Precautions for Hunters and Hunting Dogs
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Precautions for Hunters and Hunting Dogs The American Veterinary Medical Association http://www.avma.org/ has compiled a document which discusses many diseases affecting hunters and their dogs. A number of tick-borne disease are included such as Lyme, anaplasmosis, ehrlichiosis, babesiosis, RMSF, Q fever, tularemia link to PDF Precautions for Hunters and Hunting Dogs The American Veterinary Medical Association http://www.avma.org/ has compiled a document which discusses many diseases affecting hunters and their dogs. A number of tick-borne disease are included such as Lyme, anaplasmosis, ehrlichiosis, babesiosis, RMSF, Q fever, tularemia link to PDF
2010 NJ Lyme Case Numbers by
County
New Jersey was rated second in total reported CDC cases in
2010. Here is a table of the county wide distribution.
Total includes confirmed and probable numbers reported by State to CDC
annually
Rate = confirmed and probable/100,000 population (2010 census figures)
Number in parenthesis after county is rank in State by case numbers.
2010 ConfirmedProbableTotal Rate Suspect
Atlantic 95 29 124 45.2 86
Bergen
148 18 166 18.3 102
(10)
Burlington
221 25 246 54.8 69
(6)
Camden 9 0 9 1.8 122
Cape May 27 0 27 27.8 23
Cumberland 86 11 97 61.8 34
Essex 134 12 146 18.6 69
Gloucester 112 0 112 38.9 95
Hudson 35 5 40 6.3 37
Hunterdon
323 0 323 251.7 259
(4)
Mercer 145 13 158 43.1 102
Middlesex 123 11 134 16.5 172
Monmouth
328 9 337 53.5 369
(3)
Morris (1) 426 53 479 97.3 366
Ocean (5) 192 57 249 43.2 137Passaic
156 21 177 35.3 90
(9)
Salem 25 5 30 45.4 32
Somerset
180 24 204 63.1 193
(7)
Sussex (2) 312 87 399 267.3 295
Union 58 9 67 12.5 77
Warren (8) 185 3 188 173.0 166
Unknown 0 0 0 NA 0
Statewide 3320 392 3712 42.2 2895
Click here for printable pdf of NJ Lyme Disease Case Numbers by CountyTick-Borne Disease In Children And Adolescents A Medical Illness/ A Multidisciplinary “Cure” We in the Lyme world all know that tick-borne diseases are caused by complex organisms that can affect just about any part of the body, and we realize that the key to getting well is finding a Lyme- literate doctor, obtaining an accurate diagnosis, and comprehensive, efficacious treatment. While treating the medical aspect of the disease is paramount, for children and adolescents with chronic Lyme disease, medical treatment alone is often not enough. Many of these children have Lyme related psychiatric symptoms or educational impairments. Their serious symptoms, combined with the duration of the illness often leads to gaps in their
development. Their isolation can leave them lonely, and inhibit their ability to interact with peers. These issues are best addressed through the coordinated efforts of a team. Children and adolescents with chronic Lyme, often meet the DSM criteria for one or more “mental illnesses”–anxiety disorder, depression, anorexia nervosa, AD/HD, as well as disorders in which behavioral problems manifest–oppositional defiant disorder, conduct disorder, and for some, psychosis. Even though the “mental illness” may be due completely to Lyme, the serious psychiatric symptoms cannot be ignored. For many, psychiatric medications are essential, in managing the symptoms during treatment, including the complex issues of managing symptom flares (Jarisch Herxheimer reactions), brought on by the antibiotics. Thus there is a need for involvement of Lyme-literate psychiatrists who treat children. These “mental illnesses” carry a constellation of issues. The anorectic children, for example, often have an aversion to certain foods, or a rigid pattern of eating, and there is an obsessional quality to their thinking, about food and exercise. Some put a pathological spin on suggestions doctors make for a “yeast free” diet while on antibiotics, some refuse to take any medications by mouth. Weight gain typical of some Lyme patients terrifies the anorectic, and pathological weight loss brings them comfort. These issues need to be dealt with in individual and family therapy, to keep the anorectic child safe and healthy during the acute phases of the illness and Lyme treatment. Anxiety is another symptom common to children with Lyme. The anxiety presents for many in their fears about school failure, even as their cognitively impaired brains struggle to succeed. It takes a Lyme-literate team to deal with the anxious child with Lyme–the medical doctor who treats the illness, the psychiatrist who prescribes the medication for anxiety, the psychotherapist who teaches the child and family strategies for dealing with the anxiety, helps the child learn to think
in a different way (cognitively-based therapy is helpful here), and the Lyme-literate school team who provides support and accommodations for the child who has impairments that affect learning. The school nurse or guidance counselor can provide a brief respite, and support, for the anxious child, in the middle of the chaos of the school day. Behavioral problems are often due simply to the infection in the brain, and will resolve as the illness is treated comprehensively. However, the treatment could take a long time, and the behaviors need to be addressed and managed during these difficult times. Intervention and support of a Lyme-literate psychiatrist and psychotherapist, as well as involvement of a parent advocate who develops a plan for managing behaviors in the school setting can make a significant difference in the life of the child and the family. Traditional “behavior plans” are often not effective, when the behavior is driven by an infectious cause. Attention needs to be paid to the tasks of the various developmental stages the child with chronic Lyme is going through. The most difficult stage to manage is adolescence, where the Lyme patient may deny the illness and resist treatment to be “normal”, in an attempt to individuate. At this stage, some will self-medicate the Lyme symptoms with street drugs. If the child has been ill for a long time, it may be difficult to distinguish between symptoms of the illness and who the child really is. It is helpful if these symptoms are addressed in therapy, as well. Part of the work of childhood is to develop social skills, to learn how to interact with others. Children learn that at home, in their communities, in school, on the ball field. When a child is ill with chronic Lyme, often her exposure to others is very limited. Some children have been on homebound instruction for months and years, not even having the school community to interact with. Socialization needs can be addressed in therapy, and for those who are seriously ill,
some social experiences can be built into their week. CONCLUSION AND RECOMMENDATIONS While physicians who treat Lyme are focused on diagnosing and treating the medical illness, it is also important to recognize that there is more to treating the child with Lyme than ridding the body of infection. We need an integrated approach that includes doctors, nurses, psychiatrists, psychotherapists, neuropsychologists, educators, and advocates. It is important that we are aware of each other’s roles, and communicate regularly. The impact of Lyme disease on children and adolescents is not just a medical issue. By working together to support and treat the whole child, we can help our children achieve more than physical health. They can become resilient, life-loving, successful people, and put the nightmare of the Lyme years behind them. Click here for printable pdf of article. Published In Lyme Times Children’s Treatment Issue #42 – Summer, 2005 Sandy Berenbaum, LCSW, BCD Family Connections Center for Counseling Offices in Brewster, NY and Southbury, CT www.lymefamilies.com Ph: (203) 240-7787 Fax: (203) 405-6200
© 2005 Reflections On Lyme Disease In The Family Ideally, the family is a safe, protective, nurturing unit in which a child develops and grows. The early years are demanding for parents, who, in addition to bonding with their child, must make daily decisions that are vital to their child’s life and growth. In contrast, the adolescent years are emotionally challenging, as parents struggle to remain connected, supporting their children’s bid for independence, while protecting them from making sometimes disastrous choices, as the child struggles to develop her own ideas and direction. Let’s add Lyme disease to this picture. Parents of children with Lyme disease carry an enormous burden, far greater than those outside the Lyme community are likely to understand. They worry about accuracy of diagnosis, selecting the right doctor and treatment approach, paying for treatment that is very costly, and the complexities of identifying and advocating for educational supports that may be necessary for a child to make it through school. Other members of the family may be ill as well, often the case with Lyme disease. Aside from the increased financial burden, there is the stress of trying to meet the needs of several Lyme disease patients in one family. It is particularly
difficult when one of those Lyme patients is a parent, and when the ill parent suffers from neuropsychiatric problems! Given the complexity and unpredictability of symptoms, and the inadequate understanding of this illness in the greater community, parents often find that they do not have the support of family and friends, as they struggle to cope. Unwittingly, some well-meaning family members may make comments that undermine parents, even challenging the medical decisions that they make. At times, family members mistakenly attribute the child’s symptoms and behaviors to willfulness on the part of the child, or inadequate structure and limits on the part of the parents. Failing to appreciate the complex, debilitating nature of this illness, they do not acknowledge the struggle the family is going through, and are therefore not a reliable source of support. This reality in the life of the family of a child with Lyme can be particularly disappointing and painful! Behavioral problems are not uncommon in children with chronic Lyme. If the child is subject to rages or other severe psychiatric symptoms, this increases the stress level in the family, and makes the family’s day to day life far more complex. Lacking the support and help they would have hoped to get from their family and friends, parents truly feel isolated. They are often out on a limb with their child, but they are also out there alone. Where a young child is concerned, although his parents do their best to help him feel safe and protected, hiding their worries and fears, the child surely senses that something is very wrong. Parents can’t help but worry about whether their child will ever fully recover. What might the residual damage be…to his body, to his brain, to his experience of life? On some level, the young child is keenly aware that he is not growing up in the carefree environment that peers may be experiencing. Worries certainly permeate the household. Even deciding whether to allow a child to go on a school field
trip, or give permission for a teenager to go hiking with friends may be a struggle for parents, who worry that their child, already very ill, might be re-infected. A sense of normalcy is lost. Where the adolescent is concerned, a primary issue is how to support the teenager in her efforts to individuate and move toward independence, while taking appropriate precautions for treating the illness. The physical and emotional dependency of a sick teenager may delay or interfere with the task of individuating. Or, the teenager, supported by inaccurate information that is all around them, may separate by challenging the Lyme diagnosis or treatment, and refusing to go to the doctors or take prescribed medications. In denying their illness, teenagers may even come to believe that their symptoms represent who they are, as they lose touch with the fact that these symptoms are caused by a treatable medical illness. They may therefore see themselves as lazy, not very bright, quick to anger, moody. And, in the process of individuating, they might not believe the evidence their parents and doctors present that these are merely symptoms of the illnes, and not a manifestation of who they really are. How terrifying this is can be for parents! A child’s illness may call on parents to grow in unaccustomed ways. Parents may find themselves thrust into situations beyond their own comfort level, needing to be more assertive with previously trusted school and medical authority figures or more conciliatory with insurers and others, in order to acheive important goals. The needs of their children often push parents far beyond their comfort zone in these areas. It is important that parents recognize where that comfort zone is, and work to move beyond it, for the sake of their child, and his recovery. In this complex, demanding world, we need to have compassion, empathy, and understanding for those who are struggling to
raise children who have chronic Lyme disease. If we can appreciate the challenges that face them, and respect their decisions, perhaps we can make their world a little bit brighter. Parenting Strategies from the Trenches After years of helping parents, children, adolescents and families deal with some of these issues, I have developed the following strategies, to help parents ease their journey: • Maintain a problem-focused approach as you make decisions about diagnosis, doctors, and treatment. • Work at developing a consensus between you and your child’s other parent, whether or not you are still together! • Stay focused on current problems to be solved, and keep worries on the back burner. • Explain what’s going on to your child in concrete, age- appropriate terms. • Maintain your credibility with your child by being truthful. • Be careful with the words you use. Avoid words like "psychotic episode", "manic", or "incurable". Lyme disease is a scary illness. Keep your words from making it scarier. • Be firm when you need to be, but give choices when you can, lots of choices. • Establish and maintain protective boundaries, protecting yourself and your child from family members and friends who doubt your judgment and parenting decisions. Let others know what they can and cannot say. • Build a supportive network – educate your family and friends about Lyme, but don’t overload them. Remember, this is your issue, not theirs.
• Be open to support, but make it clear that you’re not open to being second-guessed. Allow people to help in concrete ways when you’re overwhelmed. Let them make meals, pick up the kids, or shop for groceries.. • Psychotherapy or family therapy, with a Lyme-knowledgeable therapist, can be an important adjunctive treatment, to help you and your children get through the hard times without residual damage. The model I use is helping Lyme patients and their families go from being victims, to survivors, to thrivers. There’s nowhere that this model is needed more than with families coping with Lyme disease. Click here for printable pdf of article. Published in Lyme Times Children’s Treatment Issue #42 – Summer, 2005 Sandy Berenbaum, LCSW, BCD Family Connections Center for Counseling Offices in Brewster, NY and Southbury, CT www.lymefamilies.com Ph: (203) 240-7787 Fax: (203) 405-6200 © 2005
Berenbaum-Canon Lyme Disease
Screening Protocol
1. History of changes in:
behavior at home, school, or in other settings
school performance or attendance
sleeping and eating patterns
socialization patterns, or dramatic change in peer group
mood
o depression
o anxiety
o temper flare-ups
o suicidal ideation or gestures
o intensification of PMS
2. History of changes in activity level, that could be suggestive
of Lyme disease
Sudden loss of interest, or inability to participate in activities,
such as organized sports, music, dance, drama, youth group, etc.
3. A discreet point in time at which problems began
4. History of onset of other psychiatric symptoms (panic attacks,
hallucinations, attentional problems not present in early
childhood)
5. History of use of psychiatric medications, with either no
success in symptom reduction or a paradoxical response
6. History of any physical illness (flu, mononucleosis, bronchitis)occurring prior to start of psychiatric, learning or behavioral
problems
7. History of short term antibiotic treatment for medical problem
(strep infection, etc.) with temporary improvement of symptoms
Click here for printable pdf
Sandy Berenbaum, LCSW, BCD Family Connections Center for
Counseling
Offices in Brewster, NY and Southbury, CT www.lymefamilies.com
Ph: (203) 240-7787 Fax: (203) 405-6200
© 2002Kids And Lyme Disease – How It Affects Their Learning Introduction: There is an urgent need for Lyme disease education and awareness in the schools throughout the United States. In addition to the "ABC’s of Lyme," and the new "Time for Lyme" video, Lyme professionals – physicians, psychotherapists, neuropsychologists, need to be seeking opportunities to provide in-service training to schools, so that teachers and other school professionals understand and appreciate the difficulties that face kids with Lyme every day. We need to call on the schools to help these children, and education is the key. The following is a presentation I gave to the Northern Dutchess County (NY) Support Group in November 2002. Perhaps it will provide ideas for other presentations to Lyme groups and schools around the country. Every child with Lyme disease should feel understood and supported, and be successful in school. Lyme disease may be a handicap that some children have, but it should not be an insurmountable obstacle. Click here for printable pdf When my colleague, Lynne Canon, and I started our private practice 16 years ago, we did so with a commitment to providing psychotherapy and family therapy to adolescents and their parents. For five years, we did just that, with no thought that a medical illness might be at the root of the psychiatric, behavioral or learning problems some of these kids might have. Then, in 1991, a client was referred to us who had a profound effect on us, and on our practice. I will call him "Jim". Jim was a 15 year old boy who refused to go to school. He was paranoid, fearing that people were out to get him as well as
his family, and he could not sleep at all. His parents reported that he had been an honors student up to a few months prior to our first session, but now, when he did go to school, he failed every test he took. He appeared to be physically fit and well disciplined. He was even skilled in the martial arts. On Intake, we asked standard history and family history questions. We found Jim to be a very verbal and engaging young man, obviously bright, and a deep thinker. We saw agitation, restlessness, and anxiety, as well as the paranoia reported by his parents. Toward the end of our initial interview, we asked about his hobbies. With great enthusiasm, Jim told us about his volunteer work at an environmental center here in Dutchess County, and of his hopes for a career involving environmental studies. Jim was a real puzzle to us. We were faced with a set of symptoms and functional problems that made no sense, even in examining his history. Realizing that there had been a dramatic onset of symptoms at a particular point in time, and that Jim had spent so much time out of doors in what we now see as the Lyme capital of the universe, we referred him to his family doctor for a Lyme assessment. His pediatrician took a titer, which came back "negative", (any of you parents have that experience?) indicating to this doctor that Lyme was not a factor! That road appearing closed, we continued to see Jim, as well as his parents, and watched a steady decline in Jim’s functioning. He could not go to school, and was placed on home teaching. His parents and we were completely baffled. 2As Jim’s symptoms got worse, we thought he might have to go into a psychiatric hospital. In a last quest for a possible medical answer, we suggested that his parents take him for a consultation to a pediatrician who we knew to be Lyme-
knowledgable. On the day that consulting doctor saw Jim, he called to tell us that he had made a CLINICAL DIAGNOSIS of Lyme disease, a diagnosis based on Jim’s clinical symptoms, NOT on a blood test. The doctor prescribed Ceftin, a drug that crosses the blood brain barrier, attacking spirochetes that were in the brain. Within three days, Jim’s paranoia disappeared. He admitted to having had hallucinations, and they too were gone. He was now sleeping 14 or more hours a day, and for the first time, had joint pain, as part of a Jarisch Herxheimer reaction to the antibiotics, a reaction in which the symptoms temporarily get worse. Thus began Jim’s long struggle with what turned out to be chronic Lyme disease. Jim went from being a teenager who could not attend school, could not participate at all in the educational process, was failing all tests, to a good student at one of the best colleges in the New York State system. He went from being a very sick kid, who was on homebound instruction for a year and a half, to a college graduate. He was helped by a supportive family, a Lyme-literate doctor, who treated him effectively, a school administrator who accepted the fact that he was, indeed, ill, and a school system that provided accommodations, to help him succeed. ————————————— Most of you know that Lyme disease is a multi-system illness. Someone with Lyme can have joint pains, heart problems, stomach problems, any kind of physical manifestation. I’d like to focus this evening on the neurological and neuropsychiatric problems, the ones that have the greatest effect on learning, and the ones that lead to the greatest misunderstandings between parents and school professionals. Most common with children and adolescents who have chronic
Lyme are intense headaches that can last for days, cognitive, attentional and mood problems, profound fatigue, and difficulty sleeping. Many kids have problems with vision, or visual and auditory overstimulation. Some have a sensitivity to flourescent lighting. Some of these symptoms may be very subtle, so it is difficult for the teachers to realize that they are dealing with a sick child, rather than a child who is daydreaming, or simply trying to avoid his school work. Once a child has been diagnosed, and is undergoing treatment, there are problems produced by the treatment itself. High doses of antibiotics and other medications the child may be taking can produce gastointestinal problems. The child may be uncomfortable, and complaining a lot, particularly of stomach aches. Since young children sometimes complain of stomach aches to avoid academic projects (I remember my stomach hurting in 3rd grade every time I had to speak 3 in front of the class), it’s hard for teachers to discern whether the problem is avoidant behavior, or the result of illness. Another problem, of course, is the flare of the symptoms when the Lyme spirochetes are being killed off by the antibiotics. A teacher who doesn’t know much about Lyme disease has a difficult time realizing that with this illness, once the medication is started, the child will periodically feel worse, and have more, rather than fewer, symptoms. My sister-in-law used to say to me, during my Lyme treatment, when I told her how bad I felt – "Oh, that’s right – worse is better", but that’s a hard concept for people who are not personally affected by Lyme to grasp. Other problems include the frequent need for medications (sometimes at school), the fatigue caused by the illness
itself, or as a result of the lack of sleep, the demand on the child’s time for long car trips to doctors who are Lyme specialists (some kids are even travelling to New Haven, CT, a 4 hour round trip). Another big problem can be that these very sick kids don’t look sick. The extent of the child’s illness is not reflected in what the teacher sees. —————————————- Another, and very important, way to look at kids with chronic Lyme is to look past their symptoms at their functional impairments. It’s the functional impairments that give us the language necessary to figure out what these kids need in school. If you have a medical problem, you ask yourself and your doctor two questions: 1. What do I need to do to get better, to get well? (This question addresses how to get your health back completely, or as completely as possible) 2. What do I need to do in the meantime, to compensate for my current functional impairments? (This addresses what in school jargon amounts to "accommodations", enabling you to function on the best level you can, hopefully the need will only be short term.) You break your leg. Before you broke your leg, you were able to walk, to drive, to go up and down stairs. You go to the doctor. He develops a treatment plan – puts a cast on your broken leg, tells you what not to do while it’s healing. You get rides to work, maybe use a wheelchair at home, someone else in the house does the laundry, if the washer and dryer are on a different level. You have a long term plan and a short term plan. The long term plan is to get permanently
better. The short term plan is for "accommodations." If a child breaks her leg, the same process is put into place — the doctor establishes the long term plan, by "treating" the broken leg. A note from the doctor, gives the child "accommodations" in 4 school as part of the short term plan, giving her an elevator pass, having someone carry her books, compensating for her "functional impairments." What’s different about Lyme? First, if Lyme is chronic, you probably don’t know when you got sick. Your symptoms crept up on you, until you finally found a doctor who put the puzzle pieces together, diagnosed you, and began treatment. (You know when you broke your leg!) When you got the Lyme diagnosis, a light bulb probably went off in your head. You remember when you were well. You had years of life experience of health, physical and mental. You know what your brain was like before your first symptom. You want to get back to that point, and that is your goal, restoring health and restoring functioning. For a child, here is the profound complication – she had little or no life experience before Lyme. One of my clients is in 5th grade. Her doctor speculates that she’s had Lyme since the age of 4. What do she and her parents know about her cognitive abilities, her attentional abilities, before Lyme touched her life? This is the problem for so many kids. They have no baseline. Having no memory of a tick bite or a rash, they really don’t know when normalcy ended, and Lyme began. Or, even if they do remember, they were so young when they got bitten that there was no evidence of their ability to do schoolwork and to
concentrate before the illness began. It’s not clear to them how competent they would have been had they not gotten Lyme disease. It’s a very puzzling picture for these children, and hard for them to be self-confident, in the face of this illness. ————————————— Now, let’s look at some of the FUNCTIONAL IMPAIRMENTS in children and adolescents who have chronic Lyme disease? One can see functional impairments at home, in school, and among the peer group. The child’s physical problems, unpredictability of symptoms, and feelings of helplessness can lead, IN SOME KIDS, to a self-focused view of life, understandable given what these kids are trying to cope with. I’d like to show you a slide that I used in a presentation at a Lyme Disease Association medical conference. It highlights what some of the functional impairments are, and points to how the school can help. In this chart (See Slide #1) I give an example of some of the common impairments we see: • Fatigue • Problems Sleeping • Lethargy • Attentional problems, such as distractibility, impulsivity, problems focusing 5 • Depression or anxiety, including obsessional thinking or racing thoughts, "brain never stopping" (thinking constantly) • Problems with eating (due to gastrointestinal symptoms, either from the Lyme itself, or secondary to the antibiotics.) • Behavioral problems, severe at times • In adolescent girls, by the way, PMS symtoms can be QUITE severe, as well.
Let’s look at some of what the functional impairments might LEAD TO. We can see the process here. The functional impairments that are the original problems produced by Lyme (and when I say Lyme, I include, of course, the co-infections) result in further problems for the child. (see the second column) • Poor school attendance • Chronic lateness • Incomplete assignments and tests • Behavioral problems at school • Withdrawal from peers (particularly when peers fail to understand how sick the Lyme patient is) • Situation-induced mood problems (aside from the mood problems coming from the infection itself) • Weight gain or loss, at times, dramatic • Mood swings, inappropriate verbal outbursts, increasing conflicts in all settings (In general, kids and adolescents do not have a high degree of frustration tolerance. We all know that. Lyme disease severely challenges the child’s already-limited resources) What, then, might the child do to COMPENSATE for what is going on? (these are what I call the "self-selected solutions") All that I have discussed so far is distressful for the child. She may try to cope with all of this by doing any of the following: • As school performance falls, and they’re less involved with activities, Lyme patients might shift to a lower-functioning peer group, cut classes, and, in the extreme, they might drop out of school (if over 16), to avoid the frustration of
dealing with academic demands • For the kids with GI problems, they might severely limit their food intake, or begin gorging and purging 6 • Self-Medicate • For energy, or to self-treat the attentional problems, they might use stimulants or cocaine • To calm them down, or to keep them from thinking about all that is going on, alcohol, marijuana or other drugs might be chosen I have seen all of the above in adolescents with chronic Lyme in my practice. Any of the functional impairments can lead to any of the results, and to any or all of the self- selected solutions. Functional impairments in school are often very significant, and call on the educators to develop creative plans to help the student with Lyme succeed. Without the support of the school, the best efforts of the parents might not be enough to keep a kid on track, in school, and successful!! ——————————————– What THERAPEUTIC SOLUTIONS might we offer, to help deal with the FUNCTIONAL IMPAIRMENTS? Please note that these solutions do NOT directly connect with any particular item in the previous column. There are different categories of therapeutic solutions, but for now, I’d like to focus on what the school can do. They can make the difference between success and failure for a child with chronic Lyme.
We see several listed on this slide. I’ll mention others later. They DO WORK, and most of them are not very costly for the district or the state: For example, • The length of the school day • Time school day begins and ends • Length of homework assignments • Length and location of tests • Physical education requirements (as well as other accommodations) I’ll just mention briefly another important area where there can be therapeutic solutions, the home front: 7 Always keep in mind that when your child has chronic Lyme, he needs to be both SUPPORTED and ENCOURAGED. It’s important that you base your expectations of him on how he is able to function, on a day to day basis, but you don’t want him to feel like, or function like, an invalid. Have expectations of him, but keep them in line with where he is in his medical treatment, as well as whether he’s having a good day or a bad day. Some families need help dealing with children with Lyme, particularly if it effects their brain, and their school functioning. That is where psychotherapy and family therapy can be helpful. Therapy can serve an important role for kids and families with chronic Lyme, but it’s important to find a therapist who is at least Lyme-open, if not Lyme-literate. The kid and the parents should be involved, in a combination of individual and family therapy. The therapy should be concrete, focusing on the problems. ————————————- Now lets look more specifically at school.
As I mentioned earlier, cognitive problems are common with kids with Lyme disease, as are attentional problems. Kids with chronic Lyme might find it hard to retain new information. Lyme also can effect receptive and expressive language, visual-spatial processing, abstract reasoning, processing speed. Just as Lyme disease can effect any part of the body, it can effect any cognitive process. These kids may appear to be distracted easily, have poor concentration, appear scattered, have just about any symptom of attention deficit disorder. Or if the child had ADD before she got Lyme, her ADD symptoms are often exaggerated by the illness. These symptoms might be intermittent and transitory, given the nature of Lyme disease, making it even more difficult to develop an education plan. When I speak to teachers’ groups, I tell them that when they have a child with chronic neurological Lyme in their class, the child may appear learning disabled one day, seem normal the next. She may act like she’s got ADD on another day, and may appear withdrawn and fatigued the next. It’s a real challenge for the classroom teacher! So what can be done to educate these children? First lets look at the issue of free and equal public education, a wonderful and radical gift our democracy has given us. Free and equal public education gives all children a right to an education in this country, this state, this county. The law protects the disabled through entitlements, to level the playing field, so that they can benefit from an education, just as those who are not disabled can. There are state and federal bodies of law that provide for those entitlements, and they are available to all those who are disabled. They are not granted at the discretion of anyone – the teacher,
administrator, school superintendent!! 8 Some of these benefits are costly. There is always a push on the part of those responsible for balancing budgets to protect our tax dollars. There is always controversy regarding which programs should be prioritized. The result is that not all entitlements are easily gotten by those entitled to services. But parents of kids who are seriously ill with Lyme disease need to know that these entitlements exist, and that it is YOUR CHILD‘S RIGHT TO HAVE ACCOMMODATIONS, AS LONG AS THERE IS EVIDENCE THAT THEY ARE NECESSARY. I’d like to discuss three stages of supports the schools can provide. Most children will only need the first stage, and when a school is cooperative, coming from an understanding that these children are indeed ill, and that the school can be a partner in their recovery, the first stage might be all that is needed. The first stage is "Informal Educational Supports." These are supports that can be given to children without any formal plans, without classification, without formal meetings. A school administrator, for example, knowledgeable about the child’s illness, and the resulting impairments, might carefully select a classroom teacher or teachers that can develop flexible schedules for a child, permanently excusing a percentage of the required homework, giving extra time for testing, seating a distractible child near the source of instruction. These teachers give support and encouragement, without blaming the child for erratic performance. Depending on their teaching styles, some teachers have an easier time providing this flexibility than others, and if the administrator realizes this, and appropriately matches the child’s unique needs to the particular teacher, problems can be avoided from the beginning. Late assignments can be
accepted, without penalty, misspelling on tests that are not spelling tests can be excused. There is no battle ground here between the school and the parents. All are partners in providing this child with the education she deserves, and there is little if any cost to the school district, or to the state. There are two reasons why informal accommodations don’t always work. The first is that the school refuses to believe that this child, who looks healthy, or is laughing with his friends in the hall, is in fact sick. Parents should certainly be prepared with documentation, to back their assertion that their child has an illness that effects her learning – clear detailed letter from the treating doctor, neuropsychological evaluation, even brain SPECT scan, if there is one. The child has a right to an education, but the school has a right to the evidence that a medical problem that effects learning DOES exist. The second reason that informal supports might not work is that the child needs more than can be provided without a formal plan. If this is the case, a 504 committee needs to be convened, and a 504 plan is put into place. Section 504 is Federal civil rights legislation. Under it, a child with a disability has a right to accommodation to compensate for the disability. And, as I said earlier, it is an entitlement. 9 By law, a letter from the treating physician should be all that is needed in order to convene a 504 meeting, and develop a 504 plan. This is the easier of the two types of accommodations to put into place, and usually leads to a quicker meeting, therefore accommodations begin more quickly.
If the 504 does not seem to be working, if it does not provide for adequate accommodations, then a parent can request the Committee on Special Education to meet. A child with a health problem qualifies to be classified Other Health Impaired, an IEP (the plan for the child), is put into place, and supports are written into the plan. Supports available with an IEP that are not usually available under 504 include Resource Room, regular counseling for the child with a the school social worker, and school psychological evaluation every three years, as long as the child remains classified. ———————————- Here are some of the accommodations that might be put into place, and how I’ve seen children helped by these accommodations. Some may require that a neuropsychological evaluation document the particular learning problem that leads to the need for the accommodation. • Unlimited time for testing – a child is afforded extended time to take tests. Some children with Lyme have problems with the speed of processing information. These children get exceedingly anxious, trying to take a timed test. This accommodation removes the anxiety, literally gives them enough time to think. • Separate testing location – this is appropriate for children who have problems with focusing and concentration, and are easily distracted. There are fewer children taking the test, in a quiet location. • Tests read to student – this is for students who have particular verbal learning problems, in which their auditory learning is less impaired than their visual learning. • Excused from a percentage of their homework. Children with profound fatigue, who have a difficult time just getting through the school day, benefit greatly from having less work to do at home.
Keep in mind that more school work is not necessarily better. If a child is fatigued and has problems with memory and organization, of what use is hours worth of homework, at the end of the school day, or on the weekend? Of what benefit is increasing the child’s anxiety by requiring that he/she perform equal to the children who are well? Are they really being treated equally, if the child who is well can do the work in 1/4 to 1/2 the time as the child who is ill? Shouldn’t the sick child have at least an equal right to down time, time to relax, and recover, to face the next learning challenge? There are long lists of accommodations, designed to fit the needs of disabled children. Those with chronic Lyme, where documentation supports the problems and the need, are entitled to 10 these accommodations. Those who say it gives these kids an edge, rather than levelling the playing field, have never known someone with chronic Lyme. I suggest to those people that if these accommodations provide an edge for these kids, then so do hearing aids and eyeglasses. Ask everyone with those disabilities to do their work without those particular accommodations, as well!!! One more thing – you parents have a very important job in this process with the school – advocating for your child. Meetings with the school professionals can be very intimidating. They’ve got formats to follow, protocols, guidelines required by law to follow, for the very design of the meeting. They are used to these meetings. You are NOT – often leading to a very uncomfortable situation for parents. Go into the meeting prepared. Take your documentation, know what your child’s needs are, and DON’T GIVE UP!! If you don’t get support from the school the first time around, find a support group for parents of classified kids, attend meetings,
network with parents who have been dealing with their children’s schools for years. They have an expertise in education law, and they are very willing to help you. Someone from the group may even be willing to attend the meeting with you. You are entitled to bring anyone you wish. Take advantage of it. It’s not always an easy path, but you already know that about Lyme disease. It’s unfortunate that yet another part of the environment can be so difficult to negotiate for families with Lyme, but for right now, until there is a greater understanding of Lyme in the education community, that’s the way it is. So just remain in your child’s corner, and don’t give up!! Click here for printable pdf of article. Article Printed in Lyme Times Fall/Winter 2002-3 Issue To subscribe, contact: Lyme Disease Resource Center PO Box 707 Ukiah, CA 95482 1 yr (4 issues) domestic $35 Sandy Berenbaum, LCSW, BCD Family Connections Center for Counseling Offices in Brewster, NY and Southbury, CT www.lymefamilies.com Ph: (203) 240-7787 Fax: (203) 405-6200
© 2002
Identifying Lyme In The
Schools
How a child or adolescent with undiagnosed Lyme Disease might
present to:
The Teacher
· Lethargy, fatigue · Difficulty remaining in class
· Moodiness, depression, anxiety · Early morning absences
· Withdrawal from peers · Erratic academic performance
· Headaches or other physical
· Declining grades
complaints
· Behavioral problems · Attentional disorders
· Speaking and writing · Poor concentration and
difficulty memory
· Declining school attendance · TardinessThe School Nurse
· Frequent headaches · Gastrointestinal symptoms
· Joint pain, twitching · Vision Problems
· Depression, anxiety, mood
· Dizziness, disorientation
swings
· Sleep disturbance · Severe PMS
· Sensitivity to sound, light, or
· Profound fatigue
other stimulation
The Guidance Counselor
· Difficulty maintaining a full · Decline in academic
schedule performance
· Erratic attendance, tardiness · Withdrawal from peers
· Change to lower
· Difficulty remaining in class
functioning peer group
· Behavior problemsNote: Lyme disease symptoms may be persistent or transitory.
Click here for printable pdf of article.
Sandy Berenbaum, LCSW, BCD
Family Connections Center for Children
Offices in Brewster, NY and Southbury, CT
www.lymefamilies.com
Ph: (203) 240-7787 Fax: (203) 405-6200
© 2005
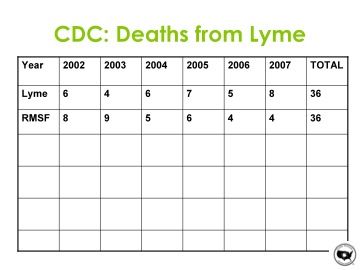
Deaths from Lyme Disease
Lyme disease can cause deaths. The chart below shows numbers
of deaths from Lyme disease and from Rocky Mountain spotted
fever (RMSF) (link to our RMSF page), another tick-borne
disease considered to be very serious. The numbers are taken
from the Centers for Disease Control and Prevention for the
years 2002 through 2007.Tick Control Measure Moves into 2012 Controlling ticks on property is something that government entities and the general public can do to help stop the spread of Lyme and tick-borne diseases. Now we have a device backed by scientific studies published in peer reviewed scientific journals. The device has been around a long time under a different name and has now been registered with EPA under a new name. Select TCS Tick Control System, formerly The Maxforce Tick Management System, is now EPA registered by Tick Box Technology Corporation based in Norwalk, CT. The owners of the company have tick control companies in five states. The TCS kills ticks during larval and nymph stages when they are contracting the Lyme bacteria and other tick-borne disease organisms from small rodents such as mice and chipmunks, interrupting the transmission of tick-borne diseases. Pesticide safety is always a concern to homeowners, and this
system minimizes that usage. The Select Tick Control System is now registered and available in Connecticut, Rhode Island, New Jersey, Minnesota, Pennsylvania, New York, Delaware, Maryland, Tennessee, Arizona, Iowa, Kansas , Virginia and New Hampshire. Other states may soon register the device. Go to www.TICKBOXTCS.COM for more information. NOTE: LDA does not endorse products nor is it affiliated with Tick Box Technology Corporation.
You can also read