Lung cancer screening: the cost of inaction - Lung Ambition ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Lung cancer screening: the cost of inaction July 2021 This report was developed for the Lung Ambition Alliance by The Health Policy Partnership and endorsed by the International Association for the Study of Lung Cancer. It was initiated and funded by AstraZeneca, a founding partner of the Lung Ambition Alliance.

Lung cancer screening: the cost of inaction
2
Table of contents
Executive summary 3
1 Introduction 7
2 Lung cancer: a public health priority 9
3 Earlier detection: the key to reducing the burden 12
of lung cancer
4 LDCT screening for lung cancer: the next big opportunity 18
in cancer detection
5 An investment in health system sustainability 21
6 Ensuring successful implementation of lung cancer 24
screening at scale
7 Conclusions 32
References 33
Appendix 1. Synthesis of published cost-effectiveness 40
studies on LDCT screening
Lung cancer screening: the cost of inaction
3
Executive summary
Lung cancer is the leading cause of cancer lung cancer deaths by sex, with mortality
deaths worldwide, accounting for one in rates mostly rising among women in
five cancer deaths.1 Smoking is the major many countries.8 With all these factors
cause of lung cancer, but lung cancer is combined, the number of people with lung
not just a smokers’ disease. Global rates cancer is likely to remain significant for
of smoking have been gradually declining decades to come.
in men, but have remained stable, or
decreased at a slower rate, in women.2 Governments around the world have
Former smokers, however, remain at high committed to reducing the burden
risk of lung cancer up to 25 years after of cancer, but few countries are on
quitting.3 In addition, the prevalence of target to meet their goals. Lung cancer
lung cancer in never-smokers is gradually accounts for the greatest economic and
rising: in the UK and US, around 20% of public health burden of all cancers.9
lung cancers occur in people who have It is responsible for nearly a quarter of
never smoked, and this figure is about productivity losses due to premature
53% in some Asian countries.4-7 There is mortality from cancer in Europe.10 Targeted
also a global shift in the distribution of efforts on lung cancer must therefore
Lung cancer screening: the cost of inaction
4
Lung cancer accounts for the reduction in the number of deaths from
lung cancer. This will have a substantial
greatest economic and public health impact on cancer mortality more generally
burden of all cancers. and, in turn, will dramatically decrease the
economic toll of cancer on our societies.
Earlier detection through screening
may transform lung cancer from a
be an integral part of all national cancer fatal to a treatable condition, with
control plans if countries wish to achieve considerable impact on quality of life.
their goals and reduce the toll of cancer The most effective means of achieving
on their societies. this shift is through targeted screening
using low‑dose computed tomography
Early detection that allows people (LDCT).18 19 Evidence from large-scale
rapid access to high-quality diagnosis clinical trials has shown that targeted LDCT
and care offers the best opportunity screening can reduce lung cancer deaths in
to reduce the number of deaths due high risk individuals by nearly a quarter.18 19
to lung cancer. Prognosis for lung Given that approximately 1.8 million lives
cancer is poor compared with most are currently lost to lung cancer every
other cancers,11-13 largely due to a high year,1 this would have a considerable public
proportion of cases being detected health, economic and societal impact.
at an advanced stage when treatment
options are limited.14 Around 20% of In light of this evidence, it is time for
people with lung cancer are diagnosed at national governments to consider
stage I, when their likelihood of surviving large‑scale implementation of targeted
5 years is between 68–92%, compared lung cancer screening. Lung cancer
with more than 40% of people being screening should be considered the next
detected at stage IV, when their likelihood big opportunity in cancer screening:
of surviving 5 years is under 10%.15-17 experts suggest it compares favourably
The proportion of people detected at with other cancer screening programmes
an advanced stage varies considerably in terms of cost-effectiveness and
by country. Shifting detection to earlier potential benefits,20 and fewer people
stages could thus result in a considerable need to be screened for lung cancer to
prevent one death compared to breast
or colorectal cancer screening.19 21 22
What’s more, a decade of implementation
research around the world has pointed to
Lung cancer screening should be factors that can help ensure successful,
cost‑effective implementation at scale.
considered the next big opportunity Of highest importance is the need
in cancer screening to secure attendance from people at
Lung cancer screening: the cost of inaction
5
Figure a. The impact of lung cancer screening extends beyond lung cancer
Reduced health inequalities
in lung cancer (in terms of
risk of late presentation,
access to appropriate
treatment and care, survival)
Complement to Targeted lung cancer
screening and broader Reduced loss of
smoking cessation
early detection productivity and fewer
policies, contributing to
premature deaths due to
creating a tobacco free Coupled with rapid access lung cancer
generation to expert diagnosis and
multidisciplinary care
Early detection of other
non-communicable diseases
(e.g. chronic obstructive
pulmonary disease,
cardiovascular disease)
Enhanced sustainability Contribution to
of healthcare systems through reduced mortality from
lower costs of care non‑communicable diseases
greatest risk of lung cancer, to optimise The benefits of investing in the early
the balance of benefits and harms from detection of lung cancer extend beyond
screening, and to integrate targeted lung cancer (Figure a). Screening
screening programmes into high-quality presents an opportunity to detect other
multidisciplinary care pathways, with early non-communicable diseases, such as
diagnosis and effective treatment options cardiovascular disease and chronic
available for all. obstructive pulmonary disease, at an early
stage in high-risk individuals.23-25 It can also
Lung cancer screening: the cost of inaction
6
The need to invest in early detection and the backlog of cases the pandemic
has created will undoubtedly exacerbate
has never been more urgent the risk of late presentation for months to
come.29-34 In England, for example, delays
in diagnosis due to COVID-19 are expected
to result in an 11.2% increase of stage IV
diagnoses of lung cancer,35 and similarly
help reduce health inequalities: people of worrying trends are emerging in other
lower socioeconomic status are at highest countries.29 36
risk of lung cancer, of presenting late
with symptoms, and of poor survival as Time is everything for people with lung
a result.26-28 cancer. As systems rebuild following the
pandemic, the need to invest in early
Investing in early detection of lung detection has never been more urgent.
cancer is also an investment in the future Failing to do so condemns lung cancer
sustainability of our health systems and patients to poor survival and diminished
post-pandemic recovery. The COVID-19 quality of life, and increases the long-term
pandemic has had a dramatic impact on the strain on overstretched, under-resourced
entire lung cancer care pathway – including health systems.
initial presentation, diagnosis and access to
treatment – and there is growing evidence Leadership as we emerge from the
that it is undoing some of the progress in pandemic means acting early – the time
lung cancer survival achieved in recent to act is now. The cost of not doing so is
years.29 Across many countries, screening too great, not just for lung cancer patients,
and urgent referrals have declined sharply, but for society as a whole.
Lung cancer screening: the cost of inaction
7
1 Introduction
Lung cancer is the leading cause of cancer is the main cause of lung cancer. In most
deaths worldwide. More than 2.2 million countries, smoking rates have declined
people were diagnosed with lung cancer in among men but remained stable or
2020i, making it the second most commonly decreased at a slower rate among
diagnosed cancer worldwide after breast women.2 However, a former heavy smoker
cancer.1 Approximately one in five cancer remains at three times greater risk of
deaths globally is due to lung cancer,37 and developing lung cancer than a person
the five-year survival rate was just 10–20% in who has never smoked, and this risk
most countries between 2010–2014.11 remains for up to 25 years after quitting
smoking.3 In addition, lung cancer is not
Despite falling smoking rates, the just a smokers’ disease and its frequency
prevalence of lung cancer is expected among never-smokers is rising globally.5
to remain high for many years. Smoking In the UK and US, around 20% of lung
i In this report we have used the most recent data available (2020). While it is possible that this number is underestimated due to
under-reporting of cases during the COVID-19 pandemic, figures for 2020 are as expected based on current epidemiological
trends, and comparable to data from earlier years.
Lung cancer screening: the cost of inaction
1 Introduction 8
cancers occur in people who have never that targeted screening of former and
smoked, and this rate is 53% in some Asian current smokers by low-dose computed
countries.4-7 There is also a global shift tomography (LDCT) can significantly reduce
in the distribution of lung cancer deaths deaths from lung cancer.18 19 Given that
by sex, with mortality rates mostly rising lung cancer currently kills approximately
among women in many countries.8 With all 1.8 million people worldwide every year,1
these factors combined, lung cancer will this impact would be considerable. But the
remain an important public health problem COVID-19 pandemic has halted translation
for decades to come. of clinical trial evidence to real-world
implementation of screening programmes
The link with smoking has caused in many countries. The pandemic has also
widespread stigma towards people with caused significant disruption to diagnosis
lung cancer. Such stigma is felt equally and care of people with lung cancer,
by people who do or have smoked and making the need to reduce the burden
those who have not.38 Many studies have of this condition on our societies much
shown that the emotional burden caused more urgent.
by a lung cancer diagnosis is considered
to be significantly higher than for other As we emerge from the COVID-19
cancers, and stigma is a big part of this.38-42 pandemic, we are faced with a unique
Lung cancer has also traditionally received opportunity: to find the most feasible
less attention and funding than other approach to reducing mortality from lung
common cancers, despite its overwhelming cancer. Investment in early detection, with
economic and societal impact.43 screening at its core, must be part of that
effort if we are to reduce the devastating
Many governments have set targets to costs of lung cancer on people, economies
improve survival from cancer over the next and health systems. This report explores
20 years.44 45 As lung cancer is the biggest not just why this is something that should
cancer killer, strategies to reduce lung be done, but the immense cost to society
cancer mortality must be part of efforts to of not doing so.
achieve those targets.37 The most effective
way to do this is through early detection,
specifically screening.
It is recommended that screening for
lung cancer take a targeted approach,
focusing on people at highest risk of lung
cancer. In 2020, the publication of the
Dutch–Belgian Randomised Lung Cancer
Screening Trial (NELSON) confirmed the
findings of the US National Lung Screening
Trial (NLST) more than a decade before,
Lung cancer screening: the cost of inaction
9
2 Lung cancer:
a public health priority
Reducing cancer deaths is a global of countries are on track to achieving
imperative target reductions in the major NCDs,46
Cancer is one of the greatest public which include cancer, and only 12
health issues of our time. Globally, countries worldwide are currently on track
it is responsible for one in six deaths to achieving specific targets to reduce
and a third of premature deaths from cancer mortality.37 One in five people still
non‑communicable diseases (NCDs) faces a cancer diagnosis before the age of
in people aged 30– 69.37 As part of their 75,37 and in 2020, 10 million people died
commitment to reducing mortality from from cancer.47
NCDs,46 many countries around the world
have set targets to specifically achieve Lung cancer presents a considerable
10‑year survival in three out of four of public health and economic burden
cancer patients by 2030.44 45 Lung cancer is the leading cause of
cancer deaths globally. One in five cancer
Despite these commitments, we are a deaths is due to lung cancer, and it causes
long way from effectively tackling the approximately 1.8 million deaths per year
global burden of cancer. Fewer than 10% (Table 1).1Lung cancer screening: the cost of inaction
2 Lung cancer: a public health priority 10
Table 1. The public health impact of lung cancer: key facts and figures
Globally, lung cancer is responsible for:
• 2.21 million new cases per year1 • 1.8 million deaths per year1
• 11.4% of all new cancer cases1 • 18% of all cancer deaths1
• 45.9 million disability-adjusted life years (2019)48 • 45.3 million years of life lost (2019)48
South
North America &
Region* Europe America Caribbean Africa Oceania Asia
New lung cancer cases 477,534 253,537 97,601 45,988 16,975 1,315,136
per year
New cases as % of total 10.9% 9.9% 6.6% 4.1% 6.7% 13.8%
regional cancer cases
Lung cancer deaths 384,176 159,641 86,627 41,171 12,012 1,112,517
per year
Deaths as % of total 19.6% 22.8% 12.1% 5.8% 17.3% 19.2%
regional cancer deaths
* Continental regional data reported by the World Health Organization Global Cancer Observatory (2020) 47
Table 2. Lung cancer costs in the European Union (based on 2009 data)49
Costs of Lung cancer
All cancers % of all lung cancer % of lung as % of all
Costs per year (billion €) cancer costs (billion €) cancer costs cancer costs
Total costs 126.2 100% 18.8 100% 15%
Direct healthcare costs 51.0 40.4% 4.2 22.5% 8%
Productivity losses 42.6 33.7% 9.9 52.8% 23%
(early death)
Productivity losses 9.4 7.5% 0.8 4.3% 9%
(lost working days)
Informal care 23.2 18.4% 3.8 20.3% 16%
Lung cancer has the highest economic toll Existing figures date back several
of all cancers. In Europe, the costs of lung years, however, and more up-to‑date
cancer are higher than breast, colorectal or estimates are needed to understand
prostate cancer9 and represent 15% of the the full economic toll of lung cancer on
total economic costs of cancer (Table 2).49 our societies.Lung cancer screening: the cost of inaction
2 Lung cancer: a public health priority 11
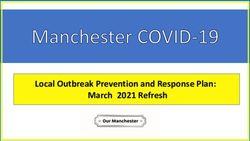
Figure 1. Lung cancer accounts for nearly a quarter of productivity losses due to premature
mortality in Europe, more than any other cancer type10
Lung €17.5bn(23%)
Breast €6.9bn (9%)
ng
Lu
Ot
her Colorectum €6.3bn (8%)
Brain + CNS €4.2bn (6%)
Pancreas €3.9bn(5%)
Stomach €3.3bn(4%)
Brea s
t Oesophagus €2.7bn (4%)
L Liver €2.4bn(3%)
NH Co
lo Leukaemia €2.4bn (3%)
ia
re
m
c tu NHL €1.9bn(3%)
r
ae
ve
m
uk
us
Bra
Li
ch
Pancreas
Le
Other €23.9bn(32%)
hag
in +
Stoma
s op
CN
Oe
S
CNS, central nervous system; NHL, non-Hodgkin’s lymphoma
The indirect costs of lung cancer, in on people’s quality of life. In most
terms of productivity losses and informal countries, it is responsible for the most
care, are particularly significant. These disability-adjusted life years (DALYs) of all
costs outweigh direct healthcare costs cancers.43 Symptoms like breathlessness
in published studies.49 50 Lung cancer’s and fatigue, along with the need to
impact on productivity is considerable:50 attend medical appointments or adapt
it accounts for nearly a quarter (23%) of to treatment regimens, may lead to
productivity losses due to premature social withdrawal and time off work.39
mortality from cancer in Europe, a The psychological distress, impact of
higher proportion than any other cancer cancer treatment and related side effects
(Figure 1).10 Many people with lung cancer substantially affect the mental health
stop working and do not return, resulting and wellbeing of people living with
in significant cost of early retirement to lung cancer and their loved ones.39 51
individuals, their families and the economy. The day‑to-day impact on loved ones
is also significant,52 with lung cancer
In addition to its high financial costs, accounting for 16% of total costs of all
lung cancer also has a dramatic impact informal cancer care.49Lung cancer screening: the cost of inaction
12
3 Earlier detection: the key to
reducing the burden of lung cancer
Late presentation is a significant issue common cancers.11 13 Progress in survival
in lung cancer for lung cancer has paled in comparison
Earlier detection is recognised as the best with that seen in some other cancers
way to reduce the burden of all cancers – (Figure 2).13 54 For example, in England in
but lung cancer is seldom detected early. 2018, half of lung cancers were diagnosed
Symptoms such as a persistent cough, at stage IV (50%), compared to 5% of breast
shortness of breath and repeated lung cancers and 25% of colorectal cancers.16
infections are often difficult for people to Although precise estimates vary by country,
recognise as symptoms of lung cancer.14 trends are similar.
As a result, many people present to
healthcare professionals only after their Shifting detection to an earlier stage
cancer has advanced to a stage where could transform lung cancer from a fatal
treatment options are limited and prognosis to a treatable condition. Prognosis for
is poor.14 53 lung cancer is highly dependent on the
stage at which the illness is diagnosed
Late presentation in lung cancer has led to (Figure 3). A person diagnosed with stage
poor survival compared with some other IV lung cancer has less than 10% chanceLung cancer screening: the cost of inaction
3 Earlier detection: the key to reducing the burden of lung cancer 13
Figure 2. Improvements in lung cancer survival have lagged-behind those seen in other
common cancers (US data)12 13 54 55
5 year relative survivala
1975–1977 2008–2014
All cancers 69.2%
Prostate 98.9%
Breastb 91.1%
Colorectal 66.2%
Lung 19.9% 9–15% across Europe, generally < 20% globally
a Five-year
relative survival rates show the percentage of people who will be alive five years after diagnosis.
This does not include people who die from other diseases. Relative survival rates account for the fact that not all
people diagnosed with a certain cancer type will die of that cancer.
b Women only. Data: https://seer.cancer.gov 54
of surviving five years after diagnosis; this Early detection of lung cancer would
increases to between 68–92% if diagnosed have a significant economic impact
at stage I.17 At stage I, patients can be Shifting detection to an earlier stage
offered surgical removal (resection) with would significantly reduce the total costs
a high probability of cure,56 as well as of lung cancer. The costs of treating a
other curative treatments, avoiding the person with late-stage lung cancer are
need for more invasive and less effective higher than for earlier-stage disease due
interventions later on, with considerable to more complex pathways for clinical
impact on quality of life.57 management.14 60 61 With earlier detection,
more people will be able to remain active
Earlier detection of lung cancer would and return to work, therefore reducing
translate into significant benefits for the substantial lost productivity costs of
population health. Given its prevalence, lung cancer. For example, people with
a stage shift in lung cancer detection would stage IV lung cancer have been shown
save countless lives lost to lung cancer to incur higher wage losses and out-of-
every year and would have a dramatic pocket expenses than those diagnosed
impact on the overall number of deaths at a marginally earlier stage (stage IIIB).52
from cancer (Figure 4).Lung cancer screening: the cost of inaction
3 Earlier detection: the key to reducing the burden of lung cancer 14
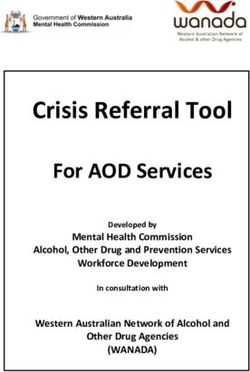
Figure 3. Non-small-cell lung cancer (NSCLC)* is commonly diagnosed at an advanced stage,
which is associated with poor prognosis
Diagnosed cases of NSCLC 5-year survival for NSCLC patients17, b
by stage (%)15, a
92
41
83
77
68
60
53
16 36
14
26
10
8
6 5 13
10
1
IA IB IIA IIB IIIA IIIB IV IA1 IA2 IA3 IB IIA IIB IIIA IIIB IIIC IVA IVB
* Non-small-cell lung cancer accounts for 80–85% of lung cancer cases58 59
Estimated
a from SEER validation data from the 7th edition of the International Association for the Study of Lung
Cancer (IASLC) staging project.
Based
b on the clinical staging data from the 8th edition of the IASLC staging project.
Earlier detection would also significantly as late diagnosis is thought to have
reduce the impact of lung cancer on quality worsened for all cancers. The World Health
of life for patients and their families. Organization reports that 55% of countries
Data suggest that people with advanced experienced disruption to cancer diagnosis
non-small-cell lung cancer (NSCLC) have and treatment during 2020.63 Cancer
worse health-related quality of life than screening programmes were halted in
people with other advanced cancer types.39 many countries and urgent cancer referrals
Shifting stage of detection can thus reduce decreased significantly.30-33 This situation is
the impact on people and their families, likely to lead to an increase in the number
including costs linked to informal care.62 of patients presenting with cancer at later
stages, when prognosis is worse.34 64
The risk of late presentation in lung A survey of 221 healthcare professionals in
cancer has been exacerbated by the Italy, Germany, France, Spain and the UK
COVID-19 pandemic reported a 52% decline in the number of
The urgency for earlier detection has been cancer patients seen per week, and a 63%
enhanced by the COVID-19 pandemic, drop in the number of patients startingLung cancer screening: the cost of inaction
3 Earlier detection: the key to reducing the burden of lung cancer 15
Figure 4. Lung cancer offers the greatest opportunity for early detection (England, 2018)16
100
Proportion diagnosed at stage IV (%)
80
Pancreas
60 Stomach
NHL
Lung
40 Oesophagus
Colorectal
Cervical
Ovarian
All other
20 Kidney
Prostate
Bladder
Melanoma
Breast
0
0 5,000 10,000 15,000 20,000
Number diagnosed at stage IV
NHL, non-Hodgkin’s lymphoma
The size of the circles shows the relative weight of each cancer type in terms of its contribution to the total
number of cancers detected at advanced stage.
Update of original figure produced by the United Kingdom Lung Cancer Coalition (UKLCC).53 Data from
Public Health England, 2018.16
cancer treatment.65 At time of writing, only same period the previous year.69 In the UK,
Germany has seen this situation improve.66 referrals to lung cancer specialists declined
by 75% in some areas during the first
Lung cancer has been hit particularly wave.68 Reduced access to CT scanners and
hard by the pandemic. The delays for lung diagnostic staff have led to further missed
cancer diagnoses have been significant due opportunities for early detection.29 Even for
to overlapping symptoms with COVID-19 those patients diagnosed early enough for
and specific pressures on respiratory surgery to be an option, limited availability
healthcare services.29 67 68 In Spain, the of surgery due to competing needs of
number of new lung cancer patients fell COVID-19 patients has had a significant
by 21–32% during the first wave of the effect on prognosis.64 70 Data for England
pandemic in 2020, compared with the suggest that a three-month delay in surgeryLung cancer screening: the cost of inaction
3 Earlier detection: the key to reducing the burden of lung cancer 16
Targeted screening is at the core of early
detection for lung cancer
Given the high toll of late presentation in
lung cancer, there have been considerable
efforts to identify an effective screening
tool in recent years. As articulated in
Europe’s Beating Cancer Plan, screening,
coupled with primary prevention, is the
most effective way to curb the burden of
cancer.72 Different approaches to screening
for lung cancer have been explored,
including for example chest X-ray aided by
artificial intelligence (AI).73 74 In particular,
LDCT screening has demonstrated
statistically significant benefits in large-
scale, international clinical trials.18 19
for bladder, lung, oesophageal, ovarian, It is recommended that lung cancer
liver, pancreatic and stomach cancers screening follow a targeted approach and
would incur 4,755 excess deaths over one be offered to those considered at highest
year, escalating to 10,760 excess deaths for risk of lung cancer, who are also most
a six-month delay.71 likely to benefit. Current recommendations
suggest that LDCT screening be offered
The pandemic has also likely reversed to current or former heavy smokers within
recent progress in lung cancer survival a specific age range.42 75 76 However, there
in many countries. Data from England is growing appreciation that smoking
suggest that delays due to missed status is insufficient to identify all people
diagnosis will lead to a 4.8–5.3% increase at high risk of lung cancer. Individual risk
in lung cancer deaths, equivalent to an prediction models, which incorporate
additional 1,235–1,372 deaths within five important risk factors for lung cancer – such
years following diagnosis.32 In Spain, as family history of cancer or pneumonia,
experts have warned that the pandemic occupational exposures (e.g. asbestos),
could set back lung cancer survival by 5%, race and ethnicity77 – are recognised as
resulting in an additional 1,300 deaths.69 helpful tools to identify high-risk candidates
Also, as healthcare systems emerge from who might be missed by only looking at
‘crisis mode’, they face a significant backlog age and smoking status.42 78
of cases which may further delay the return
to normal service levels29 34 – and this will The relative importance of smoking
inevitably include more people presenting compared with other risk factors
with advanced lung cancer. also varies by country. In Taiwan, for
example, 53% of lung cancer deathsLung cancer screening: the cost of inaction
3 Earlier detection: the key to reducing the burden of lung cancer 17
Figure 5. A comprehensive approach to early detection is needed
Rapid referral pathways
Patients who present to their primary care
physician with suspected symptoms of lung
cancer are rapidly referred for specialist diagnosis
and care82 83
Incidental nodule detection Lung cancer diagnosis and
care pathway managed
Patients with a suspicious lung nodule that by a multidisciplinary
happens to be detected through chest X-ray as care team82
part of routine care (e.g. for pneumonia screening) including oncologist,
are rapidly referred for specialist diagnosis radiation oncologists,
and care82 83 thoracic surgeons,
pulmonologist,
specialist nurse
Targeted screening programme
Patients who meet eligibility criteria for screening
are invited to undergo a low-dose computed
tomography scan, and are then followed up as
appropriate based on findings, and invited to
return for screening within a given interval82
occur among people who have never capture people with defined risk factors
smoked,7 and risk factors such as family (such as smoking status and age); however,
history, exposure to cooking fumes, and individuals who do not meet these criteria
exposure to environmental carcinogens are and present with possible symptoms of
increasingly recognised.79 Similar patterns lung cancer also need to be referred as
occur throughout East Asia, leading to quickly as possible for rapid diagnosis
recommendations that non‑smokers by a multidisciplinary care team. A
should be included in the target comprehensive approach to early detection
population for lung cancer screening in should thus include rapid referral pathways
these countries.80 81 for people who present in primary care
with possible symptoms, incidental nodule
In light of the evolving epidemiology of protocols for people who present with a lung
lung cancer, it is important that targeted nodule while undergoing a routine X-ray
screening programmes be complemented for another reason, and targeted screening
by other approaches to early detection. programmes for those who meet defined
Targeted screening programmes can screening eligibility criteria (Figure 5).Lung cancer screening: the cost of inaction
18
4 LDCT screening for
lung cancer: the next big
opportunity in cancer detection
Large-scale clinical trials have shown LDCT screening also leads to a significant
that LDCT screening is effective at reduction in lung cancer mortality in
reducing lung cancer mortality high‑risk patients. In the NELSON trial,
The evidence demonstrating the 18.4% of 868 deaths in the screening group
effectiveness of LDCT screening for lung were due to lung cancer, compared to
cancer reached a turning point in 2020. 24.4% of 860 deaths in the control group.18
The publication of the NELSON trial18 This equates to a reduction in lung cancer
showed that LDCT screening in current mortality in men of 24% over 10 years.18
and former heavy smokers can deliver a A mortality reduction of 33% was found
significant stage shift to earlier diagnosis in women, but the number of women
in lung cancer (Figure 6). In the NELSON participating in the trial was too small for
trial, 59% of cases among people in the this finding to be statistically significant.18
screening arm were early-stage, compared These findings have convinced experts
with 14% in the control population who around the world that the evidence for
were not offered screening.18 Similar figures LDCT screening to reduce lung cancer
have been found in other settings.19 84 mortality is now indisputable.84 86-88Lung cancer screening: the cost of inaction
4 LDCT screening for lung cancer: the next big opportunity in cancer detection 19
Figure 6. Screening programmes allow detection of a much higher proportion of lung cancer
cases at an early stage compared to routine care85
Diagnosed outside of a screening
Stage at programme Diagnosed in a screening programme
diagnosis
I
II
III
IV
Adapted from Sands et al. (2021). Patient decision-making aid based on combined analysis of existing clinical trials.
Any potential harms caused by LDCT positive results or subsequent unnecessary
screening are likely outweighed by procedures or treatments.85 86
its benefits
Screening is, by definition, offered LDCT screening for lung cancer
to asymptomatic individuals, so it is is expected to meet local
important to ensure the benefits of cost‑effectiveness thresholds
screening outweigh any potential risks. when designed appropriately
With LDCT screening, the main risks are Based on all published studies, LDCT
radiation exposure from the scan and screening is expected to be a cost-
misdiagnosis through a false-positive result. effective investment (Appendix 1).
Cumulative evidence from randomised Published cost-effectiveness ratios compare
clinical trials has shown that LDCT well with other population-based screening
screening presents a negligible risk of strategies, including those in place for
radiation exposure.85 If performed under colorectal, breast and cervical cancers,89
high-quality standards, LDCT screening and are likely to be within accepted
does not lead to a large number of false- economic thresholds.84 LDCT screeningLung cancer screening: the cost of inaction
4 LDCT screening for lung cancer: the next big opportunity in cancer detection 20
is also expected to be more efficient than
other screening programmes, meaning Box 1. Efficiency of lung cancer screening
that fewer people need to be screened compared to other cancer screening
for lung cancer to prevent one death programmes
compared with breast or colorectal cancer Data from different studies suggest fewer
screening (Box 1). screens are required to prevent one lung
cancer death compared to breast or
Targeted lung cancer screening is colorectal cancer:
expected to offer benefits even greater • 320 people need to be screened by
than those of existing cancer screening low‑dose computed tomography to prevent
programmes one death from lung cancer19
The benefits of LDCT screening are
• 645–1,724 people need to be screened by
likely to compare favourably to those of mammography to prevent one death from
existing cancer screening programmes. breast cancer21
Globally, the impact of LDCT screening on
• 864 people need to be screened by flexible
lung cancer mortality is expected to be
sigmoidoscopy to prevent one death from
significant (Box 2). Some experts suggest colorectal cancer22
that, if the highest-risk populations can
be reached, lung cancer screening could
have a larger absolute impact on cancer
mortality than existing cervical or breast Box 2. How many lives could lung cancer
cancer screening programmes.86 This is screening save?
also seen in cost-effectiveness studies of
LDCT screening, where optimal scenarios A summary of current estimates:
confer more benefits than any present • US: approximately 12,000 lives saved
cancer screening programme.20 per year 90
• Italy: 5,000 lives saved per year 91
• Australia: 12,000 lives saved over 10 years92
• Canada: 5,000–13,000 lives saved over
20 years93
• South Korea: 14,504 lives saved (91,362 life
years gained) over 20 years94
• Japan: 45,774 lives saved (290,325 life years
gained) over 20 years94
• Singapore: 1,290 lives saved (8,118 life years
gained) over 20 years94
• China: 471,095 lives saved (3,014,215 life
years gained) over 20 years94Lung cancer screening: the cost of inaction
21
5 An investment in health
system sustainability
The benefits of lung cancer screening pulmonary abnormalities.96 For example,
extend beyond lung cancer age and smoking history are the strongest
In addition to its impact on lung cancer predictors of lung cancer and chronic
mortality, lung cancer screening presents obstructive pulmonary disease (COPD),
an opportunity to detect other NCDs at therefore it is possible to identify a common
an early stage. As recently stated by the target population for screening and
World Health Organization, investment in detection for both conditions.25
NCD prevention and management is ‘an
insurance policy to improve population Promoting its potential to detect other
health and mitigate the impact of any future ‘big killers’ linked to smoking could
crisis’.95 Retrospective analyses of several make lung cancer screening a more
LDCT studies found a high rate of incidental attractive prevention package to high-
findings of cardiovascular disease and risk individuals. Experience from existing
respiratory conditions among screening lung cancer screening programmes has
participants.23-25 There may therefore be shown that screening can act as a life
value in LDCT screening programmes event that encourages participants to quit
also focusing on early detection of other smoking and take control of their healthLung cancer screening: the cost of inaction
5 An investment in health system sustainability 22
Evidence from clinical trials and pilot
studies shows that lung cancer screening
amplifies the success of smoking cessation
programmes, and vice versa. Experts
unanimously recommend that current
smokers invited to take part in screening
be offered smoking cessation advice
and encouraged to quit smoking.84 99 100
Several studies have shown that a positive
or indeterminate screening result in current
smokers prompts them to take up smoking
cessation and decreases smoking relapse
rates.42 101 Combining the two approaches
also increases the cost-effectiveness
of lung cancer screening programmes,
with a greater impact on reducing
mortality.42 102 103
more generally.97 98 Particularly among
former smokers, it is often seen as an Lung cancer screening may help to
opportunity to adopt behavioural changes address growing socioeconomic
such as increased physical activity and a inequalities in health
healthy diet.24 Health equity is one of the fundamental
tenets of health systems, and it has been
Targeted screening complements the threatened by the COVID-19 pandemic.
impact of smoking cessation policies The pandemic has amplified the need to
Targeted lung cancer screening should address a decade of widening inequalities
also be seen as a complement to due to socioeconomic status and
smoking cessation policies, contributing ethnicity.104 Such inequalities translate to
to countries’ anti-tobacco agendas. an inequitable gap in life expectancy.105
Smoking cessation programmes are the For example, in England there is almost
most important preventive measure for a twofold difference in mortality rates
lung cancer,2 but they are not sufficient to between people in the highest and lowest
decrease the global burden of lung cancer. socioeconomic groups.104 106 And as was
Targeted screening (and early detection recently articulated in Europe’s Beating
more generally) is needed to protect Cancer Plan, ‘there should be no first- or
people who are already at high risk of lung second-class cancer patients’.72
cancer (e.g. former smokers) and for whom
prevention has no immediate impact.42Lung cancer screening: the cost of inaction
5 An investment in health system sustainability 23
Social inequalities are highly prevalent in of late presentation, and have the poorest
lung cancer. On a global scale, the largest survival.26-28 Ensuring equitable access to
inequalities in cancer mortality rates are screening programmes is thus essential
found in smoking- and alcohol-related to address existing health inequalities.93
cancers, including lung cancer.28 People Otherwise, disadvantaged groups will
of lower socioeconomic status are at continue to experience an unjust share of
higher risk of lung cancer in all European the health burden.37 105 These combined
countries.28 107 They are also at greatest risk benefits are captured in Figure 7.
Figure 7. The impact of lung cancer screening extends beyond lung cancer
Reduced health inequalities
in lung cancer (in terms of
risk of late presentation,
access to appropriate
treatment and care, survival)
Complement to Targeted lung cancer
screening and broader Reduced loss of
smoking cessation
early detection productivity and fewer
policies, contributing to
premature deaths due to
creating a tobacco free Coupled with rapid access lung cancer
generation to expert diagnosis and
multidisciplinary care
Early detection of other
non-communicable diseases
(e.g. chronic obstructive
pulmonary disease,
cardiovascular disease)
Enhanced sustainability Contribution to
of healthcare systems through reduced mortality from
lower costs of care non‑communicable diseasesLung cancer screening: the cost of inaction
24
6 Ensuring successful
implementation of lung cancer
screening at scale
Governments should chart out a clear suitable in China, where there is a high
roadmap for implementation incidence of lung cancer in women and
Given the strength of the evidence, it is non-smokers.109 In Taiwan, for example,
now time for governments to evaluate lung cancer is common in non-smokers, so
the feasibility of lung cancer screening lung cancer screening is being proposed
programmes in their specific national for other groups at high risk of lung
contexts. So far, only a few countries – cancer.110 In Europe, several pilots are
including the US, Japan, South Korea, exploring the potential to combine LDCT
Poland, Croatia and Australia – have screening with early detection of COPD
committed to implementing nationwide or other smoking‑related conditions.111 112
lung cancer screening programmes. The European Commission-funded
However, pilot projects and local feasibility implementation study 4-IN THE LUNG RUN
studies are being conducted in almost is looking to identify the best way to
every region of the world. Findings from individualise screening intervals based on
this implementation research should be levels of risk.113
built into a clear pathway to guide decisions
around the most feasible way each country Based on this considerable research,
can replicate benefits from screening seen several key success factors emerge which
in clinical trials, while minimising potential should be built into the development
harms and ensuring the most efficient use of large-scale lung cancer screening
of local resources (Figure 8).108 programmes (Figure 9).
Findings from existing implementation
research should guide the roll-out of
lung cancer screening
More than a decade of feasibility and
pilot studies has provided a wealth of
information, with many lessons learnt
to guide implementation in different
countries. For example, studies have
shown that eligibility criteria used in
Europe and North America may not beLung cancer screening: the cost of inaction
6 Ensuring successful implementation of lung cancer screening at scale 25
Figure 8. A clear roadmap should be followed to guide decisions about local implementation
of lung cancer screening
Evidence assessment
(clinical trials)
Economic Local feasibility studies/
evaluation implementation research
Commitment to Securing funding
programme set-up sources
Organisational set-up and implementation of national programme
Development of national screening protocol covering:
Identification of the population eligible for screening
Invitation and information
Screening
Referral of screen positives and reporting of screen‑negative results
Diagnosis
Intervention, treatment and follow-up
Reporting of outcomes
Monitoring and continuous programme improvement
Note: Timing of economic evaluation and feasibility studies varies depending on screening governance
framework in each country – as does their impact on choice of national protocolLung cancer screening: the cost of inaction
6 Ensuring successful implementation of lung cancer screening at scale 26
Figure 9. There are several key factors in the successful implementation of targeted lung
cancer screening84 93 114
1 High-quality multidisciplinary lung cancer care pathways
2 Reliable means of identifying people at highest risk
3 Securing attendance, particularly among vulnerable groups
4 Essential role of primary care professionals
5 Lung cancer screening built into overall prevention messages
6 Clear nodule management protocols and personalised screening to minimise
potential harms from screening
7 Organisational model that allows optimal access and quality of screening and
efficient use of resources for staffing and physical/digital infrastructure
Local cost-effectiveness
will be influenced by all these factors
1. Effective screening requires the success of a screening programme
high‑quality, multidisciplinary depends on high-quality care
lung cancer care pathways pathways.115 Everyone with a positive
Investment in lung cancer screening result should have rapid access to
is best inscribed in a broader comprehensive diagnosis and care,
commitment to address lung led by a multidisciplinary care team.114
cancer as a priority. In particular, Embedding screening within a broaderLung cancer screening: the cost of inaction
6 Ensuring successful implementation of lung cancer screening at scale 27
focus on early detection, as mentioned care records. Some countries, such as
previously, is also crucial. the UK, have found ways to combine
data sources, often using a multistep
2. Reliable means of identifying approach where a first outreach
people at highest risk of lung cancer is made by a doctor or through
are needed a centralised invitation, and then
The success of targeted LDCT individuals are asked to complete a
screening depends on being able to structured questionnaire to determine
identify the population at highest risk smoking levels.84
of lung cancer, who are most likely
to benefit from screening. A first step As mentioned previously, eligibility
to any screening programme is thus criteria should also be looked
to ensure there is a reliable database at within the context of each
of the entire population that includes country’s epidemiology – and
smoking history and other relevant adjusted as needed to reduce the
risk factors to determine eligibility. potential for inequities in access to
However, most countries do not have screening (Box 3).
such a centralised database,84 with the
exception of those with unified primary 3. Securing attendance from
vulnerable populations is
essential to reduce socioeconomic
Box 3. The importance of localised inequalities
eligibility criteria: the US example Screening programmes must include
targeted efforts to engage vulnerable
The US recently changed its definition of ‘heavy populations, to avoid exacerbating
smoker’ to improve coverage of its LDCT
inequalities related to lung cancer.
screening programme.76 The US Preventive
Data from both trial and real-world
Services Task Force found that reducing the
pack-year* criterion to 20 pack-years from the settings show that people with lower
2013 recommendation of 30 pack-years would socioeconomic status and other
allow for inclusion of more women and non- disadvantaged groups are less likely
Hispanic Black, Hispanic, and American Indian/ to participate in cancer screening
Alaska Native persons, who were previously left programmes.114 118 119 Barriers to
out of screening.116
attending for screening may be
physical, financial, informational,
* The National Cancer Institute defines a ‘pack-
year’ as a measure for the amount a person has social or cultural.41 78 120 Tailored
smoked over a long period of time. It is calculated interventions may help overcome
by multiplying the number of packs of cigarettes some of these barriers in vulnerable
smoked per day by the number of years the person
has smoked. For example, 1 pack-year is equal to groups, and may also be effective at
smoking 1 pack per day for 1 year, or 2 packs per overcoming barriers to attendance in
day for half a year, and so on.117 other groups (Table 3).121-124Lung cancer screening: the cost of inaction
6 Ensuring successful implementation of lung cancer screening at scale 28
Table 3. Possible approaches to address barriers to lung cancer screening, particularly among
vulnerable populations
Barriers Approaches to overcome them
Limited information and awareness
• Insufficient awareness or misinformation about • Explaining benefits and harms of screening in an
the benefits of participating in lung cancer accessible format, with language- and literacy-
screening124 128 level-appropriate information42 120
• Confusion around screening results or lack • Providing patient-friendly decision aids such
of familiar care providers, especially due to as information brochures, videos and links to
language barriers or for people with lower electronic resources that people can refer to
health literacy124 129 after an appointment97 130 131
• Difficulty accessing online information services • Social media campaigns and digitally accessible
or not being registered with a healthcare information on screening to reach underserved
service129 or isolated communities121 132
Physical and financial barriers to access
• Distance from screening centres and provision • Linking underserved communities with larger
gaps in rural areas72 133 screening centres through emerging digital
• Prohibitive transport and parking costs, and health tools, to enable community access to
difficulty accessing screening centres93 134 multidisciplinary teams72 97
• Difficulty of fitting appointments around work • Decentralised mobile screening in public spaces
or caregiving commitments134 like supermarket car parks e.g. Manchester Lung
Health Check model20 126
• Offering assisted travel to imaging units e.g. the
‘hub-and-spoke’ model93
• Community pharmacists and other allied health
professionals providing information on lung
cancer screening to their clients/patients135
Psychological and social barriers
• Forgetting to attend a scheduled appointment • Postal, text and telephone reminders after first
or little awareness of the benefits of screening120 invitation letter to attend screening137 138
• Social or cultural distrust of healthcare • Personalised letter encouraging attendance
services, or other psychological factors that from family physicians138 (e.g. used for cervical
may undermine motivation to engage in cancer screening in the UK)121
screening e.g. denial, fatalistic health beliefs, • Targeted awareness initiatives involving
embarrassment due to stigma around lung community or faith leaders28 120
cancer 42 131 134 136
• Co-designing public information and education
campaigns with vulnerable groups to ensure
suitability and impact of messaging42 122Lung cancer screening: the cost of inaction
6 Ensuring successful implementation of lung cancer screening at scale 29
One model of particular interest is to refer patients for LDCT screening.141
to offer screening in public spaces Physicians should also be encouraged
in socioeconomically deprived areas. to adopt a shared decision-making
This model has been developed approach to screening with their
in some of the Lung Health Check patients.42 97
pilots now being rolled out across
England.125-127 Pilot projects in Engagement of family physicians
Manchester used mobile units near should not stop with their role in
supermarkets to tackle barriers securing attendance to screening.
such as parking and transport They should, where feasible
costs, inconvenience and location.87 depending on the organisation of the
Three quarters of attendees were health system, play an active role in
from the lowest socioeconomic following-up individuals after their first
quintile.127 round of screening, explaining findings
and making sure people continue to
4. Engagement of primary care attend screening.97 144
professionals is essential
Family physicians remain people’s 5. Lung cancer screening should
most trusted source of health be built into overall health
information and play a key role promotion messages
in engaging people to attend for Sensitive messaging about lung
screening. Misinformation about cancer screening is essential and
lung cancer and screening can be should tackle stigma related to
potential barriers to acceptance of both lung cancer and smoking.
screening.139 140 Family physicians Addressing potential fear and
can help allay people’s fears about stigma surrounding lung cancer is
screening, provide balanced important.41 42 Family physicians
information about risks and benefits, also need to find the most appropriate
and explain the importance of early way to tackle the need for smoking
detection in lung cancer. cessation. In some cultures, some
physicians may be reluctant to raise
Training of family physicians the topic of smoking cessation,
is essential. Inconsistent levels and mentioning it in invitations
of awareness around screening to attend screening may reduce
guidelines and eligibility, and poor participation.140 One approach
understanding of the risks and is to present the opportunity to
benefits of screening, have been undergo LDCT screening as part
evidenced in some countries.141-143 of a proactive wellness approach
A recent survey found US healthcare to one’s health (Box 4).
providers with lower knowledge of
screening guidelines were less likelyLung cancer screening: the cost of inaction
6 Ensuring successful implementation of lung cancer screening at scale 30
6. Clear nodule management protocols
Box 4. Lung Health Checks in England: and personalised screening
taking a wellness approach intervals can reduce harm and
The Lung Health Check model adopted across improve programme efficiency
England takes a wellness approach for all Any screening programme carries risks
respiratory disease rather than focusing on – and minimising risks is not only an
cancer. Individuals are assessed for all lung ethical imperative but also a condition
conditions and offered a CT scan if eligible. for cost-effectiveness. Protocols
The following approaches have been found guided by the most up-to-date
to encourage uptake and overcome stigma evidence148 149 are essential to guide
surrounding smoking and fear of lung cancer: healthcare professionals in determining
• Invitations do not mention smoking status which nodules to refer for further
or smoking cessation. diagnosis and possible treatment,
• Invitations do not mention lung cancer, so as and which to simply monitor.87 93 The
not to put people off taking part due to fears use of protocols reduces the number
about cancer. of false‑positive cases, patient recall
and the need for repeat scans and
• Supportive interventions (e.g. psychosocial
support) are offered as part of the investigative procedures, leading to
wellness check. lower costs overall.42 87
• Awareness campaigns accompanying the
Tailoring follow-up protocols to
programme offer good-quality information.
personal levels of risk may also
• During health checks, information is improve the effectiveness and
provided making it clear that lung cancer cost-effectiveness of screening.
can be treated if caught early.
Both annual and biennial screening
programmes have been deemed
potentially cost-effective in existing
Messaging about lung cancer and studies.61 84 102 However, personalising
smoking should be targeted to different screening intervals after baseline
groups – for example by gender. screening may minimise the need for
Lung cancer incidence has been rising potentially unnecessary investigations
in women, as have rates of smoking in people deemed at lower risk.
– but smoking is not the only factor.2 They may be particularly relevant for
145 146 Cumulative evidence from lung women, for whom nodules have been
cancer screening trials also suggests shown to have a slower growth rate
that LDCT screening may have a than for men.150 151
more beneficial effect in women than
men, both in terms of increased
early-stage diagnosis and reduced
mortality.18 84 147Lung cancer screening: the cost of inaction
6 Ensuring successful implementation of lung cancer screening at scale 31
7. The right organisational model which may help ensure high quality of
and health system resourcing are screening.114 Others locate screening
needed to ensure sufficient staffing programmes in community settings
and infrastructure to foster outreach to vulnerable
Screening is about more than just populations, linking these centres to
the scan itself, and selecting the specialist multidisciplinary teams in a
most appropriate organisational hub-and-spoke approach.93 Careful
model is key. The logistical aspects consideration of available technical
of screening – centralising invitations, and workforce capacity is also an
ensuring systematic follow-up, important factor to consider.
recording outcomes of screening
from cancer registries – require Regardless of the organisational
sophisticated information systems and model, building quality assurance
careful coordination,37 all of which and professional training across
need appropriate resourcing. It may be all centres performing CT scans
that structures or resources devoted to is essential. This can help ensure
existing cancer screening programmes CT scans are of consistent quality
can be leveraged – for example, if all and that interpretation follows a
cancer screening is offered by a central common approach.42 Benchmarking
coordinating centre.144 CT software and AI may also
help improve the reliability of
The most appropriate organisational interpretation.84 These approaches
model should be chosen, balancing can help to relieve potential capacity
the need for outreach and quality shortages in countries where
assurance. Some countries have availability of trained radiologists to
chosen to centralise screening in a perform CT scans may be limited.133 152
limited number of specialist centres,You can also read