LSL Sexual Health Strategy 2018-2021 Initial consultation event - 15 December 2017 - NHS Lambeth CCG
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

LSL Sexual Health Strategy 2018-2021
Initial consultation event
15 December 2017
Lambeth, Southwark, and Lewisham Public Health
Slide 1
AGENDA
10:00 Welcome
Jennifer Reiter
10:10 Current picture of sexual and reproductive health in LSL
Kirsten Watters
10:25 Reflection on 2014-17 strategy and achievements / challenges
Ruth Hutt
10:40 Overview of 2018-21 strategy
Kirsten Watters
10:45 Audience Q&A
10:55 Comfort break
11:05 Break-out groups and feedback
12:15 Next steps
12:30 Close
Slide
Slide 2 2Sexual and reproductive health in LSL
Kirsten Watters
Consultant in Public Health, Southwark Council
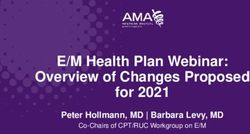
Slide 3LSL have among the highest rates of new STI
diagnoses in London
High levels of need
3,500
New sexually transmitted infection (STI) diagnoses (excluding chlamydia in under 25 year
olds) per 100,000 population aged 15 to 64
3,000
2,500
2,000
1,500
1,000
500
0
1. PHE Fingertips – Sexual and Reproductive Health Profiles - 2016 Slide 4New STI diagnoses are high but falling and testing
rates increasing
New diagnoses (excl chlamydiaThere is a social gradient within sexual health
New STI rates by deprivation decile in 2016
London average
Most deprived
Second most deprived
Third most deprived
Forth most deprived
Fith most deprived
Fith less deprived
Forth less deprived
Third less deprived
Second less deprived
Least deprived
0 200 400 600 800 1000 1200
1. PHE Fingertips – Sexual and Reproductive Health Profiles Slide 6Men are more likely to be reinfected than women; this
gap is greater in LSL than nationally
THE GENDER GAP
Reinfection with a new STI within 12 months of new STI dx at a specialist SHC in 2015
18.3
15.5
13.6
9.7 9.3 Men
7.3 7.1 Women
6.7
Lambeth Southwark Lewisham National
1. PHE (2015) LASER Reports for Lambeth, Southwark, and Lewisham Slide 7Women aged 15-24 are more likely to be reinfected with
an STI compared to the wider female population
STI DIAGNOSES & REINFECTION
Proportion (%) of new STI diagnoses at Proportion (%) of young people (aged 15-24) re-infected
specialist SHC that were in young people aged with a new STI within 12 months
15-24
37
19.7 20.2
26
15
14 13.7 14.3
19 Men
Women
Lambeth Southwark Lewisham Lambeth Southwark Lewisham
1. PHE (2015) LASER Reports for Lambeth, Southwark, and LewishamYoung people generally suffer from poorer sexual health
OVERVIEW
With respect to chlamydia screening in young people aged 15-24:
Lambeth performs well – 50.0% of young people screening in 2016
Slightly lower in Southwark (41.2%) and Lewisham (41.9%)
This compares to 27.4% across London
Chlamydia screening rates relatively stable in Lambeth and Southwark, but falling in
Lewisham
We have been hugely successful in reducing teenage conceptions and maternities:
Reduction in teenage conceptions 1998-2015:
Lambeth: -66%
Southwark: -72%
Lewisham: -71%
However, the burden of poor sexual health is still disproportionately on young
people, who have the highest rates of new STI diagnoses and highest rates of re-
infection.
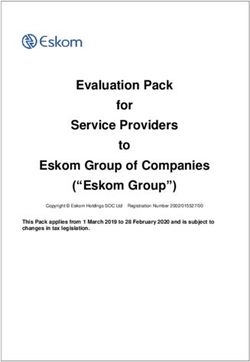
1. PHE Fingertips – Sexual and Reproductive Health Profiles - 2016 Slide 9Repeat abortion rates in young women remain higher
than the national average
REPRODUCTIVE HEALTH
Repeat abortion rate in young women aged 15-24
38.0
36.0
34.0
32.0
30.0
28.0
26.0
24.0
22.0
20.0
2012 2013 2014 2015 2016
Lambeth Southwark Lewisham London England
1. PHE Fingertips – Sexual and Reproductive Health ProfilesPoor reproductive health is a cause of health inequalities
INEQUALITIES
There is a social gradient as a consequence of poor reproductive health.
Rates of admission for pelvic inflammatory disease and rates for ectopic pregnancy
are 30% higher in most deprived decile than least deprived.
The abortion rate (all ages) is 46% higher in the most deprived decile than the least
deprived decile
The rate of prescribed LARC is lower in LSL than in England (but higher than the
London average), and across England, GPs prescribe LARC 56% less to women in
the most deprived decile, compared to women who are in the least deprived decile
The rate of LARCs prescribed in a primary care setting in LSL is falling
Slide 11In Southwark and Lewisham, HIV diagnoses continue to
fall, in line with the national picture
DIAGNOSES & PREVALENCE
New HIV diagnosis rate / 100,000 aged 15+ HIV diagnosed prevalence rate / 1,000 aged 15-59
2011 2012 2013 2014 2015 2016 2011 2012 2013 2014 2015 2016
Lambeth Southwark Lewisham London England Lambeth Southwark Lewisham London England
1. PHE Fingertips – Sexual and Reproductive Health ProfilesMSM are disproportionately affected by HIV
NEW DIAGNOSES BY EXPOSURE CATEGORY
New diagnoses by exposure category in LSL from 2011-2015
Sophie Nash, Dana Ogaz, Martina Furegato, Peter Kirwan, Bethan Swift, Alison Brown and
Valerie Delpech on behalf of the GUMCAD & HARS teamThe proportion of HIV diagnosed at a late stage has
decreased since 2011
LATE DIAGNOSES
Southwark and Lewisham have a higher proportion of heterosexual transmission and as a result, have a
higher proportion of late diagnoses.
HIV late diagnoses (%)
60
50
40
30
20
10
0
2011 2012 2013 2014 2015 2016
Lambeth Southwark Lewisham London England
1. PHE Fingertips – Sexual and Reproductive Health ProfilesThe demography of late diagnoses has fluctuated over
recent years
LATE DIAGNOSES - MSM LATE DIAGNOSES - HETEROSEXUALS
HIV late diagnoses in MSM by ethnicity (%) HIV late diagnoses in heterosexuals by sex (%)
Sophie Nash, Dana Ogaz, Martina Furegato, Peter Kirwan, Bethan Swift, Alison Brown and
Valerie Delpech on behalf of the GUMCAD & HARS team94% of people with diagnosed HIV in LSL are on treatment
but more can be done to engage people in care
HIV TREATMENT
Proportion of people diagnosed with
HIV who were receiving treatment in
2016:
Lambeth: 95%
Lewisham: 94%
Southwark: 93%
In 2014/15, there were 78 people in LSL who had been diagnosed with HIV but
were not engaged in care.
Sophie Nash, Dana Ogaz, Martina Furegato, Peter Kirwan, Bethan Swift, Alison Brown and Valerie Delpech on
behalf of the GUMCAD & HARS teamA focus on Syndemics to reframe how we think and act
THE WIDER PICTURE
• Syndemics – two or more co-existent conditions which interact to produce
and excess burden of disease within a particular group.
• Negatively impact the trajectory of each disease and enhances
vulnerabilities to other conditions.
• Better identify and understand these interacting factors for sexual health
and HIV.
Social
exclusion
Poor
mental
health
HIV
tWilson, Patrick A. et al. “Using Syndemic Theory to Understand Vulnerability to HIV Infection among Black and
Latino Men in New York City.” Journal of Urban Health : Bulletin of the New York Academy of Medicine 91.5
(2014): 983–998. PMC. Web. 14 Dec. 2017. Slide 17Sexual health in LSL
SYNOPSIS
STI rates in LSL are the highest in London/England but are falling and
testing rates are increasing.
There are persistent inequalities in sexual and reproductive health.
Key groups continue to shoulder the greatest burden of poor sexual and
reproductive health: young people, BME, MSM.
Access to reproductive health care needs improvement – especially in
primary care.
The epidemiology of HIV is changing – need to focus on increasing testing,
especially in heterosexual groups, and engaging vulnerable groups in care.
Late diagnoses are entirely preventable!
Slide 18Reflections on LSL sexual health
strategy 2014-17
Ruth Hutt
Interim Director of Public Health, Lambeth Council
Slide 19Overview
LSL Sexual Health Strategy 2014-17 four years later…
Changing context
Epidemiology
Financial climate
Service models
What we set out to achieve
Have we been successful?
Slide 202014-17 strategy recap
VISION
To improve sexual health in LSL by building effective, responsive
and high quality sexual health services, which effectively meet the
needs of our local communities.
Slide 212014-17 strategy recap
STRATEGY DRIVERS (2013/14)
Epidemiology
Finances
Prevention
Slide 222014-17 strategy recap
KEY PRINCIPLES
Key principles in development of 2014 strategy:
Identifying those at highest risk
Men who have sex with men
Young people
Black & Minority ethnic communities
Involving service users in all aspects of strategy development
Utilise technology to improve and reshape services
Making every contact count
Slide 232014-17 strategy recap
KEY AIMS
Reducing stigma associated with sexual health
Focusing on those statistically most at risk of poor sexual health, thereby
reducing inequalities
Reducing rates of undiagnosed STIs and HIV
Reducing the rates of unplanned pregnancy and repeat terminations,
especially for under 18s
Developing the workforce to deliver integrated and improved services
Commission a range of world class services from self-management to
complex and specialist care
Commissioning to improve cost effectiveness and outcomes
Slide 242014-17 strategy recap
WE DID NOT…
Imagine we would achieve the 90>90>90 targets
Predict a drop in new HIV/STI diagnoses
Expect the cuts to the public health grant
Imagine cooperation across 32 London Boroughs
Imagine that NHSE would not yet have completed the review of HIV
services…
Slide 25How did we do?
SERVICE REDESIGN
We said: We did:
We would explore a range of Support development of online STI
alternative service models services
including online Committed to working with partners
Appraise options for implementing and London SHTP to deliver ISHT
Integrated Sexual Health Tariff Reviewed Primary care provision
Review sexual health provision in Yet to fully implement changes
primary care
Slide 26How did we do?
PREVENTION
We said: We did:
We would aim to shift investment into Commission LSL sexual health
prevention promotion service – RISE
Commission modernised, evidence Developed new models of
based sexual health promotion and HIV integrated delivery of substance
prevention services targeted at MSM, misuse, sexual health & mental
BME communities & vulnerable young health for young people
people
Maintain and develop prevention
approaches outside sexual health
settings
Slide 27How did we do?
HIV
We said: We did:
We would maximise opportunities to Introduce HIV testing in hospitals,
test for HIV outside of SH services primary care & psychiatry
Look at provision of home sampling Support SH24 implementation &
for most at risk communities National HIV testing programme
Increase awareness of benefits of Lead London HIV Prevention
testing & reduce stigma as part of a Programme
London-wide programme Implement the final stages of the
Lead a London HIV prevention 2010 HIV care and support review
programme
Fully implement the HIV care and
support review recommendations
Slide 28How did we do?
WORKFORCE
We said: We did:
We would work with providers to… Introduce different skill mix
review skill-mix Provided Sexual Health in
ensure their workforces are trained Practice Training to 100s of
and standards continuously improve primary care staff
consolidate sites Consolidated sites for delivery of
services
Train community champions in
sexual health
Slide 29Key achievements
LSL have been leaders in London.
Proof of concept and model of online testing
Integrated services across the system
Prevention programmes
Innovative & collaborative young people’s services
Working with communities
Outcomes:
Teenage pregnancy rates declining
HIV late diagnosis falling
STI rates falling
Chlamydia screening stable
Abortion rates stable
Slide 30What is still a work in progress?
Inequalities
Access
Shifting investment into prevention
Mainstreaming of HIV testing
Primary care development
Self-care
Post-natal contraception
Sex and relationships education
Slide 31Overview of 2018-21 LSL strategy
Kirsten Watters
Consultant in Public Health, Southwark Council
Slide 322018-21 Strategy
BACKGROUND
Why do we need a strategy for the coming years?
Continuing but changing challenges
New opportunities, PrEP, Statutory RSE, technological innovations, ACOs (?)
Why do LSL work in partnership to improve sexual and reproductive
health?
We want to align action across the system and to do this we need a shared
and clear strategic direction for action
What do we want to do differently?
We really want to tackle the wider determinants of sexual health and upgrade
prevention
We can’t do this in isolation and recognise the importance of links to existing
strategies
Slide 332018-21 Strategy
PRIORITIES
Our Priorities
Safe and Good High quality Living well
healthy reproductive STI testing with HIV
relationships health and
across the treatment
life course2018-21 Strategy
PRINCIPLES
Our Principles
Working in High quality Listening to service Focus on reducing Supporting the
partnership, at a commissioning for users’ views and inequalities in development of a
local, London and effective and experiences and sexual and resilient sexual
national level financial sustaining using these to reproductive health health system
services, including improve what we
capitalising on do
technological
innovationsPriority Good Reproductive Health High Quality STI Testing and
Safe and Healthy Relationships Living Well with HIV
Across the Life Course Treatment Services
▪ In control of their body and fertility
▪ Increased HIV testing
What does ▪ Knowledge, confidence and skills ▪ Understand what factors impact ▪ Self-sampling of STIs
for safe, healthy and fulfilling ▪ Access to appropriate testing ▪ Earlier diagnosis
good look on fertility
relationships ▪ High quality clinical services ▪ Retention in care
like? ▪ Choice and access to a range of
▪ Holistic health management
contraceptive methods
Commissioner
Reducing stigma and promoting
High quality SRE in schools High quality SRE in schools High quality SRE in schools
good sexual health
Community outreach / targeted
Targeted work to young people Young people friendly services Young people friendly services
health promotion work
Council
Tackling homophobia, Knowledge of and access to full Come Correct condom scheme for
Online STI self-sampling or testing
transphobia, misogyny in communities range of contraceptive offers under-25s
Community outreach / targeted Come Correct condom scheme for Integrated reproductive and sexual
Online STI self-sampling or testing
health promotion work under-25s health services
Integrated reproductive and sexual Integrated reproductive and sexual
Targeted CHEMSEX work
health services health services
Specialist clinical services
Psycho-sexual health services Online offer of oral contraception Pharmacy and primary care testing Pharmacy and primary care testing
Council &
CCG
Pharmacy and primary care
FGM prevention
High quality abortion services Care and Support
CCG
Vasectomy and sterilisation
services
HPV vaccination PrEP HIV treatment services
NHSE
Cervical screening2018-21 Strategy
How will it work in reality?
Complex commissioning and provider environment + cross sectorial and
organisation action = difficult
Balance between shared and local
Within each of our pillars, we will develop shared outcomes and focuses for
improvement
However, how each borough will prioritise and focus their actions will vary
according to the local context and need
We want this to be a strategy which supports action and detailed action plans
will be developed within each pillar on an annual basis
This is just the start of the consultation process…
Governance matters – Transparent, Accountable, Participatory, Integrated,
Capacity
Slide 37Table discussions and feedback
Slide 382018-21 Strategy
QUESTIONS
1. Do you agree with our four pillars (priorities)?
2. What does ‘good’ look like in each of our four pillars?
3. In each of the four pillars, where should we aim to be at the end of the three-
year strategy period?
4. How does our proposed strategy align with your work? Are there relevant
local strategies we should align with?
Slide 39Priority Good Reproductive Health High Quality STI Testing and
Safe and Healthy Relationships Living Well with HIV
Across the Life Course Treatment Services
▪ In control of their body and fertility
▪ Increased HIV testing
What does ▪ Knowledge, confidence and skills ▪ Understand what factors impact ▪ Self-sampling of STIs
for safe, healthy and fulfilling ▪ Access to appropriate testing ▪ Earlier diagnosis
good look on fertility
relationships ▪ High quality clinical services ▪ Retention in care
like? ▪ Choice and access to a range of
▪ Holistic health management
contraceptive methods
Commissioner
Reducing stigma and promoting
High quality SRE in schools High quality SRE in schools High quality SRE in schools
good sexual health
Community outreach / targeted
Targeted work to young people Young people friendly services Young people friendly services
health promotion work
Council
Tackling homophobia, Knowledge of and access to full Come Correct condom scheme for
Online STI self-sampling or testing
transphobia, misogyny in communities range of contraceptive offers under-25s
Community outreach / targeted Come Correct condom scheme for Integrated reproductive and sexual
Online STI self-sampling or testing
health promotion work under-25s health services
Integrated reproductive and sexual Integrated reproductive and sexual
Targeted CHEMSEX work
health services health services
Specialist clinical services
Psycho-sexual health services Online offer of oral contraception Pharmacy and primary care testing Pharmacy and primary care testing
Council &
CCG
Pharmacy and primary care
FGM prevention
High quality abortion services Care and Support
CCG
Vasectomy and sterilisation
services
HPV vaccination PrEP HIV treatment services
NHSE
Cervical screeningNext steps…
Slide 41LSL Sexual Health Strategy 2018-2021
Initial consultation event
Thank you
Lambeth, Southwark, and Lewisham Public Health 15 December 2017
Slide 42You can also read