2022 Ready or Not: PROTECTING THE PUBLIC'S HEALTH FROM DISEASES, DISASTERS, AND BIOTERRORISM
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Ready or Not:
ISSUE REPORT
PROTECTING THE PUBLIC’S HEALTH FROM
DISEASES, DISASTERS,
AND BIOTERRORISM 2022
SPECIAL SECTION: Lessons of the Pandemic’s Tragic
Death Toll: What Needs to be Done to Save Lives During
the Next Public Health Emergency?
MARCH 2022
Acknowledgements
The National Health Security Preparedness Index (NHSPI)
Trust for America’s Health (TFAH) is a nonprofit,
is a joint initiative of the Robert Wood Johnson Foundation,
nonpartisan public health policy, research, and advocacy
the University of Kentucky, and the University of Colorado.
organization the promotes optimal health for every person
TFAH wishes to recognize and thank Glen Mays and Michael
and community and makes the prevention of illness and
Childress of the NHSPI for their collaboration and expertise.
injury a national priority.
Ready or Not and the NHSPI are complementary projects that
Any opinions, findings, conclusions, or recommendations
work together to measure and improve the country’s health
expressed in this report are those of the authors and do not
security and emergency preparedness. TFAH looks forward to a
necessarily reflect the views of the funders.
continued partnership in order to protect the public’s health.
TFAH BOARD OF DIRECTORS Stephanie Mayfield Gibson, M.D. Eduardo Sanchez, M.D., MPH
Director Chief Medical Office for Prevention
Gail Christopher, D.N.
U.S. COVID-19 Response Initiative American Heart Association
Chair of the Board of Directors
Resolve to Save Lives
Trust for America’s Health Umair A. Shah, M.D., MPH
Executive Director Cynthia M. Harris, Ph.D. Secretary of the Health
National Collaborative for Health Equity Associate Dean for Public Health and Washington State
Former Senior Advisor and Vice President Director and Professor
W.K. Kellogg Foundation Vince Ventimiglia, JD
Institute of Public Health
President
Florida A&M University
David Fleming, M.D. Collaborative Advocates
Vice Chair of the Board of Directors David Lakey, M.D. Leavitt Partners
Trust for America’s Health Chief Medical Officer and Vice Chancellor for
TFAH Distinguished Visiting Fellow Health Affairs TRUST FOR AMERICA’S HEALTH
Trust for America’s Health The University of Texas System LEADERSHIP STAFF
Robert T. Harris, M.D., FACP Octavio Martinez Jr., M.D., MPH, MBA, FAPA
J. Nadine Gracia, M.D., MSCE
Treasurer of the Board of Directors Executive Director
President and CEO
Trust for America’s Health Hogg Foundation for Mental Health
Senior Medical Director The University of Texas at Austin
General Dynamics Information Technology
John A. Rich, M.D., MPH
Theodore Spencer, M.J. Co-Director
Secretary of the Board of Directors Center for Nonviolence and Social Justice
Trust for America’s Health Drexel University School of Public Health
Co-Founder
Trust for America’s Health
REPORT AUTHORS EXTERNAL REVIEWERS
Matt McKillop, MPP This report has benefited from the insights and expertise of the following external reviewers. Their
Senior Health Policy Researcher and Analyst review is not necessarily an endorsement of its findings or recommendations by the reviewer or
their organization. TFAH thanks the reviewers for their time and assistance.
Rhea K. Farberman, APR
Director of Strategic Communications and Meredith Allen Stephen Redd, M.D.
Policy Research Vice President for Health Security Retired, former Deputy Director of Public Health
Association of State and Territorial Health Service and Implementation Science
Dara Lieberman, MPP
Officials (ASTHO) Centers for Disease Control and Prevention
Director of Government Relations
Stephanie Mayfield Gibson, M.D. Irwin Redlener, M.D.
Director, U.S. COVID-19 Response Initiative Founding Director
Resolve to Save Lives National Center for Disaster Preparedness
Director
Joneigh Khaldun, M.D., MPH, FACEP
Pandemic Resource and Response Initiative
Vice President and Chief Health Equity Officer
(PRRI)
CVS Health
Senior Research Scholar
Earth Institute, Columbia University
2 TFAH • tfah.org
Table of Contents Ready or Not
TABLE OF CONTENTS
Executive Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
SPECIAL SECTION: Lessons of the Pandemic’s Tragic Death Toll: What Needs to be
2022
Done to Save Lives During the Next Public Health Emergency? . . . . . . . . . . . . . . . . . 11
INTERVIEW: The Critical Role of Public Health Laboratories During COVID-19 and
Beyond. An Interview with Scott Becker, MS, CEO, Association of Public Health
Laboratories . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
SECTION 1: A
SSESSING STATES’ PREPAREDNESS . . . . . . . . . . . . . . . . . . . . . . . . 18
Indicator 1: Nurse Licensure Compact . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Indicator 2: Comprehensive Public Health System . . . . . . . . . . . . . . . . . . . . . . . . 21
Indicators 3 and 4: Accreditation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Indicator 5: Public Health Funding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Indicator 6: Community Water System Safety . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Indicator 7: Access to Paid Time Off . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Indicator 8: Flu Vaccination Rate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
Indicator 9: Patient Safety in Hospitals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
Indicator 10: Public Health Laboratory Surge Capacity . . . . . . . . . . . . . . . . . . . . . 35
Indicators Performance Matrix by State . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
SECTION 2: RECOMMENDATIONS FOR FEDERAL AND STATE POLICY ACTIONS . . . 40
P
riority Area 1: Provide Stable, Sufficient Funding for Domestic and Global Public
Health Security . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40
Priority Area 2: Prevent Outbreaks and Pandemics . . . . . . . . . . . . . . . . . . . . . . . . 43
P
riority Area 3: Build Resilient Communities and Promote Health Equity in
Preparedness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46
P
riority Area 4: Ensure Effective Leadership and Coordination . . . . . . . . . . . . . . . 48
riority Area 5: Accelerate Development and Distribution of Medical
P
Countermeasures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
Priority Area 6: Ready the Healthcare System to Respond and Recover . . . . . . . . 52
Priority Area 7: Prepare for Environmental Threats and Extreme Weather . . . . . . . . 54
APPENDIXES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
Appendix A: Year in Review: Overview of the Year’s Major Public Health Emergencies,
Threats, and Reports . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
Appendix B: Methodology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62
Endnotes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
MARCH 2022
3
Ready or Not Executive Summary
EXECUTIVE SUMMARY
2022 As this report was being prepared, over 900,000 people in the
United States and nearly 6 million worldwide had died due to
COVID-19,1 and the world had experienced two years of economic
and social disruption. In addition, 2021 saw record heat in many
states, extensive flooding, a highly active Atlantic hurricane season,
and unusual and deadly December tornados. These events led
to nearly unprecedented levels of illness, social upheaval, and
economic hardship, including overwhelmed hospitals, job loss,
property loss, children’s learning loss, and mental health concerns.
During 2021, the nation made progress At the same time, major challenges
in many areas in its response to the remained. Hospital systems in many
pandemic. As this report was being states were overwhelmed during
produced, 62 percent of the nation’s pandemic waves. Testing was difficult
population was fully vaccinated,2 to access during surges—at-home tests
averting an estimated 1.1 million were particularly difficult to find—and
COVID-19 deaths and over 10 million in some cases testing was expensive,
COVID-19-related hospitalizations.3 misinformation was abundant, and
The Biden Administration restored the public patience with and trust in public
White House Directorate on Global health guidance wore thin. Of great
Health Security and Biodefense and concern, lawmakers in many states
created the Presidential COVID- introduced or enacted laws to restrict
19 Health Equity Task Force (see the authority of public health officials.6
sidebar on pg. 15). And the approval In addition, according to The New York
of new treatments for COVID-19 has Times, approximately 500 public health
increased the likelihood of survival for officials nationwide had left the field
many patients.4 since the start of the pandemic. Some
Editor’s note: as of January 16, 2022, the Centers for Disease Control and Prevention
(CDC) defined “fully vaccinated” as a person who has received their primary series of
COVID-19 vaccines. CDC is also using “Up to Date” to denote that a person has received all
recommended COVID-19 vaccines including any booster dose(s) when eligible.5
MARCH 2022
retired, some left due to threats and increased public health laboratory These data points are meant to measure
harassment, some due to firings when capacity, sustained growth and states’ readiness on a broad set of health
public health guidance clashed with increased diversity in the public health security measures and have been the focus
what elected officials wanted to do.7 workforce, and addressing the social of this report for over a decade. However,
determinants of health. Today, only for this 2022 edition of the report (and
In addition, the pandemic has
half of all U.S. residents are protected going forward), there is one change to the
illuminated two stark realities: the
by a comprehensive local public health indicators set: the hospital participation
nation and the world’s public health
system,10 and it is estimated that state in healthcare coalitions indicator, which
systems are inadequate and in
and local health departments need to was based on 2017 data that has not been
immediate need of significant and
hire a minimum of 80,000 additional recently updated by the National Health
sustained funding. And, once again,
full-time workers to be able to meet their Security Preparedness Index (NHSPI),
the nation’s health inequities led to
communities’ basic public health needs.11 has been replaced with a new indicator,
some population groups, particularly
also tracked by NHSPI, that measures the
communities of color and low-
percentage of state populations served by
income communities, experiencing a
It is estimated that state and a comprehensive public health system.
disproportionate burden during the
pandemic, with less access to resources local health departments need Readers should note that this report is
like vaccines during the response, and to hire a minimum of 80,000 not designed to be an assessment of a
having more barriers to recovery.8,9 given state’s response to the COVID-
additional full-time workers 19 pandemic, as widescale political,
To better meet the challenges of future
public health emergencies, including
to be able to meet their funding, economic, and social factors all
influenced the virus’s impact and local
climate change, the nation must communities’ basic public
responses. Controlling the pandemic has
address underlying drivers of economic
health needs. been extremely challenging in every state.
and health inequities, including
Moreover, the pandemic has illustrated
ongoing discrimination, structural
that being prepared to adequately
racism, and social determinants of
This annual report, Ready or Not: respond to a public health emergency the
health. Investments in public health
Protecting the Public’s Health from Disease, scale of a pandemic—and execute that
infrastructure alone, while critical,
Disasters, and Bioterrorism, has tracked response—is enormously complex and
will not make the United States more
the nation’s public health emergency beyond the sole control of state and local
resilient. Equity must be an explicit and
preparedness since 2003. The report officials. However, this report measures
foundational principle in all public health
is designed to give policymakers at all critical capacities that are foundational
preparedness, response, and recovery.8,9
levels of government actionable data to protecting the public’s health every
The COVID-19 pandemic’s impact— and recommendations with which they day and during emergencies, including
including its high death tolls and extreme can target policies and spending to robust and sustained public health
economic disruption—was, at least to strengthen their jurisdiction’s emergency funding, disease surveillance capacity,
some degree, an avoidable tragedy. But preparedness. The report’s 10 key public healthcare, public health laboratory and
with this tragedy comes opportunity. health preparedness indicators give hospital surge capacity, access to safe
The pandemic has shined a bright light state officials benchmarks for progress, water, and access to paid time-off. In
on what’s needed: robust, flexible, and point out gaps within their states’ all- addition, the pandemic has shown that
sustained investment in public health hazards preparedness, and provide data there is no substitute at the state or local
infrastructure, modernization of data to compare states’ performances against level for a strong federal response during
systems and surveillance capacity, similar jurisdictions. an emergency.
TFAH • tfah.org 5
This Year’s Findings
In this 2022 report, Trust for America’s compared with last year, while 16 fell movement between tiers this year than
Health (TFAH) found that 12 states behind. Nine states improved by one in past years—in both directions—in
improved their relative standing— tier, three states improved by two tiers, part because of the introduction of a
for each indicator and overall, states and 16 states dropped one tier. (Note: new indicator.)
were scored relative to one another— There was greater year-over-year state
TABLE 1: Top-Priority Indicators of State Public Health Preparedness
INDICATORS
1 Incident Management: Adoption of the Nurse Licensure Compact. 6 Water Security: Percentage of the population that used a community
water system that failed to meet all applicable health-based standards.
2 Public Health System Comprehensiveness: Percentage of state 7 Workforce Resiliency and Infection Control: Percentage of employed
population served by a comprehensive public health system (new). population that used paid time off in a given month.
3 Institutional Quality: Accreditation by the Public Health 8 Countermeasure Utilization: Percentage of people ages 6 months or
Accreditation Board. older who received a seasonal flu vaccination.
4 Institutional Quality: Accreditation by the Emergency Management 9 Patient Safety: Percentage of hospitals with a top-quality ranking (“A”
Accreditation Program. grade) on the Leapfrog Hospital Safety Grade.
5 Institutional Quantity: Size of the state public health budget 10 Health Security Surveillance: The public health laboratory has a plan
compared with the past year. for a six- to eight-week surge in testing capacity.
Notes: The 2022 edition of the report introduces a new indicator, measuring the percentage of state populations served by a comprehensive public health
system. This new indicator replaces a previous indicator tracking the percentage of hospitals participating in healthcare coalitions. The National Council of
State Boards of Nursing organizes the Nurse Licensure Compact. Systems for Action uses the National Longitudinal Survey of Public Health Systems to mea-
sure public health system comprehensiveness. The U.S. Environmental Protection Agency assesses community water systems. Paid time off includes sick
leave, vacation time, or holidays, among other types of leave. The Leapfrog Group is an independent nonprofit organization. TFAH drew every indicator, and
some categorical descriptions, from the National Health Security Preparedness Index, with one exception: public health funding. See “Appendix B: Methodol-
ogy” for a description of TFAH’s funding data-collection process, including its definition.
Source: National Health Security Preparedness Index12
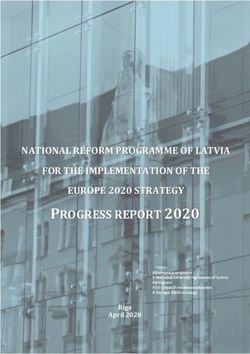
The Ready or Not report groups states and from the low tier to the middle tier had introduction of the new Public Health
the District of Columbia into one of three three primary drivers. First, while still System Comprehensiveness indicator.
tiers (high, middle, and low) based on below average, the state performed Pennsylvania also adopted the Nurse
their relative performances across the better in the new indicator (Public Licensure Compact, benefited from
10 indicators. This year, 17 states and the Health System Comprehensiveness) the new indicator, increased its public
District of Columbia scored in the high- than it had in the now-replaced measure health funding, and experienced only
performance tier, 20 placed in the middle- of hospital participation in healthcare a small reduction in the share of its
performance tier, and 13 were in the coalitions. Second, its share of employed hospitals who received an “A” rating
low-performance tier (see Table 2). (See residents who used paid time off based for patient safety at a time when the
“Appendix B: Methodology” for more on a one-month sample increased, national average fell by a greater extent.
information on the scoring process.) while the national average stayed flat. Collectively, these improvements were
Third, the state’s hospitals made marked sufficient to offset some decline in
Nine states showed notable improvement,
improvement in the area of patient safety. the share of its employed residents
moving up a tier: Alabama, Florida,
who used paid time off. Finally, South
Illinois, Iowa, New Jersey moved from the Three states—Ohio, Pennsylvania,
Carolina’s score benefited from the
middle tier to the high tier, and Arizona, and South Carolina—demonstrated
new indicator, in addition to the state
Missouri, New Hampshire, and New York exceptional progress, elevating from the
achieving accreditation by the Public
moved from the low tier to the middle low tier to the high tier. Ohio adopted
Health Accreditation Board and greater
tier. As an example of the factors behind the Nurse Licensure Compact in 2021,
usage of paid time off.
such movement, New Hampshire’s rise and its score also benefited from the
6 TFAH • tfah.org
Sixteen states fell one tier: Delaware, to the low tier). New Mexico, for
Georgia, Idaho, Maine, Mississippi, instance, saw its score fall because it lost
Nebraska, New Mexico, North its accreditation from the Emergency
Carolina, Oklahoma, Rhode Island, Management Accreditation Program,
and Wisconsin moved from the high vaccinated a smaller percentage of its
tier to the middle tier, and Kentucky, residents against seasonal flu, and had
Louisiana, Minnesota, Montana, and a slightly smaller share of its hospitals
Oregon moved from the middle tier receive an “A” rating for patient safety.
TABLE 2: State Public Health Emergency Preparedness
State performance, by scoring tier, 2021
Performance Number of
States
Tier States
AL, CO, CT, DC, FL, IA, IL, KS, MA, MD, NJ, OH,
High Tier 17 states and DC
PA, SC, UT, VA, VT, WA
AZ, CA, DE, GA, ID, ME, MI, MO, MS, NC, ND,
Middle Tier 20 states
NE, NH, NM, NY, OK, RI, TN, TX, WI
AK, AR, HI, IN, KY, LA, MN, MT, NV, OR, SD,
Low Tier 13 states
WV, WY
Note: See “Appendix B: Methodology” for scoring details. Complete data were not available for U.S.
territories.
Indicators of State Public Health Emergency Preparedness
State performance, by scoring tier, 2021
WA
MT ME
ND
OR MN VT
ID NH
SD WI NY MA
WY MI
CT RI
NE IA PA NJ
NV
IL OH DE
UT IN
CA MD
CO WV DC
KS MO VA
KY
NC
AZ TN
OK
NM AR SC
MS GA
AL
TX LA
FL
AK
High Tier
Middle Tier
HI
Low Tier
TFAH • tfah.org 7
TFAH’s Analysis Found: Emergency Management Accreditation
A majority of states have made Program accredited 42 states and the
preparations to expand healthcare District of Columbia; 32 states and the
and public health capabilities in District of Columbia were accredited by
an emergency. Thirty-seven states both groups, a net increase of three since
participated in the Nurse Licensure December 2020. Eight states (Alaska,
Compact, up from 26 in 2017,13 with Hawaii, Kentucky, New Hampshire,
Ohio, Pennsylvania, and Vermont being South Dakota, Texas, West Virginia, and
the most recent adopters.14 The compact Wyoming) were not accredited by either
allows registered nurses and licensed group. Both programs help ensure that
practical or vocational nurses to practice necessary emergency prevention and
in multiple jurisdictions with a single response systems are in place and staffed
license. In an emergency, this enables by qualified personnel.
health officials to quickly increase their Seasonal flu vaccination rates, while still
staffing levels. For example, nurses may too low, have risen significantly in recent
cross state lines to work at evacuation years. The seasonal flu vaccination
sites or other healthcare facilities. In rate among Americans ages 6 months
addition, only the District of Columbia and older rose from 42 percent during
reported not having a plan to ensure the 2018–2019 season to 52 percent
public health laboratories are prepared during the 2019–2020 and 2020–2021
for a large influx of testing needs. (The seasons.15,16 However, Healthy People
District of Columbia reported that it was 2030, a set of federal 10-year objectives
in the process of updating its Continuity and benchmarks for improving the
of Operations Plan and developing a health of all Americans by 2030, set
discrete plan for laboratory surges.) All a seasonal influenza vaccination-rate
other states had a plan to surge public target of 70 percent annually.17
health laboratory capacity for six to eight
weeks as necessary during overlapping Still, despite these positive steps, just
emergencies or large outbreaks. half of the U.S. population is served
by a comprehensive public health
Most residents who received their system—an indicator newly tracked in
household water through a community the 2022 edition of this series. Such
water system had access to safe water. On systems tend to engage in a wide array
average, just 5 percent of state residents of recommended activities to assess their
used a community water system in 2019 communities’ health and needs, develop
(latest available data) that did not meet evidenced-based public policy that
all applicable health-based standards, promotes health and safety, ensure that
down slightly from 7 percent in 2018. necessary services are accessible to all
Water systems with such violations residents, and cultivate a broad coalition
increase the chances of water-based of stakeholder partners. Comprehensive
emergencies in which contaminated systems have been shown to contribute
water supplies place the public at risk. to positive health outcomes in a cost-
Most states are accredited in the areas of effective manner. In just eight states and
public health, emergency management, the District of Columbia were a majority
or both. As of November 2021, the of residents served by a comprehensive
Public Health Accreditation Board or the public health care system.
8 TFAH • tfah.org
In March 2020, 55 percent of employed under certain conditions, but these
state residents, on average, used paid protections expired on December 31,
time off, the same percentage as in 2018 2020.19 Importantly, the United States
and 2019. Those without paid leave are could join numerous countries across
more likely to work when they are sick the world in establishing a national
and risk spreading infection. In the past, minimum standard of paid family or
the absence of dedicated paid sick leave medical leave, if proposed provisions of
has been linked to or has exacerbated the Build Back Better Act become law.
some infectious disease outbreaks.18 This
Only 28 percent of hospitals, on
has become particularly relevant during
average, earned a top-quality patient
the COVID-19 pandemic, as isolation
safety grade, down slightly from 31
and quarantine are important tools for
percent in 2020. Hospital safety scores
controlling the outbreak. The Families
measure performance on such issues as
First Coronavirus Response Act helped
healthcare-associated infection rates,
address this issue during the early
intensive-care capacity, and an overall
stages of the pandemic for employers
culture of error prevention. In the
with fewer than 500 employees and
absence of diligent actions to protect
certain public employers, temporarily
patient safety, deadly infectious diseases
requiring employees to be paid up
can take hold or strengthen.
to 80 hours of sick leave benefits
POLICY RECOMMENDATIONS
Based on the data collection and 3. Building resilient communities enterprise to enable rapid development
analysis summarized in this report, and promoting health equity in and effective deployment of life-saving
and consultation with public health and preparedness. Congress and leaders products during emergencies.
emergency preparedness experts, the at all levels of government should
6. Readying the healthcare system to
report includes recommendations for prioritize investments in health equity,
respond during and recover from
policy action in seven priority areas: incorporate equity leadership into
public health emergencies. Federal
preparedness and response, and
1. P
roviding stable and sufficient and state policymakers and the
invest in social determinants of health.
funding for public health security. healthcare system must prioritize
Congress and state and local 4. Ensuring effective leadership and effective coordination and planning
governments must invest in the coordination. Policymakers should for a surge of patients.
foundations of public health, strengthen public health leadership
7. P
reparing for environmental threats
including public health infrastructure, and communications and reject
and extreme weather. Congress and
workforce, and data systems. attempts to weaken public health
the White House should develop a
authorities. Congress should create a
2. P
reventing disease outbreaks strategic plan, along with funding, to
COVID-19 Commission to review and
and pandemics. Policymakers minimize the health impacts of climate
address gaps in pandemic response.
should support the vaccination change and promote health equity.
infrastructure, fight antibiotic 5. A
ccelerating development
For a full description of the
resistance, and support paid leave and distribution of medical
report’s recommendations, see the
for all workers. countermeasures (MCMs). Congress
recommendations section beginning
should invest in the entire MCM
on page 40.
TFAH • tfah.org 9
Report Purpose and Methodology
TFAH’s annual Ready or Not report series states in benchmarking their performance
tracks states’ readiness for public health against comparable jurisdictions. TFAH
emergencies based on 10 key indicators completed this analysis after consultation
that collectively provide a checklist of top- with a diverse group of subject-matter
priority issues and action items for states experts and practitioners.
and localities to continuously address. By
See Appendix B for more detail on the report’s
gathering timely data on all 50 states and
methodology.
the District of Columbia, the report assists
READY OR NOT AND THE NATIONAL HEALTH SECURITY
PREPAREDNESS INDEX
The indicators included in this report and are meant to be complementary,
were drawn from, and identified in rather than duplicative. With more
partnership with, the National Health than 100 indicators, the NHSPI paints
Security Preparedness Index (NHSPI), 20
a broad picture of national health
with one exception: a measure of state security, allowing users to zoom out
public health funding-level trends, and holistically understand the extent
which reflects how well-resourced key of both individual states and the entire
agencies are to prepare for and respond nation’s preparedness for large-scale
to emergencies. The NHSPI is a joint public health threats. In slight contrast,
initiative of the Robert Wood Johnson Ready or Not, with its focus on 10 select
Foundation, the University of Kentucky, indicators, focuses attention on state
and the University of Colorado. (See performances on a subset of the Index
“Appendix B: Methodology” for a detailed and spotlights important areas for
description of how TFAH selected and stakeholders to prioritize a smaller, more
scored the indicators.) focused set of improvement goals. TFAH
and the NHSPI work together to help
While state rankings in Ready or Not and
federal, state, and local officials use
the NHSPI largely align, there are some
data and findings from each project to
important differences. The two projects
make Americans safer and healthier.
have somewhat different purposes
10 TFAH • tfah.orgSPECIAL SECTION:
Lessons of the Pandemic’s Tragic Death Toll: What Needs to be Done Now to Save
Lives During the Next Public Health Emergency?
The over 900,000 U.S. lives lost due to
the COVID-19 pandemic21 is made even
more tragic by the fact that many of these
deaths were preventable. If the public
health community’s warnings of over a
decade that the country’s public health
infrastructure was dangerously inadequate
had been heeded lives would have been
saved and economic upheaval lessened.
In addition, misinformation, mistrust in
government, and political division have
driven anti-public health and anti-vaccine
policies and actions. Furthermore,
underinvestment in health equity and
social determinants of health contributed
to high rates of chronic disease, leaving
some populations vulnerable to severe
outcomes during the pandemic.
Confusing and disjointed leadership and What went wrong? and reporting processes. Where data
messaging led to disparate responses in were collected, they were spread across
Policymakers did not heed the decades-
every state. And the healthcare system, multiple data sets with no way to quickly
long call by public health experts to
which operates near capacity on many roll up into one national picture.23
fund public health on a sustained
days, was unprepared for multiple surges
basis and not just in response to an
throughout the pandemic. Communities of color were
emergency. Underfunding contributed
disproportionately affected in large
But within this tragedy is opportunity. to understaffed and overworked
part due to the ways in which structural
The pandemic has shined a light health departments using out-of-date
racism and classism impacts where people
on what is needed: Congress and technologies. In addition, lack of support
are born, grow, live, work, and age; the
states must work to create robust and and outright threats against public health
resources available in their community;
sustained investment in public health officials contributed to hundreds of
their access to healthcare; and the
infrastructure, modernization of data senior-level state and local public health
prevalence of chronic disease in their
systems and surveillance capacity, officials leaving the profession.22
communities. According to the Centers
increased public health laboratory for Disease Control and Prevention
The nation’s public health data systems
capacity, sustained growth in a diverse and (CDC), as of November 2021, nationwide
are woefully dated and not up to the
highly skilled public health workforce, American Indians and Alaska Natives
task of tracking an infectious disease
and improved public health messaging died due to COVID-19 at a rate that was
outbreak on the scale of a pandemic.
and communications. However, these 2.2 times higher than whites. Hispanic/
While data collection has improved
investments in public health infrastructure Latino Americans died at a rate that was
as Congress has invested in data
alone will not make America more resilient 2.1 times higher than whites Americans.
modernization, early in the outbreak
in the face of the next public health Black Americans died from COVID-19
basic questions such as how many
emergency. Protecting health in every at a rate that was 1.9 times higher than
people were infected by the virus, which
community will also require addressing the the rates of deaths among whites. Asian
population groups were at the highest
systemic inequities that led to COVID-19’s Americans died at a rate that was 0.9
risk, and where infections were surging
disproportionate health and economic times that of whites.24,25 In addition, as
were largely unanswerable in a timely
impacts, particularly in communities of of mid-November 2021, an estimated
manner due to insufficient testing
color and low-income communities.
TFAH • tfah.org 11167,082 children had lost a parent, by race, it undeniably exposed the
guardian, or caregiver due to COVID- “devastating inequities that come with
19; many of these children were already being a person of color in America.”30
experiencing significant social and Structural racism impacts people of color
economic adversity.26 in nearly every facet of their lives, from
where they live and work to their access
During the early stages of the pandemic
to healthcare. Racism is often at the
(2020) the federal government lacked
root of conditions that drive poor health
an evidence-based leadership role in the
outcomes in communities of color. The
pandemic response, and science and
disproportionate impact of COVID-19—
public health expertise were often not
higher rates of infection, hospitalization,
heeded. In addition, political polarization
and death—in communities of color were
at the federal and state levels confounded
stark illustrations of this fact according
critical public health guidance and
to Dawes and Castrucci. A baseline goal
contributed to a confusing spectrum
in public health must be increasing the
of responses across the country, from
health status (and therefore the strength
some areas issuing mask mandates to
and resilience) of every community. In
other jurisdictions limiting public health
order to improve the health status within
authorities. An October 2020 Columbia
communities of color, long-standing racist
University report concluded that earlier
policies and practices, and their legacies,
implementation of lockdowns, a national
in employment, housing, education,
mask-wearing mandate, and federal
and healthcare must be changed. Dawes
guidance on social distancing could
and Castrucci write that America’s pre-
have saved between 130,00 and 210,000
COVID-19 “normal” “was not equitable
American lives.27 Similarly, Peterson-Kaiser
or just”; therefore, a return to pre-COVID
Family Foundation reported in October
normal would allow the inequities that
2021 that between June and December
fueled the pandemic to persist.
2021, approximately 163,000 U.S. COVID-
19 deaths could have been prevented What’s needed?
through vaccination.28 Increased, flexible, and sustained
Social media platforms were (and still funding. Funding for public health must
are) greenhouses for misinformation be increased, flexible, and sustained
about the virus and vaccines. The Global over time. The pattern of public health
Health Security Index found that, funding in this country has long been that
despite strong health security capacity, money is found (often borrowed from
the United States had the lowest other public health priorities like chronic
possible score on public confidence in disease prevention) to fund needed
the government, a factor that has been response during an emergency. Once
common in countries with higher rates the emergency has passed, governments
of COVID-19 cases and deaths.29 return to a pattern of inadequate levels
of funding for public health. Without
Public health leaders Daniel Dawes, increased, predictable, and sustained
executive director of the Satcher Health funding—for personnel, equipment,
Leadership Institute, and Dr. Brian training, and data systems—the next
Castrucci, president and CEO of the public health emergency response will be
de Beaumont Foundation, wrote in less effective than it needs to be, putting
their February 2021 op-ed in STAT that lives and livelihoods at risk.
while COVID-19 does not discriminate
12 TFAH • tfah.orgIt is also important to note that while time staff to meet the nation’s basic make recommendations to ensure that
the pandemic response and recovery public health needs. According to the such data are comprehensive and create
funding authorized in 2020 and 2021 report, years of budget cuts have reduced a blueprint for health equity. Among
were critical to meet the urgent needs of essential state and local public health the recommendations included in its
the pandemic response, those resources staff by 15 percent over the last decade. October 2021 report was to ensure that
were one-time appropriations. What’s These reductions in the size of the public health measurement captures
needed to protect all Americans from the workforce make local and state health race and ethnicity information at the
next public health emergency is year-in, departments less able to meet community individual level whenever person-
year-out sustained, predictable funding. health needs, including responding to level data is collected, and addresses
emergencies. The report concludes that structural racism and other inequities.36
Editor’s note: In November 2021, the U.S.
the nation needs to hire an additional
House of Representatives passed the $1.75 Also released in October 2021, a report
80,000 full-time public health staff to
trillion Build Back Better Act, including from Grantmakers in Health and
ensure that basic community health
approximately $10 billion for public health— the National Committee for Quality
needs are met in all jurisdictions.34
about $7 billion over five years for public Assurance stated that having more
health infrastructure and about $3 billion for Modernized health data and disease complete data will require action across
other pandemic preparedness.31 These funds, tracking systems, including disaggregated multiple sectors, including changes in
if ultimately appropriated, would be an data collection and reporting. Improved data standards and systems; regulations,
important down payment toward rebuilding response to public health emergencies including a clear and sufficient federal
the nation’s public health system. requires 21st-century data collection and standard for data completeness; and a
management, including real-time data roadmap for collecting and reporting
Federal leadership. In an event as large
on the social determinants of health. on data in ways that will reduce health
and complex as a pandemic, there is no
Achieving health equity is rooted in inequities and provide incentives,
substitute for a strong, coordinated federal
understanding health disparities and requirements, resources, and technical
response. TFAH has made a number
what causes them. Such understanding assistance as needed.37
of policy recommendations designed
begins with a health data systems
to ensure strong federal leadership Editor’s note: Congress has allocated over $1
infrastructure that is able to surveil,
during future public health emergencies, billion through the Coronavirus Aid, Relief,
collect, disaggregate, interpret, and
including the creation of a White House and Economic Security (CARES) Act (P.L.
share data in a timely fashion, including
Health Security Directorate.32 116-136), the America Rescue Plan Act
on race, ethnicity, income, disability,
(P.L. 117-2), and annual appropriations
Editor’s note: The Biden Administration social determinants, other demographic
to support rapid public health data
created a National Security Council factors, and the drivers of health. These
modernization.38 In August 2021, CDC
Directorate on Global Health Security and capacities and these data are often
announced plans to use some of this funding
Biodefense, led by a senior director for global missing from many federal and state
for a new analytics center to better forecast
health security and biodefense, in January data sets that currently provide data
and track disease outbreaks.39
2021.33 Future administrations should on white, Black, and Hispanic people
strengthen this senior-level advisory structure but lack data on other groups, such Modernize public health labs and
at the White House. as American Indians, Alaska Natives, increase their surge capacity. Congress
Asian Americans, and Native Hawaiians must sufficiently fund CDC to support
A diverse and highly skilled public
or other Pacific Islanders, or treat sustained modernization of state and
health workforce. According to an
these groups as one homogeneous local public health laboratories, so
October 2021 report released by the
population.35 they are better connected and ready
de Beaumont Foundation and the
to meet public health threats.40 Also
Public Health National Center for The Robert Wood Johnson Foundation
needed is better coordination between
Innovations, a division of the Public created the National Commission to
public health and private laboratories,
Health Accreditation Board, state and Transform Public Health Data Systems
including clinical and academic settings.
local public health departments need to review how public health data are
Public and private laboratories both
approximately 80 percent more full- collected, shared, and used, as well as toplayed critical roles during the pandemic education, media, medicine, research, emergency, every community needs
response. (See interview: pg. 15.) social media and technology companies, access to healthcare, food, clean water,
and government stakeholders and transportation. Communities
Strengthen public health departments’
can address the issue.41 Distrust of without these resources tend to
emergency response functioning by
government and science was at the have poorer health outcomes at the
providing sufficient funding and
root of at least some vaccine hesitancy. individual and population level and are
requiring plans in order to allow
Addressing this distrust will be critical more vulnerable during an emergency.
for execution of rapid hiring, rapid
to being prepared to respond to future
procurement, and project scale-up and A 2017 report from the National
public health emergencies.
management in response to a public Academies of Sciences, Engineering, and
health emergency. Invest in the social determinants of Medicine stated that “health inequities
health and anti-poverty programs to are in large part a result of poverty,
Combat misinformation and increase
support the public’s health and promote structural racism, and discrimination.”42
the public’s trust in science and
resilience. Key drivers of everyone’s In addition, as illuminated and
government. U.S. Surgeon General
health are the conditions in which exacerbated by COVID-19, structural
Dr. Vivek Murthy has identified health
they are born, grow, live, work, and racism has contributed to a public health
misinformation as a serious threat to
age. These health drivers, also known crisis in the United States—rates of
Americans’ health. In July 2021, the
as “social determinants of health,” in illness are higher and life expectancy
Surgeon General issued an advisory,
large part determine if a population is lower for people of color, including
Confronting Health Misinformation: The
group or community has the resources Black people and American Indian
Surgeon General’s Advisory on Building
and resilience to weather and recover people, than for white people.43
a Healthy Information Environment,
from a public health emergency. In an
including ways in which institutions in
COVID-19 HEALTH EQUITY TASK FORCE REPORT ADDRESSES HEALTH INEQUITIES
The Biden Administration created the 1. Invest in community-led solutions to in modernized public health data
Presidential COVID-19 Health Equity Task address health equity. systems and equity-centered public
Force in January 2021. The October 2021 health data collection, and systems
2. Enforce a data ecosystem that
COVID-19 Health Equity Task Force Report to address the social determinants
promotes equity-driven decision
and proposed implementation plan made of health and increase access to
making.
recommendations to the President for behavioral healthcare.
mitigating the health inequities caused 3. Increase accountability for health
In a statement applauding the report,
or exacerbated by the pandemic and for equity outcomes.
TFAH President and CEO Dr. J. Nadine
preventing such inequities in the future.44
4. Invest in a representative healthcare Gracia, said: “The COVID-19 Health
The task force, chaired by Dr. Marcella
workforce, and increase equitable Equity Task Force has laid out a road
Nunez-Smith, included multisector
access to quality healthcare for all. map for reducing inequities during
experts and people with lived experience
the pandemic and before the next
concerning communities suffering 5. Lead and coordinate implementation
public health emergency. As the report
disproportionate rates of illness and of the COVID-19 Health Equity
acknowledges, we must engage in
death from COVID-19. Task Force’s recommendations
a multisector effort to address the
from a permanent health equity
In its report, the task force made 55 upstream factors that contribute to
infrastructure in the White House.
recommendations to address and underlying health inequities in order
eliminate health disparities, many of which Within those areas, the task force to promote optimal health and build
mirrored TFAH policy recommendations. recommended increased and sustained resilience in all communities.”
Among the report’s five high-level funding for the public health workforce
recommendations to the President were: and emergency response, investment
14 TFAH • tfah.orgThe Critical Role of Public Health Laboratories During
COVID-19 and Beyond
An Interview with Scott Becker, MS, CEO of the Association of
Public Health Laboratories
TFAH: How did public health laboratories year mark for the COVID-19 pandemic,
perform during the pandemic? and during this time public health
laboratories have tested more than 21
Becker: Public health laboratories
million specimens for SARS-CoV-2.
have performed remarkably well
All of APHL’s member public health
despite a number of challenges.
laboratories—that is, most laboratories
Performance issues with the initial
nationwide—are meeting the testing
CDC assay presented significant
demands within their jurisdictions.
hurdles and delays at the beginning of
the pandemic. The laboratories were The emergence of the Omicron variant
resilient, though, quickly notifying created an increase in demand for
CDC and the Association of Public COVID-19 testing for all public health
Health Laboratories (APHL) of assay laboratories. Many of these same
issues and identifying solutions, such as laboratories are also sequencing SARS-
using their own laboratory-developed CoV-2 samples to monitor for Omicron
tests. For instance, Wadsworth Center, and other variants, and they report cases
New York State Department of Health, to CDC for surveillance purposes.
secured an emergency-use authorization
TFAH: What lessons—on lab
for its real-time PCR assay. Other
performance/capacity and beyond—
ongoing challenges included the limited
should the nation learn as a result of
national supply chain for reagents and
the pandemic?
consumables.
Becker: There are significant lessons
Typically, public health laboratories
from this pandemic as well as previous
identify novel threats, perform initial
responses to Zika and Ebola viruses.
testing, and then hand off to the
First, we must look at the coordination,
private sector for high-throughput
or lack thereof, of the U.S. national
surge testing. The state public health
laboratory system and how this limits
laboratory traditionally maintains
our ability to respond to novel threats.
ongoing responsibility for testing in
APHL believes that we need to develop
high-priority or potential outbreak
a national laboratory system that
situations, as well as for regional
better integrates public and private
surveillance. In the case of COVID-19,
laboratories, including large commercial
public health laboratories have been
facilities, hospitals, and academic
in response mode for an extended
institutions. We also need to transform
period, providing sustained surge
the public health laboratory system to
capacity for their jurisdictions and, in
be more agile and interconnected to
some locations, serving as the primary
respond to all threats.
test provider. We are almost at the two-
TFAH • tfah.org 15Another area of concern is the may have instrument capacity, but important than as seen with the COVID-
shrinking public health workforce and we still need to collaborate with the 19 response. These two systems must
lack of diversity within its ranks. A key private sector and other governmental work together to provide timely and
place to address this is by building agencies, beyond CDC, to develop and accurate testing, covering a significant
and supporting a diverse, equitable, pre-position tests in laboratories. We portion of the U.S. population. As is
and inclusive public health laboratory also need to rebuild and strengthen the case with novel infectious threats,
workforce. The fundamental purpose the laboratory workforce as well as the prompt and quality testing is critical
of public health laboratories is to broader public health workforce. as it shapes treatment options and
serve their communities, so it is vital epidemiological actions such as contact
TFAH: What’s the role of public health
that lab staff represent the diverse tracing, and as it influences larger
labs in overall healthcare? Has that
communities in which they are working. public health decisions, including
relationship worked during the COVID-
A representative workforce not only quarantine.
19 pandemic?
creates a better work environment for
TFAH: Are rapid, self-administered
all staff, but it also allows a public health Becker: The quintessential role of
tests, followed by a lab test if positive,
lab to better serve the community’s public health laboratories is to monitor
part of the right approach to ending the
health needs. the diseases and health status of
pandemic?
populations. This role has evolved over
Finally, there are lessons on the use
time, especially given increasing threats Becker: As noted earlier, a multilayered
of various technologies for screening
such as natural disasters, human-caused approach of laboratory testing,
and testing. For instance, point-of-
incidents, emerging and pandemic point-of-care diagnostics, and self-
care diagnostics and at-home testing
infectious diseases, and acts of terrorism. administered (“at-home”) tests is critical
play a pivotal role in reducing the
In executing their 11 core functions, to alleviating the testing burden and
testing burden on laboratories. Such
public health laboratories engage the providing information on community
technologies also ensure access to
entire healthcare community to varying transmission. These tests must be based
testing for underserved communities.
degrees in the state public health in sound science and have performance
Understanding the quality of these
laboratory system. While there were data that support their use. Further,
screening tools and sharing results with
some initial bumps in the response, such tests should also have a reporting
public health agencies will be critical
overall, public health laboratories component, so public health agencies
for surveillance and contact tracing for
worked well with healthcare—including can determine community transmission
future pandemics.
commercial laboratories and other rates and can utilize these data for
TFAH: Does the nation have the needed private institutions including in public health actions.
level of lab capacity for when another nontraditional testing sites, such as
TFAH: New monies within the federal
pandemic happens? prisons and nursing homes.
pandemic recovery packages have
Becker: Responding to a pandemic is Public health and healthcare take been dedicated to lab building and
complex and encompasses the actual different yet equally important renovation. Is it enough?
laboratory test (assay), instruments, approaches to serving and protecting
Becker: The American Rescue Plan Act
supplies (reagents), test results the nation’s health. At the foundation
has provided funding to public health
(electronic laboratory reporting), safe of both approaches is laboratory
laboratories for COVID-19 testing and
and secure facilities, personal protective testing, which is necessary for health
surveillance, for expanding and sustaining
equipment, and trained personnel. departments to monitor disease in
a stronger workforce, for genomic
the population and identify novel
Whether or not we are ready for the sequencing and analytics, for global
threats, and for healthcare providers to
next threat will vary. We often prepare health security beyond just COVID-19, and
make decisions to treat patients. The
for what we have experienced instead for supporting the Data Modernization
interdependency of public- and private-
of preparing for a true unknown. We Initiative and more.
sector testing has never been more
1616 TFAH • tfah.orgWhile this funding is much needed and activities. Within this funding CDC
appreciated, public health laboratories received $500 million to advance
have been chronically underfunded. This surveillance and analytics infrastructure.
is a great boost, especially at a time when In August 2021, CDC announced plans to
they need it most, but these laboratories use some of this funding for a forecasting
need a consistent increase in funding center to better track emerging biological
to be able to keep up with changing threats.
technologies and threats. Federal funding
TFAH: It seems like Omicron
to significantly improve public health data
identification is moving at a faster
management operations at the state and
pace than earlier detection. Is that
local levels of government requires an
accurate? What accounts for the
additional $7.8 billion over the next five
improved performance?
years, and state and local public health
laboratory construction needs are likely to Becker: If you are comparing the pace
be around $5 billion over that same time with the detection of the Alpha variant
frame. (or B.1.1.7), which emerged in December
2020, then yes, the pace is faster. However,
TFAH: How does the overall
the pace with which we’ve detected other
modernizing of the public health data
emerging variants like the Delta variant
systems and the strengthening of lab
has been strong for many months. This is
systems work together?
almost entirely because of the investments
Becker: Like many aspects of public and improvements to genomic-sequencing
health, the effective, efficient movement capability and capacity in the U.S. public
of public health data has been chronically health system. Public health laboratories
underfunded, resulting in a fragmented as well as other key laboratory partners
and obsolete national information are a critical part of the CDC-led National
technology system. This issue has limited SARS-CoV-2 Strain Surveillance (NS3)
the ability of the nation’s public health program. In January 2021, the network
system to make actionable decisions. was publishing between 3,000 and 5,000
The perpetual funding issue, combined sequences to public databases every week.
with a sharp increase in data production Today, the network consistently publishes
from new laboratory techniques, such as between 15,000 and 20,000 specimens per
sequencing, have added great volumes of week. In November 2021 alone, 190,000
data to an already overburdened system. SARS-CoV-2 sequences were published
across the U.S. public health system. This
On the positive side, Congress has
significant increase in capacity positions us
allocated over $1 billion through the
to quickly detect emerging variants, even
Coronavirus Aid, Relief, and Economic
when circulating at low levels.
Security (CARES) Act (P.L. 116-136), the
American Rescue Plan Act (P.L. 117-2), Editor’s note: this interview was conducted in
and annual appropriations to continue December 2021.
public health data modernization
TFAH • tfah.org 17S EC T I ON 1 :
Ready or Not Assessing State Preparedness
SECTION 1: ASSESSING STATE PREPAREDNESS
2022 Every state needs to be prepared to respond to a variety of
potential public health emergencies; such readiness requires
understanding an individual state’s preparedness strengths,
risks, and vulnerabilities. To help states assess readiness, and to
highlight a checklist of top-priority concerns and action areas,
this report examines a set of 10 select indicators. The indicators,
overwhelmingly consistent from year to year, draw heavily on
the National Health Security Preparedness Index (NHSPI), a
joint initiative of the Robert Wood Johnson Foundation, the
University of Kentucky, and the University of Colorado. They
capture core elements of emergency preparedness. Based on
states’ standing across the 10 indicators (see “Appendix B:
Methodology” for scoring details) and TFAH analysis, the states
were placed into three performance tiers: high, middle, and low.
(See Table 3.)
Importantly, the implications of and administrators. Moreover, some
this assessment, and responsibility indicators are under the direct control
for continuously improving, extend of federal and state lawmakers, whereas
beyond any one state or local agency. improvement in other indicators
Such improvement typically requires requires multisector, statewide efforts,
sustained engagement and coordination including by residents.
by a broad range of policymakers
TABLE 3: State Public Health Emergency Preparedness
State performance, by scoring tier, 2021
Performance Number of
States
Tier States
AL, CO, CT, DC, FL, IA, IL, KS, MA, MD, NJ, OH,
High Tier 17 states and DC
PA, SC, UT, VA, VT, WA
AZ, CA, DE, GA, ID, ME, MI, MO, MS, NC, ND,
Middle Tier 20 states
NE, NH, NM, NY, OK, RI, TN, TX, WI
AK, AR, HI, IN, KY, LA, MN, MT, NV, OR, SD,
Low Tier 13 states
WV, WY
MARCH 2022
Note: See “Appendix B: Methodology” for scoring details. Complete data were not available for U.S.
territories.You can also read