Prostheses List Reform - Scope and Definition - September 2021 Australian Private Hospitals Association ABN 82 008 623 809
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Prostheses List Reform – Scope
and Definition
September 2021
Australian Private Hospitals Association ABN 82 008 623 809
Contents
Executive summary........................................................................................................... 1
The Department of Health’s questions ............................................................................ 5
Definition and Scope ..................................................................................................... 5
Criteria .......................................................................................................................... 6
Name ............................................................................................................................. 7
Consequence of Changes .............................................................................................. 7
Defining the Scope of the List........................................................................................... 8
Why definition by exception will not work ................................................................... 8
Why the proposal to remove several categories from the Prostheses List is not
supported ....................................................................................................................... 11
The underlying premise of this response ................................................................... 11
The problem to be solved by reform .......................................................................... 11
Problems with the Government’s proposed solution ................................................ 12
The Government has not acknowledged the radical nature of this proposal. ...... 12
The Government has not acknowledged the breadth of impact created by this
proposal. ................................................................................................................. 13
The Government’s confidence that items removed from the PL will be funded by
alternative (i.e. contractual mechanisms) without impact on the range of
technologies provided to doctors, the range of services provided, access to
services and patient out of pocket costs, is misplaced .......................................... 17
Relations with private health insurers are already strained. ................................. 20
The presumption that contractual funding mechanisms that exist in overseas
jurisdictions can be applied within the Australian context is flawed because it fails
to recognise particular characteristics of the Australian healthcare sector. ......... 20
Even though the Department has acknowledged that a reform of this magnitude
cannot be made ‘overnight’, they have failed to appreciate the complexity of task.
................................................................................................................................ 22
Removal of items from the PL is not an acceptable remedy because it is not
assured of achieving the intended aim. ................................................................. 24
The proposed reform carries the risk of consequences for the health sector as a
whole. ..................................................................................................................... 25
The business risks posed by this reform are further heightened for those
operators directly impacted by COVID-19. ............................................................ 25
Removal of categories from the PL makes no sense in terms of wider policy
objectives. ............................................................................................................... 25
Several alternative funding mechanisms have been explored by stakeholders but
each are seriously deficient. ................................................................................... 26
APHA’s alternative proposal ........................................................................................... 27
Use of TGA definitions .................................................................................................... 30
Timeframe and additional requirements in the event the Government rejects APHA’s
proposal and proceeds to remove items from the PL .................................................... 31
The context for reform and radical nature of the changes proposed ........................ 32
The decision-making process ...................................................................................... 32
Putting basic safeguards in place................................................................................ 33
Adequate notification ................................................................................................. 34
Transitional Funding Arrangements ........................................................................... 34
Appendix A: Clinical Implementation Reference Group ................................................ 36
Appendix B: The impact of the COVID-19 Pandemic ..................................................... 37
Overview of the impact to date .................................................................................. 37
Impact on the use of PL items .................................................................................... 40
Future outlook ............................................................................................................ 41
Implications for Reform .............................................................................................. 41
Appendix C: Concurrent Review and Reform Processes ................................................ 43
Appendix D: The Department of Health’s proposed changes to the Prostheses List .... 44
Intraocular Fluids ........................................................................................................ 46
Drug delivery devices .................................................................................................. 47
Enteral tubes ............................................................................................................... 48
Haemostatic devices ................................................................................................... 49
Closure devices ........................................................................................................... 52
Arterial closure devices ............................................................................................... 56
Dura defect repair ....................................................................................................... 57Executive summary
In this submission the Australian Private Hospitals Association (APHA) will not only
respond to the questions posed in the Department of Health’s (the Department)
consultation paper but also take account of the Australian Government’s key concerns
by considering the following questions:
• How can decisions about the listing of products on the Prostheses List (PL) be made
with greater clarity and consistency?
• How can the PL be reformed to operate in a way which does not suppress the
advantages for consumers which could otherwise arise from price competition?
• How can these two concerns be addressed while ensuring continued consumer
access to the technologies currently funded through PL and the services they
enable and ensuring protection of consumers from out-of-pocket costs?
APHA agrees that the PL is in need of reform. The PL has been central to protecting
consumers, payers and hospitals economic challenges that are specific to the
Australian private health sector, but in doing so it has also dampened incentives for
manufacturers to compete on price1.
However, APHA disagrees with solution proposed in the Department’s consultation
paper (i.e. the proposal to remove a number of categories from the PL) for the
following reasons:
• The Government has not acknowledged the radical nature of this proposal.
• The Government has not acknowledged the breadth of impact created by this
proposal.
• The Government’s confidence that things removed from the PL will be funded by
alternative mechanisms, i.e. commercial contractual arrangements between
hospitals and health funds, without impact on the range of technologies provided
to doctors, the range of services provided, access to services and patient out-of-
pocket costs is misplaced.
• All alternative mechanisms that do not rely on contractual negotiations between
hospitals and health funds have been shown to be either excessively complex or
unfair and inaccurate.
• Even though the Department has acknowledged that a reform of this magnitude
cannot be made ‘overnight’, it has failed to appreciate the irreducible level of
complexity and systemic risks involved.
APHA has consistently advocated that the reform process, and specifically any
proposed removal of items from the PL, should be informed by independent clinician-
led review and welcomes the decision to establish a Clinical Implementation Reference
1
Department of Health, Regulation Impact Statement (RIS) Improving the Private Health Insurance
Prostheses List, Office of Best Practice Regulation (BOPR) ID number: 4319. Canberra, 2021
1Group. This submission sets out the way in which the proposed removals will directly
impact key areas of clinical service in which the private hospital sector plays a central
role.
Data presented also shows doctors play the decisive role in determining when and
how these technologies are used. Many of these technologies are used selectively to
meet the needs of individual patients, including high risk patients. This data shows that
the role of the PL in ensuring that doctors have access to the technologies they need is
as important for the categories of device that the Department wants to remove from
the PL as it is for categories of device that have never been considered inappropriate
for inclusion.
This data underlines how important it is that all proposed reforms be subject to clinical
review. Specific recommendations as to how the reform process should be informed
by an independent clinical perspective are set out at Appendix A: Clinical
Implementation Reference Group on page 36.
Formal mechanisms for ensuring reform and management of the PL is informed by an
independent clinical perspective should be established and resourced on a permanent
basis.
The risks involved in the proposed reform are known and extensive while the
likelihood of the intended aim being achieved is uncertain. This reform proposal risks
significant consequence for the health sector as a whole. The risks posed by these
reforms are further heightened by the current and ongoing impact of the COVID-19
pandemic on private hospitals. These risks are disproportionate to the benefits sought.
By contrast, the fiscal conditions for the private health insurance sector are currently
better than in recent years, providing the opportunity for a more considered and
gradual approach to reform.
APHA proposes a less risky alternative. First, no categories on the PL should be
removed. Rather the PL should be segmented into three parts:
• PL MkI - those technologies for which doctor choice is important and those
technologies for which the conditions for price competition do not exist (even if
doctor choice is not important).
• PL MkII - those technologies for which doctor choice is unimportant and price
competition exists.
• PL MkIII - those technologies which are capital items that could be reused by more
than one patient.
Benefit setting mechanisms should be applied that suit the requirements of each of
these segments.
• PL MkI – benefits should be set through public sector reference pricing.
• PL Mk II – benefits should be set through public sector reference pricing in the first
instance and then through a refined reference pricing methodology which ensures
the benefits of price competition are even more effectively passed back to the
consumer.
2• PL Mk III – benefits should be set in accordance with the use life of the technology.
Going forward to ensure clarity and consistency in listing decisions:
• Applications falling within existing categories should continue to be accepted.
• Applications which do not should be accessed via a health technology assessment
(as the government has already committed to do) and, in addition, they should be
economically assessed in order to determine the appropriate strategy for benefit
setting and review (i.e. either PL MkI or PL MkII or PLMkIII).
• Concerns about whether an application is for an item already funded in theatre
banding should only arise if the item directly, and completely, replaces a
‘consumable’, and has no other more specialised application for which it might be
used in addition to standard consumables2.
APHA strongly commends this alternative for the Government’s consideration. The
APHA proposal meets the Government’s objectives by:
• Delivering price reductions for all PL items.
• Aligning structure of the PL with its purpose.
• Clarifying the scope by providing a test by which future applications can be
assessed as ‘consumables’ or not.
• Providing a benefit setting mechanism which ensures the outcomes of price
competition are passed back to consumers.
• Ensuring these objectives are achieved without exposing consumers out-of-
pocket costs or the loss of access to services on which they depend.
Should the Government decide to reject APHA’s proposal and conclude that its reform
objectives can only be achieved by removal of items from the PL, it will be absolutely
essential the Government rethink the timeline for implementation and make
additional investment in safeguards to protect consumers and ensure access to
services.
APHA has outlined in detail the minimum safeguards required. However, in doing so,
APHA continues to maintain the Government’s proposed intention to remove $225
million (2019) worth of technologies from the PL comes with an irreducible level of
systemic risk which will, if proceeded with, result in:
• Increased out of pocket costs for consumers.
• Reduction in the availability of services in the private sector.
• Increased reliance of the public sector to provide services for high-risk patients and
for communities in regional areas.
In discussions with the Department regarding a draft ‘Engagement Framework’ for the
PL Reform, APHA has always made clear private hospitals will:
2
In this context, the term ‘consumable’ should be taken to mean items identified by the National
Procedure Banding Committee’s (NPBC) Terms of Reference, February 2019.
3Subject to appropriate and sustainable contractual agreement between hospitals
and health funds for alternative funding arrangements, not charge out-of-pocket
costs to appropriately insured consumers for products used in a medical procedure
(including those products no longer eligible for PL listing).
The reliance on commercial negotiations between hospitals and health funds to
resolve alternative funding arrangements for items removed from the PL carries an
irreducible risk of out-of-pocket costs for consumers for the following reasons:
• If negotiations do not result in adequate reimbursement for items removed from
the PL, hospitals may have no option other than to pass costs onto the consumer
for items no longer covered.
• In discussions with APHA, the Department has conceded that health insurers are
unlikely to enter into commercial arrangements with all hospitals for items
removed from the PL. Hospitals ignored by insurers in this regard will have no
option other than to pass costs onto the consumer for items no longer covered.
• If negotiations fail completely, an increased number of hospitals will go ‘out-of-
contract’. This will mean health funds are obliged to pay only the relevant Second
Tier benefit, or minimum default benefit (which-ever is applicable) plus PL benefits
for items that remain on the List and the consumer will be directly liable for the
balance.
4The Department of Health’s
questions
Definition and Scope
Is the proposed approach to the definition of a kind of prosthesis flexible enough to
anticipate future technologies while providing sufficient clarity on the scope of the PL?
The proposed approach improves flexibility and the ability to anticipate future
technologies in so far as it removes the requirement a device be ‘implanted’. By so
doing, it allows consideration of a wider range of technologies and recognises the
evolution of technology has provided new treatment options.
The proposed reforms fail, however, to be flexible enough to recognise:
• The purpose of a device can sometimes be context specific.
• The fact that to remedy a disease or dysfunction may require use of multiple
devices in combination and it may not be possible to distinguish which is ‘the
specific’ and which ‘the adjunct’.
The proposed approach also fails to anticipate the economic impacts of future changes
as new technologies continue to emerge, clinical practice changes and markets
continue to evolve.
The proposal also fails to provide sufficient clarity:
• The distinction between ‘specific medical device’ and ‘adjunct medical’ is
ambiguous and contingent on clinical context.
• References to ‘accessories’ are unclear and potentially unfit for purpose
particularly in light of the very specific interpretation of this term within the
context of Therapeutic Goods Administration (TGA) regulations.
• The intent to remove ‘consumables’, results in a circular argument without
demonstrating the basis upon which an item is determined to be a ‘consumable’.
As such, it provides no basis for resolving future controversies which may arise as
new technologies emerge.
The attempt to define the PL negatively, i.e. by exceptions, immediately confounds any
gains in clarity by a change in terminology.
APHA proposes a different approach which recognises the centrality of the economic
role played by the PL, and the necessity of ensuring the technologies it has funded,
remain available. Rather than aiming to achieve clarity by removing items from the PL.
APHA proposes the existing List be segmented so that its effectiveness as policy tool
can be further refined. If the focus is on the purpose and function of the PL, form and
clarity will follow.
5Does aligning terms with established terms used by the TGA (such as medical devices
and biologicals) improve clarity?
Alignment of terminology will improve clarity if definitions are also aligned, but if the
policy intent of the PL requires different definitions, then it should have its own
distinct terminology when required.
Some of the information collected by the TGA will require clinical review to ensure it is
also fit for purpose in the context of the PL. This issue is discussed further in the
chapter Use of TGA definitions on page 30.
Criteria
Are the proposed listing criteria for Part A fit-for-purpose? If not, what changes are
needed?
The proposed listing criteria for Part A are not fit-for-purpose. This issue is further
discussed in the chapter Defining the Scope of the List on page 8.
Should the scope of products eligible for listing on Part B remain unchanged?
APHA makes no comment as to the scope of products eligible for listing on Part B and
reserves any comment it may make in light of the separate consultation already
foreshadowed.
Should the PL retain an option for the Minister to list items in exceptional
circumstances on Part C?
Given it is impossible to foresee the future direction of medical technologies and
likewise impossible to foresee the outcomes of future health technology assessments,
it is essential this provision be retained.
Are there any other exceptional circumstances factors that Part C should
accommodate?
APHA expresses no view as to other exceptional circumstance factors Part C should
accommodate.
Please consider the tables at Attachment B and explain which products meet the future
criteria for listing and the reasons why?
APHA welcomes proposals to include products listed in Attachment B within the PL as
a step forward in ensuring consumers have affordable access to contemporary care.
6Name
Should the name of the list be modernised and, if so, what should it be called?
APHA expresses no view as to the name of the list other than to refer to the comment
above regarding alignment with terminology used by the TGA.
Consequence of Changes
Does the list of items at Attachment A flagged for inclusion and removal accurately
reflect the proposed future criteria for listing?
APHA finds it impossible to comment because of the vague and ambiguous nature of
the criteria proposed. This issue is discussed further in the chapters Defining the Scope
of the List on page 8.
The removal of items identified at Attachment A is scheduled to commence from
February 2022. If a decision is taken to remove these items in tranches, is there a
logical bundling of the items at Attachment A that would make staged implementation
over time possible? Is the proposed staged removal aligned with PL updates workable?
What is the most appropriate timing?
Any proposal to announce in November changes effective from February 2022, would
be extremely damaging to the sector and consumers.
The proposed changes are radical in nature and, if proceeded with, will require an
extensive transition period together with implementation of government led
safeguards and monitoring processes. The proposed implementation also coincides
with a number of other proposed reform timelines will which compound the
complexity of any transitional period. These are detailed at Appendix C: Concurrent
Review and Reform Processes on page 43.
Furthermore, it is essential the financial impact of the COVID-19 pandemic be taken
into account, together with the high likelihood of continued uncertainty. These
matters are discussed further on pages 31 and following.
7Defining the Scope of the List
APHA supports the proposal to widen the scope of the PL to include both
surgically implanted or ‘single use-surgically invasive medical devices’
APHA does not support the proposal to narrow the scope of the PL to only
include devices ‘where the intention of the medical procedure is to remedy
disease or dysfunction through use of the specific medical device’, on the
basis this will remove many devices critical to a safe and successful
procedure.
APHA does not support defining the PL by exception.
Why definition by exception will not work
The Department’s consultation paper proposes to tighten the scope of the PL by
legislating three exceptions, but the problem with this approach is each of these
exceptions gives rise to further questions and ambiguities:
1. ‘General Purpose’:
• Why is it assumed a device used for ‘different types’ of procedures is
necessarily better funded through alternative funding arrangements?
• Why does the fact a specialised device used for ‘different types’ of procedure
make it necessarily less specific than a device is used for only one procedure?
• Would this exception not give rise to increased requests to list artificially
specialised devices?
• What differentiates devices which ‘assist other items’ from devices listed as
part of ‘systems’ or ‘surgical packs’ (as defined by the TGA)?
2. ‘Consumables’:
• Is this term clearly and readily understood?
• Are sutures, tubing, topical adhesives and sealants currently on the PL
inherently different from unlisted products generally referred to as
‘consumables’? If there are instances where clinicians require access to sutures,
tubing, adhesives or sealants with specific properties, this would suggest
sometimes the answer is ‘yes’.
3. ‘Accessories’:
• Can all ‘accessories’ be retained on the PL as part of a bundle (i.e. listed as a
‘system’ or ‘surgical pack’) with the device with which they are used?
• What about those products which are designed and intended by the
manufacturer to always be used together with another implantable or
8surgically invasive device but not included in ‘systems’ or ‘surgical packs’ as
defined by the TGA?
• What about those products designed to be compatible with devices made by
multiple manufacturers?
• Does listing in this way support the way in which they are actually used?
These categories of ‘exemption’ are neither helpful nor transparent. They do not
explain why some recommendations of the EY Report have been adopted while others
have not. They do not readily explain why a device needs to be funded through the PL
(or not)3. They do not reflect the way in which devices are actually used.
For example, infusion pumps and their accessories, are neither implanted nor
surgically invasive technologies, and arguably they might be excluded by any or all of
these exemptions. However, they require the PL as a funding mechanism because:
• Their use is determined by specific clinical requirements, for example the specific
rate and length of infusion required, the ability to provide infusions over long
periods of time on an ambulatory basis, the ability of patients to control the
infusion.
• Accessories are not always interchangeable and choice may be limited by the
technologies and context within which they are used.
• Although there are a number of products available in the Australian market, the
options available to meet specific clinical requirements are often limited and there
is little or no realistic prospect of substantial price competition.
• Their patterns of utilisation are not sufficiently regular for bundled funding
arrangements to be negotiated within acceptable limits of risk.
• Removal without adequate alternative funding mechanisms would result in
substantial disadvantage to consumers, out of pocket costs and loss of access to
essential services.
Each of the specific categories nominated for removal by the PL in the Department’s
consultation paper is further discussed at Appendix D: The Department of Health’s
proposed changes to the Prostheses List on page 44.
3
EY Consulting, Review of the General Miscellaneous Category of the Prostheses List, 13 July 2020.
9Defining the limits of the Prostheses List
The Government has raised concern the ‘the scope of the PL lacks specificity, meaning
there are no obvious limits on what is included in the PL’. Yet, clearly there are limits.
Generally reusable capital items used by more than one patient are not within scope. If
clarity is to be restored by removal of items for which eligibility has become
questionable in hindsight, the questions which must still be asked are:
1. What will be the impact on clinical care?
2. How else can adequate funding to access to these technologies be assured?
In the next two chapters this submission outlines, APHA’s objection to the proposal
that several categories of device should be removed from the PL and an alternative
proposal for achieving the Government’s reform objectives.
10Why the proposal to remove several
categories from the Prostheses List
is not supported
APHA is of the view that the risks associated with the proposed removal of several
categories from the PL poses substantial systemic risks and uncertain benefits in
contrast with alternative mechanisms for achieving the Government’s reform
objectives.
The underlying premise of this response
The purpose of the PL is to address economic challenges that are specific to the
Australian private health sector:
• The tendency within Australian medical device markets for the emergence of
dominant providers and markets within which products compete on attributes
rather than on price4
• The independence of the payer, the purchaser (hospitals) and the selector (doctor)
of medical devices5
• The open, demand driven, nature of the private hospital sector in which volume
and case mix are minimally constrained by the fee-for-service doctor, the capacity
of the hospital and the willingness of the consumer to pay.
The problem to be solved by reform
The PL has protected consumers, payers and hospitals from these challenges, but in so
doing it has also dampened incentives for manufacturers to compete on price 6.
4
Synder G et al The three rules in medical technology: The transformation of an industry, Deloitte
University Press,
5
EY Consulting, 13 July 2020.
6 Department of Health, Regulation Impact Statement (RIS) Improving the Private Health Insurance
Prostheses List, Office of Best Practice Regulation (BOPR) ID number: 4319. Canberra, 2021. APHA
acknowledges that the RIS also refers to concerns about PL items being used in preference to
alternatives and the potential of over-use of PL items. With respect to the first, APHA notes that as
clinicians are generally unaware of the PL, it plays no part in their decision making when they select
technologies for use. With respect to the second concern, APHA does not regard removal of items from
the list as a solution to this perceived problem rather, as was discussed in APHA’s February submission
the issue of utilisation should be addressed through engagement with clinicians. APHA, Prostheses List
Reform, February 2021. https://apha.org.au/wp-content/uploads/2021/03/APHA-Prostheses-List-
Reform-Feb-2020-FINAL-1.pdf
11Problems with the Government’s proposed solution
APHA agree with the problem identified by Government, but disagrees with the
proposed solution (i.e. the proposal to remove items from the PL).
The Government has not acknowledged the radical nature of this proposal.
• The proposed reform is a fundamental change to a funding mechanism that has
been in place in its current form for 20 years.
• The structural implications of imposing a change on the sector as a whole not only
has direct implications for all hospital operators, it also risks precipitating
fundamental shifts in the future availability and affordability of health services.
• Under current arrangements, individual hospital providers and health insurers can
and do, from time to time, elect to contract on a bundled basis for services that
would otherwise involve claims against the PL. APHA understands the practice is
extremely limited, possibly only used by one insurer, and confined to specific
services with simple and predictable requirements for which a case payment is
negotiated7. It is crucial to recognise the distinction between arrangements
entered into on mutually agreed terms between individual commercial parties, and
the scope of the reforms proposed which impose a systemic change upon the
sector as a whole.
• Imposing a change on the system as a whole means that all participants are
simultaneously placed in the situation of trying to reposition themselves. Hospitals
must therefore consider not only the internal impact of the reforms but also first
and second order consequences for their commercial partners, competitors and
the environment in which they operate.
This proposed reform outlined by the Department entails the removal of more than
$225million in PL benefits paid by private health insurers.
It is also imperative to recognise that these reforms will also directly impact services
paid for by other payers including the Department of Veteran’s Affairs, the
Department of Defence (through the ADF Health Services Contract) and compensable
payers whose rates are set either by commercial operators or relevant government
agencies. 8
7
A case payment is an agreed sum paid for a service of a particular description. It is negotiated
separately to other mechanisms such as DRG- based funding or models based on theatre bands.
8
The EY Report was in error when it failed to recognise that the PL is reference by other payers in
addition to private health insurers.
12It requires a change in the funding arrangements for services covering 2,429 separate
MBS items (2019) in addition to services for which no MBS item is indicated in
statistical data9.
This radical reform will directly affect the security of funding for more than 2.6 million
separations each year10, or 75 percent of the sectors overall activity11.
The Government has not acknowledged the breadth of impact created by this
proposal.
• The breadth of services implicated.
• The importance of those services for high-risk patients.
• The risks to patient access particularly for high-risk patients, for people in regional
areas and for people in communities served by smaller hospitals.
• The risks to patient access for services in which the private hospital plays a vital
role and consequent risks for the public hospital sector.
• Government has failed to acknowledge the materiality of the financial impact at
hospital level and particularly high financial risk for some services.
The impact will be felt across every private hospital and day hospital providing
surgically invasive procedures, endoscopic procedures, obstetrics as well of other
services using drug delivery devices such as chemotherapy and haematology, pain
management, clinical care of medical patients requiring infusions and palliative care.
Table 1 shows how important technologies that the Department wants to remove
from the PL are to selected areas of clinical service delivered by the private hospital
sector (this is not an exhaustive list of the clinical services affected by this reform).
9
The data used is this report was sourced from Hospital Casemix Protocol (HCP) data provided by the
Department of Health. This figure includes MBS for which data was suppressed by the Department to
preserve confidentiality and privacy. This data does not include activity funded by the Department of
Veterans Affairs, The Department of Defence or compensable payers.
10
This estimate is based on HCP data provided by the Department of Health and is a count of total
separations aggregated at the level of principal MBS in which use of the items in question was reported
(including suppressed data). This does not include separations for which no principal MBS was reported
so there is no way of knowing, without access to more detailed data, the size of the pool of separations
with no MBS for which alternative funding arrangements would need to be negotiated. This data
includes only activity funded by private health insurers, activity funded by other payers is excluded.
11
This percentage is an estimate made using HCP data provided by the Department of Health. The
denominator includes separations for which there was no MBS reported. Separations funded by DVA
and other non-private health insurance payers are excluded
13Table 1 Clinical Services and their reliance on PL categories slated for removal
Clinical Category and total PL Category Name13 % of total
separations (2019)12 separations where
these devices are
used
Ophthalmology (Eye and cataracts) Intraocular fluids 60.09%
237,861 separations Haemostatic devices 0.20%
Closure devices 1.06%
Chemotherapy Drug delivery devices 8.73%
237,638 separations Haemostatic devices 0.03%
Closure devices 0.49%
Arterial closure devices 0.03%
Diseases and disorders of the Drug delivery devices 3.58%
digestive system Enteral tubes 0.77%
69,473 separations Haemostatic devices 12.40%
Closure devices 52.63%
Dura defect repair 0.21%
Weight loss surgery Drug delivery devices 5.80%
21,586 separations Haemostatic devices 9.44%
Closure devices 88.25%
Dura defect repair 2.21%
Gynaecology Drug delivery devices 1.17%
93,336 separations Haemostatic devices 7.91%
Closure devices 15.79%
Dura defect repair 0.05%
Arterial closure devices 0.12%
Joint replacements Drug delivery devices 27.4%
65,061 separations Haemostatic devices 3.1%
Closure devices 52.6%
Dura defect repair 0.10%
Kidney and bladder Drug delivery devices 0.54%
63,134 separations Haemostatic devices 2.49%
Closure devices 4.93%
12
Sourced from HCP data provided by the Department of Health. Each separation was labelled with
reference to the principal MBS reported for that separation. Separations were then aggregated with
reference to the clinical categories defined in the Private Health Insurance (Complying Product) Rules
2015. Separations for which data was suppressed by the Department has been excluded from this table.
This table does not include separations for which no MBS items was provided, consequently the impact
on some services including chemotherapy and various medical interventions is under-reported.
13
The categories of device are those listed in the Department’s consultation paper at Attachment A as
being products slated for removal. This analysis includes only products slated for potential removal by
the Department as at August 2021.
14Clinical Category and total PL Category Name13 % of total
separations (2019)12 separations where
these devices are
used
Heart and vascular system Drug delivery devices 0.77%
124,639 separations Haemostatic devices 6.59%
Closure devices 12.34%
Dura defect repair 0.04%
Arterial closure devices 15.76%
Bone, joint and muscle Drug delivery devices 2.35%
76,445 separations Haemostatic devices 1.19%
Closure devices 12.52%
Dura defect repair 0.07%
Arterial closure devices 0.02%
An increasing number of patients being treated by the private hospital sector are high
risk. Technologies funded through the PL including the technologies identified for
potential removal have made it possible to treat patients who once would have had no
treatment options available to them, During the last decade, the age and complexity of
patients has been increasing. Data prior to the COVID-19 pandemic shows the
complexity of overnight patients in private hospitals has increased by nine percent14.
14
AIHW Admitted Patient Care, various years.
15If these technologies are not adequately funded, patients who can no longer be
treated in the private sector will be forced to rely on the already overcrowded private
sector. The private sector plays a central role in ensuring these patients have timely
access to care. The private hospital sector delivers around 60 percent of all surgical
services provided to Australian patients, but the impact goes beyond surgery. The
following table shows the contribution made by the private hospital sector to major
areas of clinical service enabled by the technologies the Department wants to remove
from the PL and the median wait time for these or similar services in the public
hospital sector.
Table 2: The private hospital sector's contribution to priority areas for which there is
a waiting time in the public sector
Private hospital sector contribution Median public sector wait time (elective)
(2018-2019)
Digestive system 63.5%1 Not reported
procedures Cholelithiasis 50%6
Chemotherapy More than 30%2 Not reported
Gynaecological 61%1 36 days3
procedures Excessive, frequent and irregular
menstruation 52% 6
Hernia and appendix 60% of inguinal hernia5 Inguinal hernio’phy 67 days
procedures
Musculoskeletal 60%1 Orthopaedic surgery 77 days3
system procedures Coxarthrosis71%6 Total hip 220 days4
Gonarthrosis 73%6 Total knee 223 days4
Lung and chest 22%1 Not reported
procedures
Ophthalmic 71%1 81 days3
procedures
Neurosurgery 74%1 36 days3
procedures
Ear, nose and throat 64%1 83 days3
procedures Chronic tonsils/adenoids 68% 6
Kidney and bladder 28%1 25 days3
procedures Calculus of kidney and ureter 54%6
1 AIHW. table 6.1 Number of interventions, by ACHI chapter, public and private hospitals 2018-19
2 APHA calculation based on internal data compared to AIHW data
3 AIHW. Table 6.30: Median waiting time (days) for admissions from public hospital elective surgery waiting lists, by surgical
specialty(a) and funding source, 2019–20
4
AIHW. Table 4.6: Waiting time statistics for admissions from public hospital elective surgery waiting lists, by intended surgical
procedure 2015-16 to 2019-20
5 AIHW. Table 4.6: Waiting time statistics for admissions from public hospital elective surgery waiting lists, by intended surgical
procedure 2015-16 to 2019-20
6 AIHW. Table 6.19: Separations for the 20 most common principal diagnoses in 3-character ICD-10-AM groupings for elective
admissions involving surgery, public and private hospitals, 2019–20
Small and regional hospitals will be particularly vulnerable as a result of this reform.
Hospitals where specific specialties may be represented by only one or two clinicians,
16may have to cease providing particular services altogether if the techniques used by
these clinicians are no longer affordable. Australian Institute of Health and Welfare
(AIHW) data shows 30 percent of private overnight hospitals and twelve percent of day
hospitals are in regional areas15.
Private hospitals play an essential role in providing people in regional areas with access
to timely care. Table 3 shows the extent to which people living in regional remote
areas rely on the private hospital sector for access to timely care.
Table 3: Private hospitals and day hospitals - services to people in regional/remote
areas16
Broad categories of Separations provided in the Percentage of total
service private hospital sector to people separations provided to
living in regional/remote areas people living in
regional/remote areas
Surgical
Emergency 10,212 9.7%
Non-emergency 409,501 59.1%
Medical
Emergency 32,934 4.2%
Non-emergency 285,376 27.1%
Other acute care
Emergency 3,969 13.5%
Non-emergency 218,899 58.8%
Childbirth 12,272 14.4%
Total acute care
(excluding mental health) 973,163 31.1%
Total 2015-16 1,060,104 32.1%
Total 2018-19 1,119,262 31.5%
The Government’s confidence that items removed from the PL will be funded by
alternative (i.e. contractual mechanisms) without impact on the range of
technologies provided to doctors, the range of services provided, access to services
and patient out of pocket costs, is misplaced.
• Private Healthcare Australia (PHA) cannot make commercial commitments
binding on its members.17 Indeed, some insurers have indicated they have no
intention of changing contractual arrangements to provide alternative funding
for any item removed from the PL as a result of these reforms.
15
AIHW, Private Hospitals 2012-13 (this is the most recent data available)
16
AIHW, Private health insurance use in Australian hospitals, 2006-7 to 2015-16
17 PHA, Paying for consumable items that are coming off the Prostheses List in February 2022, Revised
version August 2021
17• PHA has already signalled expectations of significant savings well beyond those
expected from public refence pricing even before negotiation of contractual
solutions have begun, let alone settled18.
• Several funds have long refused to acknowledge that removal of items from the PL
should be fully compensated by adjustment of other mechanisms on the insistence
that these costs are already accounted for and cheaper non-PL alternatives should
be used19.
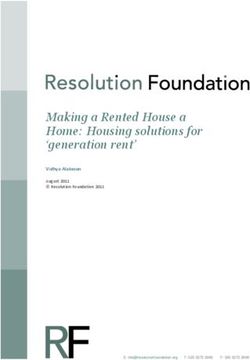
• As shown in Figure 1 the private hospital sector is fragmented in comparison to
private health insurers and other payers who use their market power unfairly and
to the detriment of private hospitals. Small payers negotiate through alliances that
multiply their market power and individual funds (including some very small funds)
exercise overwhelming power over providers in particular regions.
• In discussions with APHA, the Department has conceded that health insurers are
unlikely to enter into commercial arrangements with all hospitals for items
removed from the PL. Hospitals ignored by insurers in this regard will have no
option other than to pass costs onto the consumer for items no longer covered.
Figure 1: Estimated share of separations involving the use of prostheses20
Little Company of
Cabrini Mary
Day Hospitals Mater
Epworth
Healthe
St Vincent's
Other overnight
Ramsay Health Care
Unitingcare
St John of God
Healthscope
18 PHA Ibid.
19
EY Consulting, July 2020
20
APHA, internal data
18Table 4 shows the concentrated power of the private health insurers. Small funds
enhance their market power by negotiating through the Australian Health Service
Alliance (AHSA) and the Australian Regional Health Group (ARHG). It should also be
noted that, because of membership profiles, some funds have a far greater degree of
market power over hospitals in particular locations.
Table 4: Private health insurance percent of hospital benefits paid 2019/20 by
state/territory
NSW VIC QLD WA SA TAS ACT NT
Medibank 20.4% 30.3% 29.2% 20.8% 17.7% 24.9% 25.9% 39.3%
BUPA 23.5% 24.8% 33.0% 10.8% 48.9% 32.5% 19.5% 38.0%
NIB 13.2% 6.8% 5.2% 3.0% 3.6% 2.5% 12.7% 1.8%
AHSA 19.2% 24.5% 22.8% 9.1% 19.4% 10.5% 20.5% 12.9%
HCF 22.2% 8.3% 8.9% 5.0% 9.6% 5.5% 20.4% 4.7%
ARHG 0.6% 4.3% 0.3% 0.0% 0.3% 23.4% 0.3% 2.9%
HBF 0.8% 1.1% 0.7% 51.3% 0.5% 0.8% 0.8% 1.1%
Source: Analysis based on Private Health Insurance Ombudsman (PHIO) State of the Health Funds
Report 2019
Table 5 shows the extent to which insurers use their market power by refusing to
contract with a significant number of hospitals and day hospitals.
Table 5: The proportion of private hospitals and day hospitals without contracts with
major health insurers.
Insurer Market share Estimated proportion of Estimated proportion of
private day hospitals not private overnight
contracted with hospitals not contracted
with
Medibank 26.9% 35% 14%
BUPA 25.8% 32% 11%
HCF 11.1% 38% 18%
NIB 8.6% 18% 9%
HBF 7.5% 26% 7%
NB: HCF and HBF have slightly higher rates of contracting coverage in states where they have the
greatest proportion of their members.
Source: Analysis based on PHIO State of the Health Funds Report 2019
19Relations with private health insurers are already strained.
• Protracted negotiations and failure of the NPBC to reach agreement on issues
arising from the MBS Review21.
• Protracted negotiations and delays in resolving contractual changes as a result of
changes to the MBS – negotiations are understood to still be in train relating to
MBS changes effective Thursday 1 July 2021 resulting in financial risk and
withholding of payments for treatments since that date; notwithstanding health
insurers were advised of these changes in January 2021. Negotiations related to
changes made in previous years have in some instances remained unsettled for 12
months22.
• This experience, together with the concerns already cited above, indicate the risk
of extended and more common disputation is high, as it the risk that contracts will
be terminated or not renewed.
• Of course, unlike MBS items, against which insurers are obliged to pay a benefit,
once an item is removed from the PL insurers have no such obligation and
therefore little incentive to negotiate.
The presumption that contractual funding mechanisms that exist in overseas
jurisdictions can be applied within the Australian context is flawed because it fails to
recognise particular characteristics of the Australian healthcare sector.
• Australian private hospital neither employ nor contract doctors. Consequently,
hospitals have diminished power to influence doctor choices with regard to
selection of technologies and case mix.
• The Government has failed to realise the challenges associated with Australia’s
specific circumstances, i.e. the need for the PL as a funding mechanism which
supports clinician choice, apply equally to the changes proposed as they would to
‘big ticket’ PL items. Key differences between Australia and major international
comparators are summarised in Table 6.
• Clinical independence including ensuring the right prosthesis for the right patient is
a fundamental part of the Australian healthcare system. Removing such
independence is akin to United States-style managed care.
21
In June 2021, the NPBC agreed that it would not be able to make a recommendation concerning the
banding for several new MBS items for PCI effective from 1 July 2021 and that this fact should be
communicated to stakeholders.
22
In November 2019, changes were made to MBS items for colonoscopy. Revised payments
arrangements for these items remained unresolved twelve months after the date of effect.
20Table 6 International Comparisons23
Country Funding models Prostheses price Doctor remuneration
setting
Australia Various models + PL Government set the Fee-for-service paid by
benefits for a defined list benefit of PL items insurers/consumers
of medical technologies sending a signal to
the sector as a
whole, but hospitals
conduct their own
purchasing
France DRG+ expensive devices+ Government sets Contracted /employed by
physician fees the price the hospital
England DRG Government tenders Salaried
(NHS)
New Zealand Bundled case payments Hospitals conduct A mix of models.
for each procedure their own Increasingly paid under
including the cost of purchasing structured contracts by
medical devices used. hospitals
Germany DRG based Hospitals conduct Mainly employed/salaried,
their own some fee-for-service
purchasing
Sweden Global budget and DRG Government tenders All salaried
payments and hospitals
USA Various models Fund Salaried, paid by
holders/hospitals fundholder/ hospital
conduct their own
purchasing
Data in Table 1 on page 14 and charts in Appendix D: The Department of Health’s
proposed changes to the Prostheses List, show the devices slated for removal are used
selectively. For some MBS items their use is common, but for most it is infrequent.
These results highlight the role of clinician choice in using these technologies to meet
the needs of specific patients and to enable specific procedures. The procedures in
which they are frequently used are often procedures for which a contemporary
standard of care would be impossible without access to the specific technologies
deployed.
Even though the Department has acknowledged that a reform of this magnitude
cannot be made ‘overnight’, they have failed to appreciate the complexity of task.
• The complexity of the task that would confront the NPBC was explained at length
in APHA’s February 2021 submission, and is further evidenced by data showing the
23
Commonwealth Fund, International Health Care System Profiles England, France, New Zealand,
Germany, Sweden and the United States of America.,
https://www.commonwealthfund.org/international-health-policy-center/system-profiles
21breadth of services implicated and the complex and, in some cases, unknown
implications for service costs.
• The complexity of the task involved in updating cost studies.
• The complexity of the task involved in negotiating bundled funding arrangements.
• The added complexity posed by the difficulty in modelling the impact of this
change across so many services, while also taking into account changes to the MBS
and DRG versions and the multiple DRG versions in use within the sector.
• The timing of these proposed reforms which are concurrent with:
• ongoing reforms to the MBS
• discontinuity in data arising from the pandemic and ongoing uncertainty in
projecting service levels
• other overlapping changes to the PL that entail renegotiation of contractual
arrangements with all suppliers and management of risk across all PL use and
expenditure.
• Reliance on individual contractual arrangements would mean that hospitals will
need to work with multiple payers. Each payer will have their own model. This will
impose additional complexity over and above current PL arrangements.
• Even where delays are granted, these challenges are daunting for the largest
operators and impossible for smaller operators which, if they are offered contracts
at all, receive contracts on a ‘take it or leave it basis’.
• The delay necessary to address all of these issues would be unacceptable in light of
the pressing nature of the problems to be solved. Therefore, an alternative
solution must be found.
Data in Table 1 on page 14 and charts in Appendix D: The Department of Health’s
proposed changes to the Prostheses List show the devices slated for removal are used
across a wide range of services. Devices are used in complex combinations depending
on the preferences of individual clinicians and patient need. These combinations can
further impact other costs associated with the episode of care, including length of stay,
requirement for additional interventions or technologies, readmission versus
ambulatory care. The implications of these reforms for service viability go well beyond
the cost of the technologies themselves. If hospital cannot negotiate contracts with
both health insurers and manufacturers such that these devices remain affordable,
they will need to reconsider the services and models of care they are able to provide to
patients.
Although the total financial impact of these reforms is small as a percentage of the
total benefits outlaid for hospital care by private health insurers. Differences in cost at
a separation level (see table Table 7: Costs at separation level for selected clinical areas
and Appendix D: The Department of Health’s proposed changes to the Prostheses List)
mean the risks associated with negotiating contractual arrangements will vary
significantly between hospitals depending on their service mix, preferences, and
practices of the clinicians with whom they work and the patient population they serve.
22Table 7 shows how the costs of particular technologies can vary for a single separation.
It should be noted however that this table does not indicate the combined impact of
these changes on hospital costs.
Table 7: Costs at separation level for selected clinical areas
Clinical Areas and total PL Category Name25 Indicative cost range at separation level
separations (2019)24 (lowest 10th percentile and highest 90th
percentile across all MBS within the
clinical area)
Ophthalmology (Eye Intraocular fluids $10 $240
and cataracts) Haemostatic devices $10 $950
237,861 separations Closure devices $10 $350
Chemotherapy Drug delivery devices $10 $4,700
237,638 separations Haemostatic devices $10 $2,300
Closure devices $10 $2,700
Arterial closure devices $10 $960
Diseases and disorders Drug delivery devices $10 $1,100
of the digestive system Enteral tubes $90 $480
69,473 separations Haemostatic devices $10 $3,700
Closure devices $10 $5,900
Dura defect repair $790 $790
Weight loss surgery Drug delivery devices $10 $690
21,586 separations Haemostatic devices $30 $2,900
Closure devices $20 $4,600
Dura defect repair $790 $2,400
Gynaecology Drug delivery devices $10 $860
93,336 separations Haemostatic devices $10 $3,100
Closure devices $10 $2,500
Dura defect repair $750 $750
Arterial closure devices $370 $370
Joint replacements Drug delivery devices $10 $1,000
65,061 separations Haemostatic devices $10 $1,900
Closure devices $10 $1,700
Dura defect repair $790 $1,600
Kidney and bladder Drug delivery devices $10 $520
63,134 separations Haemostatic devices $10 $1,900
Closure devices $10 $3,500
24
Sourced from HCP data provided by the Department of Health. This analysis excludes episodes for
which no principal MBS was reported.
25
The categories of device are those listed in the Department’s Consultation Paper at Attachment A as
being products slated for removal..
23Clinical Areas and total PL Category Name25 Indicative cost range at separation level
separations (2019)24 (lowest 10th percentile and highest 90th
percentile across all MBS within the
clinical area)
Heart and Vascular Drug delivery devices $10 $570
system Haemostatic devices $10 $2,400
124,639 separations Closure devices $10 $3,700
Dura defect repair $750 $1,700
Arterial closure devices $370 $2,200
Bone, joint and muscle Drug delivery devices $10 $2,200
76,445 separations Haemostatic devices $10 $4,700
Closure devices $10 $3,200
Dura defect repair $790 $790
Arterial closure devices $370 $790
Removal of items from the PL is not an acceptable remedy because it is not assured
of achieving the intended aim.
• Even where the potential for price competition between manufacturers exists, this
is constrained by market size within Australia and the strength of dominant
providers relative to private hospitals.
• The power of private hospitals is weak relative to manufacturers and there is no
assurance they will be able to obtain the savings expected by private health
insurers. This is an additional risk that the reforms foist on private hospital
operators.
• The response of manufacturers may be unpredictable, some may withdraw
products, some may increase prices (no longer constrained by the discipline of the
PL) and expected benefits of price competition may not be realised or may be less
than would have been recognised by retention of these items on the PL combined
with the application of public sector reference pricing.
While PHA has promoted the expectation of substantial savings through increased
price competition. These expectations vary between the categories of device. PHA’s
expectations are also unrealistically 'aspirational’ in the expectation that private
hospital operators might achieve prices comparable with overseas markets; prices far
lower than achieved by public hospital operators in Australia26.
The proposed reform carries the risk of consequences for the health sector as a
whole.
26
PHA Ibid.
24You can also read