ABC3 and Quality Assurance - Dr Karin Denton Director of Cancer screening QA (SW)
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ABC3 and Quality Assurance
Dr Karin Denton
Director of Cancer screening QA (SW)
Aims of ABC3 • To update terminology • To include management protocols for HPV triage and test of cure • To update performance indicators
Adequacy • Still awaiting HTA study • No change • HTA study will be published in May 13. • Likely to be an updated version of the chapter on adequacy
Changes to terminology
Previous terminology New Terminology Result code
Borderline change Borderline change in Squamous cells 8
Borderline change in endocervical cells 9
Mild dyskaryosis Low grade dyskaryosis 3
Borderline change
(koilocytic)
Moderate dyskaryosis High Grade dyskaryosis (moderate) 7
Severe dyskaryosis High Grade dyskaryosis (severe) 4
Severe High grade dyskaryosis ?invasive 5
Dyskaryosis?invasive squamous carcinoma
?Glandular Neoplasia ?Glandular neoplasia of endocervical 6
type
?Glandular neoplasia ( non cervical) 0
The revised BSCC terminology for abnormal cervical cytology. Denton KJ, Herbert A, Turnbull LS, Waddell C, Desai MS, Rana DN, Dudding N, Smith JH; British Society of Clinical Cytology. Cytopathology. 2008 Jun;19(3):137-57
Negative ( result code 2) • Samples may be reported as negative if classified “No further review” after scanning with the BD FocalPoint Slide profiler • https://www.csp.nhs.uk/files/F000206_NHSCS P%20GPG4.pdf
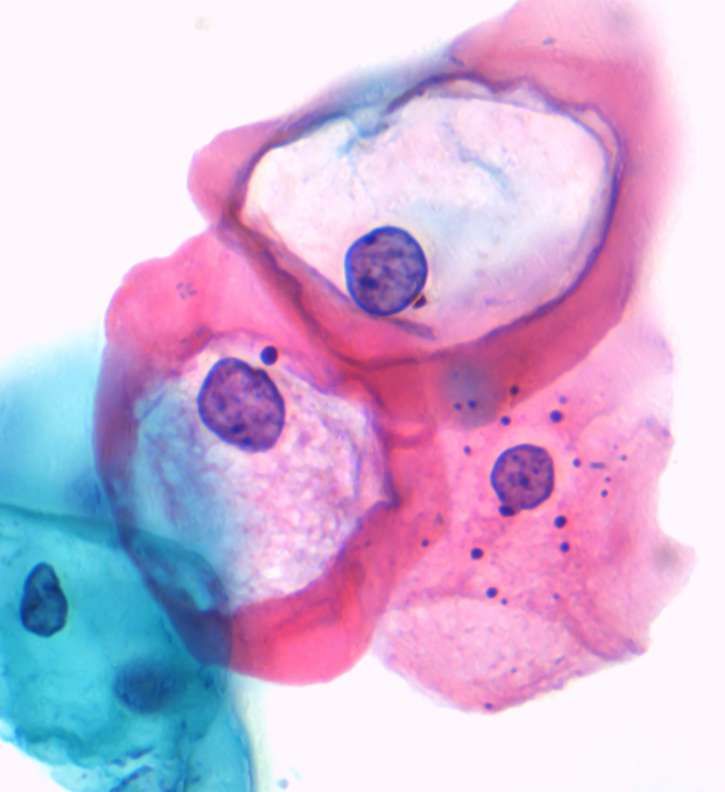
Low Grade Dyskaryosis
( result code 3)
•Dyskaryotic cells with a nuclear:cytoplasmic diameter
ratio of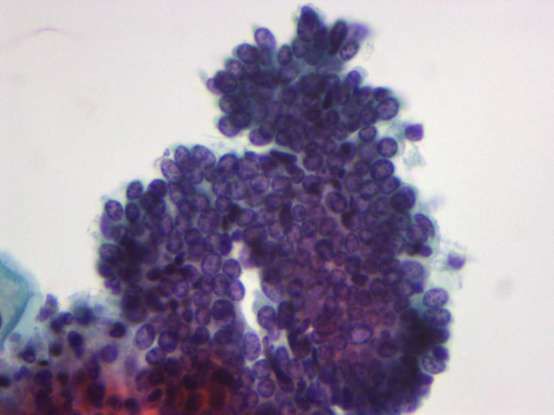
Low grade dyskaryosis
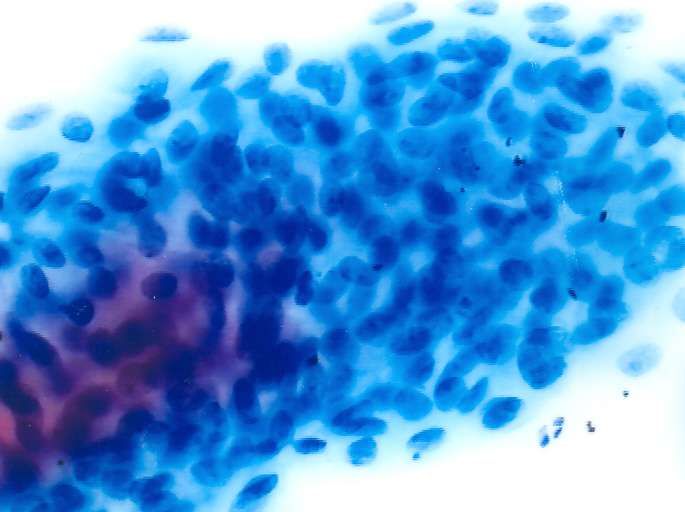
High Grade Dyskaryosis (Moderate) •Dyskaryotic cells are present with a nuclear:cytoplasmic diameter ratio of >50%. •Distinguishing precisely between high-grade dyskaryosis (moderate) and high-grade dyskaryosis (severe) is difficult and not entirely reproducible. • However, if the nuclear:cytoplasmic diameter ratio is felt to be
High Grade dyskaryosis ( Severe) This should be used when dyskaryotic cells are present with a nuclear:cytoplasmic diameter ratio of no less than 50%, and probably >75%.
• Sections on difficulties in grading dyskaryosis and difficulties in the identification of dyskaryosis
High grade dyskaryosis/?invasive
squamous cell carcinoma
(result code 5)
• No significant changes from ABC2? Glandular neoplasia of endocervical
type
• No change from ABC2?glandular neoplasia (non cervical)
Glandular neoplasia non-cervical
?Glandular Neoplasia (non-cervical) -
difficulties
• IUCD Changes
• Significance of psammoma bodies in a slide
lacking cytological abnormality
• Significance of endometrial cellsBorderline change in Squamous cells • As currently (except koilocytes) • No place for BC?high grade when HPV testing is used
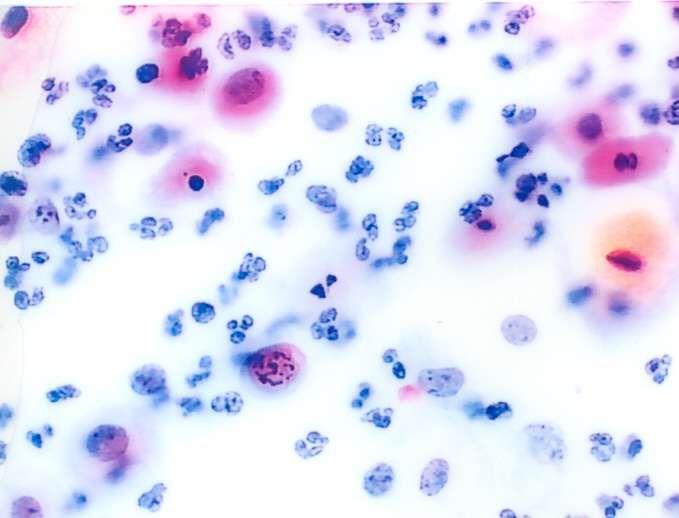
Borderline change - Pitfalls • Parakeratosis • Increasingly • Inflammation important in the era of • Metaplastic cells HPV primary screening • Atrophy
Keratinisation - Negative
Atrophy
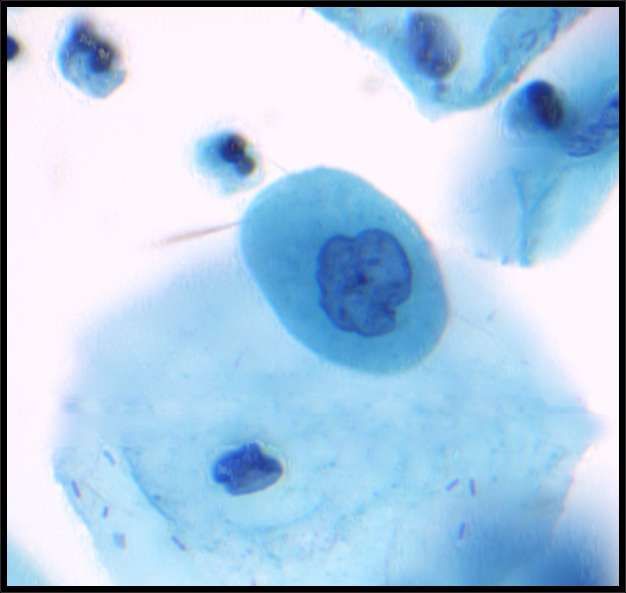
Borderline change in endocervical
cells
• Typically cell groups show either architectural
or nuclear features suggesting CGIN.
• Borderline change in endocervical cells should
be a rare diagnosis.
• Application of objective criteria and consensus
reporting are recommended to maintain the
specificity of the category and avoid
unnecessary colposcopy.BC in endocervical cells – difficulties • Cervicitis • Polyps • TEM • LUS
Management of borderline change and low grade dyskaryosis
Use of HPV testing outside Triage and
TOC protocol
All cases to be discussed at CIN meeting firstOff label HPV testing?
• Women undergoing long term colposcopy surveillance for low grade
CIN or unresolved abnormal cytology, and have not been previously
tested for HR-HPV. This could include women with cervical stenosis
where colposcopy is non-contributory
• Women who have undergone hysterectomy for CIN, or CIN was found in
the hysterectomy specimen, and subsequently present with abnormal
vault cytology but no evidence of high grade VAIN
• Women who experience difficulty tolerating colposcopy and therefore
the examination is unsatisfactory.
• Women discussed at the colposcopy MDT because of persistent
mismatch between high grade cytology and low grade histology when a
decision has been made not to treat.Standard Cytology Result, HPV
Infection and Action Codes
Each time a woman is screened a standard set
of details is recorded on her cervical screening
record.
- the coded cytology result
- the HPV infection code
- the action code which indicates the
recallHPV Infection codes
• 0 no high risk HPV DNA detected
• 9 high risk HPV DNA detected
• U HPV test result unavailable or
unreliable
• Under no circumstances may the 'U' infection code
be used where an HPV test cannot be carried out
due to equipment failure or any other problem
unrelated to the quality of the sample.Coding multiple diagnoses In rare cases, a woman’s cytology test may reveal the co-existence of non-cervical glandular neoplasia with cervical abnormalities. Treatment of the former falls outside the scope of the NHS CSP, but the following protocol should be followed to ensure appropriate management. •Where a woman has non-cervical glandular neoplasia and any form of cervical cytological abnormality, it is the latter that should be recorded and sent to NHAIS. This will determine the woman’s management within the NHS CSP. • However, arrangements must be made to inform the woman of her diagnosis of noncervical glandular neoplasia. Such communications are particularly sensitive, because the woman may previously have received a letter referring only to a borderline or low-grade cytological abnormality. • The woman must receive an urgent referral, probably to gynaecology. A member of the consultant medical staff at the cervical cytology laboratory must ensure that the referral is made and that failsafe procedures are in place, according to local arrangements.
Performance indicators ‘the objective of cervical screening is to reduce cervical cancer incidence and mortality by screening with a high sensitivity for the detection of CIN2 or worse, whilst maintaining a high specificity’.
ABC2 performance monitoring
• Abnormality detection rate - 10-90th centiles
• Sensitivity (lab and individual)
– Defined as proportion of abnormal cases identified at
primary screening
– 90% all grades
– 95% high grade
• PPV
– Defined as proportion of samples showing Moderate
dyskaryosis or worse found to have CIN2 or worse
– 10-90th centilesChallenges of performance monitoring
in a changing programme
• LBC
• HPV vaccine
• HPV Triage and TOC
• Lab configurationABC3 – mandatory performance
monitoring
Criteria Performance Range
indicator
Inadequate sample % all samples 5th - 95th percentile
reports
PPV for CIN2 or worse % of women referred 5th - 95th percentile
with high grade
cytology or worse
whose biopsy is
reported as CIN2 or
worse
Referral Value Number of women 5th-95th percentile
referred to colposcopy
to detect one CIN2 or
worse lesionTPV and RV • TPV (Total predictive value)is the percentage of women referred who have a histological outcome of CIN2+ • RV ( referral value) is the inverse of TPV
80
60
40
20
0 Referral Value from 2010/11 KC61 part C2
1 2 3 4 5
RVMeasures which may be helpful
40
30
20
10
PPV/APV
0
60 70 80 90 100
PPV%
95% CI Fitted values
APV%Mean CIN score
Examples
Outcome Lab A Lab B Lab C
Cervical Cancer 15 15 15
CIN 3 50 50 50
CIN2 30 50 50
CIN1 10 35 70
HPV only, no disease* 5 15 65
TOTAL 110 165 250
MCS 2.5 2.1 1.5
Lab A is operating at too high a specificity to detect all CIN 2 lesions and could be
considered as only having a high sensitivity for CIN 3. Lab B may be more closely
following the concept of a high detection for CIN 2 or worse whilst referring the
minimum number of women and Lab C by referring women who have a high
proportion of histological outcomes of CIN 1 and ‘HPV only’ operating at too low a
specificity.SSS Results from different centres
HPV positive rate by site and initial cytology 1
Site Borderline Mild Total
n HPV +ve n HPV +ve n HPV +ve
(%) (%) (%)
A 1263 866 (68.6) 404 370 (91.6) 1667 1236 (74.1)
B 643 224 (34.8) 523 384 (73.4) 1116 608 (52.1)
C 2557 1111 (43.4) 1507 1232 (81.8) 4064 2343 (57.7)
D 789 455 (57.7) 420 372 (88.6) 1209 827 (68.4)
E 663 406 (61.2) 557 500 (89.8) 1220 906 (74.3)
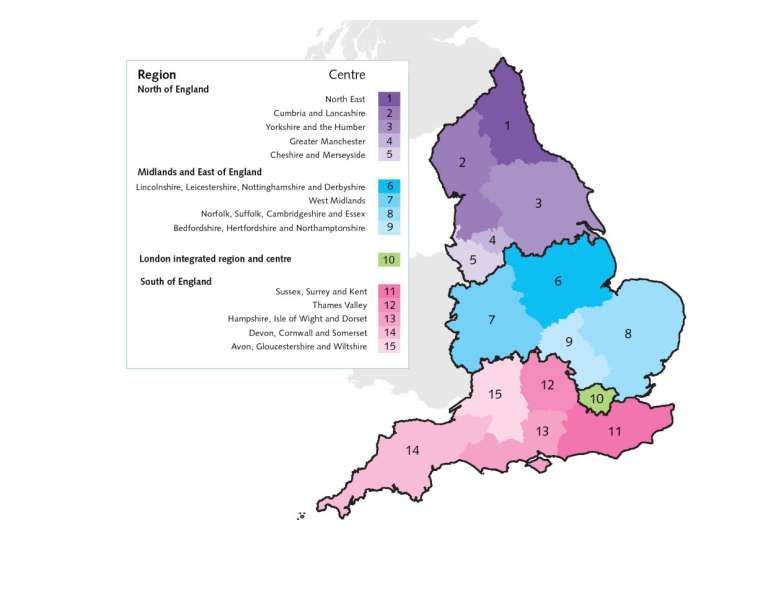
F 592 434 (73.3) 133 116 (87.2) 7255 550 (75.9)Quality Assurance in the new
NHS8 Knowledge and Intelligence Hubs • London • South West • South East • West Midlands • East Midlands • North West • Yorkshire and Humber • North East
Into the civil service...
Cervical screening QA • No Change – Standards defined by national office – Regional QARC – Visits, reports, advice
Cervical Screening QA
• Will change
– Some key posts not yet appointed
– E-mail addresses
– Incident management
– Relationships with commissioners
• AT’s
• But also CCG’s, LA’s, and PHE
– Routes for performance management
– Direct accountability to national officeYou can also read