Escalation plan for oxygen usage (Covid 19) - West Suffolk ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
.
Escalation plan for oxygen usage
(Covid 19)
TO DELIVER THE BEST QUALITY AND SAFEST CARE FOR OUR
COMMUNITY
Version 1 01/04/2020
Version 2 25/01/2021
Created By: Samantha Crouch, Service Manager
Julie Head, Head of Deteriorating Patient
Contributions by: Ian Stuchbury, Estates Manager, Estates and
Facilities.
Vijay Gopal, Consultant Anaesthetist
Jas Sidana, Consultant Anaesthetist
Mark Manning, Interim Head of Nursing,
Medicine.
Lou Boehmer, Assistant Service Manager
Page 1 of 12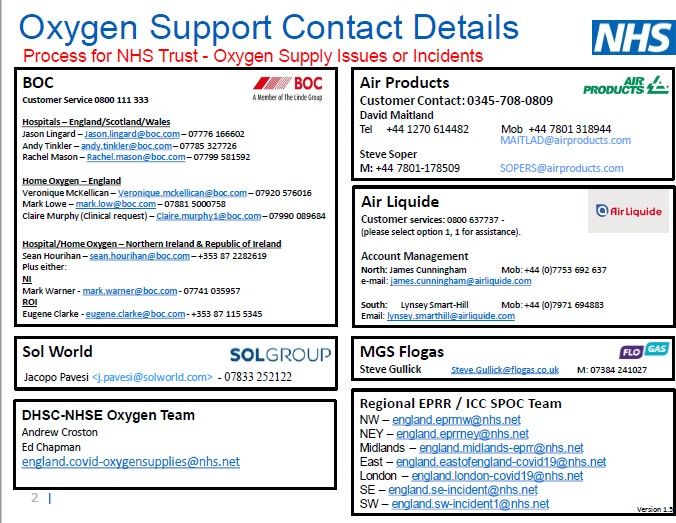
Contents
Section 1 - Introduction
Section 2 – Monitoring of oxygen usage and supply
Section 3 – Good clinical housekeeping
Section 4 –Key actions at escalation points
Section 5 – Low pressure alarms
Section 6 –Fire/health and safety
Section 7-Special consideration-ward F2
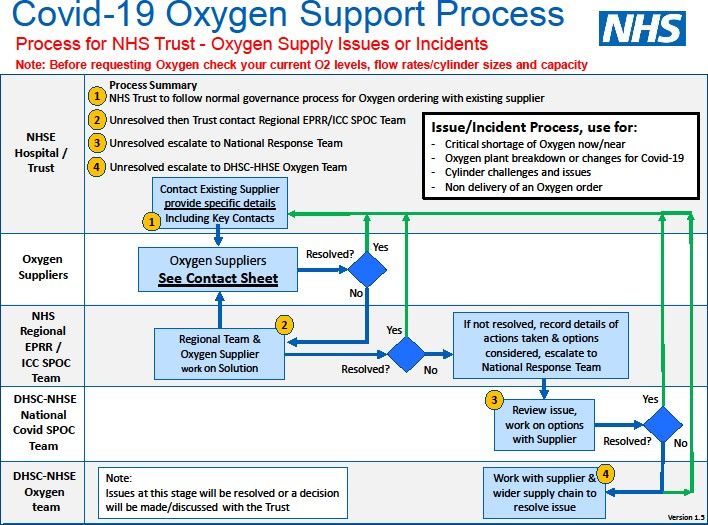
Appendix 1-Covid-19 Oxygen support Process
Appendix 2-Covid-19 worklist on e-Care
Appendix 3-Specialty guide oxygen and Corona Virus
Appendix 4-Oxygen Escalation Plan-summary
Page 2 of 12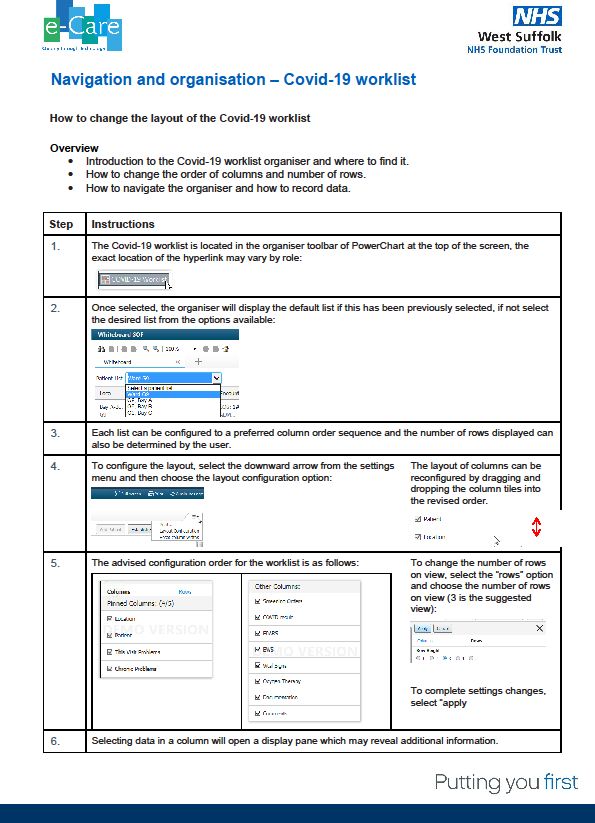
SECTION 1 - INTRODUCTION
1.1 Policy Statement
This document sets out the Trust policy to be followed in relation to the safe management of oxygen across
the West Suffolk Hospital site during a period where higher than usual usage can be expected.
Rationale
The continuing Covid-19 pandemic may lead to increases in the use of ward oxygen due to the
respiratory profile that has been observed in symptomatic patients. The use of Non-invasive Ventilation
(NIV) in the form of Continuous Positive Airway Pressure (CPAP) and increased invasive ventilation
utilising conventional Intensive Care Unit (ICU) ventilators as well as other ventilation provision using
anaesthetic machines and transport ventilators may be necessary in order to respond to demand.
The maximum oxygen (O2) output of our vacuum insulated evaporator (VIE) is 2,750L/min. A sudden
increase in the use of oxygen may lead to a failure of oxygen delivery and a low pressure in the oxygen
supply framework. If unmanaged this has the potential to cause malfunction of ventilators and other
oxygen delivery devices with catastrophic clinical consequences for patients who are oxygen and pressure
support dependent.
Therefore, it is essential that we ensure both judicious use and careful monitoring of oxygen used across
the site.
1.2 Key Principles
• The safe management of oxygen including monitoring of oxygen usage and escalation process
where levels are nearing or exceeding target gas flow rate.
• Good clinical housekeeping for patients requiring oxygen therapy.
SECTION 2 – Monitoring oxygen usage and supply
2.1 Piped oxygen
A regular report is produced by the estates manager or a deputy who documents the oxygen usage within the
preceding 24 hours, tank capacity and next expected delivery. The report is sent to Tactical and key stakeholders.
This will move to daily reporting in the event that levels reach 1,500L/min.
Page 3 of 12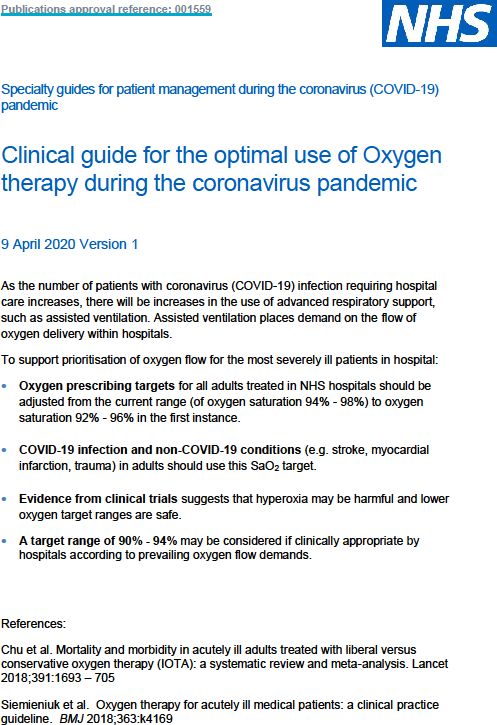
The liquid oxygen tank supplying the site is refilled by BOC when the tank level falls to 30%. BOC are remotely
monitoring the tank levels and automatically arrange deliveries. Estates are also monitoring the tank levels and
regularly de-icing the VIE oxygen plant to maintain supply to the site. Estates manager or deputy will escalate any
issues around supply as shown in appendix 1.
Primary Oxygen Tank Actions to be taken when levels reach 1,500 L/min (green), 2, 000L/min (amber) ,
2, 500 L/min (red) and 2, 750 L/min (black) are described in section 4 and summarised in appendix 4.
Standby Secondary Tank-. Estates will immediately advise the tactical office if the Primary oxygen
tank goes off line and the site is running on standby secondary vessel. In the event that the second
vessel is in use the levels at which actions apply will differ from the primary tank as the vessel is
smaller. When the second vessel is in use levels would be 900 L/min (green), 900-1,200 L/min
(amber), 1, 200L/min-1, 500L/min (red) and 1, 500-1, 700L/min (black). Actions to be taken are as
described in section 4 and summarised in appendix 4.
2.2 Cylinders
A daily report is produced by the portering department documenting oxygen cylinder holdings across the
site. BOC supply cylinders on a one for one basis, taking one empty cylinder and replacing with a full one.
Therefore, careful management of the cylinders in clinical areas particularly in regards to ensuring empty
cylinders are placed in agreed collection points is essential. Porters under the direction of the estates
manager will manage this process. BOC support the supply of cylinders including the ability to draft army
support if extra drivers are needed. Any concerns around supply will be actioned by the estates manager or
a deputy following the process described in appendix 1.
Please note the oxygen cylinder on the emergency trolley in clinical areas must only be used in emergency
situations (2222 call).
2.3 Flex-oxygen flow metres
Oxygen flow metres have been installed to key wards/units to monitor the oxygen demand in litres per minute
(L/min) they are located in the following areas:-
●ITU
● AAU
Page 4 of 12●F7
● G9
The readings from these metres are recorded within the regular report produced by the estate’s
manager or a deputy.
Limits to be observed by ward/unit staff would be the following:
ITU-500L/MIN
F7-200L/min
G9-250L/MIN
AAU-250 L/min
If the levels are met or exceeded the immediate action will be to: -
● Check the local medical gas alarm panel to see if any alarms are sounding, in particular ‘low pressure’ alarms
● Inform the clinicians about the high volume of oxygen being drawn through the system and get them to review their
patients on oxygen.
● Inform estates of any medical gas alarms or high readings on or above the sated levels.
●Inform Tactical of the high flow rate so decisions can start to be made on the admission of new patients or relocation
of existing patients as needed.
2.4 Oxygen management group
A dedicated and multi-professional group of clinicians, operational staff and estates staff working together to
maintain the safe supply of oxygen within the limitations of our infrastructure. The group will meet routinely monthly
and the frequency of meetings can increase as needed according to prevailing circumstances.
Additionally, the Medical Gas committee has responsibility for the safe delivery of all medical gasses from the plant to
patient bedside.
SECTION 3 - Good clinical housekeeping
Daily actions
3.1 Wards
1. Revised O2 targets for patients: 92-96% (88-92% for COPD/OSA/other chronic respiratory diseases).
Please see appendix 3.
2. Daily review of O2 targets by clinicians on the ward. Use of covid19 worklist for clinicians (appendix 2)
Page 5 of 123. Check oxygen delivery device/positioning/kinking etc.
4. Medical/nursing handovers should highlight if any patients are on high flow O2 or 15L o2.
5. HFNO (AIRVO) oxygenation is available however this uses a very high amount of oxygen and should be used
sparingly and initiated only by on call specialist registrar, consultant and outreach nurse. No more than two
should be used on ward F7 without discussion and consideration of oxygen supply.
6. Location of emergency O2 cylinders on each ward should be known to facilitate transfer and emergency
usage.
7. Doctors to review patients on oxygen routinely during ward rounds.
3.2 ICU and theatres
ITU- as all patients in ITU are monitored closely, reduce oxygen to 88-92%
Theatres-peri-op Spo2 target 94-96%
Theatres-Turn off flow meters after machine check and before transfer to recovery
Theatres-Switch off the oxygen in recovery if target saturations are achieved.
Page 6 of 12SECTION 4 – Key actions at escalation points
4.1. Green 1,500 L/min for primary vessel.
If secondary back up vessel is in use 900L/min
Clinical action-Ensure daily actions described in section 3 are taking place.
Clinical action-Ensure clinical staff are using CV19 worklist. Guide to accessing this is contained in
appendix 2.
Clinical action-Nursing and medical handovers to review o2 usage and necessity
Clinical action-Critical Care Outreach to be informed if patients are requiring 5L o2 or above.
4.2 Amber 2, 000 L/min
If secondary back up vessel in use 900-1, 200 L/min
As for green and additionally;
Clinical action-Four hourly medical reviews of all patients on o2 therapy.
Clinical action-Ward staff to establish the oxygen requirement for the clinical area in case
situation moves to red.
Estates action-reporting of piped oxygen levels to be increased to 12 hourly rather than daily.
Estates action-Porters to identify locations and stock levels of oxygen cylinders and prepare to
distribute additional cylinders to areas if situation deteriorates to red.
Red 2, 500L/min
If secondary back up vessel in use 1, 200-1, 500 L/min
The immediate requirement is to reduce oxygen use across the hospital.
Page 7 of 12Immediate tactical action to mobilise medical, nursing and operational staff to enact the actions described
below, to include;
Medical registrar medic bleep 434, ITU doctors medic bleep 759, Critical outreach 666, charge
hand porters medic bleep 959, estates manager or deputy in hours or engineer on call out of
hours.
Estates/porters action-consider emergency order of oxygen cylinders. Distribution of additional
cylinders to areas as needed.
Clinical action (wards)-Consideration of lower saturations targets.
Clinical action (wards)-Conversion of patients on lower level oxygen (4L or less) to cylinder use.
Tactical action-Consideration of action required to ensure continued patient safety; diversion of
incoming patients, transfer of patients to other sites.
4.3 Black 2, 7500 L/min
If secondary back up vessel in use 1, 500-1, 700 L/min
Tactical action with strategic discussion to consider if the declaration of a major incident is
warranted.
As for red including tactical action-consideration of action required to ensure continued patient
safety; diversion of incoming patients, transfer of patients to other sites. Oxygen plant is now
at a critical level with a heightened chance of plant failure. In addition;
Clinical action-Consideration to reduce O2 for any patients on O2 therapy.
Clinical action- to conserve o2 for ventilated patients.
Clinical action-Consideration to swap additional patients to cylinder o2 supply.
SECTION 5 – Low pressure medical gas alarms
5.1 Each ward/area using piped oxygen must know where the nearest oxygen pressure alarm is and how to
respond to this alarm. In hours, contact estates helpdesk on 5555 stating that the medical gas alarm has
activated and an urgent response is required. Out of hours, contact engineer on call via switchboard.
Key actions on hearing the alarm are as per red escalation. In addition;
Clinical action (wards)-Consideration to reduce O2 by 2-4 L/min immediately. Only to be
Page 8 of 12increased if saturation s 85% (assuming this is acceptable to consultant intensivist).
Reference: Oxygen protection: East Of England Critical Care Network
SECTION 6- Fire/health and safety
Higher than normal oxygen usage is a potential fire risk particularly in areas with no mechanical ventilation
General precautions in potentially O2 rich environments
After using alcohol-based hand sanitiser staff should allow alcohol to evaporate, at a safe distance away,
before contact with oxygen generating equipment, patients on oxygen or electrical equipment. Ignition
of alcohol-based hand sanitisers in oxygen enriched environments can lead to serious fires.
Reference ECRI. Fire risk from alcohol-based hand sanitisers worsens in oxygen-enriched environments
Health Devices 2006. Oct 35 (10): 390
The following is taken from Fire Safety Protocol FSP13 Medical Gases Emergency Isolation in Event Of Fire
Link to this policy is to be found at http://staff.wsha.local/Intranet/Documents/E-
M/Estatesandfacilities/Firesafety.aspx
• Where there is no mechanical ventilation system, windows must be kept open on wards and in side
rooms to provide natural air flow and to safely dilute the oxygen level
• Do not use oil-based emollients or alcohol-based sanitiser on patients who are on oxygen or on
yourself if you are close to them. All skin protectants and any emollients with white soft paraffin
are flammable and must not contaminate oxygen equipment/valves.
• Know the location of oxygen isolation points; Area Valve Service Units (AVSU) and the area served
(number and location of patients) eg. Ward F2 (seven patients). These are normally be located
adjacent to Ward/Department entrance or nurse station and will indicate type of gas affected
• Know the location of medical gas indicator panels
Medical gas indicator panel alarm
In case of medical indicator panel alarm contact estates in hours on 5555 or out of hours contact the senior
engineer on call via switchboard.
Isolation of supply in case of fire or leak
Page 9 of 12As a prescribed drug, any decision to isolate a medical gas supply must be made and carried out by
clinical staff;
• Initially at the bed head piped supply outlet, or at a cylinder valve,
• If it is not possible to isolate the supply at the outlet, then isolate the piped supply to the whole ward /
department at the AVSU.
o Identify the gas supply and number of patients affected
o Ensure that any patients are placed on alternative supplies,
o Break Glass and turn valve 90 Degrees to ‘closed’ position.
o Inform Estates AND Authorised Person (MGPS) immediately to reinstate medical gas
supplies.
Oxygen Level Monitors
Areas where there is a high oxygen usage and no mechanical ventilation will require monitoring devices to measure
oxygen levels in the environment. This is to ensure the oxygen level is maintained below 23.5% in air. Oxygen
(enrichment) above this level is a fire hazard. WSFT have purchased a number of portable oxygen monitors for use
in individual ward/bays/side rooms with high oxygen usage. This will go in to alarm mode if the oxygen level gets too
high. If the alarm activates:
● Immediately open any windows to increase natural ventilation
● Clinicians to review the patients use of oxygen to look to reduce
● Inform estates in hours or estates senior engineer on-call for out of hours of the alarm activation
Please see Fire Safety Protocol FSP22 Oxygen Gas Monitoring Procedure for further information regarding these
devices. Link to this policy is to be found at
http://staff.wsha.local/Intranet/Documents/E-M/Estatesandfacilities/Firesafety.aspx
SECTION 7-Special consideration-ward F2
The maximum oxygen usage in F2 should be 70L/min. If a need to increase this level is identified some
patients would need to be moved to other areas i.e. recovery. There is potential for this area to become an
oxygen rich environment. Levels of oxygen in the air will be monitored using an oxygen level monitor. The
general precautions regarding an oxygen rich environment are contained in section 6.
Page 10 of 12Appendix 1
Appendix 1
Please note the supplier for West Suffolk Hospitals Trust (including Newmarket) is BOC
Page 11 of 12Appendix 2
Page 12 of 12Appendix 3
Page 13 of 12Appendix 4
OXYGEN ESCALATION PLAN
1,500 LPM Clinical – Daily good clinical housekeeping. Use
COVID19 worklist.
GREEN
(900l/min if second vessel in use)
Nursing and medical review of o2 usage at
handover
2,000 LPM
Clinical – Actions as per GREEN status plus:
4 hourly medical reviews of patients on o2.
AMBER
Ward staff to establish o2 requirement for area.
(900 – 1,200 LPM if second vessel in use)
2,500 LPM Immediate tactical actions to mobilise key staff.
Red or Low Consider urgent actions needed to ensure
(1,200 – 1,500
RED
Pressure Alarm LPM if second continued patient safety.
Sounded vessel in use) Urgent clinical action required to reduce oxygen
usage across the hospital.
2,700 LPM
Actions as per RED status including immediate
Oxygen Plant
tactical actions plus:
Critical – Risk (1,500 – 1,700
BLACK
LPM if second Further clinical actions to reduce o2 usage.
of Plant Failure
vessel in use)
At all stages staff to be aware of location of emergency/transfer o2 cylinders
Page 14 of 12You can also read