BELGIAN CONSENSUS MEETING - on TRAVEL MEDICINE May 31, 2013
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
BELGIAN
CONSENSUS MEETING
on TRAVEL MEDICINE
May 31, 2013
Pr. A. Van Gompel (ITG)
Pr. F. Jacobs (Hôp. Erasme, ULB)
Belgian Pr. P. Lacor (UZ-Brussel)
Scientific Study Dr. Ph. Leonard (CHU-ULg)
Pr. W. Peetermans (U.Z. - K.U.Leuven)
Group on Travel Pr. S. Callens(UZ.- U.Gent)
Dr. S.Quoilin (iph.fgov.be)
Medicine Dr.P. Soentjens (Belgian Defence)
Pr. B. Vandercam (CHU. St. Luc, UCL)
Pr. Y. Van Laethem (CHU. St. Pierre, ULB)
PART 1a yellow fever version 23-08-2013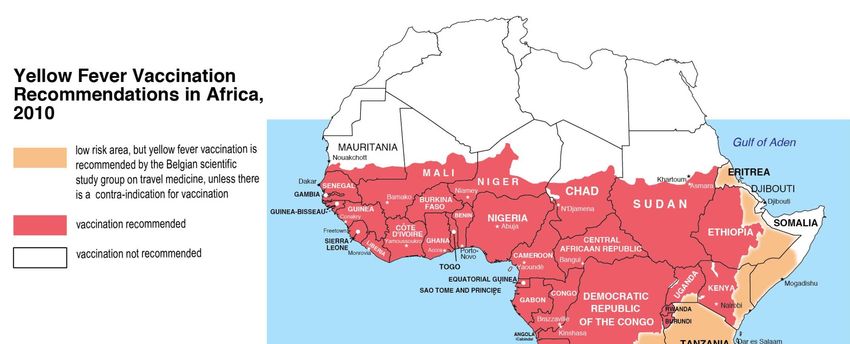
2013
REPORT
BELGIAN CONSENSUS MEETING on TRAVEL MEDICINE
May 31, 2013 – PART 1a
• The consensus meeting was chaired by A. Van Gompel
• Secretary of the meeting was Y, Van Laethem
• A preliminary PowerPoint, prepared by A. Van Gompel,
was presented
• The discussion and recommendations of the
meeting are included in this finale presentation.
• The ESSENTIAL SLIDES (pdf-version) & the
CONSENSUS BROCHURE (in Dutch and French)
highlighting the proposals for changes will been sent to
all participants. May be used for teaching.
• These documents will serve as a proposal for approval
by the governmental Belgian Health Council – section
Vaccinations, on 10-10-2013
• Responsable final redaction : A. Van Gompel
2013 Not an exhaustive review of travel medicine • What has changed • Tips • Answers to questions, asked in the last months • All slides of the consensus document, as well as the hand-outs will be available on the website of the ITM, and may be used for teaching purposes
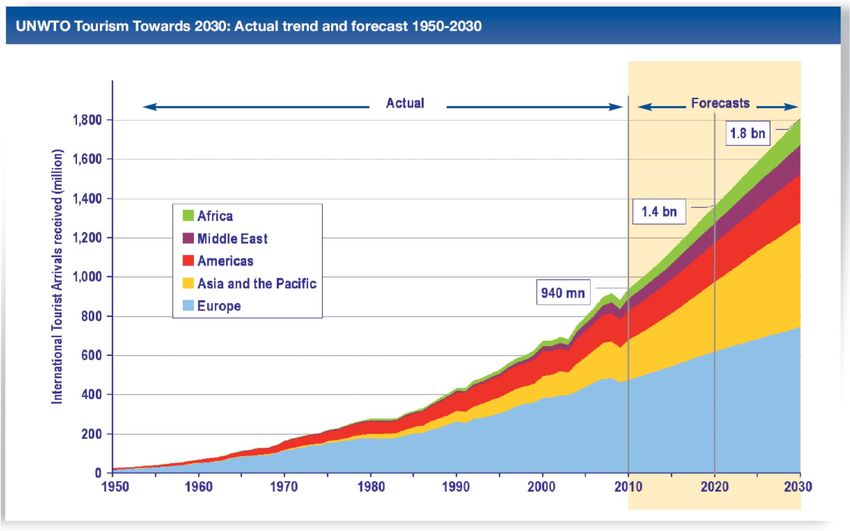
2013 www.unwto.org
2010
2013 www.unwto.org
2013 www.unwto.org
2013 Local Organizing Committee (LOC) and Regional Advisory Committee (RAC) CISTM 2013 Maastricht The Netherlands Chair: Gerard JB Sonder MD PhD director National Coordination Center for Travelers Health Advice LCR Amsterdam For Belgium: Alfons Van Gompel MD Antwerpen (Instituut voor Tropische Geneeskunde ITG Antwerpen) Steven Callens MD PhD Gent (Universitair Ziekenhuis-Universiteit Gent UZ.- U.Gent) Yves Van Laethem MD Brussel (Hôpital Staint- Pierre, Université Libre de Bruxelles ULB) Philippe Leonard MD Luik (Centre Hospitalier Universitaire- Université de Liège CHU-ULg)

2013 PDF’s of the lectures are available on the website of the ISTM for the ISTM members (ISTM has 65 Belgian members) and probably also non-members http://www.istm.org/WebForms/M embers/MemberActivities/Meeting s/Congresses/cistm13/Materials.a spx
2013
• Additional sources for the update
– the 2012 edition of International Travel and Health (WHO)
– the 2014 edition of Health Information for International Travel (CDC)
– The discussion forum of the International Society for Travel Medicine
– International literature
• The updated 2012-13-edition of “Medasso”, edited by A. Van Gompel and
the staff of the medical service of the Institute for Tropical Medicine Antwerp,
is also recommended as a valuable source of information.
www.who.int/ith http://wwwn.cdc.gov/travel/contentY
ellowBook.aspx2012
http://www.who.int/ith/chapters/en/index.html
http://www.who.int/ith/chapters/fr/index.html
COUNTRY LISTV – LISTE PAR PAYS
Only these chapter are freely downloadable2013 • Not every advice is applicable to / acceptable in the European situation • many maps are not nuanced enough (e,g, schisto-map; malaria country-maps)
Gebruik geen verouderde versies, daar ze onbruikbaar zijn geworden en check steeds de meest recente electronische versie ! Les éditions imprimées anciennes sont dépassées et donc inutilisables ! Consultez toujours la version électronique la plus récente.
2013 PART 1 • 1.a - Vaccination for Yellow Fever • 1.b - Malaria PART 2 • 2.A - Other vaccinations • 2.B - TD, other infections, …., • 2.C - VARIA
Yellow Fever
WHO - Yellow Fever Vaccination
WER 17-05-2013 SAGE
WER 05-07-2013 POSITION PAPER
WER 12-07-2013 AFRICA LATIN AMERICAWHO - Yellow Fever Vaccination
1. LIFELONG IMMUNITY
2. MEASLES VACCINATION
3. PREGNANCY & BREASTFEEDING
4. IMMUNODEPRESSION – YOUNG & OLD AGEWER 17-05-2013 SAGE
YELLOW FEVER VACCINATION
induces LIFELONG
PROTECTION2013
SAGE 17-05-2013
New WHO recommendations ??“specific risk groups could possibly benefit from a second primary or booster dose” such as infants (below 2 years ?) or HIV-infected patients • other (not-severely) immunosuppressed patients ? • pregnant women ? • children who got MMR and YF vaccine within less than 30 days ? • Immunoscenescence ? 2013
POSITION PAPER 05-07-2013
New WHO recommendations CISTM 13 Gilles Poumerol, WHO, Switzerland Monday, 20 May 2013 18.30-19.15 at the CISTM-13 Maastricht The Brussels Room, Level 0, Room 0.4 Special Update: Highlights from the New Editions, WHO and CDC
New WHO recommendations CISTM 13 • No changes to the provisions for the duration of validity of the yellow fever vaccination certificate under the international Health Regulations • WHO will discuss with the countries how to best proceed • Countries have discretion to implement the certificate procedure • WHO will stimulate individual countries to take into account this scientific advice • Changes in the implementation by countries will take time • Prevailing requirements will continue
How to cope with the new scientific WHO/SAGE guideline versus the yet unchanged International Health Regulation ? Scientific 2013 WHO advice: “If no immune problems exist, the immunity is considered lifelong” Somebody who will be vaccinated today, can be told “the vaccination is valid at least for 10 years – probably lifelong” Swiss (BOFSP 15-7-13) :” Il est recommandé de ne plus indiquer la date d’expiration mais seulement celle du début de validité (10 jours à compter de la date de vaccination)” – this position is endorsed by the Belgian Scientific Studygroup on Travel Medicine “specific risk groups could possibly benefit from a second primary or booster dose” such as – infants (below 2 years ?) – HIV-infected patients QUID • other (not-severely) immunosuppressed patients ? • pregnant women ? • children who got MMR and YF vaccine within less than 30 days ? • Immunoscenescence ?
… on the one hand the situation may now
become more simple
– For countries with risk of yellow fever
transmission not requiring proof of
vaccination: one vaccination is valid for life
– For persons with an actual absolute or relative
contra-indication, but formerly vaccinated
against yellow fever before becoming
immune-depressed, the immunity is
supposedly also longstanding possibly for life… on the other hand the situation may now
become temporarily also more complex
– At this moment many countries (with or without
risk of YF transmission) still require a renewed
proof of vaccination after 10 years – if a person
plans to cross the border(or in transit)
• from one country with (a real or supposed) risk for YF
transmission
• to another country
she/he will then need an up-to-date Certificate –
that traveler may think to be in order
“immunologically”, but not “politically” or “legally”
or administratively”
– No waiver can be delivered but for proper medical
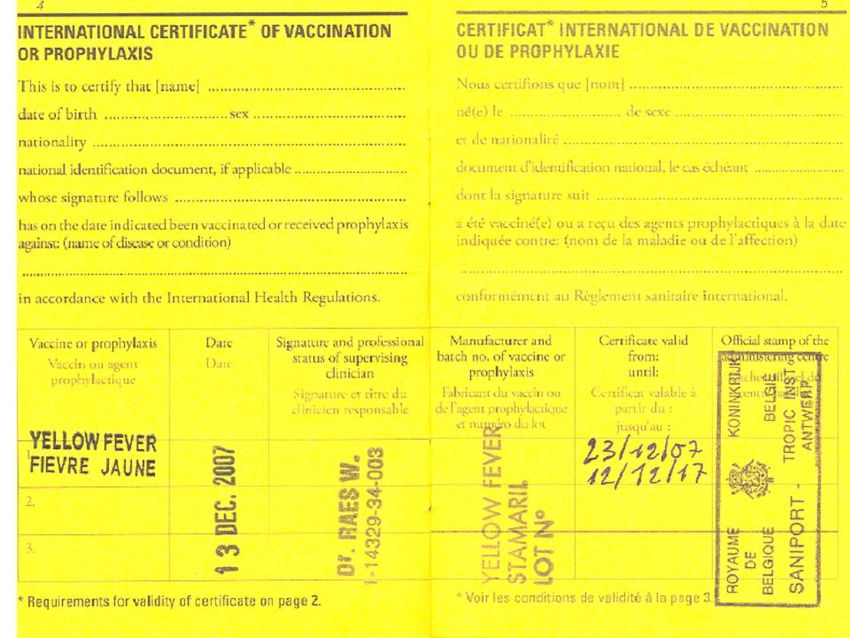
reasons (absolute or relative contra-indication)15‐07‐2013 L’Office fédéral de la santé publique, le Comité d’experts en médecine des voyages et la Commission fédérale pour les vaccinations après examen attentif des documents mis à disposition ont adapté la recommandation de la manière suivante : 1. Une vaccination de rappel contre la fièvre jaune n’est désormais plus recommandée aux voyageurs qui se rendent dans une zone d’endémie dans laquelle aucun certificat de vaccination contre la fièvre jaune n’est exigé. 2. Lors de voyage dans les pays avec certificat de vaccination obligatoire, la pratique vaccinale appliquée jusqu’ici reste pour l’instant inchangée. Un rappel tous les 10 ans doit être effectué. L’abandon des rappels tous les 10 ans ne s’appliquera qu’au fur et à mesure que les pays concernés auront intégré cette modification à leurs exigences de vaccination antiamarile. 3. Toute vaccination contre la fièvre jaune (1e dose ou rappel) doit être inscrite dans le certificat international. Il est recommandé de ne plus indiquer la date d’expiration mais seulement celle du début de validité (10 jours à compter de la date de vaccination). Le SAGE a par ailleurs demandé à l’OMS de revoir les dispositions relatives à la période de validité des certificats internationaux de vaccination antiamarile dans le règlement sanitaire international (RSI) 2005.
2013 The wording needs to be changed (in the fall of 2013)
Swiss example :
WHO - Yellow Fever Vaccination
MEASLES VACCINATIONSAGE 17-05-2013
2013SAGE 17-05-2013
POSITION PAPER 05-07-2013
POSITION PAPER 05-07-2013
12-07-2013
Combination of life-attenuated vaccines 2012
Vaccine 1998
2011 Vaccine 2011
2011
Combination of YF-vaccine and MMR-
vaccine
• Administration of two life-attenuated vaccines can be
done simultaneously without relevant influence on
immunogenicity.
• For measles and varicella the doses, when not given
simultaneously, must be separated by 30 days
because of the interferon production induced by the
first vaccine shot.
• This is not so for the combination of measles and
yellow fever vaccination.
• CDC says that any interval can be used if yellow fever
vaccination is indicated, irrespective when measles
vaccine was given previously. …….
• Studies are actually ongoing that might change this
advice :2011 combination of measles and yellow fever vaccination • Subjects injected YFV and MMR simultaneously had lower seroconversion rates – 90% for rubella, 70% for yellow fever and 61% for mumps – compared with those vaccinated 30 days apart – 97% for rubella, 87% for yellow fever and 71% for mumps. • Seroconversion rates for measles were higher than 98% in both comparison groups. • Geometric mean titers for rubella and for yellow fever were approximately three times higher among those who got the vaccines 30 days apart. • For measles and mumps antibodies GMTs were similar across groups.
2011 combination of measles and yellow fever vaccination • MMR’s interference in immune response of YFV and YFV’s interference in immune response of rubella and mumps components of MMR had never been reported before but are consistent with previous observations from other live vaccines. • These results may affect the recommendations regarding primary vaccination with yellow fever vaccine and MMR.
2011 combination of measles and yellow fever vaccination • These conclusions apply to primary vaccination in children less than two years old. • As primary vaccination against yellow fever in older children and adults, and a booster dose at any age induce stronger immune response, interference from other live virus vaccines should be less pronounced and possibly irrelevant.
CDC 2014
Simultaneous Administration of Other
Vaccines and Drugs
• ACIP recommends that yellow fever vaccine be given at the
same time as other live-virus vaccines.
• Otherwise, the clinician should wait 30 days between
vaccinations, as the immune response to one live-virus
vaccine might be impaired if administered within 30 days
of another live-virus vaccine.
• A recent study involving the simultaneous administration
of yellow fever and measles-mumps-rubella (MMR)
vaccines in children found a decrease in the immune
response against yellow fever, mumps, and rubella when
the vaccines were given on the same day versus 30 days
apart.
• Additional studies are needed to confirm these findings, but
they suggest that if possible, yellow fever and MMR
should be given 30 days apart.WHO - Yellow Fever Vaccination
PREGNANCY &
BREASTFEEDINGSAGE 17-05-2013
2013SAGE 17-05-2013
20133 cases of benign self-limiting meningoencephalitis because of
transmission of vaccine strain of yellow fever virus to an infant via
breast milk have been published
• 1 Kuhn S, Twele-Montecinos L, MacDonald J, Webster P, Law B.
Case report: probable transmission of vaccine strain of yellow fever
virus to an infant via breast milk. CMAJ. 2011;183(4):E243-245.
Epub 2011/02/18.
• 2. Transmission of yellow fever vaccine virus through breast-
feeding - Brazil, 2009. MMWR Morb Mortal Wkly Rep.
2010;59(5):130-132. Epub 2010/02/13.
• 3. Traiber C, Coelho-Amaral P, Ritter VR, Winge A. Infant
meningoencephalitis caused by yellow fever vaccine virus
transmitted via breastmilk. J Pediatr (Rio J). 2011;87(3):269-272.
Epub 2011/04/05.POSITION PAPER 05-07-2013
POSITION PAPER 05-07-2013
Relapsing remitting MS
2012WHO - Yellow Fever Vaccination
IMMUNODEPRESSION
YOUNG & OLD AGE2013 SAGE 17-05-2013
SAGE 17-05-2013
POSITION PAPER 05-07-2013
POSITION PAPER 05-07-2013
POSITION PAPER 05-07-2013
POSITION PAPER 05-07-2013
Yellow Fever Vaccination
and
Relapsing & Remitting
Multiple SclerosisRelapsing remitting MS ???
20122012
CDC 2012 YF vacc & Multiple Sclerosis
• The Multiple Sclerosis Council for Clinical Practice Guidelines, published in 2001,
contain the clinical practice guidance on “Immunizations and Multiple Sclerosis.”
• The expert panel that developed this guidance used CDC recommendations as their
foundation. Updated comments are posted on the National Multiple Sclerosis Society
website (www.nationalmssociety.org ).
• People with MS who are having a serious relapse (exacerbation) interfering
with the activities of daily living should defer immunization until 4–6 weeks
after onset of the relapse.
• Inactivated vaccines are generally considered safe for people with MS. Administration
of tetanus, hepatitis B, or influenza vaccines does not appear to increase the short-
term risk of relapses in people with MS. However, published studies are lacking on
the safety and efficacy of other vaccines (such as those against pneumonia,
meningitis, typhoid, polio, hepatitis A, human papilloma virus, and pertussis).
Inactivated vaccines are theoretically safe for people being treated with an interferon
medication, glatiramer acetate, mitoxantrone, or natalizumab, although efficacy data
are lacking.
• In the past, many practicing neurologists have strongly advised their MS
patients against the use of live-virus vaccines at any time.
• Live-virus vaccines should not be given to people during therapy with
immunosuppressants, such as mitoxantrone, azathioprine, methotrexate, or
cyclophosphamide, or during chronic corticosteroid therapy.
• However, a few published studies suggest that measles, rubella, and varicella
vaccines may be safe in people with MS if administered several weeks in advance of,
or several weeks after, immunosuppressive therapy.
• Yellow fever vaccine …… should not be given unless there is a compelling
reason to do so (such as unavoidable direct exposure) and there has been a
consultation with the patient’s neurologist.2013
CDC 2014 YF vacc & Multiple Sclerosis
• Inactivated vaccines are generally considered safe for people with MS, although
vaccination should be delayed during clinically significant relapses until patients
have stabilized or begun to improve from the relapse, typically 4–6 weeks after
it began.
• Administration of tetanus, hepatitis B, or influenza vaccines does not appear to
increase the short-term risk of relapses in people with MS. However, published
studies are lacking on the safety and efficacy of other vaccines (such as those
against hepatitis A, human papilloma virus, meningitis, pertussis, pneumonia,
polio, and typhoid). Inactivated vaccines are theoretically safe for people being
treated with an interferon medication, glatiramer acetate, mitoxantrone, fingolimod, or
natalizumab, although efficacy data are lacking.
• A few published studies suggest that measles, rubella, varicella, and zoster
vaccines may be safe in people with stable MS if administered 1 month before
starting or 1 month after discontinuing immunosuppressive therapy. Modern MS
therapy includes aggressive and early immunomodulatory therapy for almost all MS
patients, even those with stable disease.
• Live-virus vaccines should not be given to people with MS during therapy with
immunosuppressants, such as mitoxantrone, azathioprine, methotrexate, or
cyclophosphamide; during chronic corticosteroid therapy; or during therapy with the
agents listed in Table 8-02. However, patients on glatiramer acetate and interferons
have more limited immune deficits.
• Yellow fever vaccine and smallpox vaccine have not been well studied in people
with MS and should only be given if there is a compelling reason to do so (such
as unavoidable direct exposure and the risks of potential adverse events are
carefully weighed against the likelihood of exposure to these potentially fatal
illnesses); these decisions should be made in consultation with the patient’s
neurologist.Useful literature
• ORIGINAL STUDY Yellow Fever Vaccination and Increased Relapse Rate
in Travelers With Multiple Sclerosis. Farez & Correale. Arch Neurol.
2011;68(10):1267-1271. Online June 13, 2011.
doi:10.1001/archneurol.2011.131
• COMMENTS AND OPINIONS Methodological Issues With the Risk of
Relapse Study in Patients With Multiple Sclerosis After Yellow Fever
Vaccination. Pool & al. & REPLY Farez & Correale. Arch Neurol.
2012;69(1):144-145
• REVIEW Vaccination against infection in patients with multiple sclerosis,
Loebermann & al. Nat. Rev. Neurol. 8, 143–151 (2012); online 24 January
2012, doi:10.1038/nrneurol.2012.8
• SEP et vaccins : l'état des lieux, Mrejen & Papeix (département de
Neurologie, hôpital de la Salpêtrière, Paris) Journal international de
médecine 2012 Publié le 11/07/2012 http://www.jim.fr“Medasso” 2012-13
• Patiënten met Multipele Sclerose mogen ook gevaccineerd worden
indien ze geen immuundeprimerende medicatie nemen – in geval
van de relapsing-remitting vorm moet er wel een afweging gemaakt
worden:
• In 2011 werd een studie gepubliceerd (Archives of Neurology -
Farez & Correale, 2011) over een kleine groep patiënten met
relapsing-remitting Multipele Sclerose die gele koorts vaccinatie
gekregen hadden – er werd een significante stijging van relapse
risico vastgesteld in de 6 weken na de vaccinatie, vergeleken met
de twee jaar follow-up periode nadien.
• Hoewel het om een kleine niet-dubbel blinde studie gaat, met grote
confidentie-intervallen, moet bij patiënten met MS die naar een
gelekoortsgebied reizen het risico voor een relapse dus zorgvuldig
afgewogen worden tegen het risico van blootstelling aan de
potentieel dodelijke gele koorts.
• Voor details in verband met vaccinaties bij Multipele Sclerose zie
ook www.nationalmssociety.org – search: 'vaccinations'.“Medasso” 2012-13
• Les patients atteints de sclérose en plaques peuvent également être
vaccinés s’ils ne prennent pas de médication immunosuppressive –
en cas de type à rechutes et rémissions il faut peser le pour et le
contre :
• en 2011, une étude a été publiée (Archives of Neurology - Farez &
Correale, 2011) sur un petit groupe de patients avec une sclérose
de type à et rechutes et rémissions ayant reçu une vaccination
contre la fièvre jaune – et on a constaté une augmentation
significative du risque de rechute pendant les 6 semaines après la
vaccination, comparé avec la période de suivi de deux ans de suivi
ultérieure ensuite.
• Même s’il ne s’agit que d’une petite étude, non en double aveugle,
avec de grands écarts d’intervalles de confiance, il faut
soigneusement peser le pour et le contre du risque de rechute
comparé au risque d’exposition à la fièvre jaune potentiellement
mortelle pour les patients avec SEP qui se rendent dans une un
pays endémique de fièvre jaune.
• Pour de plus amples détails en matière de vaccinations dans la
sclérose en plaques, voir également www.nationalmssociety.org –
search: 'vaccinations'.In the 2012 National consensus report was said : “There is a relative contraindication / precaution for using live-virus vaccines in patients with an exacerbation of relapsing remitting multiple sclerosis.” This will be for 2013 changed in to : • In a limited and contested study of YF vaccination in clinical relapsing remitting MS the risk of relapse within 3 months after YF vaccination was significantly increased. • Therefore YF vaccination is generally contra- indicated (= relative contraindication / precaution), although the risk of relapse due to vaccination should always be weighed against de risk of acquiring a letal travel related infection.’
2013 CDC YF vacc & Multiple Sclerosis • MS en gele koortsvaccinatie – zie mailverkeer met Paul De Munter • & travelmed april 2013
Some former slides on Yellow Fever Vaccination
2012
For Details See WWW.ITG.BE
= strongly
recommended or even
obligatory
See www.itg.beFor Details See WWW.ITG.BE
2012
= strongly recommended
or even obligatory
See www.itg.be2011
2011 The Belgian group (as well as The Netherlands) reformulates this advice as follows: “low risk area, but yellow fever vaccination is recommended unless there is a (relative) contra-indication for vaccination”.
= CHANGED IN :
2011
• (1) Het blootstellingsrisicio voor gele • (1) Le risque d'exposition au virus de la
koorts virus is in deze gebieden laag fièvre jaune dans ces régions est bas à
tot zeer laag. Gele koorts vaccinatie très bas. La vaccination contre la fièvre
wordt aangeraden op voorwaarde dat jaune est recommandée à condition que
er geen (relatieve) medische le patient ne présente pas de contre-
tegenindiciatie bestaat. Gele koorts indications (relatives) à la vaccination.
vaccinatie is zeker aanbevolen voor La vaccination contre la fièvre jaune est
reizigers die een verhoogd certainement recommandée chez les
blootstellingsrisico hebben met het gele voyageurs qui sont à risque accru
koorts virus (bijvoorbeeld lang verblijf, d'exposition au virus de la fièvre jaune
verhoogde blootstelling aan muggen (par exemple un voyage prolongé, une
overdag, onvermijdbare exposition importante à des moustiques
muggensteken). pendant la journée, l'incapacité à éviter
• Bij het overwegen van de gele koorts les piqûres de moustiques).
vaccinatie moet bij elke reiziger het • Lorsque l'on considère la vaccination, il
blootstellingsrisico met het gele koorts faut prendre en compte chez chaque
virus, de vereisten van het voyageur le risque d'exposition au virus
desbetreffende land, de mogelijke de la fièvre jaune, les exigences en
toekomstige reizen naar gele koorts matières vaccinales du pays visité, les
gebieden en de individuele éventuels futurs voyages dans des zones
risicofactoren afgewogen worden à risque, ainsi que les facteurs de risque
tegenover de zeer zeldzame ernstige individuels (par ex. âge,
neveneffecten bij een primovaccinatie. immunosuppression) de réactions
Dit kan steeds besproken worden in sévères très rarement associées à la
het gespecialiseerde primo-vaccination.
vaccinatiecentrum. • Ceci est à discuter au sein du centre de
vaccination.2008
2008
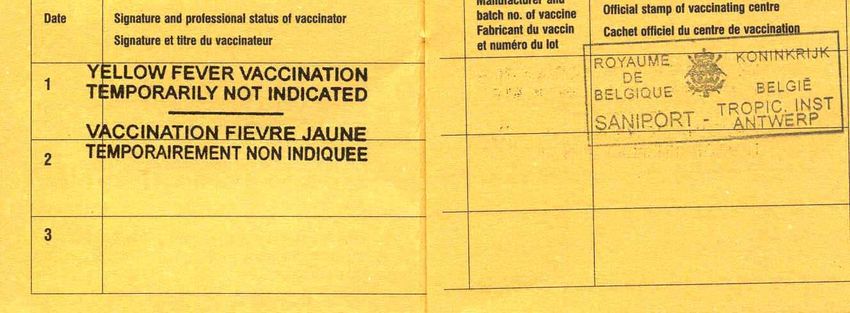
yellow fever certificate : waiver / exemption.
• If a waiver has to be declared, it must be specified that the
waiver is given for a limited period of time. The proposed
statement says “yellow fever vaccination temporarily not
indicated”.
• It seems wise to give an explanatory letter to the patient who
then must decide to whom this letter is given in order to
explain the medical reason for the yellow fever vaccination
waiver (CDC 2008)
No need for children less than 6 mo – 12 mo
(according to guidelines per country)yellow fever certificate : waiver / exemption 2006 + indication of time period
WHO 2008
yellow fever certificate : waiver / exemption
WHO : no need to specify diagnosis
Travellers who possess an exemption from yellow fever vaccination, signed
by an authorized medical officer or an authorized health worker, may
nevertheless be allowed entry, subject to the provisions of the foregoing
paragraph of this Annex and to being provided with information regarding
protection from yellow fever vectors. Should the travellers not be
quarantined, they may be required to report any feverish or other
symptoms to the competent authority and be placed under surveillance.
Les voyageurs en possession d’un certificat d’exemption de vaccination
antiamarile signé par un médecin autorisé ou un agent de santé agréé
peuvent néanmoins être autorisés à entrer sur le territoire, sous réserve
des dispositions de l’alinéa précédent de la présente annexe et pour
autant qu’ils aient reçu des informations sur la protection contre les
vecteurs de la fièvre jaune. Les voyageurs qui n’ont pas été mis en
quarantaine peuvent être tenus de signaler tout symptôme fébrile ou tout
autre symptôme pertinent à l’autorité compétente et placés sous
surveillance.
http://www.who.int/csr/ihr/wha_58_3/en/index.html IHR 2005CDC
http://wwwn.cdc.gov/travel/yellowBookCh4-YellowFever.aspx
2008
CDC model
Waiver Letter from Physicians
contains the diagnosis
A physician’s letter clearly stating the contraindications to vaccination is
acceptable to some governments. Ideally, it should be written on letterhead stationery
and bear the stamp used by health department and official immunization centers to
validate the ICVP. Under these conditions, it is also useful for the traveler to obtain
specific and authoritative advice from the embassy or consulate of the country or
countries he or she plans to visit. Waivers of requirements obtained from embassies or
consulates should be documented by appropriate letters and retained for presentation
with the completed Medical Contraindication to Vaccination section of the ICVP2011
Transit in aeroport
In principle yellow fever vaccination is not required
if the traveler stays in the transit zone of the
airport for maximum 12 hours with an entry and
exit record of the same day.
Some countries require vaccination certificate for
any transit in an endemic country, irrespective of
the duration (e.g. South Africa uses any transit
time).
The recommendation must also take into
consideration that flight itineraries can change
unannounced (e.g. stopover in Ethiopia or
Senegal).
Changes ?Belgian cases ?? 2012
risk assesment 2010
!! PRIMOVACCINATION !!
• the risk of a serious side effect due to vaccination
(varying from 0, 00… to 4 / 1.000.000 …..depending on age)
is on average lower than
• The risk of death caused by Yellow Fever in an endemic area
(varying from 20 to 1600 / 1.000.000 per month)End Yellow Fever
You can also read