Intravitreal triamcinolone and laser photocoagulation for retinal angiomatous proliferation
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Downloaded from bjo.bmj.com on April 24, 2013 - Published by group.bmj.com
1357
SCIENTIFIC REPORT
Intravitreal triamcinolone and laser
photocoagulation for retinal angiomatous
proliferation
T R Krieglstein, A Kampik, M Ulbig
...............................................................................................................................
Br J Ophthalmol 2006;90:1357–1360. doi: 10.1136/bjo.2006.092536
Stage II is classified as the extending of intraretinal
Background: Recently, the entity of retinal angiomatous
neovascularisation beyond the photoreceptor layer into the
proliferation (RAP) as a subtype of exudative age-related subretinal space, and is called subretinal neovascularisation.
macular degeneration was described, but no treatment It may be combined with a pigment epithelium detachment
options have been established as yet. The only two (PED). Stage III includes choroidal neovascularisation as well
therapeutic modalities being discussed are surgical lysis of as retinal choroidal anastomosis (RCA).
the feeding arteriole and draining venule, and the use of Since then, few studies have evaluated therapeutic options
photodynamic therapy combined with intravitreal triamcino- for this new subtype of ARMD, and as yet there is no effective
lone injection. treatment. Surgical ablation of RAP has been described in a
Aim: To examine focal laser treatment of early extrafoveal small number of patients with RAP stage II associated with
intraretinal neovascularisation of RAP. serous PED,2 and it has been shown that visual acuity
Methods: Prospective case series. We included 13 consecu- improved and macular thickening resolved. Other reports
tive patients with an extrafoveal RAP stage I lesion. All showed benefit from combined photodynamic therapy (PDT)
patients underwent a complete ophthalmic examination, with intravitreal triamcinolone in single cases.3 4 With regard
including fluorescein angiography and optical coherence to the late stages of RAP such as choroidal neovascularisa-
tomography (OCT) III before treatment and at 2 weeks, 1, 2 tion, RCA and associated PED, the unique conviction in the
and 4 months afterwards. In cases with marked macular literature is a high risk for pigment epithelium tears caused
oedema (.350 mm retinal thickening in OCT III, r = 12), by PDT.5 The effects of triamcinolone injection are limited
intravitreal injection of 4 mg triamcinolone was given before and temporary. Recently, combined surgical ablation and
focal laser treatment to reduce the oedema. intravitreal triamcinolone for RAP stage III has been
Results: This case series indicates anatomical improvement reported.6 This treatment was safe and anatomically effective,
but recurrence after surgical ablation has been described by
or stabilisation in patients with an extrafoveal RAP lesion
another author.7
after treatment. Initial visual acuity ranged from 0.1 to 0.6 on
A literature search showed no studies evaluating treatment
the Snellen chart. By calculating logarithmic values, visual
options for RAP stage I.
acuity was seen to be improved in five cases (2 to 5 log lines),
The purpose of this study was to determine the effects of
deteriorated in four cases (22 to 5 log lines) and stabilised in
laser photocoagulation in combination with prior triamcino-
four cases (21 to +1 log line change). Exudation on lone injection on RAP stage I.
fluorescein angiography was stopped in 11 cases.
Conclusions: This preliminary case series suggests laser
photocoagulation combined with prior intravitreal triamci- MATERIALS AND METHODS
nolone injection as a viable treatment option for RAP stage I. We prospectively included 13 consecutive patients with RAP
In cases with marked macular oedema, intravitreal triamci- stage I at least in one eye. They were identified in the Ludwig-
Maximilians-University Munich, ARMD outpatient clinic
nolone injection improved visual acuity. For long-term
between October 2004 and May 2005 and showed typical
stabilisation, additional laser treatment is mandatory. These
signs of ARMD, including soft Drusen, retinal pigment
preliminary results warrant a more detailed prospective
epithelium changes or atrophy.
clinical trial.
Patients were both male and female (3 men and 10
women); their age ranged from 61 to 95 years (average age
75 years). None of their eyes had received any treatment
before inclusion into our study.
T
he entity of retinal angiomatous proliferation (RAP) as a
To be eligible, patients were required to have an extrafoveal
subtype of age-related macular degeneration (ARMD)
RAP lesion stage I (> 500 mm from the fovea), classified by
was first described by Yannuzzi et al.1 This new type of
clinical slit-lamp biomicroscopy by one experienced examiner
neovascular lesion in ARMD does not originate from the
(MU), fluorescein angiography and optical coherence tomo-
choroid, but begins with intraretinal new vessels, extends to
graphy (OCT) III. Other neovascular maculopathies such
the subretinal space and eventually communicates with new
as pathological myopia, angioid streaks, inflammatory
choroidal vessels. Yannuzzi et al distinguished three different
stages that indicate deep intraretinal capillary proliferation
within the retina (intraretinal neovascularisation) as stage I. Abbreviations: ARMD, age-related macular degeneration; BCVA, best-
corrected visual acuity; CRA, chorioretinal atrophy; FVS, fibrovascular
This is typically characterised by multiple small intraretinal
scar; IVTA, intravitreal triamcinolone; MAR, minimum angle of
haemorrhages and intraretinal oedema surrounding the core resolution; OCT, optical coherence tomography; PDT, photodynamic
of proliferating capillaries. It also includes hard exudates as therapy; PED, pigment epithelium detachment; RAP, retinal angiomatous
well as retinal–retinal anastomosis. proliferation; RCA, retinal choroidal anastomosis
www.bjophthalmol.comDownloaded from bjo.bmj.com on April 24, 2013 - Published by group.bmj.com
1358 Krieglstein, Kampik, Ulbig
Table 1 Visual acuity (logarithm of minimum angle of resolution units) of patients with retinal angiomatous proliferation stage I
who underwent combined triamcinolone injection and laser photocoagulation
Final VA
Patient Baseline VA VA 2 weeks VA 1 month VA 2 months 4 months Total VA change
number Age (log MAR) (log MAR) (log MAR) (log MAR) (log MAR) in loglines Complication
1 82 1 1 1 0.4 0.7 3 RAP stage I of
fellow eye
2 76 0.5 0 0 0 0 5
3 74 0.7 0.7 0.7 0.7 0.7 0
4 80 1 0.9 1.3 1.3 1.3 23
5 76 0.7 1 1 1 1 23
6 61 1 0.3 0.4 0.2 0.2 8
7 66 0.7 0.4 0.4 0.4 0.4 3
8 63 0.5 0.7 1 0.8 1 25 PDT 1
9 72 0.8 1 0.6 2
10 71 0.2 0.2 0.2 0.3 0.2 0
11 78 0.5 0.4 0.3 0.2 0.3 2
12 87 0.3 0.4 0.3 0.4 0.2 1 IVTA 2
13 95 0.6 0.5 0.7 0.5 21
Mean 0.65 0.57 0.6 0.57 0.54
The table also includes the age of the patients and complications, as well as eventual further additional treatment.
IVTA, intravitreal triamcinolone; MAR, minimum angle of resolution; PDT, photodynamic therapy; RAP, retinal angiomatous proliferation; VA, visual acuity.
chorioretinal diseases, tumours or trauma were not included. Another case showed rapid deterioration in the fellow eye,
Also excluded were late stages of RAP such as RCA or serous which progressed from RAP stage I to III during the period of
PED. review.
According to these criteria, 13 eyes of 13 patients were During the period of review, only one study eye progressed
included. All patients underwent a complete ophthalmic to RAP stage III. The other eyes with deterioration in visual
examination, including fluorescein angiography and OCT III acuity, nevertheless, showed stabilised angiographic findings.
at 2 weeks, 1, 2 and 4 months afterwards. Angiography was There were no complications related to intravitreal injec-
carried out with a Heidelberg Retina Angiograph II tion or laser treatment.
(Heidelberg Engineering, Heidelberg, Germany) at 30 s, 1, 3
and 5.5 min after injection of 10 ml 10% fluorescein (Alcon, Visual acuity
Texas, USA) into the cubital vein. In the case of marked This study showed visual improvement in six patients. In
macular oedema (.350 mm retinal thickening in OCT III, 12 four patients, visual acuity remained unchanged and three
of 13 cases), an intravitreal triamcinolone injection (4 mg) patients showed deterioration. At baseline, BCVA ranged
was given. The decision for laser treatment was based on the from logarithm of minimum angle of resolution (log MAR) 1
clinical findings and fluorescein angiography by one retinal to log MAR 0.2 (decimal equivalent 0.1–0.6 Snellen scale). At
specialist (MU). Photocoagulation was also carried out by the 1-month and 4-month visits the BCVA ranged from log
one retinal specialist (MU) by means of a Humphrey Visulas MAR 1.3 to log MAR 0.2, whereas the average BCVA changed
532 nm laser (Zeiss, Jena, Germany) and the ‘‘Area from log MAR 0.65 to log MAR 0.6 at the 1-month visit and
Centralis’’ lens (Volk, Mentor, Ohio) after a mean interval to log MAR 0.54 at the 4-month visit (fig 1).
of 4 weeks. The number of spots applied varied from 9 to 36 The BCVA improved in six patients (46%) by 2–8 log lines
(mean = 19 spots). The power was from 150 to 300 mW (average gain in this group was 3.8 log lines, decimal
(mean = 266 mW), with a spot size of 200 mm. The exposure equivalent 0.2–1.0 Snellen chart). The BCVA stabilised in four
time varied from 200 to 300 ms. patients (31%) (no log line change in visual acuity, decimal
Follow-up visits were performed at 2 weeks after laser equivalent 0.2–0.6 Snellen chart). In three patients (23%) the
treatment and at 1, 2 and 4 months after the treatment. All BCVA decreased by 2–5 log lines ( average loss in this group
follow-up visits included best-corrected visual acuity (BCVA) was 3.6 log lines, decimal equivalent 0.05–0.1 Snellen chart
with a Snellen chart at 6 months, full clinical examination (table 1).
with slit-lamp biomicroscopy, fluorescein angiography, opti-
cal coherence tomography and fundus photography. All Fluorescein angiography findings
examinations were also carried out on the fellow eye. Exudation on fluorescein angiography was completely
The main outcome measure was a change in visual acuity . stopped in 11 of 13 (85%) eyes at the 4-month visit. Even
Improvement was defined as a change in visual acuity from 2 in the group with deterioration of visual acuity, we observed
to 5 log lines, stabilisation by change in visual acuity from 21 stable angiographic findings.
to +1 log line, and deterioration was classified as a loss of 22
to 25 log lines.
Additionally, angiographic exudation was analysed. Table 2 Fellow eyes of patients under study and clinical
stage of age-related macular degeneration
RESULTS Clinical stage of ARMD Number of eyes
In one case, laser photocoagulation had to be repeated to
ARMD with mild Drusen 5
achieve complete cessation of exudation and stabilisation of RAP stage II or III 3
visual acuity. Another case showed persistent exudation and FVS 2
leakage, with extension into the subfoveal area. In this case, CRA 3
PDT was successfully carried out.
ARMD, age-related macular degeneration; CRA, chorioretinal atrophy;
One patient underwent intravitreal triamcinolone injection FVS, fibrovascular scar; RAP, retinal angiomatous proliferation.
and PDT on the fellow eye for advanced RAP.
www.bjophthalmol.comDownloaded from bjo.bmj.com on April 24, 2013 - Published by group.bmj.com
Retinal angiomatous proliferation 1359
A B
C D
E F
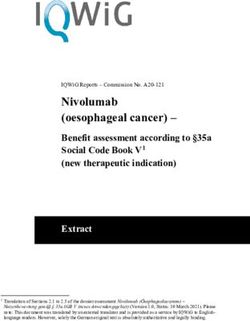
Figure 1 (A–D) Case 2: A 76-year-old woman with retinal angiomatous proliferation (RAP) stage I with extrafoveal leakage in the right eye. Visual
acuity was 0.3 (logarithm of minimum angle of resolution (logMAR) 0.5). (A, B) Angiography as well as optical coherence tomography (OCT) findings
showed extrafoveal leakage in combination with intraretinal oedema. Clinically, we found superficial intraretinal haemorrhages and hard exudates.
(C, D) Findings 4 months after intravitreal injection of triamcinolone and consecutive laser treatment. The visual acuity changed from 0.3 to 1.0 (log
MAR 0). There was no exudation in fluorescein angiography and no intraretinal oedema on OCT. (E) Fundus photography of treated RAP stage I lesion
after 4 months. (F) Fellow eye with RAP stage III.
In one eye with unchanged BCVA, angiographic extension DISCUSSION
of neovascularisation to the subfoveal area was noted. In this This study presents a novel treatment option in retinal
case, additional PDT was successful and the visual acuity angiomatous proliferation stage I. As the neovascular origin
stabilised. of the lesion is in the deep intraretinal vascular plexus,
Another patient showed recurrent exudation at the edge of photocoagulation of extrafoveal lesions was carried out to
the laser scar with intraretinal oedema at the 4-month visit. prevent progression to RAP stage II or III.1 This led to
Additional intravitreal triamcinolone injection and photo- stabilisation or improvement of visual acuity and stable
coagulation were scheduled in this case. angiographic findings in most of the eyes.
Thermal laser photocoagulation has been considered
Fellow eyes unfavourable with poor visual outcome previously because
The study eyes with treated RAP stage I lesion had better it does not spare retinal pigment epithelium.2 Especially in
function in 8 (62%) eyes compared with their fellow eyes. The eyes with associated PED, studies suggest little benefit.8–10
fellow eyes had either RAP lesions (stage II or III) or a Only one case reported laser treatment for RAP with
fibrovascular scar (table 2). cilioretinal artery anastomosis.11 However, since the specific
www.bjophthalmol.comDownloaded from bjo.bmj.com on April 24, 2013 - Published by group.bmj.com
1360 Krieglstein, Kampik, Ulbig
classification of RAP into different stages, there have been no Correspondence to: T R Krieglstein, Department of Ophthalmology,
further trials that evaluated conventional laser photocoagu- Ludwig-Maximilians-University of Munich, Mathildenstr. 8, 80336
lation as a treatment option for extrafoveal stage I RAP Munich, Germany; Tina.Krieglstein@med.uni-muenchen.de
lesions. However, the therapeutic gold standard for small
Accepted 1 June 2006
extrafoveal classic choroidal neovascularisation is thermal
Published Online First 2 August 2006
photocoagulation.12
According to the results of this preliminary study, early
detection and treatment of RAP stage I are recommended, and REFERENCES
a high level of visual acuity and quality of life can be sustained.
1 Yannuzzi LA, Negrao S, Iida T, et al. Retinal angiomatous proliferation in age-
Early detection is of most importance. These patients rarely related macular degeneration. Retina 2001;21:416–34.
had distortion, and as the RAP tends to form in an extrafoveal 2 Borrillo JL, Sivalingam A, Martidis A, et al. Surgical ablation of retinal
part of the macular area, only a mild decrease in visual acuity angiomatous proliferation. Arch Ophthalmol 2003;121:558–61.
3 Bottoni F, Romano M, Massacesi A, et al. Remodeling of the vascular channels
was reported. Presentation in the clinic is usually because of a in retinal angiomatous proliferations treated with triamcinolone acetonide and
RAP stage II or III lesion in the fellow eye. Yannuzzi et al1 photodynamic therapy. Graefe’s Arch Clin Exp Ophthalmol, 2006. Epub
observed RAP lesions to be bilateral. They begin with small ahead of print.
intraretinal, extrafoveal new vessels. Therefore it is mandatory 4 Hunter MA, Dunbar MT, Rosenfeld PJ. Retinal angiomatous proliferation:
clinical characteristics and treatment options. Optometry 2004;75:577–88.
to examine the fellow eye for early changes. 5 Pece A, Introini U, Botttoni F, et al. Acute retinal pigment epithelium tear after
We do acknowledge that our study presents only a small photodynamic therapy. Retina 2001;21:661–5.
number of patients and has a limited period of review. 6 Boscia F, Furino C, Prascina F, et al. Combined surgical ablation and
Nevertheless, it was shown that extrafoveal RAP stage I can intravitreal triamcinolone acetonide for retinal angiomatous proliferation.
Eur J Ophthalmol 2005;15:513–16.
benefit from combined treatment with intravitreal triamci- 7 Sakimoto S, Gomi F, Sakaguchi H, et al. Recurrent retinal angiomatous
nolone and thermal laser photocoagulation. This justifies a proliferation after surgical ablation. Am J Ophthalmol 2005;139:917–18.
more detailed and prospective clinical trial. The treatment of 8 Hartnett ME, Weiter JJ, Staurenghi G, et al. Deep retinal vascular anomalous
complexes in advanced age-related macular degeneration. Ophthalmology
RAP stage I may prevent the progression to RAP stage II and 1996;103:2042–53.
III for some time. 9 Slakter JS, Yannuzzi LA, Schneider U, et al. Retinal choroidal anastomoses
and occult choroidal neovascularisation in age-related macular degeneration.
..................... Ophthalmology 2000;107:742–53.
Authors’ affiliations 10 Kuhn D, Meunier I, Soubrane G, et al. Imaging of chorioretinal anastomoses
T R Krieglstein, A Kampik, M Ulbig, Department of Ophthalmology, in vascularized retinal pigment epithelium detachments. Arch Ophthalmol
1995;113:1392–8.
Ludwig-Maximilians-University of Munich, Munich, Germany 11 Ghazi NG, Conway BP. Retinal angiomatous proliferation with a cilioretinal
Competing interests: None declared. artery anastomosis: an unusual presentation. Graefe’s Arch Clin Exp
Ophthalmol 2005;243:493–6.
Presented in part at the Société Francaise d̀ Ophthalmologie meeting, 12 Ulbig MW, Mc Hugh DA, Hamilton AMP. Photocoagulation of choroidal
May 2005, Paris, France and the joint meeting of 103rd DOG neovascular membranes with a diode laser. Br J Ophthalmol
Congress/15th SOE Congress, September 2005, Berlin, Germany. 1993;77:218–21.
www.bjophthalmol.comDownloaded from bjo.bmj.com on April 24, 2013 - Published by group.bmj.com
Intravitreal triamcinolone and laser
photocoagulation for retinal angiomatous
proliferation
T R Krieglstein, A Kampik and M Ulbig
Br J Ophthalmol 2006 90: 1357-1360 originally published online August 2,
2006
doi: 10.1136/bjo.2006.092536
Updated information and services can be found at:
http://bjo.bmj.com/content/90/11/1357.full.html
These include:
References This article cites 11 articles, 1 of which can be accessed free at:
http://bjo.bmj.com/content/90/11/1357.full.html#ref-list-1
Article cited in:
http://bjo.bmj.com/content/90/11/1357.full.html#related-urls
Email alerting Receive free email alerts when new articles cite this article. Sign up in the
service box at the top right corner of the online article.
Topic Articles on similar topics can be found in the following collections
Collections
Ophthalmologic surgical procedures (1024 articles)
Retina (1293 articles)
Notes
To request permissions go to:
http://group.bmj.com/group/rights-licensing/permissions
To order reprints go to:
http://journals.bmj.com/cgi/reprintform
To subscribe to BMJ go to:
http://group.bmj.com/subscribe/You can also read