONAL Pt + family consent
THERAPY
? ANABOLIC AGENTS Poor prognosis
A rational approach to the treatment of weight loss in the elderly.Algorithm for managing weight loss in outpatients
NO DEHYDRATION? Treat
YES
DECREASED FOOD AVAILABILITY?
YES Refer to social
NO worker
APPETITE PROBLEM?
YES NO
Treat DELIRIUM? MALABSORPTION? Treat
YES YES
NO NO
Treat DEPRESSION?
HYPERMETABOLISM?
YES
NO
YES
CONSIDER OREXIGENICS
Treat
LOOK FOR TREATABLE CAUSES
? Malignancy ?otherNutritional supplementation Palatable meals high in protein and fats Give priority to ethnic food preferences Nutritional supplements as meal replacements or late night snacks Liquid energy supplements to swallow medications (Medpass 2.0 can treat weight loss in nursing homes) Begin aggressive efforts to assure adequate intake 48h after acute hospital admission Enteral tube feeding (NG or J tube) has fewer problems, is more cost-effective and efficient than parenteral feeding (TPN) Peripheral parenteral nutrition (PPN) for short term support (10% dextrose, amino acids and intralipid)
Calculating enteral feeding requirements
Clinical condition Amount
Protein* Maintenance 1.2 – 1.5 g/kg/day
Stress* 1.5 – 2.0 g/kg/day
Calories# Maintenance 25 – 30 kcal/kg/day
Stress 30 – 40 kcal/kg/day
Sepsis 40 – 50 kcal/kg/day
Free water 30 – 35 ml/kg/day
*Use IBW in obese persons
# Use 120% IBW in obese personsPharmacological treatment of weight loss Small gain in weight without evidence of decreased morbidity and mortality or improved function and quality of life Orexigenic (appetite-stimulating) and anabolic medications Only 4 have been studied in randomized trials
Orexigenic Drugs AGENT MECHANISM OF ACTION Megestrol acetate Progestagen/anticytokine Dronabinol Cannabinoid Cyproheptadine Antiserotonin Anabolic steroids (Oxandrolone) Mainly on muscle Growth Hormone Central Corticosteroids Central Metoclopromide Increased gastric emptying Antidepressants Treat depression (Mirtizapine) 5HT1 agonist, 5HT2 antagonist
MEGESTEROL ACETATE Progestational effect antagonizes estrogen (which ↓ food intake) Main effect is antagonism of cytokine production (TNFα, IL6) Increases appetite, weight, well being and fat mass Useful in older persons with anorexia caused by cytokine excess (cancer, AIDS, P ulcers, arthritis, recurrent infections) May cause DVT or adrenal suppression
Orexigenic drugs and Their Side Effects
Cyproheptadine Delirium
Testosterone (gel,patch, Increased Hct
injection) Not with prostate Ca
Fluid retention
Skin irritation
Oxymethalone/oxandrolone Liver dysfunction
nandrolone Renal failure
Growth hormone Carpal tunnel syndrome
Arthralgias
Increased death
Megestrol acetate Deep vein thrombosis
hypoadrenalism
Dronabinol DeliriumMorley. Clin Geriatr Med Nov 2002
Addressing Weight Loss Issues in the Elderly
Voluntary Weight Loss Dietary modification required because of OW/OB Weight modification because of diagnosed medical conditions Personal feelings of OW
Involuntary Weight Loss Depression (> in LTCF) Cancer Cardiac disorder Alcoholism Benign gastrointestinal diseases Medication Polypharmacy Cognitive impairment
Nutrition Assessment is Key Physiologic Anorexia of Aging
By the age of 65 years, approximately 50 percent of Americans have lost teeth!
Weight loss should NEVER be considered as part of the normal aging process.
Nutritional Assessment Anthropometric measures General physical assessment Dietary assessment Self assessment Medication review Environmental scan
Treatment Team approach Use of flavor enhancers Small, frequent meals Exercise Medications Feeding tubes
Voluntary Weight Loss Issues Planning Exercise ↓ fat usually preferred Small, frequent meals/snacks
!!! REMEMBER !!! Eating food is one of life’s greatest pleasures as we mature!
QUESTIONS? Naushira Pandya, MD, CMD pandya@nova.edu Cecilia Rokusek, EdD, RD rokusek@nova.edu
You can also read

















































