Coronavirus: COVID-19 The SENAD Group - COVID-19 Infection Prevention & Control (IPC) framework policy Adults
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
COVID-19 PATHWAY – Adult Care Homes England
Coronavirus: COVID-19
The SENAD Group
COVID-19 Infection Prevention &
Control (IPC) framework policy
Adults
Issue: December 2021
Reviewed: December 2021
Next Review: January 2022
Version: 5
Policy Ref:305.2A
Owner: SK
Section 3/305.2A/V5/DEC21/SK Page 1 of 17COVID-19 PATHWAY – Adult Care Homes England
Overview
This Infection prevention and Control pathway is specific to Adult Care in England.
It reflects current government guidance and provides summaries and links to
enable timely revision of COVID-19 Management plans in an evolving situation.
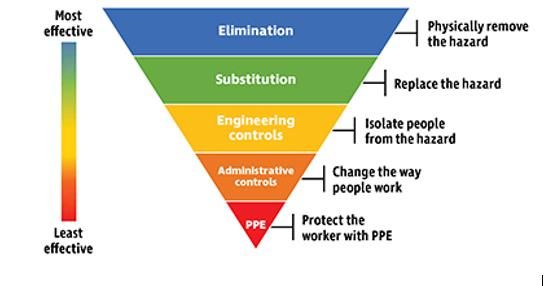
As with previous polices we will still follow the Hierarchy of Controls but in this
instance, they will be tailored to the needs of Adult care.
Controls
Elimination
Early recognition of symptoms and identification of Cases and Isolation
Omicron Variant
The new variant continues to create challenges and the government is changing
guidance as the situation requires it to sometimes more than weekly. It is
therefore important that managers communicate any changes to staff.
Travel
Anyone who enters the UK from abroad must follow the required testing regime
and isolation where required.
Symptoms of Covid 19
Symptoms can be interpreted differently when people have a learning disability or
autism, so whilst it is appropriate to know the main symptoms, it is also useful to
consider other symptoms the person may be displaying - Symptoms of
coronavirus (COVID-19) - NHS (www.nhs.uk)
Main symptoms
• High Temperature- hot to the touch / 37.8°C
• A new continuous cough – for more than 1 hour of 3 or more episodes
in 24 hrs
• A loss or change to send of smell or taste
Section 3/305.2A/V5/DEC21/SK Page 2 of 17COVID-19 PATHWAY – Adult Care Homes England
Other symptoms to consider
(Staff should also keep vigilant for any notifications of changes to
symptoms from different variants).
Residents including older and younger people with a learning disability, and
autistic people may also present with softer signs, including:
• shortness of breath
• if residents are less alert
• if residents have a new onset of confusion
• if residents are off food
• if residents have reduced fluid intake, diarrhoea or vomiting.
Managers and staff should consider COVID-19 as the possible cause of any
worsening in physical or mental ability when there is no other known cause.
Staff Protocols
Staff who have Covid symptoms
If a staff member develops symptoms they should inform their manager, stay at
home or leave work and return home and arrange a PCR test.
PCR positive-
Inform their line manager immediately. Self-isolate from the day the symptoms
started plus 10 full days. They can end their self-isolation period before the end
of the 10 full days by undertaking an LFD test on the 6th day and 7th day of their
isolation period (24 hours apart) if both are negative and return to work on day
8 if:
• They have no symptoms
• Take daily LFD tests on day 8, 9 and 10 prior to work.
• Isolate and wait 24 hours if any are positive before taking the next LFD test
• If the LFD test is positive on the 10th day, daily LFD testing should continue
and the staff member should not return to work until a
negative LFD test result is received.
• They must follow IPC protocols and PPE must be worn properly throughout
the day
• if they work with residents who are especially vulnerable to COVID-19, by risk
assessment consideration given to redeployment for the remainder of
the 10-day isolation period.
If any of these cannot be met they should continue isolation for the full
10 days.
Return to work following isolation following Covid 19 infection-
Staff can return to work provided their symptoms have improved, they have
been not had a fever for 48 hours without the use of medication to control fever,
and are medically fit to return
Negative PCR-
Staff member can return to work if medically fit i.e., considering the symptoms
that may indicate another infectious illness.
Inconclusive PCR-
Section 3/305.2A/V5/DEC21/SK Page 3 of 17COVID-19 PATHWAY – Adult Care Homes England
If the PCR is inconclusive, take another PCR and continue to self-isolate until
isolation period ended.
Positive LFD
Self- isolate and follow the above if the PCR is positive, if the PCR is negative
they can stop self-isolating.
Asymptomatic testing
PCR/ LFD Positive
Self-isolate as above, unless they develop symptoms during their isolation at
that point they will need to start their 10 days again/ or 7 following the above
for someone with symptoms.
• Staff providing care wearing full PPE
If a staff member is providing care to or is in close contact of someone with
Covid and is in the required PPE and it is not breached, they will not be
classed as a contact for tracing and isolation regardless of the vaccination
status of the variant.
• Fully vaccinated staff member other contacts
If identified as a close they should inform their manager. They can continue
working so long as they:
• Don’t have symptoms
• Have no requirements relating to travel
• Return a negative PCR test prior to returning to work
• Do LFD tests every day for the 10 days following their last contact even on
days off and it must be negative to come into work on work days.
• They wear the required PPE and follow IPC protocols and where possible they
are not deployed to work with highly vulnerable residents.
If a staff member has had COVID infection in the past 90 days, they do not do
the PCR but undertake daily LFD antigen tests.
If any of the above cannot be met, the staff member should not come to work
and should follow the stay at home guidance for the full 10-day period.
• Unvaccinated or partially vaccinated staff contacts
If notified they are a contact of a COVID-19 case, by NHS Test and Trace or at
work, they must self-isolate if advised to do so by NHS test and trace unless
they tell them they are exempt (because they are under 18, unable to be
vaccinated due to medical reasons or are taking part or have taken part in a
clinical trial for a COVID-19 vaccine).
Resident Protocols
Any resident who develops symptoms of Covid 19 or test positive should
be isolated.
Hospital Contacts of Covid 19 Discharged from hospital
If inpatients are discharged to care settings, they should be advised to remain
isolated from others for the remainder of their 14-day-exposure window.
Resident Contacts within the Care Home
Section 3/305.2A/V5/DEC21/SK Page 4 of 17COVID-19 PATHWAY – Adult Care Homes England Residents who do not have symptoms who are exposed to a confirmed COVID-19 case should be isolated or cohorted for 14 full days from last exposure to a COVID. This also applies even if they have previously recovered from COVID-19. If they develop symptoms in the 14-day period from exposure, then testing should be performed. If individuals who have been cohorted with other residents subsequently test positive for SARS-CoV-2, then all the residents they have been cohorted with will need to re-start their 14-day-isolation period from the date of their last exposure to newly diagnosed case. Asymptomatic and fully vaccinated residents will not require self-isolation if additional mitigations are in place, they have received a negative PCR test and undertake daily LFD testing during their contact period (up to 10 days). During this period, they should avoid contact with other highly vulnerable residents in the care home, continue to follow all outbreak measures in the event of an outbreak, even where they have tested negative. If they become symptomatic then usual testing and isolation protocols apply until their COVID-19 status is confirmed. 90 Day Rule on re-test Staff and Residents- (Not staff close contacts who still do LFD) Staff, patients and residents (who are not severe immunosuppressed), and who have previously tested positive for COVID by PCR, should be exempt from routine re-testing, by PCR or LFD antigen tests, if within 90 days from their initial illness onset or test date (if asymptomatic), unless they develop new COVID-19 symptoms or are required to take a PCR test upon entry into the UK. If an individual is re-tested by PCR within 90 days from their initial illness onset or prior positive PCR test date and their test is positive, a clinical risk assessment involving the HPA/ IPC lead should be undertaken to identify any possible re-infection risks. Outbreaks An outbreak is defined as 2 or more confirmed or suspected cases amongst people in the same setting with onset of symptoms within 14 days, however you should inform HPT if you have a single possible or confirmed case of Covid19. HPT will risk assess when restrictions can be lifted considering the risks and variants. The length of time a service is in outbreak depends on the variant and risks. The health protection team (HPT) will undertake a risk assessment to determine the safest timeframe, this could mean outbreak controls may be in place for up to 28 days following the last positive case especially as we learn more about real- world vaccine effectiveness and disease severity of the Omicron variant. Safe management of referrals and new admissions Newly admitted residents who are transferring from an interim care facility or another care home. These residents will no longer need to self-isolate upon arrival if they are fully vaccinated and have not been in contact with a case of COVID -19 Before admission the care home has considered the circumstances at the care home or interim care facility from which they are transferring. Section 3/305.2A/V5/DEC21/SK Page 5 of 17
COVID-19 PATHWAY – Adult Care Homes England
They should have a PCR test 72 hours before admission, a PCR test on the day
of admission and a further PCR test 7 days following the day of admission.
Additionally, it is recommended they have daily rapid lateral flow testing until
the day 7 PCR result has been received
New residents admitted from the community
They do not need to self-isolate if they are fully vaccinated (plus 2 weeks) and
have not been on contact with a case of COVID 19 during the previous 14 days
or told to self-isolate.
They should have a PCR test 72 hours before admission, a PCR test on the day
of admission and a further PCR test 7 days following the day of admission.
Additionally, it is recommended they have daily rapid lateral flow testing until
the day 7 PCR result has been received.
Note-If a resident cannot undergo testing, they should be assumed to be
potentially infectious. Their COVID-19 status is unknown, and they
should self-isolate for 14 days as a precaution.
Urgent admissions
For urgent admissions (regardless of symptoms) the individual should be tested
upon arrival and care home managers should follow the 14-day isolation
guidance.
Isolation of asymptomatic residents who have not tested positive
wellbeing-
During their 14-day self-isolation period, those who both are well enough and wish
to should still be supported to leave their room to go outdoors within the
boundaries of the care home’s grounds away from others.
COVID-19 and Refusal of Admission
COVID-19 positive people should only be admitted to a designated setting. Where
it is not possible i.e. it is unsafe for them to be cared for at home until they have
completed isolation, the local authority and NHS trust should agree plan for their
care during their isolation period. No care home should be forced to admit a new
resident to the care home if they cannot safely care for the resident in their
isolation period.
Management of visiting in and out of the Home
Guidance on care home visiting - GOV.UK (www.gov.uk)
Visiting restrictions during an outbreak
• During an outbreak care homes should stop indoor visiting, but should still
offer visits in well-ventilated spaces with substantial screens, pods or behind
windows. These rooms should be left to ventilate between visits wherever
possible if a comfortable temperature can be maintained. By risk assessment
the HPT, outbreak controls may be in place for up to 28 days following
the last positive case especially as we learn more about real-world vaccine
effectiveness and disease severity of the Omicron variant.
Section 3/305.2A/V5/DEC21/SK Page 6 of 17COVID-19 PATHWAY – Adult Care Homes England
Visiting in the care home at other times
• Every care home resident can nominate up to 3 visitors who will be able to
make regular visits not including essential carers or preschool children.
• Visits should be agreed in advance with the care homes and they should not
be time limited if undertaken safely
• They should be in a room most practical and comfortable for the resident.
Homes may have dedicated visitor suites arranged specially for this purpose.
• Visitors should have a negative LFD and report it on the day of their visit,
either by home test or when they arrive at the care home.
• Visitors should wear a face mask when visiting the care home, particularly
when moving through the care home and should be reminded, and provided
facilities, to wash their hands for 20 seconds or use hand sanitiser on
entering and leaving the home.
• Every care home resident should be supported to have an identified essential
care giver to offer companionship or help with care needs who can also visit
during periods of outbreak affecting the care home.
• Essential care givers should take a minimum of 3 lateral flow tests a week
and 1 PCR: one lateral flow test on the same day as a PCR test, one lateral
flow test 2 to 3 days later, and then again after another 2 to 3 days. In line
with care home staff, be subject to additional testing should the care home
be engaged in rapid response daily testing or outbreak testing.
• Physical contact should be enabled with IPC measures such as ventilation,
PPE for the visit, and hand washing before and after holding hands.
• Visitors should not enter the home if they are feeling unwell, even a negative
test and being fully vaccinated plus booster, as other viruses can put
residents at risk. If visitors have any symptoms such as cough, high
temperature, diarrhoea or vomiting, they should avoid the care home until at
least 5 days after they feel better.
• Visitors identified as a close contact who are not legally required to self-
isolate are not to visit for 10 days, unless absolutely necessary, even if fully
vaccinated. Where visits do occur, visitors should have received a
negative PCR test result prior to their visit, and a negative lateral flow test
result earlier in the day of their visit.
• Visiting professionals should be fully vaccinated unless exempt and have a
negative test within 72 hours of visiting.
Visits out of the care home
If a resident with the relevant mental capacity wishes to go out, then in most
cases members of staff at the home cannot lawfully prevent them from doing so.
If a resident lacks capacity, decisions will need to be made in their best interests
in consultation with families, friends and care team as appropriate.
Residents should be supported to undertake visits out of the care home as
appropriate:
• Residents who are fully vaccinated, or are exempt from vaccination,
should not have to isolate following most visits out of the care home but should
undertake lateral flow tests every day for 10 days following the visit.
Section 3/305.2A/V5/DEC21/SK Page 7 of 17COVID-19 PATHWAY – Adult Care Homes England
• Residents who are not fully vaccinated, and are not exempt from
vaccination, should not go out on visits unless isolate for 14 days on return.
• Isolation regardless of vaccination status -All residents should isolate for
14 days following an emergency stay in hospital, or other visits deemed to be
higher risk.
• Planned hospital stays- Residents do not need to isolate upon discharge
provided they are fully vaccinated and had booster if available, complete testing
requirements i.e. negative PCR / LFD and avoid contact with highly vulnerable
residents.
• If a member of care home staff is supporting a resident on an outdoor visit,
managers should assess the COVID risk to the care worker and ensure that the
necessary precautions are in place such as PPE for care etc. Staff supporting
medical visits should have a negative LFD one the day.
• Out of the home residents should avoid mixing with people they don’t normally
meet regularly, avoid large groups, ask those they are visiting to take tests and
have vaccinations.
Serious Illness Support /End of life visits
SENAD understand the need for family contact at this time and the Registered
Manager will review this on a ‘case by case’ basis in line with the underlying
guidance and in close liaison and discussion with the service users family to
ensure their dignity and to provide personalised support.
IPC Protocols for Visiting
Each home will ensure their specific procedures for visits are communicated to
visitors when they book visits and are at least be available to be read by visitors
on arrival. These include handwashing, the appropriate use of PPE and any
restrictions on movement and contact with others. For example, all visitors are
required to wear IIR/ FRSM masks within the home. If a visitor cannot wear a
mask the Registered manager should look at safe alternatives to visiting
Record Keeping
Care homes should keep a temporary record (including contact details) of
current and previous residents, staff and visitors (including the person or people
they interact with), as well as keeping track of visitor numbers and staff.
Vaccination
Staff Vaccination/ Those coming into the care home
Managers will ensure staff follow the company policy on vaccination - 430-COVID
19- COVID 19 Mandatory Vaccination Policy and Working Procedure V1
Aug 21. They should read this policy in full.
All care home staff should be vaccinated, unless they are exempt. i.e. they have
a medical condition that stops them getting the vaccine. The Manager is ultimately
responsible for ensuring that everyone who enters their care home has evidence
of vaccination or exemption. They will decide who can enter in an emergency
situation and ensure appropriate records are kept. The checks can be undertaken
by other staff.
Section 3/305.2A/V5/DEC21/SK Page 8 of 17COVID-19 PATHWAY – Adult Care Homes England
People can enter a care home if:
• They live there i.e. are a resident
• They are fully vaccinated
• They are exempt due to a medical condition
• They are providing help in an emergency. This includes police, fire and
ambulance workers
• They are fixing something that could be a risk to life, or is needed to ensure
continuity of care like a water leak.
• They are a friend, relative or carer to someone who lives in the care home
• They are visiting someone in the care home who is dying
• They are comforting someone whose loved one has died
• You are under the age of 18.
Residents, their families and friends do not need to show they are vaccinated,
however potential residents should be vaccinated if they want to visit the care
home before moving there. If they are not vaccinated, they can look at the home
by video link.
Evidence of vaccination could be for example be:
• The NHS App
• The NHS website –NHS.uk
• The NHS COVID Pass letter (sent via post on request by the individual to
whom it relates, can be requested by calling 119, usually takes around
one week
Staff Vaccination status- On seeing proof of vaccination or exemption, a copy of
the data will be stored securely by the HR team on Isys and on the Staff / Agency
Worker file. It will be shared confidentially with the Registered Manager.
Examples of other people who have to be vaccinated or are exempt if they go
inside a care home include:
• Funeral directors and staff
• Students over 18 come into the home to learn new skills
• Volunteers
• Staff who work outside of the care home – Visiting professionals,
contractors and trades people, head office staff, trainers, hairdressers,
contract cleaners etc
• A person coming for a job interview. They will only be employed once fully
vaccinated
• Postal and delivery workers who want to make a drop-off or collection inside
the home.
Residents & Visitors
It is strongly recommended that residents and visitors receive 2 doses of the
COVID-19 vaccine, plus their booster where applicable.
If eligible, visitors should also get their flu jab when it is offered to them.
Substitution
• It is not possible to substitute anything less harmful for COVID -19
Engineering controls
Ventilation
Section 3/305.2A/V5/DEC21/SK Page 9 of 17COVID-19 PATHWAY – Adult Care Homes England
Maintain well-ventilated communal areas using natural ventilation where safe to
do so such as opening windows to help reduce the risk of spreading Covid 19.
COVID-19 but, actions to improve ventilation should not compromise other
aspects of safety and security (for example, avoid propping open fire doors), and
should consider other consequences such as health and wellbeing impacts from
thermal discomfort.
Ventilation Guidance – Care homes(herefordshireandworcestershireccg.nhs.uk)
Portable fans are however not recommended for use during airborne outbreaks
of infection or when a patient is known or suspected to have an infectious agent
e.g. Clostridium difficile, MRSA, Coronavirus, Norovirus. This will include the use
of fans in communal areas. See link for further information.
Additional facilities for hand hygiene and cough etiquette
• Handwashing
Staff should wash their hands on immediately entry to the care home.
Handwashing should be performed:
➢ before putting on and removing PPE.
➢ before touching a patient
➢ before clean or aseptic procedures
➢ after body fluid exposure risk
➢ after touching a patient
➢ after touching a patient’s immediate surroundings
➢ Staff should be ‘Bare Below the Elbows’
➢ Liquid soap and paper towels dispensed from wall units should be
available
Alcohol Based Hand Rubs should be available for hand hygiene in any setting.
Personal dispensers may be preferable in learning disability and mental health
homes for safety.
• Respiratory and cough hygiene
A sufficient number of tissues, and waste bins (lined and foot operated) should
be available for staff, residents and visitors to use.
Testing
The government has produced a guide to testing in care homes see full content:
Coronavirus (COVID-19) testing for adult social care settings - GOV.UK
(www.gov.uk)
Section 3/305.2A/V5/DEC21/SK Page 10 of 17COVID-19 PATHWAY – Adult Care Homes England
Asymptomatic testing staff:
• Weekly PCR, same day each week
• 3 LFT’s- 1 on day of PCR, then one every 2 to 3 days
• LFD Immediately before their shift, if working in multiple locations, and have
worked somewhere else since their last shift in the home.
• LFD before work when after leave and missed weekly PCR.
Asymptomatic testing residents:
You should test all residents:
• Monthly PCR
PCR If they are new
NB- Test immediately if they develop symptoms, with a PCR. Do not wait for the
next test in the regular testing pattern.
Further testing may be required for visits in and out of the care home,
on admission or if the resident is exposed to COVID-19.
Rapid Testing staff- One or more positive LFD/PCR
In addition to the table below
• Contact your local health protection team (HPT) for advice
• Don’t bring staff in on their days off, it’s only those working
If any further positives, see Outbreak testing and follow guidance of HPT.
Section 3/305.2A/V5/DEC21/SK Page 11 of 17COVID-19 PATHWAY – Adult Care Homes England
Outbreak Testing- 2, or more, positive or clinically suspected cases of COVID-
19 during a 14-day period.
Cleaning and decontamination
• Safe Environment
➢ The environment must be visibly clean and free from non-essential items
and equipment to facilitate effective cleaning.
➢ Staff groups should be aware of their environmental cleaning schedules for
their area and clear on their specific responsibilities.
➢ The frequency of cleaning should be increased during the pandemic to at
least twice daily.
➢ Frequently touched sites or points should be cleaned between individual
use.
➢ Domestic staff should be advised to do a terminal clean of isolation room(s)
after all other unaffected areas of the facility have been cleaned. Ideally,
isolation room cleaning should be undertaken by staff who are also
providing care in the isolation room.
o In low risk environments-
➢ Staff should decontaminate all re-usable non-invasive equipment between
every resident using approved detergents / disinfectant agents (unless
contaminated with blood or body fluids).
Routine_decontamination_of_reusable_noninvasive_equipment.pdf
(publishing.service.gov.uk)
➢ Patient care equipment should be single use where possible.
➢ Reusable non-invasive equipment should be allocated to the individual
patient or cohort of patients or decontaminated between patients.
➢ Cleaning protocols should include responsibility for, frequency of, and
method of environmental decontamination.
In higher risk environments
➢ Decontamination of the environment must be performed using a combined
detergent or disinfectant solution at a dilution of 1,000 parts per million
available chlorine.
➢ Alternative cleaning agents or disinfectant products may be used with
agreement of the local Infection Prevention and Control Lead.
➢ Staff performing environmental decontamination (cleaning) should be
allocated to specific area(s) and not be moved between COVID-19 and
non- COVID-19 areas and be trained in which PPE to use and the correct
methods of putting on and removing PPE
Section 3/305.2A/V5/DEC21/SK Page 12 of 17COVID-19 PATHWAY – Adult Care Homes England
➢ Dedicated or disposable equipment (such as mop heads, cloths) must be
used for environmental decontamination.
➢ Reusable equipment (such as mop handles, buckets) must be
decontaminated after use with a chlorine-based disinfectant
➢ As above for decontamination of environment and re-usable equipment.
Equipment should be cleaned in line with manufacturers’ guidance.
Waste handling
Waste generated from people with symptoms of (or who have tested positive
for) COVID-19, and are still in isolation, needs to be managed carefully.
➢ For care homes that have an offensive (tiger stripe) waste
stream- PPE and waste from personal care should be placed in a tiger
striped (offensive) waste bag and be disposed of as healthcare waste (for
example, an external lockable yellow wheelie bin) for collection by a
hygiene waste collection company. However, this waste will need to be
stored within the wheelie bin for 72 hours before it can be
collected.
➢ Nursing and Care homes may have the orange clinical or infectious
waste stream- Waste can be placed directly into specialist waste bins
provided by your waste management company as normal. Storing for 72
hours is not required.
➢ Care homes that don’t have an offensive (tiger stripe) or orange
clinical or infectious waste stream- Waste from residents with
symptoms of (or who have tested positive for) COVID-19, waste from
cleaning of areas where they have been (including disposable cloths and
used tissues), and PPE waste from their care should be managed as
follows:
put in a plastic rubbish bag and tie when three-quarters full and place the
plastic bag in a second rubbish bag (for example, a black domestic bin
liner) and tie it then put these bags in a suitable and secure place and
mark for disposal 72 hours later
Waste should be stored safely and securely, for at least 72 hours,
keeping it away from vulnerable persons and children. They must not be
left in in communal areas such as bathrooms, toilets, corridors, stairwells
or living areas. Ideally, a locked outdoor space would be best. After the 72
hours, the waste can be put into the normal domestic waste.
Do not put any items of PPE (or face coverings of any kind) in the
recycling bin.
Linen /Laundry Handling
➢ Wear PPE as required
➢ Wash items as appropriate in accordance with the manufacturer’s
instructions.
➢ Dispose of items that are heavily soiled with body fluids, such as vomit or
diarrhoea, or items that cannot be washed, with the owner’s consent.
Section 3/305.2A/V5/DEC21/SK Page 13 of 17COVID-19 PATHWAY – Adult Care Homes England
➢ Do not place dirty laundry on the floor or other surfaces to prevent
contamination.
➢ Shake dirty laundry before washing to minimise the possibility of dispersing
virus through the air.
➢ Staff uniforms and clothing should be protected from contamination by PPE.
For staff taking uniform home for laundering, use a plastic bag.
Environmental safety
Staff should ensure that the environment remains safe during the COVID-19
Pandemic and not forget other risks within the home to vulnerable people.
Controlling one risk must not present another.
➢ Risk assessments should be in place for the safe storage, handling use and
disposal of cleaning products considering the safety of residents. This
includes the risk of ingestion from alcohol hand gels.
➢ Open windows and doors to improve ventilation must not increase the risk
of fall from height or the spread of fire.
➢ Extra deliveries of PPE/ materials must not obstruct evacuation routes and
should be stored safely.
Administrative Controls
Communication
All cases of COVID-19 will be reported using the Notify email inbox-
notify@senadgroup.com
This will inform senior managers and the Quality Team who can provide
additional support if needed.
RIDDOR reporting is only for staff and not service users who are infected with
COVID 19 at work or if there is a dangerous occurrence involving COVID-19.
Services should discuss individual cases with the Group Health and safety
Manager before submitting a RIDDOR. RIDDOR reporting of COVID-19
(hse.gov.uk)
During any outbreak appropriate communications should be in place for staff,
families and healthcare professionals to ensure the best outcomes and earliest
resolution.
Monitoring and reviewing control measures
Managers should ensure that all controls remain effective by carrying out:
➢ Observations of the safe and appropriate use of PPE
➢ Ensuring testing regimes are being adhered to
➢ Undertaking walk arounds of the environment to ensure standards are
met
➢ Listening and acting upon the concerns of residents and staff
➢ Checking cleaning schedules and ensuring appropriate resources are in
place
Section 3/305.2A/V5/DEC21/SK Page 14 of 17COVID-19 PATHWAY – Adult Care Homes England
➢ Reviewing all controls in the event of a case of COVID-19 within the home
Appropriate risk management.
• General and person-centred risk management
➢ The care home should have a COVID-19 risk assessment in place identifying
all potential hazards and controls needed to prevent or control the risks
from COVID -19.
➢ There should be a risk assessment to manage on-site visiting specific to the
home which includes the cleaning and decontamination of areas used by
different residents for example pods or visiting rooms after each visit.
➢ Each resident should have risk assessments in place for their visiting
arrangements and needs. This includes offsite visits to medical
appointments.
➢ Staff should have specific risk assessments in place if they are extremely /
clinically vulnerable/ pregnant where needed.
➢ Dynamic risk assessments should be in place during a COVID-19 outbreak
to manage the outbreak on a day to day basis until it ends. This should be
reviewed during any outbreak investigation to prevent a recurrence.
Training and competence
Staff will undergo:
➢ Infection prevention and control training as part of their induction and this
will be refreshed as required.
➢ All staff should have donning and doffing training where required for their
role
➢ Staff should be given information, instruction and training on the risks and
controls within their service for the prevention and control of COVID-19
Safe Staffing
Care managers will ensure safe staffing levels at all times considering the need to
prevent the movement of staff where possible between services. However, it is
accepted that in exceptional circumstances this may be unavoidable in order to
meet the needs of people using the service and keep them safe at all times.
Restricting workforce movement between care homes and other care settings -
GOV.UK (www.gov.uk)
If any manager has concerns about staffing they should contact their line
managers for support.
Business continuity and contingency planning
The business continuity plan for all services should include the steps needed to
take during an outbreak of COVID-19 in the home and the contact details of
relevant agencies and support.
Posters and visual aids- to laminate
Section 3/305.2A/V5/DEC21/SK Page 15 of 17COVID-19 PATHWAY – Adult Care Homes England
➢ Cough hygiene- catch-bin-kill.pdf (england.nhs.uk)
➢ Hand washing turn tap- handwashing-poster-landscape-and-portrait.pdf
(westsussex.gov.uk)
➢ Hand Hygiene elbow tap- PHE handwashing advice
(publishing.service.gov.uk)
➢ Alcohol hand gel- 82385-PanFlu-GelWash-A4 (sthelensccg.nhs.uk)
PPE- Personal protective equipment
All PPE should be:
• located close to the point of use
• well fitting
• stored to prevent contamination in a clean, dry area
• within expiry date
• single use and disposable, unless specified by the manufacturer that it is
reusable (eye protection)
• changed immediately after each patient and/or completing a procedure or
task
• discarded if damaged or contaminated
• disposed of after use into the correct waste stream
• safely doffed (removed) to avoid self-contamination
• Standard PPE
➢ Donning Non-AGP Poster- How to work safely - Putting on personal
protective equipment (PPE) (publishing.service.gov.uk)
➢ Doffing Non-AGP poster - How to work safely – Taking off personal
protective equipment (PPE) (publishing.service.gov.uk)
➢ Donning and doffing video – No AGP- COVID-19: putting on and removing
PPE – a guide for care homes (video) - GOV.UK (www.gov.uk)
• Aerosol Generating procedures (AGP’s)
If staff are required to support service users with AGPs the PPE that needs to
be worn is different. AGPs are procedures are tasks such as supporting a
resident on a CPAP or Bi PAP machine, tracheostomy suction and other
procedures that can generate aerosols. If staff need to support residents with
this which you will be given specialist training on if required.
PPE for AGPs will be taught 1-1- staff must be fit tested for FFP3 respirators or
be trained in the use of specialist hoods. The donning and doffing training will
be done on the same day and an observation will be undertaken to ensure safe
practice.
Donning & Doffing AGP and video - COVID-19: personal protective equipment
use for aerosol generating procedures - GOV.UK (www.gov.uk)
Section 3/305.2A/V5/DEC21/SK Page 16 of 17COVID-19 PATHWAY – Adult Care Homes England
See table below for PPE selection and use. Personal Protective Equipment (Protect people with PPE)
Fit tested
Disposable
FFP3 /
IIR as standard
Scenario Gloves Apron Eye Protection Powered- Gown
at SENAD
Air-
Purifying-
Hood
within 2 metres of a resident
and carrying out direct
personal care to someone who Yes Yes Yes Yes
is COVID-19 positive or who is
isolating
within 2 metres of a resident
and carrying out direct
personal care (for example,
physical care) where there is a Yes Yes Yes Yes
risk of contact with respiratory
symptoms or body fluids i.e.
coughing or sneezing
Within 2 metres of a resident
Yes - can be left
who has no symptoms and a
on when task is
negative test for COVID-19, Yes Yes
completed unless
and carrying out direct
contaminated
personal care
Not unless there is a risk of contact
When within 2 metres of an with body fluids, risk of contact from
individual but not carrying out residents who may be coughing, Yes
direct personal care sneezing or spitting or a risk of
splashing from cleaning products
More than 2 metres from a Not unless you are carrying out
No - (unless
resident undertaking domestic domestic type duties within a
there is a risk No - (unless there is a
duties or other activities and resident’s room where the resident
of contact with risk of contact with body
not delivering personal care- has had a positive COVID-19 test Yes
body fluids or fluids or contamination
see conditions which may within 14 days and is isolating, or has
contaminated of clothing)
mean items of PPE are respiratory symptoms or is unable to
waste)
required maintain a safe distance
Aerosol Generating Procedures
Yes Yes- if disposable FFP3 and not Hood Yes Yes
Section 3/305.2A/V5/DEC21/SK Page 17 of 17You can also read