MEDICAL TIMES LILAVATI HOSPITAL - JUNE 2022
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

LILAVATI HOSPITAL
MEDICAL TIMES
JUNE 2022
CHAIRPERSON - LHMT From COO's Desk . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Lt. Gen. (Dr.) V. Ravishankar, VSM
Editorial . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
CHIEF EDITOR
Dr. Rajeev Redkar Overview: Lilavati Hospital and Research Centre . . . . . . 4
EDITORIAL TEAM Case Reports . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Dr. Amey Medhekar ! Dermatology
Dr. Bhavesh Vajifdar = En coup de sabre corrected with Autologous Fat Grafting . . . . . . . 6
Dr. Chandralekha Tampi ! Anesthesiology
Dr. D.R.Kulkarni = A Case of Neurofibromatosis Type 1 with Severe Cervical Kyphosis
for Corrective Spine Surgery- Anesthetic management of a Difficult
Dr. Kiran Coelho Airway & Intraoperative Neuromonitoring . . . . . . . . . . . . . . . . . . . 8
Dr. Leena Jain = Anaesthetic challenges in management of a large thyroid with
Dr. Salil Mehta retrosternal extension with thymic mass : A case report . . . . . . . . 11
Dr. Sheikh Minhaj Ahmed ! Plastic Surgery
= Extensive Degloving Injury of the Abdomen and Thigh: A
multidisciplinary approach . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
CO-ORDINATOR ! Histopathology
= KIKUCHI FUJIMOTO DISEASE IN CHILDREN – an Uncommon
Mr. Kundan Singh Entity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
! Orthopaedic
= Masquelet Technique . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
All the correspondence should be
addressed: List of Publications. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
To, Straight from the Heart - Patient Testimonials . . . . . . . . 26
The Chief Editor
Lilavati Hospital Medical Times Services Available . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Lilavati Hospital & Research Centre
A-791, Bandra Reclamation, Bandra (W) Important Telephone Numbers. . . . . . . . . . . . . . . . . . . . . 28
Mumbai - 400 050.
Email: medicaltimes@lilavatihospital.com Drug Safety Alert . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
Website: www.lilavatihospital.com
Few Honorable Mentions . . . . . . . . . . . . . . . . . . . . . . . . . 31
Doctors Associated with Lilavati Hospital . . . . . . . . . . . . 32
The views expressed in the Medical Times are not of Lilavati Hospital or the editor or publisher. No part of the Medical Times can be reproduced
in any form including printing or electronic without the written permission of the chief editor or publisher. The information provided on
medicines, materials, investigations, procedures, therapies and anything medical is the sole responsibility of the author of the article and the
hospital shall not be responsible for any such information.
From COO's Desk
It brings me great happiness to present to you this year’s second Lilavati Hospital Times.
We are proud to feature in “Top 10 Best Multispecialty Hospital” presented by Outlook & NEB
Research for ‘Outlook Health’. Our hospital was ranked 2nd in the west zone, and was
recognized as “Best Infertility Hospital”.
Our second floor Visitor’s cafeteria is now certified as “Eat Right Campus” & awarded five star
rating by “Food Standards Safety Authority of India (FSSAI)”. It is a great achievement by our
Hospitality team and Institute as a team.
We are glad to announce the restarting of the Hydrotherapy centre (Oxygen therapy) called Belhydro PURO2 on the 8th floor
of the hospital. This uses water and oxygen for skin moisturising and deep skin cleaning as well as naturally making the skin
supple.
Some minor renovations have been done in the Emergency Department (casualty). Notable are the blue antimicrobial coated
curtains which are effective for 3-4 years. There is a plan to develop minor OT in the casualty area which will aid in performing
minor surgeries right there without the logistic difficulties of taking patients to OR and attain better patient satisfaction.
Lilavati Hospital has been conducting “Community Basic Life Support Training” sessions regularly. To mention a few, the
training sessions have been taken for Traffic police, students at various colleges, employees of various corporate houses,
congregation’s at Church, Satsung, etc. We are happy to announce restarting the Yoga sessions at Lilavati 5th floor for the
community and Lilavati staff. Thus this institute believes in giving back to society. I am also looking at restarting the
academic sessions soon.
A delegation from Trinity College Dublin visited LHRC, and praised us for the quality service being offered to our patients.
Our DNB Student Dr. Raksha Kulkarni (Nuclear Medicine Resident) & DrNB Student Dr. Vikas Gupta (Critical Care Medicine
Resident) were awarded “Certificate of Commendation” for outstanding research work in thesis by National Board of
Examinations, New Delhi.
We extend our congratulations to Mr Raju Kokane on being conferred the “Life Time Achievement” award from Indian Society
of Extra Corporal Technology (ISECT). He was felicitated by ISECT for his 30 years of service as perfusionist and his exemplary
work with ECMO (artificial lung as a life saving device) machines in covid patients. I would also like to Congratulate Dr Faiyaz
Shaikh for being an invitee at Raj Bhavan, where ‘Shri JJT University conferred Honorary D.Litt. Degree to Hon. Governor
of Assam Dr Jagdish Mukhi in presence of Hon. Governor Bhagat Singh Koshiyari’.
To smoothen the OPD and Visa appointments dedicated direct lines have been made functional. (OPD-8657907751/52/53,
Visa-8657907756).
It is my proud privilege and honour to extend warm greetings and heartfelt gratitude to all the staff of LHRC for the exemplary
performance and achievements.
As we move on we hope to say 'Goodbye' to the pandemic and wish all a safe and healthy days ahead.
Lt. Gen. (Dr.) V. Ravishankar
Chief Operating Officer and Consultant Cardiothoracic Surgeon
1
Editorial
I consider it my privilege to bring forth the 2nd Lilavati Hospital Medical Times as the Chief
Editor. I sincerely thank our COO Dr. Ravishankar, the Lilavati Hospital Management and my
Editorial team for bestowing the trust in me, and for extending a wholehearted support in
bringing out this Edition and my ideas.
Lilavati Hospital has recovered well from the COVID times and the Outpatients, Inpatients,
Diagnostic Services and Operating Theaters are chugging towards a pre-COVID normalcy. The
pivotal role played by the support Staff, Nursing teams, Resident doctors, Esteemed Consultants
and the Hospital Management is highly appreciated. They all have been working rigorously,
tenaciously and with unflinching loyalty to make sure the Institute has been doing well.
I take great pride to announce that Lilavati Hospital featured in “Top 10 Best Multi-Specialty Hospital” presented by Outlook
and NEB Research for “Outlook Health”. Our Hospital was Ranked 2nd in the West Zone and was recognized as the ‘Best
Infertility Hospital’.
Covishield Vaccination for Covid has been going on in full swing on the 5th Floor. Our Emergency Department (Casualty) of
Lilavati Hospital has been recently renovated with blue anti-microbial curtains and there is a proposed plan to start a Minor
Operation Theater around the Casualty. The Hydrotherapy and Oxygen Therapy Centre called the BelHydroPURO2 has been
restarted on the 8th Floor.
There has been an active participation of the Consultant Doctors and the Resident Staff in contributing wonderful Articles and
Case reports for the Lilavati Hospital Medical Times. I request that this enthusiasm persists for the ongoing Editions of the
Medical Times. As decided earlier, there are Best paper award being instituted since the Last edition of Lilavati Hospital
Medical Times. All the papers were assessed by an Awards committee using a Score based on the innovative content and
practice changing aspects of the research work. The Best papers were 1) Risk Prediction Scoring System to Predict the
Postsurgical Outcomes of Biliary Atresia & 2) A Clinical audit of quality indicators in anesthesia practice over last 5 years in
Lilavati Hospital and Research Centre.
I request you to go through the Medical Times from cover to cover and maximally utilize the presented information to create a
positive impact on the patient care.Please let us know how the experience of reading this Times has been with your valuable
feedback, criticisms and suggestions. The more we share the more we learn!
The COVID wards in our Hospital have been closed, sterilized and opened to general public. However, with us being a
Tertiary Care Hospital and the looming fear of the resurgence of COVID, we should be taking all the possible precautionary
measures and maintain a high index of vigilance with our Staff and Patients.
I wish all a Safe and Healthy time ahead.
Respectful regards
Dr. Rajeev Redkar
M.Ch., FRCS (Paed. Surg), MS, DNB, FRCS (Edin), FRCS (Glas), FCPS, IAS
Chairman, Indian Association of Pediatric Surgeons (Maharashtra Chapter)
2
OUTLOOK HEALTH
BEST HOSPITAL RANKING 2022
TOP 3 BEST TOP 10 BEST
MULTISPECIALITY MULTISPECIALITY
HOSPITAL HOSPITAL
(Mumbai) (All India)
BEST
INFERTILITY
HOSPITAL
(All India)
3
Overview: Lilavati Hospital & Research Centre
Lilavati Kirtilal Mehta Medical Trust
Lilavati Hospital and Research Centre is run and managed by Public
Charitable Trust - Lilavati Kirtilal Mehta Medical Trust which was
formed in 1978. The Trust was started by late Shri Kirtilal Manilal Mehta.
The Trust has engaged in innumerable charitable endeavors across India.
The Lilavati Kirtilal Mehta Medical Trust
is being managed and administered by Board of Trustees:
Smt. Sushila V. Mehta Shri Nanik Rupani
Shri Kishor K. Mehta Shri Rashmi K. Mehta
Smt. Charu K. Mehta Shri Dilip Shanghvi
Smt. Rekha H. Sheth Shri Chetan P. Mehta
Shri Niket V. Mehta Shri Bhavin R. Mehta
Shri Ayushman C. Mehta
Principal Advisor to the Board of Trustees and
Lilavati Hospital & Research Centre
Shri S. Lakshminarayanan, IAS (Rtd.)
Lilavati Hospital And Research Centre
Late Shri Vijay Mehta wished to fulfill his parents desire to build a world-class hospital where everyone
in need for relief from disease and suffering come in with a certainty to receive the best possible medical
care. His passion, attention to details and perseverance resulted in iconic healthcare landmark called
Lilavati Hospital.
Lilavati Hospital & Research Centre is a premier multispecialty tertiary care hospital located in the heart
of Mumbai, close to the domestic and the international airport. It encompasses modern healthcare
facilities and state of art technology dedicatedly supported by committed staff.
Lilavati Hospital has focused its operation on providing quality care with a human touch; which truly
reflects the essence of its motto, “More than Healthcare, Human Care”. Being a centre of medical
excellence where technology meets international norms and standard, the hospital has got what it takes
to be a pioneering quality healthcare institute that is also one of the most sought after and patient
friendly hospital.
Mission: To provide affordable healthcare of international standard with human care
Motto: More than Healthcare, Human Care
4
Highlights
! 326 bedded hospital including 77 intensive care beds. Currently number of beds have been temporarily
increased for helping fight the COVID pandemic. We have dedicated 144 ward beds and 48 ICU beds to treat
COVID positive patients.
! 12 state-of-the-art well equipped operation theatres.
! Full-fledged Liver Transplant, Heart Transplant, Heart Failure, Hypertension, Bariatric, Foot and Ankle,
Dental and Dermo Cosmetology Clinic.
! State of art PET – SPECT CT department.
! Lilavati Hospital is equipped with Coronary GRAFT Patency Flowmeter which is first of its kind in India.
This imaging system is used in Cardiac surgery to assess GRAFT flow / perfusion in coronary bypass
surgery.
! The hospital has installed state-of-art Philips Azurion 7F20 in its cath lab. This is the first of its kind high end
configuration system installed in India. The new system enables excellent imaging for Coronary, Cerebro &
Peripheral Vascular Diseases.
! The department of Invasive Cardiology has been upgraded with the addition of a High Definition Optis
Mobile OCT (Optical Coherence Tomography) system. It has the latest configuration which gives better 3 –
Dimensional perspective of Coronary Artery before and after stent deployment.
! The hospital has added Intraoperative Nerve Monitoring system which enables surgeons to identify, confirm
and monitor motor nerve function of the patients which helps to reduce the risk of nerve damage during
various operative surgeries.
! The hospital has upgraded its ENT department by adding a top-of-the line surgical operating microscope to
carry out various microsurgeries under high magnification. The microscope electronics allows the surgeon to
electronically control object focusing, magnification,illumination, surgical recording, etc.
! All days round the clock OPD Pathology and Radiology investigations without any Emergency charges.
! More than 300 consultants and manpower of nearly 1,800.
! Hospital attends to more than 10000 In-patient, 40000 Out-patient and performs thousands of surgeries
every year.
! Modern Cathlabs having specialized SICU & ICCU with highly trained cardiac care medical staff.
Lilavati Kirtilal Mehta Medical Trust Research Centre
The Lilavati Kirtilal Mehta Medical Trust Research Centre is a Scientific and Industrial Research Organization approved
by Ministry of Science and Technology (Govt. of India). The Research Centre under guidelines of Dept. of Science &
Technology works in close collaboration in evaluating and developing technologies for better healthcare to the sick people.
The research centre has undertaken multidisciplinary researches in the fields of Cardiology, Radiology, Cerebrovascular
Diseases (Stroke), Ophthalmology, Chest Medicine, Nuclear Medicine, Pathology, Oncology, Orthopedics etc., to cite a
few. One of the important aim of the research centre is to establish community based epidemiological researches in
cerebrovascular disease in stroke.As a policy, Drug and Device Trials are not undertaken at the Research Centre.
5
CASE REPORT I: DERMATOLOGY
En coup de sabre corrected with Autologous Fat Grafting
Dr Delanthimar Joshika Bhandary, MD (Dermatology & Venerology),
Clinical Associate.
Dr Nilesh Narendra Goyal, MRCP UK, DNB (Dermatology & Venerology),
DVD, SCS Dip Consultant.
Keywords:
Fat grafting, morphoea, scleroderma
INTRODUCTION
Autologous Fat Grafting (AFG) is a process of acquiring fat from a donor area on body and placing it under the skin in areas requiring volume
restoration. The first report of this procedure dates back to 1893 when Neuber used fat chunks for correcting scars of tuberculosis in Germany.
But the procedure gained prominence when liposuction was invented in 1970s. Pierre Fournier, an Aesthetic surgeon from Paris restarted fat
grafting on to the face for volume restoration.
Soft tissue volume defects of the face can be corrected with AFG. Scleroderma, HIV patients on protease inhibitors who get drug induced
lipodystrophy and patients undergoing radiation treatment have shown to respond well to AFG. En coupe de sabre is a rare form of localised
scleroderma involving the fronto-parietal region. The skin and underlying tissues undergo fibrosis and thickening. Once the disease has gone
into remission, patients are left with cosmetic defect which has a significant bearing on their appearance denting their confidence.
Case
A 23-year-old man presented to the outpatient department with a deformed left half of face that was the outcome of scleroderma he suffered at
age of 7 years. His left half of face showed stunted growth of bone and soft tissues with darkening of overlying skin. [Fig. 1, 2, 3, 4] There was a
stark mismatch of volume when compared with right side of face. The disease had stopped progressing within a year of its onset. A recent MRI
of face showed minimal thickening of skin in the left half of frontal region, left periorbital region, left half of nose, left malar prominence and
left maxillary region with complete loss of subcutaneous fat in these regions and complete loss of buccal pad of fat on left side.
Fig No 1 Fig No 2 Fig No 3 Fig No 4
It was, hence, decided to use fat filling for correction of volume deficit as fat loss was noticed and significantly large volumes would be
required. The patient underwent an autoimmune screen with viral markers to rule out any underlying systemic illness. The procedure was done
with full aseptic precautions. Fat was harvested from central para umbilical area which was anaesthetized using Klein’s formula for tumescent
anaesthesia (Dilute solution of Lidocaine, Adrenaline and Sodium Bicarbonate in Normal saline). The marked donor area was infiltrated with
the solution and after a waiting time of 20 minutes, fat was aspirated using 2.5mm (10G) aspiration cannula attached to a 10ml Luer Lock
syringe. During aspiration attention was paid to keeping suction pressure to a minimum so as to cause least damage to the adipocytes.
The recipient area was marked, prepped and then anesthetized using the same Klein’s solution (smaller quantities). The entry points were
anaesthetized with 1ml of lidocaine plus adrenaline solution. An 18G needle was used to make the entry points and then using a blunt tipped
0.9mm injection cannula attached to a 1 ml luer lock syringe fat was placed deep under the soft tissues in the supraperiosteal plane. The fat was
placed while cannula was being withdrawn ie. retrograde fashion. Care was taken to place micro droplets of fat in any one area. A total of 30 ml
of micro fat was required for filling the affected area. Postoperative instructions were to take oral antibiotics and pain killers for a few days and
avoid massaging face for a week.
6
Fig No 5 Fig No 6 Fig No 7 Fig No 8
The process was repeated every 3 months for the first three sessions.[Fig 5, 6, 7, 8] During each session around 20 – 30 ml of fat was placed. By
this stage good correction was achieved. After 6 months of the 3rd session, some reduction of the volume of left half of face was felt. Hence
further two sessions were done over the next six months in a similar manner. At each of these sessions required an average of 20 ml fat was
required for correction. The patient underwent a total of 5 sessions over a period of 2 years during which a total of 120ml of fat was placed to fill
the entire left half of face with some on the frontal bone above left eye. [Fig 9, 10, 11, 12]
Fig No 9 Fig No 10 Fig No 11 Fig No 12
Patient was satisfied with the improvement in his appearance. There was no recurrence of disease activity at any time during the two years.
DISCUSSION
Localized scleroderma has a variety of clinical presentations such as, generalized, guttate, nodular (keloidal), subcutaneous (morphea
profunda), and linear scleroderma, including en coup de sabre morphea. It is not life-threatening but can cause disfigurement, such as hypo- or
hyperpigmentation with depressed atrophic areas in approximately 50% of patients.[1] Although medical line of treatment with high potency
topical corticosteroids, calcipotriol ointments, imiquimod, and UVA irradiation helps in curbing the disease activity, atrophic areas of skin with
pigmentary changes persist for life. [2][3]
Autologous fat scores over other filler substances such as hyaluronic acid, collagen, silicone because of the fact that fat is safe, readily
available, noncarcinogenic, and autologous, which decreases host immune response. Fat is a rich source of Adipose Derived Stem Cells
(ADSCs) also known as Multilineage Differentiating Stress-Enduring cells (Muse cells) which are of mesenchymal origin. Additionally, the
pericytes, fibroblasts and endothelial cells present in fat graft show upregulation in their regenerative capacities resulting in good outcomes
post fat grafting.[4] Liposuction done from less than half centimeter round incisions and fat injection using blunt tipped cannula has made this
procedure easy to perform. The procedure is scarless with minimal downtime. [5]
A disadvantage of autologous fat transfer is the unpredictable resorption of the graft. The adipocytes at the periphery of fat parcels establish
contact with living tissue at the recipient site, revascularise and survive. The cells at the centre of the grafted fat undergo necrosis due to
ischemia, thereby reducing fat volume at the transplanted site. [6] Therefore the injected fat parcels have to be kept small to maximize survival,
necessitating the need for repeat transfers in many cases.[7]
REFERENCES:
1. Hawk A, English JC, 3rd. Localized and systemic scleroderma. Semin Cutan Med Surg 2001;20:27-37
2. Dytoc M, Ting PT, Man J, Sawyer D, Fiorillo L. First case series on the use of imiquimod for morphoea. Br J Dermatol 2005; 153: 815-20
3. Dutz J. Treatment options for localized scleroderma. Skin Therapy Lett 2000; 5: 3-5
4. Heneidi S, Simerman AA, Keller E, Singh P, Li X, Dumesic DA, Chazenbalk G. Awakened by cellular stress: isolation and characterization of a novel population of pluripotent
stem cells derived from human adipose tissue. PLoS one. 2013; 8(6): e64752
5. Roh MR, Chung KY, Goyal NN, Al Shehri F. Autologous fat transfer—principles, techniques, and outcomes for facial rejuvenation, scars, breast, and buttocks. Dermatological
Reviews. 2021 Aug;2(4):205-19.
6. Nguyen A, Pasyk KA, Bouvier TN, Hassett CA, Argenta LC. Comparative study of survival of autologous adipose tissue taken and transplanted by different techniques..Plast
Reconstr Surg 1990;85: 378-86
7. Spear SL, Wilson HB, Lockwood MD. Fat injection to correct contour deformities in the reconstructed breast. Plast Reconstr Surg 2005; 116: 1300-5
7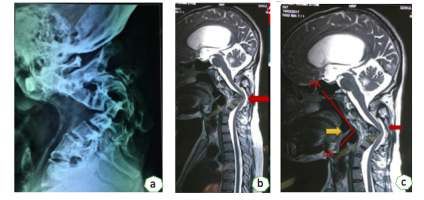
CASE REPORT II: ANESTHESIOLOGY
A Case of Neurofibromatosis Type 1 with Severe Cervical Kyphosis for
Corrective Spine Surgery- Anesthetic management of a Difficult Airway &
Intraoperative Neuromonitoring
Dr Sucheta Gaiwal, DA, DNB, FCPS, PGDMLS, PGDHA, Consultant Anaesthesiologist
Dr PragnaSree Ravulapalli, DNB Resident, Anaesthesia
Dr Priyank Patel, MS Orthopedics, Consultant Spine Surgeon
Dr Premik Nagad, DNB Orthopedics, Consultant Spine Surgeon
Dr Shekhar Bhojraj, MS FCPS (Orthopedics), Consultant Spine Surgeon
Keywords:
cervical kyphosis, Neurofibromatosis, difficult airway, awake fiberoptic intubation, Intraoperative neuromonitoring.
INTRODUCTION
Neurofibromatosis type I (NF 1) is a relatively common single gene disorder with an incidence of 1:2500-3000. It is due to mutation of NF 1
gene located on chromosome 17 and shows an autosomal dominant pattern of inheritance.1 It has a widespread effect on ectodermal and
mesodermal tissues resulting in multiorgan system involvement. It is associated with a variety of conditions often requiring anaesthesia for
surgical treatment, including painful neurofibromas, severe kyphoscoliosis, pseudo arthroses, hydrocephalus, intracranial tumours and other
malignancies.2
Although the spine is one of the most commonly affected part of the skeletal system in NF1,3 only a few cases of cervical kyphosis with an
angle of >90° have been reported so far. The severe dystrophic changes in vertebrae in cervical kyphosis make surgical correction and fusion of
the deformity extremely difficult in addition to the challenges it poses to the anesthetist with regards to the airway management.
Intraoperative neuromonitoring under anesthesia (SSEP’s, MEP’s) has become a standard of care in complex spine surgeries where the
integrity of spinal cord is threatened. It helps prevention or early detection and minimizing the chance of permanent neurologic injury from
surgical manipulations. We describe the perioperative management of patient of NF 1 and 110° dystrophic curve of cervical spine with
emphasis on difficult airway management and role of intraoperative neuromonitoring in spine instrumentation.
Case report
We report a case of 27-year-old male who is a known case of neurofibromatosis type-1 (Café-au-lait spots, left cerebellar neurofibroma) with
severe cervical kyphoscoliosis posted for 2 stage corrective spine fixation, 1st stage-Anterior decompression with C4, C5 corpectomy & 2nd
stage C2-C6 posterior lateral mass screw and rod fixation.
Patient was otherwise normotensive, non-diabetic presented with worsening neck pain since last 3 years associated with increasing neck
flexion deformity. There was no bladder or bowel disturbances, no neurological deficits or no fine motor disturbances.
Patient was diagnosed as a case of Congenital fusion of C2-C4 vertebrae with kyphoscoliosis of cervical spine with cord compression
secondary to NF-1.
Patients systemic examination was unremarkable except for severe kyphosis of the cervical spine. His airway examination revealed
Mallampatti Class-III, with adequate mouth opening and severe restriction of neck movements -fixed flexion deformity and minimal
extension (Fig 1: Lateral radiograph of the cervical spine (a) showing fusion of C2-C5 vertebrate with kyphotic Fig 2:
angle of 110o. MRI of spine (b&c) showing cervical kyphosis causing marked tracheal deviation at an a. Anterior curvature of the tip of bronchoscope
angle of 90o with vertebral body fusion from C2-C5 resulting in spinal cord compression. Yellow arrow b. Posterior curvature of the tip of bronchoscope
(c) points to the sharp angle at the level of epiglottis which made negotiation of tip of bronchoscope
difficult.
On the day of surgery in the preoperative area oxymetazoline nasal drops were instilled along with lignocaine nebulization and lignocaine
gargles. Patient also received intravenous 0.2 mg glycopyrrolate as premedication. Once the patient was wheeled into the operation theater,
after attachment of minimum standard ASA monitors including electrocardiography, Non-invasive blood pressure and pulse oximetry 2 large
bore intravenous lines (16G and 18G) were secured. Patient was prepared for awake fiberoptic nasal intubation by topicalization of airway
with 10% lignocaine, trans tracheal block along with dexmedetomidine infusion at 0.7 mcg/kg/hour. Performing the trans tracheal block was
challenging due to the fixed flexion deformity of the neck. Spray as you go technique was also used during the fiberoptic bronchoscopy. The
significant tracheal deviation with loss of alignment of the oral and pharyngeal axis due to short neck posed great difficulty in maneuvering of
bronchoscope. The use of even the posterior tip of bronchoscope having more curvature with passive outward traction on the tongue also didn’t
prove to be successful. Then the patient was asked to protrude his tongue which helped push the epiglottis forward hence allowing the passage
of the bronchoscope and visualization of vocal cords.
Airway was secured with size 7 reinforced endotracheal tube. After confirming the position of tube patient was given IV fentanyl 2 mcg/kg and
IV propofol 2mg/kg. General anesthesia was maintained with Air/O2 in 50:50 ratio at 2L/min with Sevoflurane. Right radial artery was
cannulated to provide continuous invasive blood pressure monitoring. In order to facilitate intraoperative neuromonitoring a modified
anesthetic technique including minimal use of inhalational anesthetics (MAC 70-80% fall
in amplitude) in the MEP’s.
The neurophysiologist immediately notified both the anaesthetist and the surgeon and surgery was paused. All possible causes of interference
with neuromonitoring were evaluated- MAC of inhalational anaesthetic, MAP, use of any muscle relaxant, use of nitrous oxide. The
inhalational anaesthetic was turned off and MAP was maintained above 75 mmHg ensuring BIS was within range of 40-50. It was presumed
9that the fall in MEP’s could be a result of traction on the cord from the lateral mass screws.
A decision to redo the mass screw fixation was made. TCeMEP’s returned to baseline after
redoing of the mass screws. Evoked potentials recorded before starting surgical wound
closure and after completion of the closure were comparable to the baseline readings. Final
readings were taken after the patient was made supine. Surgery lasted for 8 hours with blood
loss of 1000ml. One unit packed red blood cells was transfused. Patient was awakened post-
surgery and put on T-piece electively in view of difficult airway, cervical spine manipulation
and prolonged duration of surgery. Neurological evaluation done immediate postop did not
reveal any focal deficits. Patient made an uneventful recovery
DISCUSSION
Airway management in patient with neurofibromatosis is often difficult and challenging due Fig 3:
to the wide spectrum of involvement of airway. An estimated 5% of the patients with NF 1 a. Baseline motor evoked potentials
have an intra oral manifestation of the disease b. Sudden fall in MEP's on left side
c. Return of MEP to baseline after redoing lateral
involving the tongue or the larynx. Plexiform neurofibromas commonly occurring in the mass screws
cervical region and tumors of the para pharyngeal space may result in distortion of the
airway.4 Careful history taking during pre-anesthetic assessment can identify symptoms of
obstruction, dyspnea, stridor, change of voice or dysphagia which could be warning signs of potential airway problems. Any suspicion should
warrant specialist examination with indirect
laryngoscopy and CT/MR imaging. Massive neurofibromas of the face also have been reported which make mask ventilation extremely
difficult.5 Fiberoptic intubation has been the gold standard for difficult airway management. Nevertheless, there have been documented cases
of patients with NF1 with failed awake fiberoptic intubation due to grossly distorted anatomy who eventually required tracheostomy.6 In our
case tracheostomy was considered not feasible due to the fixed flexion deformity of the neck. Simple maneuver like patient protruding the
tongue actively helped significantly in our case to negotiate the fiberoptic bronchoscope which was not possible with passively pulling tongue
out by assistant. Hence the plan of awake fiberoptic intubation with conscious sedation with dexmedetomidine entailed us the advantage of
patient responding to verbal commands and simultaneously being cooperative for the procedure. It is also of immense importance in
awakening the patient in case of a can't intubate scenario.
Intraoperative neuromonitoring provides a real-time neurological status to guide intraoperative manoeuvres and decisions. Traditionally,
SSEP has been the mainstay of IOM. However, SSEP only directly monitors the ascending (sensory) pathways within the spinal cord. It may
fail to reflect spinal cord injury that affects the descending (motor) pathways.7 Hence Combined SSEP and MEP monitoring, with its high
sensitivity of 98.6% and specificity of 100% is an effective method for monitoring spinal function during spine surgery and obviates the need
of an intraoperative wake up test.8 There have been many documented cases of scoliosis surgeries where fall in MEP’s from baseline has
alerted the surgeons to a possible injury to the cord and prompt adjustment of instrumentation has prevented a possible permanent neurological
injury. In our case a sudden fall in MEP during mass screw fixation prompted the surgeon to redo the screws which probably released traction
on the cord and returned the MEP’s to baseline. Other possible causes of interference with recording of evoked potential including MAC of
inhalational anaesthetic, hypothermia, hypotension and haemodilution have been ruled out in our case. Therefore, a successful interpretation
of IOM requires a close working relationship among the surgeon, anesthesiologist and the neurophysiologist.
REFERENCES:
1. 1. Boyd KP, Korf BR, Theos A. Neurofibromatosis type 1. J Am Acad Dermatol. 2009;61(1):1-14.
2. Bagam KR, Vijaya DS, Mohan K, Swapna T, Maneendra S, Murthy S. Anaesthetic considerations in a patient with von Recklinghausen
neurofibromatosis. J Anaesthesiol Clin Pharmacol. 2010;26(4):553-4.
3. J. B. Craig, S. Govender .Neurofibromatosis Of The Cervical Spine A Report Of Eight Cases J Bonejoint Surg [Br] 1992, 74-B; 575-8
4. N. P. Hirsch , A. Murphy J. J. Radcliffe Neurofibromatosis: clinical presentations and anaesthetic implications British Journal of
Anaesthesia 2001; 86(4)
5. Saini S, Bansal T. Anesthetic management of difficult airway in a patient with massive neurofibroma of face: Utility of Rendell Baker
Soucek mask and left molar approach for ventilation and intubation. J Anaesthesiol Clin Pharmacol. 2013;29(2):271-2.
6. H. Wulf, G. Brinkmann, M. Rautenberg. Management of the difficult airway. A case of failed fiberoptic intubation.Acta Anaesthesiol
Scand. 1997 Sep; 41(8): 1080–1082.
7. Kim SM, Kim SH, Seo DW, Lee KW. Intraoperative neurophysiologic monitoring: basic principles and recent update. J Korean Med Sci.
2013;28(9):1261-9.
8. Padberg AM, Wilson-Holden TJ, Lenke LG, Bridwell KH. Somatosensory- and motor-evoked potential monitoring without a wake-up
test during idiopathic scoliosis surgery: an accepted standard of care. Spine (Phila Pa 1976). 1998;23(12):1392-1400.
10CASE REPORT III: ANESTHESIOLOGY
Anaesthetic challenges in management of a large thyroid with retrosternal
extension with thymic mass : A case report
Dr. Samidha Waradkar Thakur, DA, DNB Anaesthesiology, PGDMLS,
Consultant Anaesthesiology
Dr. Munasshira Sayeed, Resident DNB Anaesthesiology
Dr. Sasi Mouli, Endocrine Surgery, Junior Consultant, MS, DNB (General Surgery),
FMAS, MCh(Endocrine Surgery)
Dr. Amol Bhanushali, MS, FICS, FALS(VATS), FMAS, FIAGES,
Fellowship in Thoracic Surgery
Dr. Ritesh Agarwal, Consultant Endocrine Surgery, MS (General Surgery),
MCh (Endocrine Surgery), FAIS
Lt. Gen (Dr.) V. Ravishankar, MS, DNB (General Surgery),
MCh (Cardiothoracic Surgery), Consultant - Cardiovascular and Thoracic Surgery
Key words:
VATS-Video assisted thoracoscopic surgery, OLV-One lung ventilation, DLT-Double lumen tube, BP-blood pressure, etCO2-end tidal CO2,
Paw-peak airway, MAC-minimum alveolar concentration, ABG-arterial blood gas
Abstract:
Thyroidectomy is the most common endocrine surgical procedure being carried out throughout the globe[1,2]. Preoperatively, deranged thyroid
physiology warrants optimal preparation, while anticipated difficult airway due to enlarged thyroid gland further adds to the anaesthetic
challenges. The complexity of surgical intervention adds to these existing challenges.[3]
Thymoma is the most frequent type of tumour in the anterior-superior mediastinum. The presentation of thymomas is variable.[4]
This case report discusses various perioperative anaesthetic challenges and considerations during management of a large thyroid mass with
retrosternal extension along with a thymic mass.
INTRODUCTION:
Thyroid disease has been long recognized: goitres were first described by the Chinese in 2700 BC[5]. Retrosternal goitres usually cause
compression of mediastinal structures and may also cause serious complications like cerebral hypoperfusion and axillosubclavian vein
thrombosis[6].
Management of large thyroid mass with thymoma requires a comprehensive contingency plan involving anaesthetist, endocrine surgeon and
CVTS surgeon who are experienced in recognition,assessment & management of potentially difficult airway, possibility of acute
cardiorespiratory decompensation, blood loss, post operative pain management & rehabilitation.
Case report:
46yr old obese female with a BMI of 32kg/m2 incidentally detected with thyroid nodule having retrosternal extension on CT done for COVID
pneumonia in April 2021 posted for total thyroidectomy with bilateral neck dissection with VATS sos sternotomy.
Preoperative evaluation:
Patient was vitally stable. All her routine investigations, ECG, 2Decho were found to be normal.
11Chest X-ray showed mild tracheal shift to the right side.
USG neck showed multinodular goiter with retrosternal extension on
left side.
PET CT showed heterogeneously enlarged soft tissue lesion in
anterior mediastinum possibly in continuation with the left lobe of
thyroid. (Fig:1&2)
Premedication:
T.Pan-D 40mg two hours prior to surgery.
After confirming her adequate fasting status, was taken inside OR.
Fig 1: PET showing Fig 2: PET image showing
Intraoperative: retrosternal mass mediastinal mass
All ASA monitors attached.
Two large bore IV accesses of 18G secured.
Left radial arterial line insertion done under LA.
Induction: IV.Fentanyl 100mcg,IV.Midazolam 1mg, IV.Ondansetron 8mg, IV.Glycopyrrolate 0.2mcg,
IV.Propofol 150 mg, IV.Cisatracurium 10mg.
The intraoperative plan was confirmed with endocrine surgeon and thoracic surgeon, Intubation was
done using 37Fr DLT. The position of DLT was confirmed using fiberoptic bronchoscope.
Position: Supine.
Monitoring: ECG, SpO2, Invasive BP, EtCO2, Temperature, Urine output, ABG, MAC, PaW.
For total thyroidectomy with neck dissection both the lungs were ventilated.
Maintenance: Air:O2 =50:50 mixture, sevoflurane 1-2% & boluses of cisatracurium. Once VATS was
started OLV was initiated ventilating only the left lung.
Total intraoperative duration of surgery along with anaesthesia was 8 hrs out of which OLV was for
2hrs.(Fig 3) At the end, the patient was reversed and extubated without any sequelae. The surgeon gave Fig 3: Total surgical specimen
intercostal nerve blocks under vision for post operative pain relief and was shifted to ICU for further in anatomical position
observation.
DISCUSSION:
Surgery for goiter may vary from simple excision to manubriotomy,
sternotomy, thoracotomy or minimally invasive VATS[7][8].
In the current environment of enhanced recovery protocols and cost
containment, VATS suggests adoption of individualised tailored,
precise anaesthesia. In addition to a perfect lung collapse for surgical
interventions with adequate oxygenation during OLV, anaesthesia
goals include a rapid, complete recovery with adequate postoperative
analgesia leading to early discharge and minimised costs related to
postoperative inpatient services.
OLV is achieved by DLT having tracheal cuff & bronchial cuff.
Tracheal lumen terminates above the carina while bronchial lumen is
angled to fit the appropriate main stem bronchus[9]. The most accurate
method of selecting the correct size DLT is by measurement of left Fig 4: Labelled picture of DLT
main stem bronchus diameter by CT scan. (Fig:4)[10]
Patients requiring OLV are at an increased risk of developing acute lung injury. The suggested ventilator strategies as part of lung protective
strategies include[11]:
1. Maintain FiO2 as low as possible.
2. Low tidal volumes (6 ml/ kg predicted body weight).
123. To maintain Paw as low as possible, not more than 35 cm H2O.
4. PEEP of 5-8 cm H2O.
5. Frequent recruitment manoeuvres.
6. Permissive hypercapnia.
To conclude, the optimal technique of lung isolation will depend on several factors, including the indication for OLV, the patient’s airway, the
expertise of the anaesthetist and the availability of equipment.
CONCLUSION:
The perioperative morbidity in patients with thyroid disease having thymic mass can be greatly reduced by proper preoperative preparation &
optimization of their physiologic status, management of airway and ventilation and postoperative pain management.
REFERENCES:
1. Dionigi G, Dionigi R, Bartalena L, Tanda ML, Piantanida E, Castano P, et al. Current indications for thyroidectomy. Minerva Chir.
2007;62:359–72. [PubMed] [Google Scholar]
2. Agarwal G, Aggarwal V. Is total thyroidectomy the surgical procedure of choice for benign multinodular goiter? An evidence-based
review. World J Surg. 2008;32:1313–24. [PubMed] [Google Scholar]
3. Hardy RG, Bliss RD, Lennard TW, Balasubramanian SP, Harrison BJ, Dehn T. Management of Retrosternal Goitres. Ann R CollSurg
Engl. 2009;91:8–11. [PMC free article] [PubMed] [Google Scholar]
4. Elisabetta Congedo 1, Paola Aceto, Alexander Cardone, Rosanna Petrucci, Alessandra Dottarelli, Germano De Cosmo.
5. Huins CT, Georgalas C, Mehrzad H. A new classification system for retrosternal goitre based on a systematic review of its complications
and management. Int J Surg. 2008;6:71–76.
6. Santos GH, Ghalili K. Axillosubclavian vein thrombosis produced by retrosternal thyroid. Chest. 1990;98(5):1281- 3.
7. Shrager JB, Deeb ME, Mick R, Brinster CJ: Transcervicalthymectomy for myasthenia gravis achieves results comparable to
thymectomy by sternotomy. Ann ThoracSurg, 2002; 74:320-6.
8. Bramis J, Diamantis T, Tsigris C: Video-assisted transcervicalthymectomy. SurgEndosc, 2004 ; 18 :1535-538.
9. V. Ashok and J. Francis* Norfolk and Norwich University Hospital NHS Trust, Norwich, UK
10. Eberle B, Weiler N, Vogel N, et al. Computed tomography based tracheobronchial image reconstruction allows selection of individually
appropriate double lumen tube size. J Cardiothorac Vasc Anesth 1999; 13: 532e7
11. Kilpatrick B, Slinger P. Lung protective strategies in anaesthesia. Br J Anaesth 2010; 105: 108e16.
13Home Sample Collection
Across the City
• WESTERN LINE (Churchgate to Bhayander)
• CENTRAL LINE (CST to Kalyan) • HARBOUR LINE (CST to Panvel)
Appointments Collection Charges
8879677193 / 8879677196 ` 250
(call between 9am to 5pm per visit per person
from Monday to Saturday)
14CASE REPORT IV: PLASTIC SURGERY
Extensive Degloving Injury of the Abdomen and Thigh:
A multidisciplinary approach
Dr. Leena Jain, MS (General Surgery), MCh - Plastic Surgery,
Consultant Plastic and Reconstructive Microsurgeon
Dr. Dilroop, Post Graduate - General Surgery
Dr. Narender Nikam, MS, FMAS, FBMS, FRAGES, FLCS,
Consultant General and Laproscopic Surgeon
Dr. Prakash Jaindhani, MD (Emergency Medicine), Intensivist
A young male patient was shifted to Lilavati Hospital from another tertiary care hospital 48 hours following a high velocity run over accident
on August 15th 2021. He had an open massive, heavily contaminated, degloving injury of the entire infraumbilical anterior abdominal wall,
scrotum, penis, bilateral groin and complete right anterior thigh along with pelvic fracture. He was conscious, vitally stable but on the
ventilator with foul smelling wounds and discharge.
There were neither any visceral injury nor any long bone fractures. There was a distal penile urethral tear. On arrival, supportive management
was started. He was taken for a pulse lavage of the wounds and extent of degloving was evaluated. The degloving in the abdominal wall was
through a plane below the anterior rectus sheath, so the entire aponeurotic layer along with skin and subcutaneous tissue were lost; hwoever
the rectus abdominis muscle was intact completely. Degloving extended from just below the umbilicus to just below the left inguinal region
and on the right side it extended along the inguinal ligament, anterior thigh upto just above the knee joint. Transversely it extended from right
ASIS to left ASIS and medial to lateral thigh border. Right iliac crest was exposed from anterior superior iliac spine to laterally for about 3-4
cms. The right femoral triangle was deroofed hence, femoral neurovascular bundle lay exposed. In the midline phallus and scrotum were
degloved till base of scrotum resulting in exposure of both testes. There was extensive contamination in between all muscle planes with gravel
and sand. There was necrosis of entire right sartorius, rectus femoris, vastus lateralis, and parts of vastus medialis (figure 1). A thorough
debridement was done. Gracilis muscle flap was used to cover the femoral triangle Tracheostomy was done in view of repeated surgeries and a
relook debridement done 48 hours later with left orchidectomy in view of degloving and ischemia. Distal half of gracilis was dead and hence
debrided, with sparingly less cover on femoral artery. Negative pressure wound dressing was then applied. Subsequently all wounds were
covered with cadaveric human skin as skin is the best biological dressing. However, a check dressing three days later revealed loss of almost
entire homograft. Patient had a few temperature spikes and antibiotics were stepped up as per culture reports which had grown Klebsiella. The
wound continued to look unhealthy till about 4th NPWT dressing change and then it started improving. NPWT was continued for two more
weeks and partly exposed femoral artery and iliac crest also were covered with healthy granulation (figure 2). For a definitve cover, once the
wounds were well granulated, split skin graft was harvested from his left thigh and leg using an electric dermatome. The grafts were expanded
using a mesher to1.5times, anchored on the wounds with staples and immobilised using NPWT. Graft take up was about 92-95 %; residual
scattered raw areas started healing with dressings (figure 3). Definitive urethral repair was planned secondarily.
He was then rehabilitated with physiotherapy, decannulation and high protein diet. Two months after discharge, his grafts and donor sites are
supple and well healed. He can walk for about 4-5kms continuously. For his extensor lag, he is on quadriceps strengthening exercises.
Fig 1: Extensive degloving of anterior Fig 2: Wound bed preparation by repeated Fig 3: Healed wounds after skin grafting.
abdominal wall and penis. debridements and NPWT dressing
15DISCUSSION
Degloving injuries of abdominal wall are rare compared with those of extremities. In the latter, bone provides a solid counteractive force, while
in the former, degloving occurs against the musculo-aponeurotic layer, a tough structure comparable to bone(1).Toughness of this same layer
usually protects the viscera and solid organs in such injuries .
Extensive degloving injury can induce septicaemia in view of contamination, devitalisation of tissues, haematoma and progressive catabolis(2).
The outcome of these injuries depends on extent of acute haemorrhage, haemodynamic instability, hypoproteinaemia, complications of
massive transfusion, heavy contamination of wounds, sepsis, ARDS and MODS(3).
After initial stabilization, repeated debridements to reduce colonization are the key in prevention of septicaemia.
At primary presentation, harvesting skin graft from the degloved abdominal/ thigh flap is an invaluable therapeutic option to cover the
extensive wound before inflammation sets in. This spare part surgery reduces blood loss, chances of infection and need for extensive grafts in
the setting of limited donor site availability, secondary intention wound healing and scar formation which decreases skin plasticity. It promotes
faster wound healing and rehabilitation (4). Homografts from skin banks are quite helpful in such settings till wounds start showing signs of
healing and grafting can be planned. Due to extensive area of degloving, local/distant flaps were not an option.
When the patient presents later where the golden period is lost, negative pressure wound therapy plays an essential role for an optimal outcome.
CONCLUSION
A multidisciplinary approach is essential in management of such devastating injuries. Debridements, NPWT and skin grafting are the key
players to ensure a successful outcome.
REFERENCES:
1. Sonmez, A., Bayramiçli, M., Numanoglu, A. Degloving injury of the anterior abdominal wall. Plast Reconstr Surg. 2002; 110: 363.
2. Kudsk KA, Sheldon GF, Walton RL. Degloving injuries of the extremities and torso. J Trauma 1981;21:835e9.
3. Veena PW, Babu R, Venkatesh MS, Udayashankar C, Deepak KL.. Degloving injuries of the abdominal wall. journal of woundcare vol 22, no 10, October
2013
4. Raposo-Amaral CE, Denadai R, Raposo-Amaral CA . Degloving injury of the abdomen and external genitalia successfully treated with full-thickness
degloved skin graft in a child: A 10-year follow-up. J Plast Reconstr Aesthet Surg. 2014 May;67(5):735-7.
16FOR APPOINTMENT CALL: 8657896447
(BETWEEN 9AM TO 5PM)
17Call: 8291280428
between 9am to 5pm Monday to Saturday
18IMPORTANT INFORMATION
KINDLY NOTE OUR NEW BOARD LINE NUMBERS
022 69318000 AND 022 69301000
FOR HEALTH CHECK-UP APPOINTMENT
8657896447
OUR NEW DIRECT CONTACT NUMBERS
FOR DOCTOR'S APPOINTMENT
8657907751/52/53
FOR VISA APPOINTMENT
8657907756
19CASE REPORT V: HISTOPATHOLOGY
KIKUCHI FUJIMOTO DISEASE IN CHILDREN – an Uncommon Entity
Dr Shalini Saurabh, Clinical Associate
Dr Chandralekha Tampi, MD (Pathology), Consultant Histopathologist
BACKGROUND
Kikuchi Fujimoto disease, a histiocytic necrotising lymphadenitis is an uncommon benign cause of lymph nodal enlargement with a self
limited evolution most commonly seen in Japan and other Asian countries. It was first described by Kikuchi and Fujimoto in 1972 , in Japan(1).
Patients are usually young women between the ages of 20-35 years presenting with painless persistent cervical lymphadenopathy of modest
dimension accompanied by fever, and it is uncommon in children(2). Also, unlike in adults,which shows female preponderance,in children , the
ratio is reversed, being 2.8 :1(3), being more common in male children. Paediatric patients also present with painless lymphadenopathy most
commonly in the cervical lymph nodes accompanied by flu like symptoms. Etiology is unknown but EBV, HHV8, HHV6 and other viruses
have been implicated(4). The most important differential diagnosis are with malignant lymphoma on clinical and also on histopathological
examination.
CASE REPORT
This review reports two unusual cases of Kikuchi Fujimoto disease, both in children.
The first one involves a 12 year old male child presenting with fever and headache and enlarged and persistent lymphadenopathy in the neck
and inguinal region since three weeks.Imaging showed lymph nodes seen in neck and left inguinal region, with non-necrotic thickened cortex.
An excision of one of the lymph nodes was done.
The second case is of a six year old female presenting with recurrent fever spikes since one month.She had multiple enlarged lymph nodes in
both sides of the neck.One lymph node was excised.
MICROSCOPIC EXAMINATION
In both cases, the excised lymph nodes showed a fairly similar appearance. The lymph nodes showed preserved architecture with variably
sized follicles in the cortex with paracortical expansion and increased vascularity (Fig 2 &3).Variably sized paracortical non expansile
necrotizing lesions were seen with mildly atypical lymphoid proliferation, karryorhectic debris, monocytoid and plasmacytoid histiocytes and
few phagocytic histiocytes with peripherally placed crescentic C shaped nuclei (Fig1). No neutrophils ,plasma cells or granulomas were seen.
IHC with CD123 highlighted the plasmacytoid dendritic cells (Fig 4).
Fig 1: NECROTISING AREAS IN Fig 2: IHC with CD20 HIGHLIGHTS Fig 3: IHC with CD3 HIGHLIGHTS Fig 4: IHC with CD123 HIGHLIGHTS
H & E stain (400x) THE CORTICAL LYMPHOID THE T CELL ZONE (400x) THE PLASMACYTOID
FOLLICLES (40x) DENDRITIC CELLS (400x)
A diagnosis of Kikuchi Fujimoto disease was made.
In both cases, they were given symptomatic treatment and their symptoms and lymphadenopathy resolved.
DISCUSSION
The differential diagnosis of cervical lymphadenopathy includes reactive, infectious and neoplastic causes. Nodes suspected of being
infectious or neoplastic are those that come most often for pathological evaluation. Kikuchi disease is a rare self limiting benign cause of
cervical lymphadenopathy and fever with a mildly atypical lymphoid proliferation which can mimic lymphoma(5). The additional
characteristics of a non expansile histiocytic necrotising areas on microscopic examination, and the IHC profile, help to differentiate it from
20Lymphoma. Although rare, Kikuchi Fujimoto disease(KFD) must be considered in the differential diagnosis of persistent lymphadenopathy in
children, especially in Asian pediatric patients. In addition to cervical lymphadenopathy, axillary and supraclavicular lymphadenopathy have
also been reported(6,7). Tenderness of the lymph nodes may or may not be present. The characteristic histological features, supported by
immunohistochemical staining is useful in distinguishing Kikuchi Fujimoto disease from other differentials. The prognosis is excellent, but
some have recurred and occasionally have also developed SLE subsequently(8). Some studies have shown that the characteristic necrosis is due
to cytotoxic lymphocyte mediated apoptotic cell death(9). Etiology is unknown but EBV, HHV8, HHV6 and other viruses have been
implicated(4).The treatment is aimed at symptomatic control and it usually resolves within six months. However patients can be placed under
follow up, as 12-14 % of them can recur (10)
CONCLUSION
Paediatricians should also consider Kikuchi Fujimoto disease in the differential diagnosis of persistent lymphadenopathy, with fever of
unknown origin.Excision biopsy of the node for histopathological evaluation is important for an accurate diagnosis .
REFERENCES:
1. Fujimoto Y, Kojima Y, Yamaguchi K. Cervical subacute necrotizing lymphadenitis. A new clinicopathological entity. Naika. 1972;20:920–7.
2. Erna Kristiani, Selina Natalia, Elizabeth Victoria Fedora Ritonga, Stanislaus Djokomuljanto, Erick Fransisco Kan,Kikuchi-Fujimoto Disease in
Pediatrics,Journal of Pediatric Surgery Case Reports,Volume 73,2021,
3. Hye jeong han et al,Gye–Yeon Lim et al, Kikuchi disease in children: clinical manifestations and imaging features 2009,dec;24(6);J Korean Med Sci
4. C.-H. Chuang, D.-C. Yan, C.-H. Chiu, Y.-C. Huang, P.-Y. Lin, C.-J. Chen, et al. Clinical and laboratory manifestations of Kikuchi's disease in children and
differences between patients with and without prolonged fever
5. Chamulak GA, Brynes RK, Nathwani BM. Kikuchi-Fujimoto disease mimicking malignant lymphoma. Am J Surg Path. 1990;14:514–23.
6. Kukukardali Y, Solmazgul E, Kunter E, et al. Kkikuchi-Fujimoto disease: analysis of 244 cases. Clin Rheumatol. 2007;26:50–44.
7. Bosch X, Guilabert A, Miquel R, Campo E. Enigmatic Kikuchi Fujimoto disease: a comprehensive review. Am J Clin Pathol. 2004;122:141–52.
8. Chen HC, Lai JH, Huang GS, Gao HW, Chen CH, Kuo SY, Chang DM. Systemic lupus erythematosus with simultaneous onset of Kikuchi-Fujimoto's
disease complicated with antiphospholipid antibody syndrome: a case report and review of the literature. Rheumatol Int. 2005;25(4):303–306.
9. Rosai and Ackerman Surgical pathology, edn tenth, chapter- Lymph nodes, pg no 1785
10. Shoba N Selvanathan et al. Kikuchi-Fujimoto disease in children,J Paediatr Child Health. 2020 Mar.
21CASE REPORT VI: ORTHOPAEDIC
MASQUELET TECHNIQUE
Dr Shahrookh Vatchha, MS (Ortho), Consultant Orthopaedic Surgeon
Dr Mahesh H Patel, DNB Resident
Dr Amit Kohli, D. Ortho, Fellowship in Spine and Arthroplasty,
Consultant Orthopaedic Surgeon
ABSTRACT
Masquelet technique, which is the use of a temporary cement spacer followed by staged bone grafting, is a recent treatment strategy to manage
a posttraumatic bone defect. This paper describes a case of 65-year-old, female patient treated with this technique of staged bone grafting
following placement of an antibiotic spacer to successfully manage infected osseous long bone defects. The injured limb was stabilized and
aligned at the time of initial spacer placement. In our case, osseous consolidation was successfully achieved. This technique gives promising
result in the management of posttraumatic bone defects, infected non-union, large bone defects.
INTRODUCTION
Bone defects of limbs refer to the bone defects with no new bone formations or the areas where regenerated new bone is less than 10% of the
bone defect at the limbs. The length of such bone defect is about 2–3 folds of the defect diameter, which is generally caused by trauma, resection
of malignant tumours, or chronic osteomyelitis. Bone defects are considered challenging to manage, especially the long segmental bone
defects with the lengths >5 cm, which generally require complex treatments, resources from multiple departments, and interventions from
various experts. At the same time, the outcomes are still unknown. Currently, clinical treatments for bone defects of limbs include simple bone
grafting, membrane induced osteogenesis (namely Masquelet technique), placement of iliac or fibular bone grafts with blood vessels separated
with microsurgical techniques, and bone transport under external fixation. All these methods have their own advantages in repairing bone
defects and lead to good outcomes. But there are corresponding indications for all such methods. For instance, when the bone defects are ≤5
cm, autogenic or allogenic bone grafting is generally applied. In comparison, for the bone defects >5 cm, placements of bone grafts with blood
vessels or the Ilizarov bone transport technique is used. Besides, the risk of bone resorption in bone defects >5 cm is increased even when the
defects are well-covered with soft tissues. Masquelet technique, which provides a safe but straightforward method for the treatment of long
segmental bone defects, was first reported by Masquelet et al. in 1986. Treating bone defects with Masquelet technique includes two stages: the
first stage includes complete debridement, maintaining the stability of fracture ends, placement of bone cement, and closing the wound without
tension; the second stage operation, which is per formed 6–8 week later, the induction membrane is cut open, and the bone grafting is
performed after removing the bone cement. The primary principle of the Masquelet technique is inducing pseudo membrane by the
physiological foreign-body reactions surrounding the polymethyl methacrylate (PMMA) spacer. In the second stage, the PMMA spacer is
replaced by the bone grafts to stimulate the bone union. Masquelet technique has been widely applied and optimized by numerous researchers
since the first report, especially for patients with long segmental bone defects and insufficient volume of autogenic bone, or with the risk of
inducing dangerous complications in the donor area, which could cause more pain to the patients. No previous studies have investigated the
quantitative relationship between the size of bone defects and volumes of autogenic bone grafts. In this study, we retrospectively analysed the
data from patients with bone defects treated with the Masquelet technique at our hospital and further investigated the relationship between the
size of bone defects and bone graft volumes. The aim of this was to achieve good clinical effectiveness by performing sufficient preoperative
preparations and reducing the complications of the Masquelet technique.
CASE REPORT
A 60-year-old female, presented to our hospital with pain and discharging sinus at operative site on left distal thigh, immobilization since an
event of road traffic accident. Patient had a history of road traffic accident in November 2020, sustained comminuted fracture of left distal
femur, fracture left shaft tibia and fibula, fracture right shaft radius. Patient was operated for same with ORIF (open reduction internal fixation)
of left distal femur fracture and right radius shaft fracture, and with intramedullary nailing and screws at left tibia shaft fracture, at KEM
22You can also read

















































