Welcome Public Forum For Education (PFE) - 16 November 2016
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Welcome Public Forum For Education (PFE) 16 November 2016 Children’s Mental Health Issues Department of Children’s Services
Mental Health and Wellbeing in Schools Dr Sarah Exall Specialty Registrar in Public Health Department of Public Health Acknowledgements: Clare Offer Mark Vaughan
Contents • Background • What is the local need? • What do children tell us? • What is the national context? • What is happening locally?
Background • Nationally, around 1 in 10 children aged between 5 and 15 have a mental health disorder. 25% of children with mental health disorders in 2005 had the same disorder 3 years later. • Many more children will experience emotional or behavioural difficulties.
• Risk factors for emotional and behavioural difficulties in children include problems with parenting and family functioning, parental mental health, and socioeconomic disadvantage. • Bullying in childhood is strongly associated with poor emotional wellbeing and future mental health difficulties. • NICE guidelines and national evidence support the promotion of children’s emotional and social well being, particularly in schools.
What is the local need?

• It is estimated that there are currently just under 8,500 children aged between 5 and 15 with diagnosable mental health disorders in Bradford • The rate of mental illness among children rises as they get older • Children in the most deprived wards in Bradford show poor levels of social and emotional development when they start school, which is associated with poorer social, emotional and mental health outcomes later in childhood

Primary classroom Secondary classroom

Self Harm • Bradford’s rate of admission for self-harm among young people aged 10 to 24 is 373.7/ 100,000 • Nationally, rates of admission range from 82.4 to 1,152.4/100,000. • In Bradford, there are an average of 240 admissions relating to self harm in 0-19 year olds each year.
What do children tell us? Images: NHS photo library, www.sesamestreet.org; www.bbc.co.uk; Microsoft clipart; www.shutterstock.com
National strategy and policy
What is happening locally? • Support is provided at school level by school nurses, VCS, pastoral workers, school counsellors, youth workers • Education is provided for the children’s workforce and can be accessed by teachers and other staff working with children and young people
Future in Mind: Children and Young People’s Transformation Plan (2015-2020)
7 work streams: 1. Schools engagement 2. Crisis care 3. Single point of access 4. Eating disorders 5. Caring for the most vulnerable 6. Developing the workforce 7. Accountability and transparency
Aims of the Schools Engagement workstream: •ensure that children and families receive care at the earliest possible opportunity •promote resilience for children and young people •support schools to identify children and young people at risk of mental health issues •provide support for low level need in schools and develop clear access routes offering choice, with easy access to appointments •develop a culture in schools which does not stigmatise mental distress or ill-health
How this will be achieved: •increasing the number of Primary Mental Health Workers •developing a Mental Health Champion role for each school •developing a mental health in schools pathway
Useful links • https://jsna.bradford.gov.uk/documents/Health%20Needs%20As sessments/Mental%20Health%20Needs%20Assessment/Menta l%20Health,%20Emotional%20and%20Social%20Wellbeing%2 0in%20Children%202015.pdf • https://jsna.bradford.gov.uk/documents/home/Children%20and %20Young%20Peoples%20Lifestyle%20Survey%202013%20 %20SUMMARY.pdf • https://www.bradford.gov.uk/media/3030/ cyptransformationplanbradfordfutureinmind.pdf
Thank you • Any questions? Sarah.Exall@bradford.gov.uk Mark.Vaughan@bradford.nhs.uk
Mental Health Matters in Bradford: Addressing Self Harm in Schools Dr Philippa Grace Specialist Senior Educational Psychologist 16/11/16 Department of Children’s Services
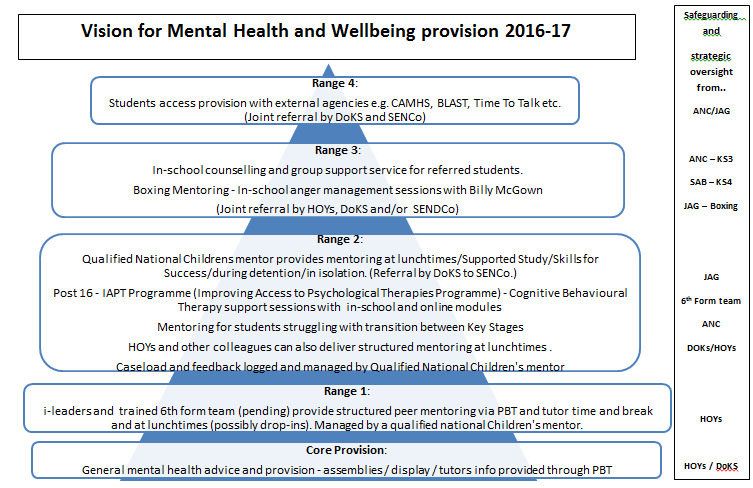
Mental Health in Schools Strategy Group: Aiming to • Deliver a core offer across Bradford schools • Harness and maximise existing resources • Respond to local needs • Build on evidence based practice and pilot and quality assure new initiatives Department of Children’s Services
Mental Health Matters: Core Principles • Increase knowledge and reduce shame, stigma and secrecy • Normalise emotional distress • Deliver support where children, young people and parents say it works best Department of Children’s Services
Mental Health Matters! • Self harm policy and recording protocol • Mental Health Awareness Raising Assemblies • Mental Health Information Hubs in Secondary Schools • Getting Through Tough Times leaflets for secondary aged pupils • Mental Health Matters Conference Department of Children’s Services
The self harm protocol policy means…… • Vulnerable pupils receive appropriate support from confident staff • There is a consistent approach to responding to pupils who self harm, and in monitoring self harm in school Department of Children’s Services
This protocol policy provides….. • a structure for school staff, • using good practice guidelines from the National CAMHS guidance on self harm • reassurance to staff, and identifies relevant information, and where appropriate onward referrals
The Core Message • The best prevention for self harm in young people is to have people who they can talk to and who will take them seriously • National CAMHS guidance p 10 Department of Children’s Services
What is Self Harm? • ‘Self harm happens when someone hurts or harms themselves…. • Since we cannot answer the question definitively of what counts as ‘deliberate’ we define self harm as ‘what happens when someone hurts or harms themselves Department of Children’s Services
How Common is Self Harm? • 10-15% of 11-15 year olds Lancet 2012 • 20% of 11-15 year olds WHO 2013 • 18.8% of 11-15 year olds diagnosed with depression • 9.4% of 11-15 year olds diagnosed with anxiety • 7.5% of 5-10 year olds with conduct/ hyperkinetic disorder Department of Children’s Services
Young people explain the self harm to… • Punish themselves • Relieve tension or stress • Communicate their distress to other people • Take control when they feel powerless • Make themselves feel real, if they feel numb and remote from the world • Nurture themselves, through caring for the wounds
The cycle of self harm Negative emotions Tension Self harm act Positive effects ( endorphins and tension released) Negative effects
A continuum of self harm ‘it is most helpful to consider self harm as a continuum from behaviour which has a strong suicidal intent ( e.g. some overdoses) to behaviour which is intended to help the young person to stay alive.’ •Coleman 2004
Myths and Stereotypes • Self harm is manipulative? • It is a form of revenge? • It’s attention seeking? • It’s a cultish teen behaviour? • It’s a failed suicide attempt and the person should be placed on suicide watch? • Evidence of a borderline personality disorder?
Safeguarding and confidentiality • Young people anonymously report a much higher rate of self harm ….from this we can infer the importance of confidentiality and the wish to control their own situation…. • ‘those young people who spoke to an adult said that once they had done this all decision making and control were taken from them’ Truth Hurts 2008 Department of Children’s Services
Good reasons for early intervention • Early intervention may tackle the cause of the emotional pain, or offer alternative ways of coping • Some people may want to stop self harming, but they need advice and/ or encouragement • Early intervention can prevent escalation
How can we help our
children through tough
times?
• Normalise feelings of despair
• Teach and / or model coping skills
• Improve the situation
• Teach strategies to reduce tension
• Identify positive and physical activities
• Teach / model self talk – rehearse this
• Promote belonging and sense of
connectednessAlternatives to self harm Self harm websites usually have lots of ideas about alternatives to self harm. These include: • Clenching ice cubes ( make them with fake blood) • Draw red lines on your skin • Elastic bands on wrist • Harmless pain – eating a chilli Looking at these together reduces shame and increases sharing and the feeling of being understood
When you find out about self harm
• Do • Don’t
• Make sure they are safe • Tell them to stop
• Remove possible • Encourage them to
equipment carry on
• Listen • Rush to tell parents –
• Show concern take care!
• Debrief with colleagues • Show fear, revulsion or
and report panic
• Deal with it alone
• Feel responsibleManaging Self Harm in School Protocol for responding to self harm in schools: •Brief overview •Key components •Resources •Onward referrals
Future in Mind:Mental Health Champions in Every School Support to deliver evidence based interventions in schools Training and supervision for school staff Developing and delivering psychoeducational resources for school staff
References • National CAMHS Support Service • ‘Self Harm in Children and Young People Handbook 2011 • Royal College of Psychiatrists Self Harm fact sheets • www.psych.ox.ac.uk/news/new-guide-for parents-who-are-coping-with-their child2019s-self-harm-2018you-are-not alone2019 • Dealing with Self Injury Young Minds
Thank You Dr Philippa Grace Specialist Senior EP (Mental Health) philippa.grace@bradford.gov.uk
Rhian Beynon,
Team Manager
Adoption and Fostering
Jamie Gutch
Assistant Headteacher
Ilkley Grammar SchoolChildren’s Mental Health and the
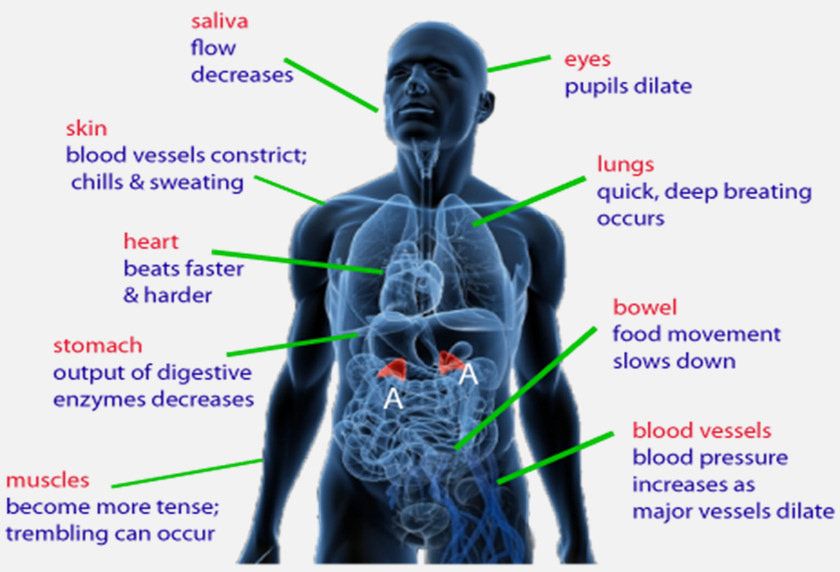
neurobiology of stressThe Triune Brain
Reason
Relate
RegulateThe Executive Functions
• emotional regulation • reflection
• inhibition
• concentration
• empathy
• self-awareness
• planning
• decision making • rationalising panicFight or Flight • The Lower brain deals with survival and is 40 times faster than our rational brain • The lower brain receives sensory information first and responds to perceived danger by activating our stress response system. • It has memory templates for things that are safe and things that are dangerous. • New experiences are initially categorised as potentially � dangerous. � • Children who have experienced attachment-related traumas � are very easily triggered into a powerful dysregulated state. �
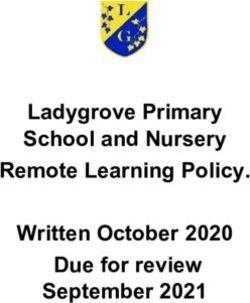
Stress Response
Dissociation • Reduction of Heart rate • Disconnect from self or environment • Memory Gaps • Compliance • Lack of Individuation • Fainting
A child who has experienced abuse, neglect and loss is likely to have deeply embedded beliefs, such as ….. • The world is a dangerous and frightening place • I cannot trust anyone • I must take control of my own survival • I am never certain of the motives of others • Food and comfort are in short supply
Life on Planet Shame • It was all my fault • I am a bad child • I am a loser • I am rubbish • I am unlovable • I don’t deserve to be cared for • I don’t deserve good times • People will hurt me • People will abandon me
Shame – Be Alert • Shame is ‘I am a bad child’ not ‘I am a good child who � made a mistake’ � • Shame is toxic • A child in shame learns nothing from an experience, it � only confirms to them they are bad � • Social Learning Theory only works if the child trusts the motivations of the caregiver. • Is my response going to increase or decrease feelings of shame?
Feeding the monster • Shaming – red traffic lights, sad faces, dark clouds � reinforce the child’s self view � • Excluding – denying good times and positive experiences � • Taking things away – reinforcing old lessons • Rewards and praise – may clash with the child’s inner � narrative � • Control battles – trauma will usually win
Surprising the monster with P.A.C.E • Playfulness – fun, relaxed, lightness, non critical, � enjoyment, humour, soft tone. � • Acceptance – You’re ok, feelings are valid, I accept your � sadness/anger/fear (not behaviour) � • Curiosity – Non-judgemental, I wonder…, I’m interested, reflection, I want to understand. • Empathy – I feel your pain, I’m here with you, You are � not alone, I can handle your distress. �
The Three ‘R’s
Reason
Repair/Relate
RegulateFreeze
Working with students with �
Attachment difficulties and the practical implications �
for decision-making in schools �
A work in progress by
Jamie Gutch �Jamie Gutch � •Arrived at IGS in Jan 2015 and joined the Leadership team in a T&L role…. •Previously Head of Languages at Harrogate Grammar School, G&T Co-ordinator, Pupil Premium focus. Been in education since September 2005 •Current role (as of Sept 2015 with some twists and turns…) – AHT Groups, Inclusion and Intervention – LM Learning Support – LM Key Stage 4 – LM CEIAG and Alternative Curriculum •Key changes at IGS 2016-17 – Move to non-teaching HOYs – New SENDCo in place – Beth Donkin
IGS context • Ilkley Grammar School is a non-selective comprehensive Academy (2011) for 11-18 year olds. • There are 1614 students on roll, (354 students in post 16). • The academic profile on entry in year 7 is consistently sig. above the nat. ave. • Pupil Premium funding for 127 students (7.9% of our school population). 36 Year 7 students are PP. • 226 students (14.0%) with SEND (below the nat. ave). This includes 208 SEN K students and 24 with a Statement or EHCP (10 in Y7) . • 110 teachers (31 part time) and 87 support staff • Attendance is high and isolation, exclusion and permanent exclusion rates are low. • Taking into account starting points, the overall progress of students exceeds ‘good’ in many areas across the curriculum including English and mathematics. This is supported by a significantly positive P8 score of +.23 in 2015, and estimated scores of at least +.3 in 2016. The percentage of students making 4LOP is higher than adjusted national figures in every subject. But….
But…
• We have a growing incidence of mental health issues due to..
– Family breakdown
– Social media
– High expectations
• We had 38 children who met the threshold for CAMHS last year.
• There is a core of children and families (around 8%) who are very disengaged and
difficult to reach precisely because they are relatively small in number. These are
very isolated in the context of IGS due to their deprivation relative to the majority.
A number of these are well known to the police .
• We currently have 21 children who are LAC or who have been adopted from care.Discovering a framework
for
managing children with
attachment difficulties..
Where are we? At the start of a journey
– Sig. increase in the number of students exhibiting symptoms of
fight, flight or freeze.
– A skills/training gap emerged.
– Contacted by a number of parents of adopted children and
began working with some key students and families. Patterns
emerged.
– At a CAF Nicky Poprikova offered the possibility of delivering
CPD with her colleague Rhian Beynon.
– CPD was attended by around 25 IGS colleagues and resonated
deeply with our struggle to manage key students.Challenges for (secondary) schools
• Fight : Violent behaviour – students are often physically quite big and
are in a non-rational, dysregulated state.
• Flight : Safeguarding – on a large school site there are multiple
‘changeovers’ between different professionals during a school day.
(e.g. at least 26 people involved in a recent communication re provision for
1 student)
• Freeze : Refusal to follow instructions leading to frequent escalation.
(e.g. Teacher-LSA-HOY-AHT-DHT-Parent-Police)
Adolescence is a time of huge change – mentally, physically, sociallyChallenges cont.
Personalisation V consistency �
Parents – ‘my child doesn’t fit your behaviour policy why can’t you adapt
what you do?’
Students – ‘they get away with it, why can’t I?’
Teachers – ‘I’m being inconsistent and risk being a hypocrite’
Some of the challenges for decision-making… �
•Consistency (Implementing the Behaviour policy)
•Financial cost (Provision of expensive interventions)
•Time cost (Intensive deployment of staff, often 1:1)
•Risk management (honouring non-negotiable safeguarding responsibilities)
– Children seem to inhabit a different reality (Memory gaps / dysregulated states)
– Children display a lack of trust (Authority seems undermined)Solutions that seem to be working for us…
1. Allow sanctions to be delayed and students to ‘take 5’.
2. Provide ‘Time in’ (freeze) and ‘Time out’ (fight/flight) cards.
3. Explore pro-active rather than re-active interventions
4. Plan high-quality whole school CPD on Attachment Disorder
5. Try interventions which explore risk management
6. Ensure Transparency re decision-making, include all stakeholders
7. Agree safe spaces and identify key ‘trusted’ colleagues as part of a support
plan.
8. Always have a plan A,B,C,D,E,F,G…a creative, graduated and structured
response which accepts that
– it takes a disproportionately long time to build trust
– interventions often won’t work
– rejection of intervention may not seem rational
– Plan H,I and J may require a move to a different setting
It is sometimes more about doing something than doing the right thing �« Time in » card
Y9 Alternative Curriculum « Skills for Success »
Pro-active interventions
You can also read