London International Model United Nations Foundation
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
1
WHO LIMUN 2021
Table of Contents
Directors’ Welcome 3
Introduction to the Dais 4
Director - Nikita Julius 4
Director - Farrah Farnejad 4
Assistant Director - Marina Markarian 4
Introduction to the Committee 5
History of the Committee 5
Structure and Functions of the WHO 5
Strengthening Multilateral Global Health Cooperation in Light of the
COVID-19 Pandemic 7
Topic Background 7
Discussion 12
Multilateralism in the WHO 12
The Case for Multilateral Health Cooperation 12
The Need for WHO Reform 13
International Health Regulations (IHR) 15
Middle- and Low-Income States 17
A Case Study in Multilateralism: The COVID-19 Vaccine 19
Bloc Positions/Key Stakeholders 20
Association of Southeast Asian Nations 20
China 21
Taiwan 22
The African Union 23
The Middle East & Israel 23
United States of America 24
United Kingdom and the European Union 25
Points a Resolution Should Address 27
Further Reading 28
Bibliography 29
2
WHO LIMUN 2021
Directors’ Welcome
Dear Delegates of the WHO,
Welcome to LIMUN 2021, the first ever online session of LIMUN!
We would like to welcome you to the World Health Organisation
committee, a specialised UN agency that works to shape the health agenda,
provide aid and leadership on global health issues, and offer assistance to
countries indeed. In the current climate of the pandemic, our debate topic
of “Strengthening Multilateral Global Health Cooperation in light of the
COVID-19 Pandemic,” is a great opportunity to discuss timely issues of global
concern; we as chairs, have a strong interest in this issue.
We hope that this topic proves to be interesting, allowing for a successful
debate. We have created this study guide to aid your understanding of this
topic. However, please note that the study guide is only meant to introduce
you to the basics of the topic and underlying issues; it really cannot replace
any detailed research you will do into your assigned country. Equally, do not
be put off by the length of the study guide - a large portion consists of
references, which we do encourage you to use to guide your research!
MUN is an unforgettable event for all those participating, so we will do our
very best to make it a mentally gratifying and delightful experience. We are
greatly looking forward to meeting you all, despite the online setting, and
hope this is an amazing experience for you all. We will make sure that this
conference will be filled with engaging debates, lively socials and
enlightening academic advancements.
Please do not hesitate to contact us with any questions via email at who-
2021@limun.org.uk.
Sincerely,
The WHO Chairing team
Farrah, Nikita & Marina
3WHO LIMUN 2021
Introduction to the Dais
Director - Nikita Julius
My name is Nikita Julius and I am a Translational Neuroscience MSc student
at Imperial College London. I studied Natural Sciences and specialised in
Biology and Maths at Durham University beforehand. I aim to pursue a PhD
next, and remain in research with the hope of eventually becoming a
professor. Model UN has been a longstanding hobby of mine and I have
participated, as chairs and delegates, in national and international Model
UN conferences since 2014. Besides MUN and academics, I enjoy playing
golf, DJing, and travelling. I am looking forward to chairing the WHO
Committee at LIMUN 2021 and hope that everyone enjoys their weekend!
Director - Farrah Farnejad
Distinguished Delegates, My name is Farrah Farnejad and it is my great
pleasure of being one of your committee chairs at this year’s LIMUN. I am a
second-year global health student at the Queen Mary University of London,
where I had the privilege of being the DISEC chair for this year’s QMMUN.
Over the past 4 years, I have been a part of various national and international
MUN conferences, both as a delegate and chair. During my free time, I enjoy
avidly reading books about public health, travelling whilst attempting the
local language, and volunteering. Congratulations for your acceptance into
the conference! Despite the COVID-19 circumstances, I am greatly looking
forward to meeting all of you, and to assist you in any way I can. I hope you
have an amazing time at LIMUN 2021!
Assistant Director - Marina Markarian
Dear delegates, my name is Marina Markarian and I am grateful for the
opportunity to meet you all very soon. I am currently a political science
major concentrating in human rights and transitional justice. On a more
personal note, I have always been passionate about standing up for things I
believe in and look for ways to bring about change. I enjoy reading, writing
and especially watching a movie or show for some comic relief. The
maintenance of a positive aura is vital for myself which encourages me to
help everyone find happiness. This year marks my 5th year involved in MUN
conferences that never fail to amaze me. I am very excited to be chairing the
WHO committee alongside Nikita and Farrah and hope those three days
will become a memorable experience.
4WHO LIMUN 2021
Introduction to the Committee
History of the Committee
In 1945, diplomats from 50 different nations across the world met in San
Francisco for the United Nations Conference International Organisation
(UNCIO), to establish the United Nations.1 During this time, they had
discussed setting up a global health organisation. On the 22nd of July 1946,
51 members of the UN, and 10 other nations, signed the constitution of the
World Health Organisation (WHO).2 The Constitution came into force on the
7th of April 1948 – World Health Day.3 The WHO is a specialised UN agency,
and on the 24th of June 1948, the first Health Assembly opened in Geneva,
with delegations from 53 of the 55 UN Member States.
Major achievements of the WHO include the 1986 Global Programme on
AIDS, and the 1979 worldwide eradication of smallpox after the 1958
programme.4 This achievement was accomplished through the
collaboration of many countries, including the United States, England,
Russia and South Africa who worked with the WHO in 1981.5 In the face of
the challenge posed by the COVID-19 pandemic, the WHO, CEPI and GAVI
set up the COVAX scheme this year,6 collaborating with around 150
countries to search for an effective vaccine for all countries.7
Structure and Functions of the WHO
The WHO comprises over 7000 staff from more than 150 countries, which
includes public health specialists, economists, scientists and emergency
relief staff.8 194 Member States have accepted the WHO’s constitution. The
WHO has three core functions: normative, directing and coordinating, and
research and technical cooperation, with key functions outlined in the WHO
Constitution.9
The WHO plays an active role in the global governance of health and
disease. Global health improvement is facilitated by the WHO via means
such as the transfer of medical and public health knowledge and
1
WHO, “Global Health Histories.”
2
Ibid.
3
Ibid.
4
WHO, “WHO in 60 years: a chronology of public health milestones.”
5
CDC, “History of Smallpox.” CDC.
6
WHO, “Archived: WHO Timeline - COVID-19.”
7
WHO, “More than 150 countries engaged in COVID-19 vaccine global access facility.”
8
WHO, “WHO - organizational structure.”
9
WHO, “CONSTITUTION OF THE WORLD HEALTH ORGANIZATION.”
5WHO LIMUN 2021
technology. This includes the sharing of best practices, health promotion
and prevention strategies, and medical treatments.10
Global health functions include actions taken to promote global public
health services. Global health services include, inter alia: global advocacy for
health; bio-ethical and human rights instruments; the surveillance for
diseases and risk; direct global action; investment in health problems; the
usage of norms and standards.11 The WHO addresses these functions via
eight divisions: communicable diseases, non-communicable diseases and
mental health, family and community health, sustainable development and
health environments, health technology and pharmaceuticals, and policy
development.
The WHO is the only agency within the UN system that is able to assume
authority in the development and implementation of international health
norms and standards.12
The World Health Assembly (WHA) assumes the role of the WHO’s supreme
decision-making body. WHO Member States employ delegations to the
WHA. The WHO assembly meets in May; they consider the financial policies
of the WHO and approve the programme budget. The Executive Board
comprises 34 elected members with health-oriented technical
qualifications. Ultimately, the Board has the function of carrying out
Assembly-ratified policies, advising it, and facilitating its work in general.13
Contributions from donors and Member States are the WHO’s source of
funding. Collaborative efforts are generally at the forefront; as of 2017, the
WHO had 80 partnerships with non-governmental organisations, the
pharma industry, and other foundations. Such collaborative efforts form the
bulk of the WHOs financing, exceeding contributions from Member States.
Please note that in our debate at LIMUN 2021, we shall be simulating the
work of the World Health Assembly.
10
Ruger and Rach, “The Global Role of the World Health Organisation.”
11
Yach, Fluss, and Bettcher, “Health and the environment.”
12
Ruger and Rach, “The Global Role of the World Health Organisation.”
13
Yadav, “Structure and Functions of the World Health Organisation.”
6WHO LIMUN 2021
Strengthening Multilateral Global
Health Cooperation in Light of the
COVID-19 Pandemic
Topic Background
The WHO has played a large role in previous outbreaks, as well as the
current COVID-19 pandemic. One such pandemic was the Severe Acute
Respiratory Syndrome (SARS) pandemic that started in 2003. The virus
responsible, SARS-CoV, was first discovered in Asia, in February 2003.14 Gro
Harlem Brundtland, former director general of the WHO, leading the fight
against the 2003 SARS pandemic, had faced criticism and subsequently fell
out of favour with the international community for her actions during the
outbreak.15 Gro Brundtland had confronted China over the outbreak and
issued warnings against travel to SARS-affected countries, acting without
approval from the countries concerned or without authority.16 She had also
publicly criticised China for being slow to share information about SARS
with the rest of the world.17
After this, China, as well as the US and other developed nations, opposed
WHO reform, thus missing an opportunity to reform, which would have
given the organisation more power and a wider remit. Although
Brundtland’s approach was not always popular, the WHO’s response to
SARS was considered a huge success; fewer than 1,000 people died
worldwide, despite it reaching 26 countries.18 The WHO led efforts in
scientific advancements of the SARS virus, developed public health
strategies, and established clinical treatment protocols.19 This pandemic had
been defeated through non-pharmaceutical interventions; travel warnings,
tracking, testing, isolating cases, and a huge information-gathering
operation across multiple countries, made possible from the WHO’s
willingness to hold authority.20 After this, the WHO drew a new version of
14
CDC, “CDC SARS Response Timeline.”
15
Fidler, “The World Health Organization and Pandemic Politics.”
16
Parry, “China joins global effort over pneumonia virus.”
17
Ibid.
18
Buranyi, “The WHO v coronavirus: why it can't handle the pandemic.”
19
Parry, “China joins global effort over pneumonia virus.”
20
Ibid.
7WHO LIMUN 2021
the IHR, asking members to prepare public health threats according to
WHO standards, report outbreaks, and allow the WHO to declare a PHEIC,
however, the document did not give the WHO any power if states refuse to
comply.21 After adopting the International Health Regulations (IHR), WHO
member states gave the WHO state sovereignty, and expanded the need
for WHO’s scientific, medical, and public health capabilities; these capacities
were tested in the 2009 influenza pandemic.22
The first confirmed case of the influenza Swine Flu outbreak was on the 11th
of March 2009 in Mexico;23 the UK confirmed its first case detection on April
27. The Swine Flu outbreak revealed problems with the WHO and IHR’s
performance and functioning, emphasising the importance of the WHO’s
leadership and IHR’s role in global health governance.24 The WHO intended
to avoid damage to the Mexican economy by labelling the outbreak the
“Mexican Flu,”25 however faced consequences such as the Egyptian
government’s mass culling of pigs. After recognising these consequences,
the WHO halted bans and measures; on April 26th 2009, it issued a press
release to emphasise that trade and travel restrictions were not
recommended, and stated the next day that there was no risk of infection
from pork, resulting in official complaints from Egypt and the World Trade
Organisation.26 The WHO declared Swine Flu as a pandemic on the 11th of
June 2009, a month after 30 countries had already detected cases. After
publishing confusing information about the alert phases for the virus, the
secretariat deleted its Influenza guidelines from the WHO website.27
The WHO’s previous shortcomings carried into the 2014 Ebola outbreak,
resulting in a disaster for the WHO and IHR.28 WHO’s director general
Margaret Chan failed to act on any information the WHO received from non-
governmental sources, and did not challenge governments that wanted to
keep the outbreak silent.29 The first case of Ebola was reported on March
23rd 2014, and the WHO did not declare the epidemic a PHEIC until August
8th 2014, after the epidemic was already a crisis and the curve had mostly
21
Ibid.
22
Ibid.
23
CDC. “Outbreak of Swine-Origin Influenza A (H1N1) Virus Infection - Mexico, March-April
2009.”
24
Ibid.
25
Kamradt-Scott, “What Went Wrong? The World Health Organization from Swine Flu to
Ebola.”
26
Ibid.
27
Ibid.
28
Fidler, “The World Health Organization and Pandemic Politics.”
29
Kamradt-Scott, “What Went Wrong? The World Health Organization from Swine Flu to
Ebola.”
8WHO LIMUN 2021
flattened.30 This poor response resulted in Ban Ki-moon, UN Secretary-
General, creating an ad-hoc emergency response effort.31 Additionally,
numerous governments disregarded the WHO’s recommendations by
implementing travel restrictions, and this crisis exposed substandard IHR
implementation worldwide, leading to criticisms of the WHO’s performance
and recommendations to strengthen its capabilities to respond to serious
public health crises. 32
Past criticisms of the WHO, particularly regarding delays in declaring
outbreaks as a pandemic, and misinformation, underscore the need for the
improvement of the transparency of the WHO’s processes and
recommendations for dealing with future emergencies; the recent Covid
pandemic is yet another case in point.
On the 31st of December 2019,33 the WHO’s office in the People’s Republic of
China (henceforth referred to as China) had picked up a statement by the
Wuhan Municipal Health Commission regarding cases of “viral
pneumonia”34 in Wuhan. This led to reports about cases of “pneumonia of
unknown cause”35 in Wuhan, and several health authorities worldwide
contacted the WHO for additional information.
The WHO activated its Incident Management Support Team on January 1st
2020, as a part of their emergency response framework.36 This ensured
coordination across the levels of the WHO, informed the Global Outbreak
Alert and Response Network, which includes public health agencies,
laboratories, sister UN agencies, international organizations and NGOs, 37
about the cluster of public cases.
From January 2020, the WHO had requested more information about the
cases from Chinese authorities and issued the first Disease Outbreak News
report on the virus on the 5th of January 2020.38 This contained information
about the virus and recommendation, partially based on information
provided by China later on.39
30
CDC, “2014 Ebola Outbreak in West Africa Epidemic Curves.”
31
Ibid.
32
Ibid.
33
WHO, “Listings of WHO’s response to COVID-19.”
34
Ibid.
35
Ibid.
36
Ibid.
37
Ibid.
38
Ibid.
39
Ibid.
9WHO LIMUN 2021
Since December 31st 2019 and reiterated again on January 5th, 2020, Taiwan
had implemented health screenings from all flights arriving from Wuhan,
citing that they were unable to get verifiable answers from the WHO or
Chinese CDC.40 Early in the pandemic, Taiwan had received reports from
Wuhan that Chinese medical staff were getting ill from treating patients, a
clear sign of human-to-human transmission, and they reported this to the
International Health Regulations (IHR) and Chinese health authorities, on
December 31st 2019.41 Taiwanese government officials had said that this
warning was not shared with other countries by the WHO.
Figure 1: COVID-19 Cases as of March 2021. Graph by Felix Richter, Statista.42
On the 30th of January 2020, the WHO had declared that COVID-19
constitutes a Public Health Emergency of International Concern (PHEIC). 43
However by this date, 581 COVID-19 cases had been confirmed globally in
countries such as the US, Thailand, Japan and Republic of Korea.44 There
have been concerns that the WHO had declared COVID-19 a PHEIC and
Pandemic too late.45 Lack of information sharing and WHO warning of
COVID-19’s severity, arguably played a part in the rise in cases, with countries
in turn failing to effectively impose measures to stop spread. Although the
PHEIC declaration did not directly change anything, it would have
heightened the emergency and awareness of the virus situation worldwide
40
Taiwan Centres for Disease Control, “In response to pneumonia outbreak in Wuhan,
China and related test results, Taiwan CDC remains in touch with China and World Health
Organization and Taiwan maintains existing disease control and prevention efforts.”
41
Financial Times, “Taiwan says WHO failed to act on coronavirus transmission warning.”
42
Richter, “Pandemic at a Crossroads as New Variants Loom.”
43
WHO, “COVID-19 Public Health Emergency of International Concern (PHEIC) Global
research and innovation forum.”
44
WHO, “Novel Coronavirus (2019-nCoV) SITUATION REPORT - 3.”
45
Science Media Centre, “Expert reaction to WHO’s decision to declare the Wuhan
coronavirus outbreak a PHEIC (Public Health Emergency of International Concern).”
10WHO LIMUN 2021
to other countries. Additionally, it would have opened up financial support
opportunities by donors who typically focus on funding emergency
responses.
COVID-19 was declared a pandemic by the WHO on the 11th of March 2020,
and urged countries to take urgent and aggressive action.46 Following on to
the 13th of March, the WHO and partners launched a COVID-19 Solidarity
Response Fund,47 raising more than US$70 million from more than 187,000
individuals and organisations in just 10 days. This shows the impact that
philanthropy can have between countries. Questions can be raised about
whether multilateral health cooperation, transparency, and information
sharing could have limited the virus spread earlier.
The WHO is responsible for international public health,48 vital for
international emergencies such as a pandemic, where multilateralism is
needed. Many countries have expressed their concern that the WHO did not
ensure the global cooperation between countries and between
organisations and did not effectively inform countries about the risk.
Since then, the WHO has announced a $675 million budget49 to respond to
the rising COVID-19 cases that were present in almost every continent. This
has been seen in the $9 trillion spent by governments,50 as well as laws and
recommendations of wearing masks have been implemented.
Multilateralism has also been seen by many EU member countries; France
has donated masks, Germany delivered medical equipment to Italy,
Luxembourg has taken intensive care patients from France, and the Czech
Republic donated protective suits to Italy and Spain.51 Schemes such as
COVAX have also been set up to share vaccines. The Global Health Cluster
COVID-19 Task Team was established to strengthen the coordination
between the WHO and member countries during the pandemic.52
46
Ibid.
47
WHO, “COVID-19 Solidarity Response Fund.”
48
KFF, “The U.S. Government and the World Health Organization.”
49
WHO. 2021. “US$675 million needed for new coronavirus preparedness and response
global plan.”
50
IMFBlog, “Tracking the $9 Trillion Global Fiscal Support to Fight COVID-19.”
51
News European Parliament, “Solidarity: how EU countries help each other fight Covid-19.”
52
WHO, “COVID-19 Task Team.”
11WHO LIMUN 2021
Discussion
Multilateralism in the WHO
While countries were faced with worsening public health situations,
multilateral cooperation was slowly forgotten. A unified response from the
international community against this virus is necessary to overcome this
heavy obstacle.53 In 2019, twelve multilateral agencies were launched to
connect countries to each other to help perform better and support one
another in times of dire health crises. 54 The goal of this plan was also to
promote further emphasis on the UNDP’s 17 Sustainable Development
Goals. The director general of the WHO, Tedros Adhanom Ghebreyesus,
stated that the plan was named “Stronger Collaboration, Better Health,” and
prioritised global engagement of countries for strategising and prioritising
multilateralism worldwide to improve communication, coordination, and
implementation.55
The Case for Multilateral Health Cooperation
The COVID-19 pandemic has strongly emphasised the need for a
strengthened multilateral approach to global health. The pandemic has
proven the lack of preparedness of the international community. The
uncoordinated nature of the global response begs change.
The attention needed to inform countries and people about the pandemic
was not achieved until doctor Li Wenliang was killed by the virus, on
February 7th 2020.56 He died trying to issue a warning about the severity of
COVID-19 in Wuhan, but the Public Security Bureau accused him of making
false comments/rumours, and disturbing the social order. 57 Doctor Li
Wenliang’s death and the publicity that surrounded his entire situation,
through reporting by news media outlets, helped to increase global
awareness and recognition of the severity of the situation.
Coordination of global efforts is necessary for states to move beyond “what
is best for their country.” Even if some countries have achieved near-
eradication of COVID-19, or vaccinated the whole population, many
countries will still be struggling with the impacts of the pandemic. Spotting
disease outbreaks in developing countries will be of global importance.
53
UNGA, “COVID-19 Pandemic Demonstrates Multilateral Cooperation Key to Overcoming
Global Challenges.”
54
WHO, “Multilateral agencies launch a joint plan to boost global health goals.”
55
Ibid.
56
BBC, “Li Wenliang: Coronavirus kills Chinese whistleblower doctor.”
57
Ibid.
12WHO LIMUN 2021
Indeed, if the COVID-19 outbreak was spotted quickly and contained in the
first place, it would not have spread to other countries, including developing
countries, thus potentially reducing the public health, socioeconomic and
political damages brought by COVID-19.
On 4th June 2020, the Global Vaccination Summit was held in London,
where $8.8 billion of pledges were made in order to catapult research for a
vaccine, thereby proving the pertinence of multilateral action.58
International cooperation was a contributing factor to the eradication of
smallpox, the reduction of both prevalence and mortality of HIV/AIDS, the
containment of SARS, H1N1, and Ebola.59 The move away from multilateral
efforts but towards populism, a lack of transparency and proliferation of
misinformation, has hampered efforts to combat the COVID-19 pandemic.
The Need for WHO Reform
The COVID-19 pandemic has demonstrated the need for multilateral
cooperation in overcoming global challenges. It is clear that collective
action is needed to tackle this public health crisis. Despite collaborative
efforts and frameworks, more is needed. In particular, the need for WHO
reform has been recognised by the WHO itself since 2012.60
Among other existing health cooperative frameworks, the IHR (discussed
below) provides a legal framework, defining countries’ rights and
obligations in the handling of public health events. The WHO coordinates
the implementation of the IHR, which requires countries to detect, assess
and report, and respond to public health risks. Despite this, the WHO has
no way of compelling nations to adhere to the IHR.
The WHO and partners launched the Access to COVID-19 Tools (ACT)
Accelerator in April 2020.61 The ACT-Accelerator is an international
collaboration aimed to develop tools to fight COVID-19. This initiative,
among other things, fast-tracks the development, production and
accessibility to COVID-19 tests, treatments and vaccines across the globe. To
date, $11 billion pledges have been made. The ACT-Accelerator provides a
framework for collaboration. Despite the ACT-Accelerator promoting
58
UK Government, “Global Vaccine Summit.”
59
Duong et al., “More, not less, multilateralism is needed to fight the coronavirus
pandemic.”
60
Ibid.
61
WHO, “The Access to COVID-19 Tools (ACT) Accelerator.”
13WHO LIMUN 2021
equitable access to tools, it is undermined by private bilateral agreements
between high-income countries and manufacturers of COVID-19 vaccines.62
Despite these existing attempts at multilateral cooperation, the WHO has
faced claims of being ‘severely underfunded, chronically over-mandated by
Member States, and weak by design.’63 It is clear that the WHO would
benefit from structural reform. After the 2014 Ebola outbreak, a group of
independent experts decided the “WHO does not have the capacity or
organizational culture to deliver a full emergency public health response.”64
Namely, the organisation’s internal management was highlighted as a
cause of concern due to its lack of accountability.
Another issue is the WHO’s heavy dependence on its donors, hindering its
governing structure. Key to this is Member States’ priorities which may
conflict with those of major donors. Large donors to the WHO are
catapulted to a position of cherry-picking projects, side-lining issues that
aren’t seen as an immediate threat or importance to these donors. 93% of
the money given to the WHO in 2016 was earmarked for specific health
projects.65 Whilst the WHO could, theoretically, question donors’ wishes,
donors have the capacity to withdraw their funding and use it elsewhere,
undermining the WHO’s capacity to deliver.
Moreover, the WHO constitution means that the autonomy given to
regional offices (see structure and function) causes issues when aligning
regional and country offices with overall WHO aims. In particular, regional
directors are selected by regional governments rather than the WHO; these
regional directors work with their region more closely than with the WHO,
presenting greater opportunity for the downplay of events/misinformation
shared with the Geneva HQ, as seen by the downplaying of the Ebola
outbreak by the Guinea government in 2014.66 This selection policy is hard
to reverse, given that amendments to the constitution requires a two-thirds
majority by the WHA.
The bureaucratic nature of the WHO presents an overly complicated and
expensive management structure. The WHO lacks the mandate to
independently assess situations of major health risks specific to Member
States or to receive such information from non-state actors. This level of
62
Figueroa, “Urgent needs of low-income and middle-income countries for COVID-19
vaccines and therapeutics.”
63
The Economist, “The world needs a better World Health Organisation.”
64
Huang, “How to Reform the Ailing World Health Organization.”
65
Kelland, “The World Health Organization’s critical challenge: healing itself.”
66
Ibid.
14WHO LIMUN 2021
bureaucracy could be targeted, allowing the WHO to act on unofficial data
thereby driving better response times and decreasing reliance on trust.
More specific reforms to the WHO have been suggested as a result of
lessons learned during COVID-19. The European Council has called for an
international treaty on pandemics, a move that has been supported by the
director general of the WHO.67 This new global framework would address
existing deficiencies in the IHR. Such a framework is not unheard of, with
the WHO’s Framework Convention on Tobacco Control (FCTC), which was
rapidly embraced as a multilateral regime in health.68 The FCTC fulfilled the
following functions: it was legally binding, had a uniform reporting system,
ensured the transfer of knowledge and technology, and worked with non-
health sectors under an international legal system.69 Most importantly, such
a treaty must have the functions of activating financial mechanisms,
defining both the obligations and breaches of signatories, and have
mechanisms in place to evaluate compliance. On top of this, talks are
planned at the WHA in May 2021 to address other relevant proposals to the
improvement of the WHO. The modification of the PHEIC alarm system is
up for debate; colour-coded warning levels are being considered. It is
thought that countries may be more willing to share information regarding
health risks if a system was in place to raise a low-grade alarm, which would
also be less likely to halt economic activity.70 Multilateral health cooperation
is about sharing best practices to bring countries together to achieve the
WHO’s motto of “health for all.”
International Health Regulations (IHR)
The WHO Health Emergencies Programme was established to work with
countries in order to detect, respond to and recover from emergency health
threats.71 A key aim of this programme is to inform public health decision-
making. A reporting infrastructure was established via this programme
whereby Member States are required to provide annual reports on their
capacities, required under IHR.72 Joint external evaluations of IHR capacities
are carried out by internal and external experts, ensuring transparency and
accountability.
67
Nikogosian and Kickbusch, “The case for an international pandemic treaty.”
68
Ibid.
69
Ibid.
70
Maxmen, “What a US exit from the WHO means for COVID-19 and global health.”
71
Giang and Tran, “WHO Health Emergencies Programme.”
72
WHO, “Monitoring country emergency preparedness.”
15WHO LIMUN 2021
The IHR is a well-established instrument, providing “an overarching legal
framework that defines countries’ rights and obligations in handling public
health events and emergencies that have the potential to cross borders.”73
The IHR are an instrument of international law that is legally binding on 196
countries, including 194 WHO Member States.74 A notable requirement is
the reporting of public health events, allowing for the determination as to
whether an event meets the criteria to be declared a “Public Health
Emergency of International Concern'' (PHEIC). The WHO’s role is to
coordinate IHR implementation. The IHR requires the following from all
countries:75
1. Detect: Make sure surveillance systems can detect acute public
health events in timely manner
2. Assess and report: Use the decision instrument in Annex 2 of the IHR
to assess public health event and report to WHO through their
National IHR Focal Point those that may constitute a public health
emergency of international concern
3. Respond: Respond to public health risks and emergencies.
Despite this, many countries’ obligations to the IHR have not been met; the
IHR’s role has been side-lined amidst the pandemic. An example of this is
the case of public health authorities in Wuhan, China. Some evidence has
suggested that COVID-19 was suspected in China for some weeks before the
WHO received this information.76 As it stands, the IHR does not allow non-
state actors (e.g. the WHO) to seek information from states without being
subject to verification from the state in question.77
The IHR sets out binding core capacities for domestic public health systems.
States still maintain autonomy in developing their own national health
legislations, however this is required to “uphold the purpose of the IHR.”78
However, only one third of countries meet this. Naturally, it follows that
global solidarity and international support is needed in order to bolster the
IHR provisions by means such as incorporating a financial mechanism in
order to assist middle- and low-income countries in order to meet these
73
Mackenzie, “International Health Regulations.”
74
Ibid.
75
Ibid.
76
Huang et al., “Clinical features of patients infected with 2019 novel coronavirus in Wuhan,
China.”
77
Taylor et al., “Solidarity in the wake of COVID-19: reimagining the International Health
Regulations.”
78
WHO, “International Health Regulations (2005) Third Edition.”
16WHO LIMUN 2021
capacities.79 Again, it is clear from this that a multilateral cooperative and
collaborative effort is needed to enable an effective reporting mechanism
to monitor and sustain the implementation of the aforementioned IHR
obligations. Furthermore, equal action from the WHO to uphold the IHR
standards is required; specifically, in reporting information received via the
IHR to Member States. The case of Taiwan is an example of the WHO’s failure
in this (see 80).
Ultimately, despite the IHR’s role in providing an international framework to
fuel global cooperation and solidarity, the rise of nationalism and lack of
transparency within the WHO has undermined this effort. It is clear that
failure to uphold this global health law threatens the future of global health.
Middle- and Low-Income States
COVID-19 has asserted its need for a range of measures: better laboratory
facilities and protocols, contact tracing, personnel and equipment. These
measures are lacking in the developing world, with COVID-19 medical
products being less accessible (see above).81 This transnational health crisis
therefore requires global cooperation, solidarity and coordination toward
global health equity.
Importantly, global health organisations must ensure representation from
middle- and low-income countries, thus ensuring the advocacy for
communities most affected by the pandemic.
With the development of a UN COVID-19 response plan, known as the UN
COVID-19 Response and Recovery Fund, there is hope for aid to middle- and
low-income countries.82 The fund seeks to help such countries cope and
recover from impacts of the pandemic by developing emergency response
projects, it currently operates across 67 countries. The fund operates on the
Leaving No One Behind principle. Moreover, the UN and WHO have played
key roles in supporting these countries by providing means of testing and
PPE equipment. Gavi, the Vaccine Alliance, made up to $200 million
available by April 2020 to provide these vital supplies to middle- and low-
income countries via UNICEF.83
79
Ibid..
80
Riordan, et al., “Taiwan says WHO failed to act on coronavirus transmission warning.”
81
Ibid.
82
Ibid.
83
English and Mercado, “COVID-19: Gavi and UNICEF to secure equipment and diagnostics
for lower-income countries.”
17WHO LIMUN 2021
Reluctance, or even refusal by national leaders to meet financial
commitments to the WHO’s pandemic response, however, has undermined
the organisation’s ability to provide an effective response.
One of the most pertinent threats to a multilateral response to the
pandemic lies within violations of International Health Regulation (IHR)
obligations whereby failures to share timely and accurate information has
been seen, including the lack of action on the WHO’s recommendations
and warnings.84 Such failures to enable international coordination has been
detrimental to the fight against COVID-19, particularly threatening middle-
and low-income countries.
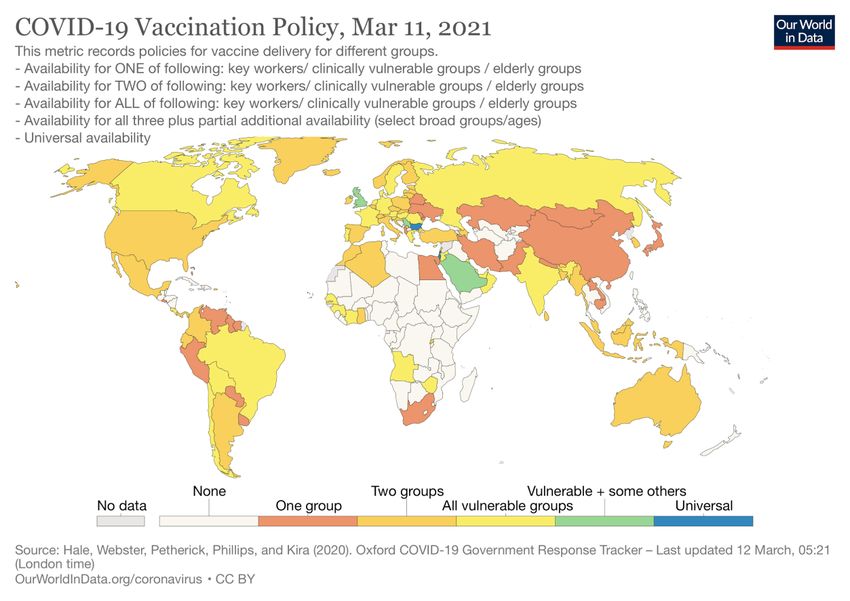
In the early months of the pandemic, isolationist and protectionist policies
directly affected the movement of health supplies, thus affecting countries
most in need. These health supplies included PPE supplies, and medical
equipment such as ventilators. High-income countries have channelled
their funds to secure their early vaccination rollout schemes. The scramble
for vaccines has fragmented the geopolitical landscape.85 A world map of
vaccine distribution can be seen in Figure 2.
Despite most of the WHO’s mandate focussing on developing countries, its
governance has provided a platform for the collaboration of all states in
guiding global health policy. The WHO has been a key actor in providing
both technical and normative standards for global health management.
Middle- and low-income states tend to rely on support via means of
technical and operational guidance, whereas high-income states depend
more on information share and research coordination from the WHO. The
WHO sought collaboration from state and non-state actors in order to
coordinate collaborative COVID-19 research.86 The Solidarity trial for
treatments, initiated by the WHO in March 2020, is a multinational clinical
trial which can be seen as symbolic in initiating a results-sharing platform.
This trial incorporates efforts from Asia, South Africa, Europe and the
Americas.87 Despite its creation, it is clear that this effort will need political
support, efficient collaboration, well-placed expertise and resources, and
informed guidance.
Intellectual property rights present a problem in battling COVID-19, with
differing stances on the matter presenting issues. Whilst the concept of
84
Ibid.
85
Ibid.
86
Ibid.
87
Cattani, “Global coalition to accelerate COVID-19 clinical research in resource-limited
settings.”
18WHO LIMUN 2021
intellectual property rights incentivises the development of vaccinations
and medical equipment, such as ventilators and virus-tracing software, the
developing companies have a monopoly over their products, thus allowing
them to dictate prices88. The WHO created a voluntary product pool. The
product pool was intended to collect patent rights, regulatory test data, and
other information regarding the fight against COVID-19.89 Such a move
would increase affordability and enable more equitable access to such
products, in a bid to support middle- and low-income countries.
Governments such as the UK, US, Switzerland and Canada have opposed
this pool, undermining the WHO’s attempt at multilateralism. Currently,
vaccine prices have varied widely across the globe (see90).
Figure 2: Map of Vaccine Distribution as of 11/03/2021. Map by Hale et al. (2020) 91
A Case Study in Multilateralism: The COVID-19 Vaccine
As many vaccine programmes have been implemented throughout
different countries, the WHO has voiced concerns about “vaccine
88
Bonadio and Cadillo Chandler, “Intellectual property and COVID-19 medicines: why a
WTO waiver may not be enough.”
89
Silverman, “The WHO launched a voluntary Covid-19 product pool. What happens next?”
90
Newkey-Burden, “What do Covid vaccines cost - and who is paying over the odds?”
91
Hale et al., “COVID-19 Vaccination Policy, Mar 11, 2021.”
19WHO LIMUN 2021
nationalism”, especially the shortfall in the supply of EU COVID-19 vaccines.92
The WHO asked countries to work together in solidarity to ensure that the
vaccination of health workers and older people was underway in all
countries. Programmes such as COVAX and ACT Accelerator were set up,
with aims of distributing vaccines, treatments and diagnostics equally
across the globe.
COVAX brought countries together to pool funds and resources to
cooperate and provide fair access to vaccines,93 aiming to achieve 2 billion
doses by the end of 2021. There are 172 economies in discussions to
participate with COVAX.94 80 countries have made submissions to join the
92 LMICs that are eligible to be supported by COVAX. The issue of vaccine
nationalism has been discussed; it is not just a matter of ethics, but it also
ignores efforts to prioritise vaccine access to those most in need. Many
countries have participated in the COVAX scheme; however, it is difficult to
know which countries will drop out.
On the 4th of March 2021, Italy blocked a 250,000-dose shipment of
AstraZeneca vaccines going to Australia,95 becoming the first country to use
the bloc’s regulations to allow exports to be stopped if the company failed
to meet EU obligations. There was also a confrontation between London
and Brussels over a vaccine supply as the EU tried to block the movement
of EU produced vaccines from Ireland to Northern Ireland. The EU wanted
all its Member States to access these manufacturing lines, and if not, the EU
permitted its members to restrict the supply of any of their vaccines to the
UK.96 The UK government’s contract with AstraZeneca appears to have a
clause that protects the supply of pre-ordered vaccines under contract from
the NHS from being diverted to other countries.97
Bloc Positions/Key Stakeholders
Association of Southeast Asian Nations
ASEAN Member States responded to the COVID-19 pandemic by
implementing self-imposed measures and restrictions prior to the WHO’s
92
Eaton, “Covid-19: WHO warns against “vaccine nationalism” or face further virus
mutations.”
93
Ro, “Vaccine Multilateralism Is The Alternative To Vaccine Nationalism.”
94
WHO, “172 countries and multiple candidate vaccines engaged in COVID-19 vaccine
Global Access Facility.”
95
BBC, “Covid: Italy 'blocks' AstraZeneca vaccine shipment to Australia.”
96
Morris, “UK vaccine approval: Did Brexit speed up the process?”
97
BBC, “Covid: What’s the problem with the EU vaccine rollout?”
20WHO LIMUN 2021
declaration of the global pandemic outbreak. The way in which Members
responded to the virus varied initially. ASEAN states have faced challenges
to their individual health systems with countries such as Indonesia facing a
crisis. In the Philippines, it was acknowledged by health officials that limited
COVID-19 testing and already-challenged health systems could lead to
underreported infection rates in the region. Southeast Asian countries have
adapted their response to the virus, by converging their policies and
facilitating a united regional response. A region-wide response was initiated
as early as January 2020, followed by a statement from ASEAN Economic
Ministers in March 2020.98 In the statement, ministers agreed to strengthen
information share, collaboration and coordination in the region. As a result,
the ASEAN Centre on Public Health Emergencies and Emerging Diseases
was launched in November 2020, aiming to pool resources to fight COVID-
19 and future pandemics.99
China
In tandem with the WHO, the Chinese government downplayed the
severity of the COVID-19 outbreak, claiming there was “limited human-to-
human transmission.”100 The Chinese government initially denied the need
for “excessive actions”, particularly in the form of a PHEIC declaration and
travel bans aimed at Chinese nationals.101 By the time the virus began
spreading across Europe and the US, China had managed to assert control
over COVID-19. Despite the delay in reporting COVID-19 to international
health authorities, China had a relatively rapid and effective response in
curbing the effects of the pandemic, which was recognised by the WHO,
despite much backlash from the US.102 China’s centralised epidemic
response system meant that transmission speed was the first focussed on;
other measures including increased PPE production and a contact tracing
system were mobilised swiftly. At the 73rd WHA, China pledged to: provide
$2 billion in international aid, coordinate with the UN by providing a global
humanitarian crisis response hub, and provide any vaccine as a global
public good.103 Despite China’s promises on delivering a vaccine, they have
98
ASEAN, “Strengthening ASEAN’S Economic Resilience in Response to The Outbreak of
The Coronavirus Disease (COVID-19).”
99
Caballero-Anthony, “COVID-19 in Southeast Asia: Regional pandemic preparedness
matters.”
100
Mitchell et al., “China and Covid-19: what went wrong in Wuhan?”
101
Ibid.
102
Kelland and Mason, “WHO reform needed in wake of pandemic, public health experts
say.”
103
Idrus, “China ‘ready’ to include ASEAN in $2B COVID-19 aid.”
21WHO LIMUN 2021
faced scrutiny due to the lack of transparency surrounding data on their
vaccines. 104
Taiwan
On December 31st 2019, Taiwan health officials had asked for more
information from the WHO about the virus, seizing on reports coming from
a Wuhan hospital about patients with “SARS-like” symptoms and a new
coronavirus-like virus samples, as well as unconfirmed reports about
human-to-human transmission.105 Both Taiwanese and US officials later
emailed the WHO to argue that the ignored early warning from Taiwan
about human-to-human transmissibility of COVID-19 could be important.106
At the time, the WHO echoed Chinese health officials saying that there was
“no clear evidence of human-to-human transmission,”107 although cases
increased and suspicion about contagion was raised, as Taiwan continued
to indicate that the virus was transmitting human-to-human, thus
explaining the rise in cases in Wuhan. Leading on from this, on January
22nd 2020, the WHO passed a statement suggesting that human-to-
human transmission was present in Wuhan, but needed more evidence;
this was followed by China announcing a lockdown order on Wuhan the
next day (January 23, 2020).108 On the 30th of January, four countries had
evidence of human-to-human transmission; China, Japan, the United States
of America, and Vietnam, and on the 9th of February, the WHO published
considerations for quarantine to risk transmission.109 This exemplifies larger
issues, including the WHO’s response speed, trust in the WHO, and the open
sharing of information between other countries. If the information-share
about transmission was more transparent, the spread of COVID-19 might
have been contained. If countries had worked together, if Taiwan had been
able to share their information, or if COVID-19 was declared a global health
emergency or pandemic earlier, then this may have helped limit the spread
of COVID-19. For instance, Taiwan had also dispatched investigators to
Wuhan, bilaterally and not via the WHO, due to not being a member. Taiwan
had also banned flights from Wuhan and mandated 14-day quarantines.
However, Taiwan was unable to share this data and practices with the world.
104
Reuters Staff, “Piecemeal data releases threaten to undermine Sinovac's COVID-19
vaccine.” Reuters, December 28, 2020.
105
Watt, “Taiwan Says It Tried to Warn the World About Coronavirus. Here’s What It Really
Knew and When.”
106
Ibid.
107
Ibid.
108
Ibid.
109
WHO, "Listings of WHO’s response to COVID-19."
22WHO LIMUN 2021
The African Union
The African Union (AU) Member States prioritised addressing the
importation and containment of onward COVID-19 transmission. The Ivory
Coast was the first to implement travel surveillance measures as early as 2nd
January 2020, with other nations following suit.110 The Africa Centre for
Control and Prevention (Africa CDC) played a pivotal role in mobilising a
continent-wide response, initiating an emergency response meeting by
African health ministers on 22nd February 2020.111 This meeting yielded rise
to the Africa Joint Continental Strategy for COVID-19,112 led by the African
Task Force for Coronavirus. From this, the African Union demonstrated a
strong collaborative approach to tackling the pandemic as a region. 270
million COVID-19 vaccines were secured by the taskforce by January 2021,
marking the first batch of vaccines secured for a continent-wide effort.113
Aside from this, some African countries are eligible to receive donated
vaccines through COVAX, with the facility expected to provide 600 million
more vaccine doses for 20% of populations in African countries. 114
The Middle East & Israel
Middle Eastern nations have stark variations in resources, growth indices
and economic strengths. The region is plagued with violent conflicts which
have directly weakened health infrastructure. Problematically, there has
been little cooperation in the region, with the Arab League not addressing
the issue.115 Initially, countries in the region responded to the outbreak
individually. Iran, becoming an epicentre for COVID-19, were criticised for
underreporting cases initially; they cooperated with the WHO’s Regional
Office for the Eastern Mediterranean (EMRO) later.116 The WHO-EMRO was
pivotal in developing a response plan for Middle Eastern countries.
Both the Command and Control System and The Saudi Centre for Disease
Control and Prevention was developed in response to MERS-CoV, both of
which are leading faculties in the response to COVID-19, however, do not
integrate the entire region. There is still no evidence of collaboration and
cooperation in the Middle Eastern region to fight the pandemic. The UN has
110
Loembé et al., “COVID-19 in Africa: the spread and response.”
111
Ibid.
112
Ibid.
113
Jerving, Sara. 2021. “African Union secures first batch of COVID-19 vaccines.”
114
Ibid.
115
Sawaya et al., “Coronavirus Disease (COVID-19) in the Middle East: A Call for a Unified
Response.”
116
Ibid.
23WHO LIMUN 2021
been instrumental in providing assistance and coordinating small-scale
responses, instead.117
Israel provides a contrast to the rest of the region by leading the world in its
vaccination rollout; though, China has carried out vaccine research and
development with the United Arab Emirates, Egypt, Bahrain and Morocco
from the LAS.118 Israel, unlike many other countries in the Middle Eastern
region, has a strong public health infrastructure and was able to quickly
develop a mass vaccination plan.119 In November 2020, it was reported by the
World Economic Forum that Israel spent the most money on research and
development in the world, in terms of percentage of its gross domestic
product (GDP). Currently, Israel has vaccinated about 80% of its adult
population.120
However, Israel has faced criticism from the UN regarding their negative
stance on sharing their vaccine stockpile with the Palestinians. There is
debate as to whether Israel shoulders the responsibility of providing
vaccines to Palestinians in the West Bank and Gaza. Human rights groups
and Palestinians claim that Israel, as an occupying power, is responsible; the
UN cites the Fourth Geneva convention to support this. Israel argues that
under the Oslo Accords (agreed in 1993 and 1995), Palestinians have to take
care of their own health.121 From this case of Israel and Palestine, the
vaccination can be seen to be utilised as a political tool. The Deputy Regional
Director for the Middle East and North Africa at Amnesty International
highlighted “Israel’s COVID-19 vaccine programme highlights the
institutionalised discrimination that defines the Israeli government’s policy
towards Palestine.”122
United States of America
As the WHO’s largest donor, the US contributes approximately $450 million
in funding a year, forming 15% of the WHO’s budget.123 In particular, the US
played an important role in the 2005 reformation of the IHR.
117
Nasrawi, “Why no joint Arab response to Covid-19?”
118
MFA News. 2020. “China Holds a Webinar with the League of Arab States (LAS) on China's
Advanced Experience in Responding to the COVID-19's Impact on Economy.”
119
McKee and Rajan, “What can we learn from Israel’s rapid roll out of COVID 19
vaccination?”
120
Kellman, “Israel celebrates 5 millionth coronavirus vaccination.”
121
Reality Check, “Covid-19: Palestinians lag behind in vaccine efforts as infections rise.”
122
Amnesty International, “Denying COVID-19 vaccines to Palestinians exposes Israel’s
institutionalised discrimination.”
123
Nature, “Getting out of the World Health Organization might not be as easy as Trump
thinks.”
24WHO LIMUN 2021
On 29th May 2020, Trump announced that he would terminate funding to
the WHO, claiming that he thought the WHO was too lenient with China.124
Prior to the announcement, Trump sent a letter to the WHO’s director
general, Tedros Adhanom Ghebreyesus, threatening the halt of these funds
unless the WHO could “actually demonstrate independence from China” in
a period of 30 days.125
The Biden administration reversed Trump’s decision to withdraw from the
WHO on 20th January 2021.126 During the COVID-19 pandemic, the US has
deployed resources throughout the country and across the globe. The US
had also taken a hold of PPE as it was struggling with its own supply, aiming
to meet the demand, such as the FEMA (Federal Emergency Management
Association) seizing 50,000 N95 respirators without explanation.127 The
government had interfered with supply chains, taking the masks that were
needed for health workers for themselves.128
The US Government has announced more than $1.5 billion129 for USAID (U.S.
Agency for International Development), State Department, emergency
help, economic, humanitarian and development assistance. The aim is to
help governments, international organisations and NGOs (non-
governmental organisations) during the pandemic by saving lives,
improving public health education, aiding healthcare facilities, increasing
lab and disease-surveillance.130 The United States has been the largest
contributor to global health security and humanitarian assistance for more
than half a century, previously aiding with Ebola, HIV/AIDS, TB and Malaria.131
The US has made more than $20.5 billion available to aid the combat against
COVID-19, as well as supporting other partner countries.
United Kingdom and the European Union
An example of a bloc who are generally considered as adhering to
multilateralism, is the EU. With a reputation of backing (more specific)
mandates such as the Global Vaccine Alliance, the Global Fund and specific
programmes of the World Bank,132 their efforts in backing the WHO have
124
Maxmen, “What a US exit from the WHO means for COVID-19 and global health.”
125
Ibid.
126
Newey, “US will rejoin WHO in one of first acts of Biden presidency.”
127
Bland, “I sent masks to health workers but the Trump administration seized them
instead of helping.”
128
Ibid.
129
US Department of State, “Foreign Assistance for Coronavirus (COVID-19).”
130
Ibid.
131
USAID, “USAID'S COVID-19 RESPONSE.”
132
van Schalk, Jørgensen, and van de Pas, “Loyal at once?”
25WHO LIMUN 2021
been lacking. Pre-COVID-19, funding for the WHO primarily came from
development cooperation budgets, with the EU not especially keen on
funding large global health programmes.133 Early fractures in a potential
multilateral response occurred as early as February 2020; Italy requested
medical equipment via the activation of the EU’s Protection Mechanism.
Little sympathy was shown by Member States, with some (such as France
and Germany) responding by, initially, banning the export of medical
equipment.134 This was exemplified when China sent support to Italy, while
their EU partners ignored them. The uncoordinated efforts of national
governments undermined the core functions of the EU in the early stages
of the pandemic. Despite adaptations towards a collaborative approach,
violations of EU policy have been seen by some Member States, with
Germany most recently striking a deal with Pfizer/BioNTech in order to
secure 30 million more doses of the vaccine, outside of the EU-wide deal.135
This is a clear breach of the common EU strategy, highlighting fractures
within the EU’s multilateral approach.
The EU has slowed virus transmission inside and outside the EU through
coordinated travel restriction,136 safeguarding frameworks, agreeing
information, publishing travel measures, and providing reliable up to date
information,137 helping countries to make coordinated decisions based on
the epidemiological situation. Vaccination started in the EU on the 27th of
December 2020,138 however there has been criticism for the slow EU vaccine
rollout, and claims that delays have cost lives.139 Many countries have sent
teams of doctors to treat patients, send ventilators, and share vaccine doses,
further funding €800 million to Member States to help them fight the
pandemic.140
Locking down as late as March 23rd, 2020, the country had been relatively
slow to move into lockdown compared to other countries. However, the UK
has arguably helped decrease the spread of COVID-19 through vaccine
collaborations such as Oxford AstraZeneca, expecting to produce 2 billion
133
Steurs et al., “The Global Health Policies of the EU and its Member States: A Common
Vision?”
134
Gostyńska-Jakubowska and Scazzieri, “THE EU NEEDS TO STEP UP ITS RESPONSE TO
THE COVID-19 OUTBREAK.”
135
Newkey-Burden, “Germany ‘violates’ EU joint vaccine scheme by buying 30 million extra
doses.”
136
Ibid.
137
Council of the European Union, “10 things the EU is doing to fight COVID-19 and ensure
recovery.”
138
Ibid.
139
Ellyatt, “A year on, Europe faces slow Covid vaccine rollouts and fears of another wave.”
140
Ibid.
26You can also read