COVERAGE EVALUATION OF JAPANESE ENCEPHALITIS SUPPLEMENTARY IMMUNIZATION ACTIVITIES (JE SIA) IN BALI ISLAND - 2018 Department of Public Health and ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

COVERAGE EVALUATION OF
JAPANESE ENCEPHALITIS
SUPPLEMENTARY IMMUNIZATION
ACTIVITIES (JE SIA) IN BALI ISLAND
2018
Department of Public Health and Preventive
[DocumentMedicine
subtitle]
Faculty of Medicine Universitas Udayana
[Document subtitle]
1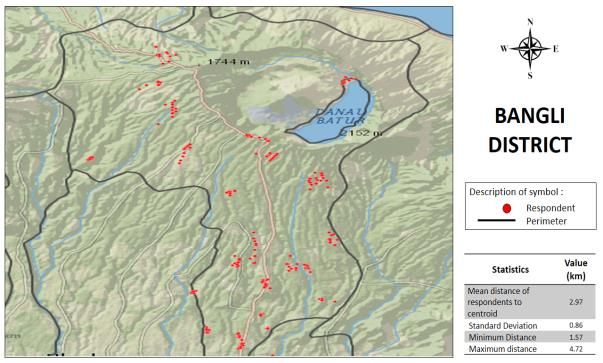
PREFACE
Japanese encephalitis is prevalent in Bali province, therefore attaches high priority on prevention effort
through immunization. In 2018 the Japanese encephalitis immunization campaign was conducted in Bali
and has reached the coverage of 101% among the estimated total eligible children aged 9 months to 15
years old. The population-based survey is needed to provide more accurate feature of the JE
immunization coverage and related attributes.
Result of the JE immunization campaign survey are useful for the evaluation of the achievements of the
immunization campaign and serve as basis for developing the plan for management of JE and JE
immunization in the future.
I would like to express my deepest gratitude to Bali Province Health Office and District Health Office for
their field assistance during the survey, WHO Indonesia for preparation and funding for the survey, for
the Universitas Udayana team to execute the preparation, field survey and finalizing the report, and for
the WHO Headquarter and WHO Regional Office for providing technical assistance of the data analysis.
2ii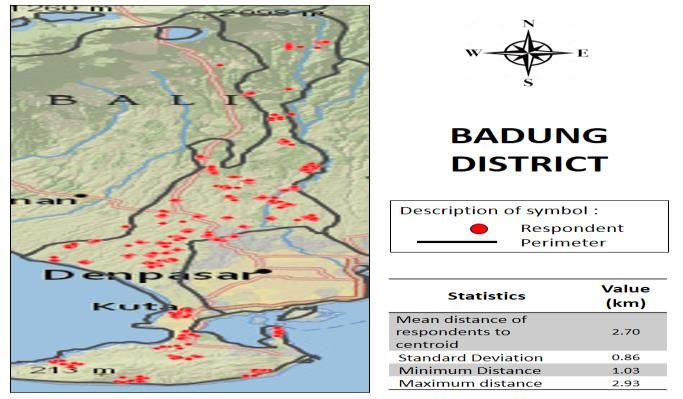
COVERAGE EVALUATION OF JAPANESE ENCEPHALITIS
SUPPLEMENTARY IMMUNIZATION ACTIVITIES (JE SIA)
IN BALI ISLAND
2018
AUTHORS:
dr. Anak Agung Sagung Sawitri, MPH (Project Coordinator)
dr. Putu Cintya Denny Yuliyatni, MPH (Principal Researcher)
dr. I Made Dwi Ariawan, S.Ked (Researcher)
dr. Komang Ayu Kartika Sari, MPH (Researcher)
Department of Public Health and Preventive Medicine Faculty of Medicine, Universitas Udayana
iii
3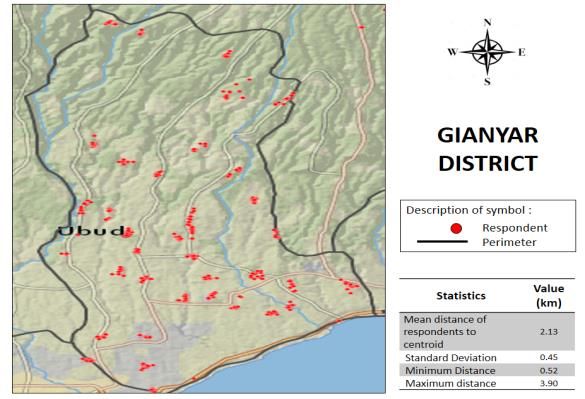
ACKNOWLEDGEMENT
WHO Indonesia
Dr. Vinod Kumar Bura, Haditya L. Mukri, Sidik Utoro
Faculty of Medicine Universitas Udayana
Dr. dr. I Ketut Suyasa, Sp.B, Sp.OT (K) (Dean Faculty of Medicine), Dr. dr. I Dewa Made Sukrama,
M.Si., Sp.MK (K) (Vice Dean I), Dr. dr. Anak Agung Wiradewi Lestari, Sp.PK (Vice Dean II)
Bali Province Health Office
dr. Gede Wira Sunetra, MPPM (Disease Prevention and Control Officer), dr I Gusti Ayu Raka
Susanti (Vaccination Program Section Chief)
District Health Office
I Nengah Suarma Putra, ST,M.Kes (Tabanan DHO), I Ketut Gita (Denpasar DHO), Drg. Komang
Sri Ria Astiti (Gianyar DHO), I Nyoman Sunika (Jembrana DHO), I Putu Arnaya (Klungkung DHO),
Agung Alit Naya (Badung DHO), Ni Wayan Eka Wartini (Bangli DHO), Ni Nyoman Artini
(Karangasem DHO), Ni Nyoman Mertiasa, SKM (Buleleng DHO)
All staff of Public Health Center in Bali Province for their assistance and support; Head of Village
and Kelian Banjar (Head of Sub-district) of selected cluster for their support and permission to
conduct the survey; and our field survey team: Study Coordinator, Assistant Study Coordinator
and Enumerator for their hard work and active contribution to successfully complete the survey
activity.
iv
4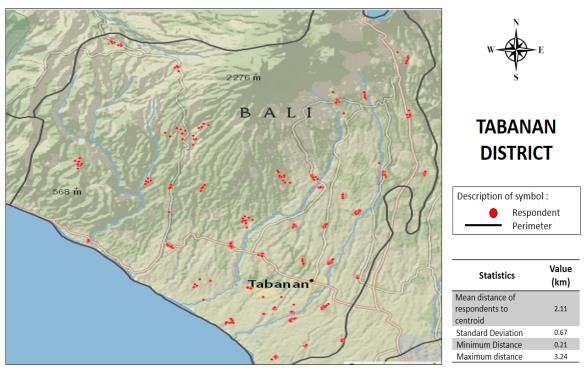
EXECUTIVE SUMMARY
Bali province has reported the most frequent positive cases of Japanese Encephalitis (JE)
through the JE sentinel surveillance. The JE Immunization Campaign (JEIC) represents the first
campaign in Bali and in Indonesia as a whole. The JEIC targets all children (from 9 months to
95% vaccination coverage. The JEIC survey aims to measure the estimation coverage
at the provincial and district level.
A cross-sectional survey was conducted from June to August 2018; the sample population was
households in Bali. Sample selection was performed randomly in two stages. The first stage
selected clusters of sub-villages (Banjar) (n=441), and the second stage selected households in
each cluster (n=13). These clusters were distributed proportionally based on the number of
target children in each district.
The focus was to gather data on the demographics of respondents and children, immunization
status by recall and validation, knowledge and beliefs about JE and JE immunization, sources of
information, types of services, procedures and adverse events, and general satisfaction level
with the JE immunization service. The data were collected using an electronic questionnaire
(Epi-collect version 5). Validation of JE immunization status refers to WHO guidelines, which
require the collection of three aspects including the child’s name, date of immunization, and
immunization record: Valid immunization was only confirmed if all three aspects were fulfilled.
Trained interviewers qualified to a minimum level of Diploma of Health conducted the data
collection. Study coordinators qualified to a minimal level of Bachelor of Health supervised the
interviewers. Data collection was conducted on a case-by-case basis in each district because
the preparation of household listings in each district was simultaneously carried out alongside
data collection. Immunization data validation was also conducted on the completion of the
household surveys in each district, and the study coordinator and research team examined the
data for completeness according to the WHO guidelines (mentioned above).
Data collection began in July 2018 and ended on 25 August 2018. Data management and
analysis were conducted simultaneously at the completion of data collection for each district.
In total, 5630 households were visited, of which 2193 household had eligible children. This
resulted in a total of 3331 children to undergo analysis. The validation process in the health
centers was successfully conducted in 6 of the 9 districts due to the technical constraints related
to validation at the outset of the survey. Weighting was applied to the sampling design and
response rate at the district level and post-stratification was applied at the province level. The
following findings were derived from the weighted data.
The key findings of JE immunization coverage were as follows:
Coverage of JE immunization by recall in Bali province was 93.58%, with the highest
coverage found in Bangli (98.78%) and the lowest coverage in Jembrana (88.66%). From
the 9 districts surveyed, 6 have achieved the target of 95% immunization coverage.
Valid JE immunization coverage in Bali is based on 6 districts that passed validation;
including Tabanan, Gianyar, Denpasar, Badung, Klungkung, and Karangasem. Overall,
5v
valid JE immunization coverage in Bali was 73.88%, with the highest coverage in
Klungkung (92.15%) and the lowest in Denpasar (58.13%).
Alternate calculation of valid JE immunization coverage based only on valid records as
denominators found higher coverage; ranging from 76.55% to 96.26% across Bali. The
highest coverage by district was found in Klungkung and Badung, and the lowest
coverage was found in Denpasar and Tabanan.
The gap in the coverage rate by recall and validation was mainly due to inadequacies in
the recording, filling, and reporting system. To some extent, those situations added
difficulties to validate the immunization status. This may have also been due to a
shortage of human resources during the JE immunization campaign.
The key findings on the implementation of JE immunization were as follows:
Providers had made efforts to screen children’s health status before immunization,
however, some of these efforts were not in accordance with the technical guidelines
(e.g. mainly the use of the screening form, the monitoring and the length of monitoring
after immunization at the health post and at home). The immunization injection was
mainly given in the right arm as per the guidelines, although a proportion received the
injection in the left arm.
At the district level, the screening process (i.e. asking for and providing screening forms)
tends to be higher in Gianyar, Badung, and Denpasar. The proportions of injection in
the left arm were balanced among the districts. In addition, follow-up monitoring was
poorly conducted, as only half the samples were included.
Health providers stated that they were overwhelmed during the JE Immunization
campaign and felt that the ratio of available health providers to the number of children
to be immunized was less than ideal.
The proportion of children suffering adverse reactions to immunization was 4.73% in
Bali overall, with fever and local reaction the most frequently reported complaints.
Respondents in Tabanan reported the highest level of adverse reactions (12.8%) and
Karangasem the lowest (2.0%).
Key findings of knowledge and beliefs were as follows:
Knowledge level of respondents in Bali were low (5.17), with the highest score found in
Denpasar (5.96) and Badung (6.02), and the lowest score was at Jembrana (3.55).
Source of information related to JE and JE immunization in Bali province were mainly
from three sources included television, health staff and sub-village cadres. School
children and teacher were contributed at fair proportion. There was different trend of
source of information among districts.
In Bali province, beliefs on susceptibility relatively low, however beliefs on severity was
high particularly belief that JE may resulted death and disability. Beliefs on benefit of JE
immunization were high, while barrier was seen on adverse event of JE immunization
but not to health providers. There was different trend of beliefs in district level.
The key findings on knowledge and beliefs were as follows:
The knowledge level of respondents in Bali overall is low. From a maximum of 10 points
(signifying the highest level of knowledge about JE immunization), the overall score for
vi
6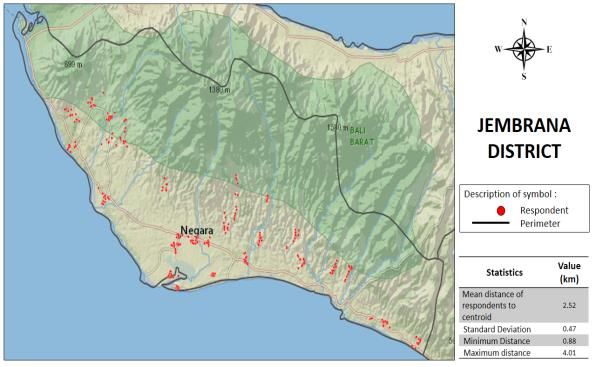
Bali was 5.18. By district, the highest knowledge-level scores were found in Badung
(6.03) and Denpasar (5.96), and the lowest in Jembrana (3.55).
Information on JE and JE immunization in Bali came from three main sources: television
campaigns, health staff, and sub-village cadres. Further, school children and teachers
(who had been educated about JE) also represented sources of information. Further,
the sources of information differed among the districts sampled.
In Bali as a whole, beliefs on an individual’s susceptibility to JE are relatively low;
however, beliefs on JE’s severity are high; particularly the belief that JE may result in
death and disability. The majority of respondents believe that JE immunization is highly
efficacious, while adverse reactions to JE immunization do represent a barrier to
immunization; these concerns are rarely voiced to health providers. However, at the
district level, a different trend of beliefs was evident. For example, participant’s beliefs
about susceptibility to JE were less varied, with the highest scores in Denpasar. Beliefs
about the severity of JE in terms of its potential to cause death and disability were also
higher in Denpasar and Badung districts. In terms of respondent’s beliefs about the
importance of JE vaccination, that JE immunization is efficacious in preventing JE and
level of trust in health providers conducting JE vaccinations only those in Badung scored
poorly while the majority believes.
vii
7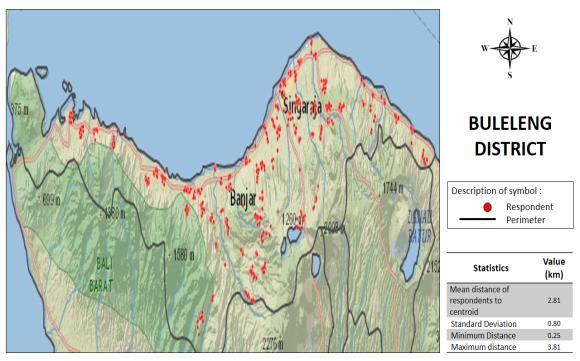
TABLE OF CONTENT
Page
COVER ………………………………………………………………………………………………………………………..….. i
PREFACE ……………………………………………………………………………………………………………………….... ii
AUTHORS ………………………………………………………………………………………………………………………. iii
ACKNOWLEDMENT ………………………………………………………………………………………………………… iv
EXECUTIVE SUMMARY ………………………………………………………………………………………………….. v
TABLE OF CONTENT ……………………………………………………………………………..………………………... viii
LIST OF FIGURES ……………………………………………………………………………………………………..……… x
LIST OF TABLES ………………………………………………………………………………………………..…………….. xi
LIST OF ANNEXES ……………………………………………………………………………………………..……………. xii
1. INTRODUCTION ………………………………………………………………………………………..……………. 1
1.1 Situation Analysis ………………………………………………………………………………..…………… 1
1.2 Demographics and Population ……………………………………………………………..…………. 2
1.3 JE Immunization Campaign Program ………………………………………………………..……… 3
1.4 Objectives of the Survey ………………………………………………………………………..………… 3
1.5 Benefits of the Survey …………………………………………………………………………………….. 4
1.6 Organization of the Survey ………………………………………………………………….…………. 4
1.7 Design, Population and Sampling …………………………………………………………………….. 4
1.7.1 Design …………………………………………………………………………………………………….. 4
1.7.2 Population and Sampling ……………………………………………………….……………….. 5
1.8 Variables and Definition of Coverage of JEIC …………………………………………………. 7
1.9 Questionnaire Development and Pretest, Training and Field Survey ………..……….. 8
1.9.1 Questionnaire Development and Pretest ……………………………………..……….. 8
1.9.2 Training ………………………………………………………………………………………………….. 8
1.9.3 Field Survey …………………………………………………………………………………………… 8
1.10 Data Management ………………………………………………………………………………………….. 10
1.11 Response Rate & Weighting ……………………………………………………………………………. 11
2. SOCIO-DEMOGRAPHICS …………………………………………………………………………………………. 13
2.1 Socio-Demographics Characteristics of Respondents …………………………………….. 13
viii
8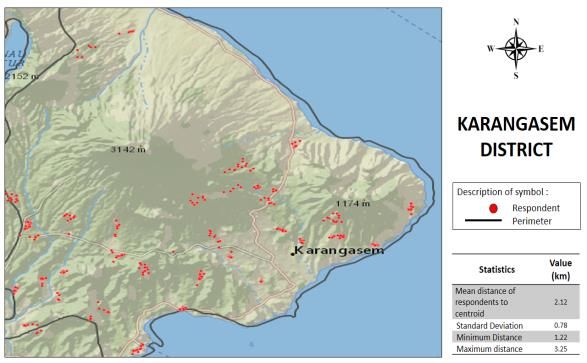
2.2 Socio-Demographics Characteristics of Children ……………………………………………. 16
3. COVERAGE OF JE IMMUNIZATION CAMPAIGN ……………………………………………………… 18
3.1 Coverage of JEIC …………………………………………………………………………………………….. 18
3.1.1 Coverage by Recall ………………………………………………………………………………… 18
3.1.2 Coverage by Validation …………………………………………………………………………. 18
3.2 Qualitative Result Related to Coverage ………………………………………………………….. 22
3.2.1 Determining Target for Immunization …………………………………………………….. 22
3.2.2 Logistics and Resources ………………………………………………………………………….. 22
3.2.3 Collaboration and Coordination AmongStakeholders …………….……………….. 22
3.2.4 Acceptance of the JEIC in the Community ……………………………………………… 23
3.2.5 Recording and Reporting ………………………………………………………………………… 23
3.2.6 Dissemination of Information About JEIC ……………………………………………….. 23
4. PROCEDURE OF JE IMMUNIZATION CAMPAIGN ……………….……………………………………. 25
4.1 Result from Quantitative Survey …………………………………………………………………….. 25
4.1.1 Procedure ……………………………………………………………………………………………… 25
4.1.2 Adverse Events Following JE Immunization (Quantitative Result) ……………. 28
4.2 Result from Qualitative Survey …………….…………………………………………………………. 28
4.2.1 Arrangement of Schedule for JEIC ……….…………………………………………………. 28
4.2.2 Screening of Eligibility for JE Immunization ……………………………………………. 28
4.2.3 Implementation for JE Immunization ………………………………………………………..29
4.2.4 Adverse Events Following JE Immunization (Qualitative Result) ………………..29
5. KNOWLEDGE & BELIEFS OF JE AND THE JE IMMUNIZATION ………………………………….. 31
5.1 Level of Knowledge ……………………………………………………………………………………….. 31
5.2 Source of Information of JE and JE Immunization …………………………………………… 33
5.3 Perception or Beliefs to JE Infection and JE Immunization ……………………………… 35
6. COVERAGE OF BASIC IMMUNIZATION ……………………………………………………………………. 38
REFERENCE ……………………………………………………………………………………………………………………… 40
ANNEXES
ix9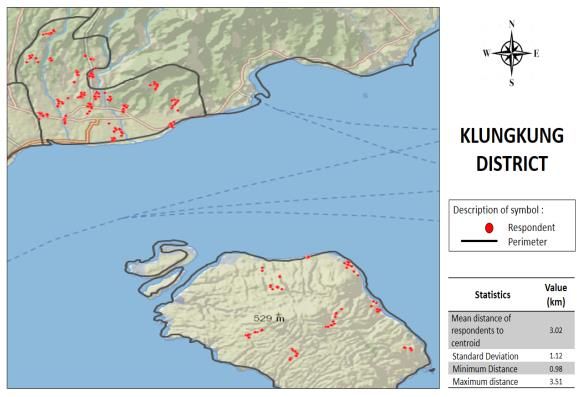
LIST OF FIGURES
Page
FIGURE 1 Distribution of Selected Clusters in Bali ………………………………….………………. 6
FIGURE 2 Knowledge Level of JE and JE Immunization per District in Bali ……………… 31
FIGURE 3 Source of Information ……………………………………………………………………………. 33
FIGURE 4 Percentage of Respondents Who Believe in JE Infection and JE
Immunization ……………………………………………………………………………………….. 35
x
10LIST OF TABLES
Page
TABLE 1 Attributes to Calculate Coverage …………………………………………….…………… 7
TABLE 2 Validation Activities in Public Health Centers (PHCs) per District in Bali 10
TABLE 3 Characteristic of Survey Clusters …………………………………………………………. 11
TABLE 4 Characteristic of Surveyed Households and Subjects ……………..………….. 12
TABLE 5 Socio-Demographic Characteristics of Survey Respondents in Bali ………. 14
TABLE 6 Socio-Demographic Characteristics of Survey Respondents per District in
Bali ....................................................................................................... 15
TABLE 7 Demographic Characteristics of Children in Bali ……………….………………….. 16
TABLE 8 Demographic Characteristics of Children per District in Bali ………………….. 17
TABLE 9 Unweighted and Weighted Recall/Crude Coverage in Bali ……………….…… 19
TABLE 10 Unweighted and Weighted Valid Coverage in Bali ……………………………….. 20
TABLE 11 Validation Status ………………………………………………………………………………….. 21
TABLE 12 Procedure of JE Immunization in Bali ………………………………………………….. 25
TABLE 13 Procedure of Immunization per District in Bali ……………………………………. 27
TABLE 14 Side Effects Following JE Immunization in Bali …………………………………….. 28
TABLE 15 Proportion of Correct Answers of Knowledge Items of JE and JE
Immunization per District in Bali …………………………………………..……………… 32
TABLE 16 Source of JE Information per District in Bali ………………………………………… 34
TABLE 17 Beliefs to JE Infection and JE Immunization per District ………………………. 37
TABLE 18 Coverage of Basic Immunization in Bali ……………………………………………….. 38
TABLE 19 Coverage of Basic Immunization per District in Bali …………………………….. 39
xi
11LIST OF ANNEXES
ANNEX 1 Target Population
ANNEX 2 Sample Size Calculation
ANNEX 3 Systematic Random Sampling Technique for Cluster and Household Selection
ANNEX 4 Distribution Number of Cluster
ANNEX 5 Map Distribution of Selected Clusters of JE Immunization Campaign Survey in
Each District in Bali Province 2018
ANNEX 6 List of Key Informants of Qualitative Survey
ANNEX 7 List of Variable and Variable Definition
ANNEX 8 List of Person Involved in the Survey
ANNEX 9 Informed Consent and Quantitative Survey Questionnaire
ANNEX 10 Informed Consent and Qualitative Survey Questionnaire
ANNEX 11 Value of Weight for Sampling Design and Response Rate & Post-Stratification
Weight
xii
121 INTRODUCTION
1.1 SITUATION ANALYSIS
JAPANESE ENCEPHALITIS (JE) is an infection caused by an arthropod-borne virus that targets the
central nervous system. JE is considered a mosquito-borne viral disease, with Culex
tritaeniorhynchus as the major transmitter. Pigs, large mammals, and swamp birds act as
amplifying hosts, and the disease cycle ends in humans. JE is endemic across the whole of Asia,
particularly in East Asia (Japan and Korea), South Asia (India and Sri Lanka), Southeast Asia
(including Indonesia), and Australia. JE can be fatal, especially among children under 15.
Generally, among children with JE, 40-50% will suffer permanent disability, and it will prove
fatal for 20-30% (Kemenkes RI, 2013).
The Ministry of Health’s (MOH) Health Research and Development Agency (Badan Penelitian
dan Pengembangan Kesehatan Kementerian Kesehatan/HRDA-MOH), Directorate of
Prevention and Disease Control (Ditjen P2PL) and NAMRU 2, successfully isolated the JE virus
in mosquitos in 1972 (and in pigs, birds, cows, buffalos, horses, and goats in 1975) in several
areas in Indonesia (Jakarta, West Java, Central Java, West Nusa Tenggara, West Kalimantan,
South Sumatera and Sulawesi). In response, the MOH developed the JE Sentinel Surveillance
System in 1981, particularly targeting high-risk areas for JE transmission. This sentinel
surveillance found 25.4% of confirmed JE cases from the total number of specimens gathered
(Kemenkes RI, 2013). Further, research and surveillance from 2001-2005 covered all districts in
Bali in a collaborative study carried out by Sanglah Central Hospital and the Korean
International Cooperation Agency (KOICA). This study found that among 239 children with
clinical JE, 86 (36%) were suffering from confirmed cases of JE; 4 (2%) were probable; and 149
(62%) were not suffering from JE (Kari, Liu, Gautama, et al., 2006).
Some Asian countries carry out routine surveillance-based JE control programs. Malaysia has
conducted routine surveillance for JE and Acute Encephalitis Syndrome (AES) since 1989 using
an annual reporting system. Another, 14 Asian countries (including China, North Korea, and Sri
Lanka) conduct routine vaccinations and monthly surveillance programmes (Kemenkes RI,
2013). In Indonesia, previous control efforts and surveillance were limited to non-routine
sentinel surveillance and depended on the availability of funding support. However, the
authorities have since realized that the control of JE is a priority because Indonesia is an
endemic JE area.
Initial efforts began with the support of the MOH to establish JE sentinel surveillance in Bali in
2013 as a pilot project for Indonesia. Bali was chosen because it has a high JE incidence and a
pre-existing JE surveillance system in place. The most recent report on JE incidence in Bali in
2008 was 7.2 sufferers per 100.000 people per annum (Dinkes Provinsi Bali, 2014). JE and AES
sentinel surveillance in Bali remain ongoing: 23 public and private hospitals represent JE
1sentinels led by the Provincial Health Office. The most up-to-date data from Indonesia’s AES
National Sentinel Surveillance in 11 provinces reported 326 AES cases in 2016, of which 43
(13%) cases were confirmed as JE. The most frequent cases of JE (17; 39.5%) were reported in
Bali.
The JE immunization campaign (JEIC) represents the introduction of the JE immunization into
Indonesia’s national immunization program. Despite having the most frequent cases of JE (as
well as having a JE surveillance system already in place), Bali has strategic value as an
international tourism destination. The JE catch-up campaign involves implementing an
immunization program among the target population in the shortest time possible. The results
of the JE catch-up campaign is expected to form the basis of a strategic plan in other JE-endemic
areas of Indonesia (Kemenkes RI, 2017).
Bali Provincial and District Health Offices set up the JEIC in 2017 and have been preparing for
its technical implementation. The program is reported to be running well, and as planned. At
the JEIC’s completion, JE immunization coverage had exceeded the estimated number of target
children (101%). However, coverage was based on an estimated number of children; this may
have been subject to bias due to initial overestimation of the number of children immunized.
However, while the JEIC’s high level of coverage should achieve a good level of protection for
the community, if this assumption is incorrect it will provide a false sense of security against JE
infection. Universitas Udayana is a government health partner and assigned to the JEIC Bali
Province Task Force’s monitoring and evaluation division. Universitas Udayana provides
scientific assistance in evaluating immunization coverage and the factors that may be related
to the JEIC’s coverage.
1.2 DEMOGRAPHICS AND POPULATION
Bali consists of nine districts, namely Tabanan, Gianyar, Badung, Klungkung, Bangli,
Karangasem, Jembrana, Buleleng and Denpasar. Geographically, Bali is composed of one main
island (Bali), and four smaller islands: Nusa Penida, Nusa Lembongan, and Nusa Ceningan in the
southeast, and Menjangan Island in the northwest.
According to the 2010 census, Bali’s population was 3.89 million, with approximately 1 million
under 15. In the same year, an estimated 1.8 million people (48.3 % of the population) lived in
urban areas, and more than 83.46 % were Hindu.
Population migration rates from other districts in Bali are relatively high. This is driven by the
rapid urbanization of Denpasar, Badung and Gianyar in the southern part of Bali (the three most
developed districts and the center of government and tourism). In addition, the numbers of
migrants from neighboring regions such as Java and Nusa Tenggara increase from year to year.
Bali has two unique social characteristics relevant to this paper:
21) The Banjar (sub-village council) system represents the smallest unit of local governance
(below the village level). Bali has two kinds of Banjar: Banjar Adat and Banjar Dinas.
Banjar Adat are more concerned with traditional ceremonial matters (i.e. religious
ceremonies at the temple, marriages, and funerals) while Banjar Dinas represent the
formal local-government level responsible for administration and civil registration
matters.
2) Bali’s religious and traditional ceremonies are very frequent and may last for days, weeks
or even months. The Balinese calendar indicates auspicious dates for particular
ceremonies to be held. May-July 2018 (when this survey was conducted) was considered
a good period for these ceremonies, with two districts (Gianyar and Bangli) holding a
Ngaben Massal (traditional Balinese mass funeral ceremony) involving a full month’s
schedule of ceremonies.
1.3 JE IMMUNIZATION CAMPAIGN PROGRAM
In general, Bali’s JEIC aims to control the transmission of JE; and in particular, decrease AES-
and JE-related morbidity. The JEIC’s target population is children aged >9 months to 9 months to1.5 BENEFITS OF THE SURVEY
1. The findings will be used for planning and/or implementing future JEIC (or other
immunization programs) both in Bali and at the national level.
2. The survey will provide a learning resource so that students can experience how a
well-planned field survey should be carried out.
3. The findings will be used for teaching and scientific purposes such as seminar material
and written publications.
1.6 ORGANIZATION OF THE SURVEY
The JEIC survey was carried out by the Department of Public Health and Preventive
Medicine at the Faculty of Medicine, Universitas Udayana. Funding was provided by the
World Health Organization Country Office Indonesia. The WHO Country Office Indonesia,
WHO Headquarters, and the WHO Regional Office provided technical assistance in the
design and analysis of the survey data.
A survey steering committee was established consisting of the Provincial and District
Health Office and Universitas Udayana representatives. The technical team consisted of
members of the same organizations, as well as the Department of Public Health and the
Preventive Medicine Faculty of Medicine at Universitas Udayana. The technical team from
the DHOs supported the discussion and decision-making on technical issues relating to the
survey implementation.
The survey was supported by field coordinators, most of whom were postgraduate Masters
Students and current Masters Students on the Masters Study Program in Public Health at
Universitas Udayana. More than half of the enumerators were students and alumni of the
Bachelors Study Program in Medicine, the Bachelors Study Program in Public Health, and
the Masters Study Program in Public Health. Most have worked on similar surveys before,
and more than half have been involved in data collection for national health surveys such
as RISKESDAS.
1.7 DESIGN, POPULATION AND SAMPLING
1.7.1 Design
A quantitative survey was created to follow the WHO’s manual for Immunization Coverage
Surveys (2015), and then adjusted to follow the WHO’s Vaccination Coverage Cluster Survey
reference manual (2018). In addition, a qualitative survey was conducted to gather data on
respondent’s perceived obstacles to JEIC.
To measure the immunization coverage, evidence was collected from vaccination cards and
immunization registers at health facilities, as well as from vaccination history as recalled by the
4child’s caretakers. This involved two main activities: 1) surveying the child’s recalled
immunization history, and 2) validation of this recalled immunization history (as defined in the
next sub-section).
1.7.2 Population and Sampling
1.7.2.1 Sample Size Calculation
The target population for the JEIC survey is children in Bali aged >9 months to 4.72
kilometres (Fig.1). Two areas are uninhabited: a particularly hilly area on the border of
Jembrana and Buleleng (West Bali National Park) and the Mount Agung area in northeast
Karangasem. The distribution of samples in Denpasar district was denser than other districts. A
detailed breakdown of cluster distribution per district is available in Annex 5.
5Figure 1. Distribution of Selected Clusters in Bali
The lists of the selected 13 households were prepared by the research team and shared to the
study coordinators (SC), who then distributed the 13-item lists to the assigned enumerator.
Before data collection, the enumerators made phone calls to the respective village heads to
confirm that the 13 selected households were, in fact, registered as living in the selected
cluster(s). SCs were allowed to substitute the chosen households with the higher or lower
ranked households on the list if the household head was not resident in a particular Banjar or
had died, one day preceding the data collection at the latest. Substitution and re-combination
of clusters were also permitted due to inaccurate cluster data and/or changes in sub-village
status. In general, 13 households in each cluster were successfully visited. However, some
clusters had less than 13 households, including Denpasar (6 clusters; 6.9%), Badung (1; 1.6%),
Bangli (1; 3.3%), and Buleleng (6.6%). This occurred mainly because the selected household
could not be found during data collection.
All eligible children in the selected households were sampled. One re-visit was applied to
households that were known to have eligible children but could not be interviewed on the first
visit. Households were eligible for inclusion in the survey if the following conditions were met:
Having children 9-59 months of age and children 5-15 years old, at the time the JE
immunization campaign was carried out (March-April 2018); and
Having a knowledgeable mother or caretaker who was willing to be interviewed, evidenced
by written consent from the respondents.
The qualitative survey involved 20 key informants (Annex 6) and qualitative observations during
the survey enrollment. This assessment looked at perceived obstacles to the JE immunization
campaign, focusing on resource-based factors (e.g. logistics, target population numbers,
timelines, staffing, support from stakeholders and providers, norms and/or cultural
6considerations) and immunization-process factors. All key informants at the province and
district level will be interviewed, however, key informants at the sub-village level were
purposively selected based on consideration of their location (i.e. urban or rural areas) and
school characteristics (Kindergarten, Elementary School, Junior High School; government or
private schools; rural or urban schools).
1.8 VARIABLES AND DEFINITION OF COVERAGE OF JEIC
This survey provided socio-demographic data about caretakers (age, sex, education,
occupation, parity) and their children (age, sex, education, birth rank) and data on their
immunization status by recall and validation. Data relating to respondent’s knowledge,
source(s) of JE information, type of services, procedures, perceptions of JE and JE
immunization, overall satisfaction with the service, and adverse reactions related to the JEIC
were collected. A detailed definition of the main variables is presented in Annex 7.
Table 1. Attributes to Calculate Coverage
Recall Coverage (RC) Valid Coverage (VC)
Valid Immunization status from recall Valid immunization (a) defined if the name, date,
Immunization was considered as “not valid” and mark were available in a written JE
status immunization document
Invalid immunization (b) defined if:
a) The child’s name exists on the written JE
immunization document but is otherwise
incomplete (i.e. three criteria are unmet)
Immunization status cannot be validated (c) if:
a) The child’s name could not be found on
any JE immunization registers
b) The SC could confirm validation of JE
immunization status
Numerator Number of children who Number of children who fulfilled the criteria for
caretakers recalled as having valid immunization
been immunized with the JE
vaccine
Denominator Total number of eligible 1. Total number of eligible children participating
children participating = a + b + c + unimmunized children
2. Number of children a, b, and unimmunized
3. Number of children a and unimmunized
Type of Crude and weighted Crude and weighted
numbers
Coverage of JE immunization was measured in two ways: (i) recall from knowledgeable
caretakers, and (ii) by the validation of written documents such as immunization cards and/or
immunization registers. The written immunization documentation had to meet three criteria
7to show that the children had indeed been immunized: (i) the child’s name, (ii) the date of
immunization, and (iii) a mark confirming immunization (such as a ticked box or circle). If these
three criteria were met (on the child’s immunization card or on the register), a valid JE
immunization was recorded. The table 1 presents the methods used to determine the children’s
immunization status in this survey.
1.9 QUESTIONNAIRE DEVELOPMENT AND PRETEST, TRAINING AND FIELD SURVEY
1.9.1 Questionnaire Development and Pretest
The research team was responsible for questionnaire development. The development of
questions for knowledge, perceptions, procedures, and adverse reactions were based on the
MOH’s technical guidelines for JEIC (Petunjuk Teknis Kampanye Imunisasi Japanese Encephalitis
(JE) Kemenkes RI, 2017) and on discussion with the technical team from the PHO and DHOs
(Denpasar, 22 June 2018). First, questionnaires were created on paper; this draft was then
transferred to an electronic version using Epicollect 5. The resultant questionnaire was then
tested on three caretakers for substantive content and flow, and the results were compiled into
Epicollect.
Prior to the data collection, the electronic questionnaires were pretested with 10 caretakers to
ensure the questions were clear, easily understandable, and the results could be recorded
properly in the system. In the light of this pretesting, new questions were added and changes
were made to improve the survey.
1.9.2 Training
A total of 6 study coordinators were involved from an early stage: at the study team’ technical
meeting, in the pretesting, and in the questionnaire revision process. SCs were introduced to
the JEIC recording and the reporting system to ensure they understood the survey method and
the validation process for JE immunization status. SCs were also involved in training the
interviewers and facilitating the interviewer-respondent discussions.
A total of 34 respondents (males n = 9; females n = 25) participated in the survey training for
the interviewers. The training took place over two days: 28-29 June 2018 in Denpasar. The
training included class presentations from the PHO technical team and Universitas Udayana
representatives, and mock interviews with interviewers and ‘respondents’ in small groups. All
participants were trained on using the Epi-collect questionnaires and assigned to interview
three parents at home on the first day and report the interview results on the following day.
The second day focused on data management reporting; from Epi-collect to the data manager.
1.9.3 Field Survey
1.9.3.1 JEIC Survey
The JEIC survey employed six teams to collect the data: each team was lead by one study
coordinator, and comprised of five to six interviewers. Fieldwork took place from 2 June- 25
August 2018, although it was extended from the planned date to July 30, 2018.
8The field survey was extended due to the prolonged time required to prepare the sampling
frame and obtain written permission to carry out the data collection. Formal permission (in
writing) for fieldwork was obtained from the Bali Province One-Stop Investment and Integrated
Services Office (Dinas Penanaman Modal dan Pelayanan Terpadu Satu Pintu Provinsi Bali) on 4
June 2018 and was sent to the District Investment Services and One Stop Services office in the
same week. However, most of the District Offices responded after the extended Ramadhan
holiday. In addition, permission letters also had to be sent from the Sub-districts Office to the
heads of villages, and finally, to the heads of the sub-villages (Banjar).
Enumerators were encouraged to contact the head of the sub-village at least two to three days
before visiting the Banjar. During data collection, the head of sub-villages or cadres in the sub-
villages accompanied most enumerators. This assisted the enumerators in finding the target
households more easily, lessened the possibility of refusal by participants, and also eased the
clarification of eligible children’s availability in the selected households.
Prior to the first data collection, all team members attended a technical meeting to strengthen
interviewer’s preparedness. In addition, two evaluation meetings with all team members were
set up for the first and second districts to correct any errors and solve any problems that arose
during the interviews. Meetings were held every evening to follow up on the day’s activities
and prepare for the next day's interviews because the preparation of the sampling frame and
the data collection had to run simultaneously over a short time.
A list of those involved in the survey implementation is provided in Annex 8. The survey
questionnaires and informed consent forms are provided in Annexes 9 and 10.
1.9.3.2 Validation Process
In general, the six study coordinators carried out the validations. However, due to the limited
time available and difficulties in the validating process, eight enumerators were trained to assist
in the validation process at health centers. Unfortunately, the field data collection ran on longer
than expected which resulted in the validation process becoming delayed. It was not possible
to carry out validation at the same time as the survey because the validation process involved
several complex tasks including finding the name of the child on the register or other source
documents, confirming immunization status validity, and documenting the evidence for each
child. In addition, a child’s domicile was sometimes different from the place of immunization.
This was particularly evident among school children, and especially in Denpasar, Badung, and
Gianyar, where many children went to school outside their local area. The validation process
also took longer because only hardcopy records (i.e. on paper) were available and these
featured huge variations in type and recording technique, unstructured filing, as well as being
bulky and voluminous, particularly in health centers that served a lot of target children. Also, in
Denpasar and Badung, children were allowed to be immunized by a pediatrician in a private
clinic or hospital, thus increasing the difficulty in validating their records, even though in
Denpasar, these records are collected by the PHC or DHO. Validation visits often required more
than one visit to a PHC. This became worse when dealing with less-than-cooperative health
staff at some PHCs. In light of these constraints, it is possible that on occasion, the validation
9team may not have been able to find a child who had been recorded on the register or
validation may have been subject to error.
A total of 77 (64.2%) public health centers were sampled across six districts in Bali. SCs visited
all PHCs a total of 128 times; however, completing the validation process per PHC, took an
average of 3.3 days. At the end of the timeline, six of the nine districts were validated, including
Tabanan, Gianyar, Denpasar, Badung, Klungkung, and Karangasem. In terms of register quality,
the average score for all provinces was fair (7/10), however, it was noted that the lowest
individual score for register quality was still very low (2.5/10). This also occurred in terms of
health center staff’s cooperativeness, where, in general, the average score was quite good
(7.5/10), however, the lowest individual score was just 2/10. Health centre staff’s
cooperativeness was important for the successful validation of immunizations because they are
able to explain and clarify any unclear immunization cases; particularly if the registers were not
well kept. Valid immunization coverage at the province level is represented by six districts.
Table 2 presents the validation data across these 6 districts.
Table 2. Validation Activities in the Public Health Centers (PHCs) per District in Bali
Number of visits Average (days) Average score of Cooperativeness of
Districts for validation per validation per register health staff
PHC child (score 1-10) (score 1-10)
min- min- min- min-
Average Average Average Average
max max max max
Province 1.6 1-4 3.3 1-7 7.0 2.5-10 7.6 2-10
Tabanan 2.16 1-3 4 1-5 7.13 4-9 7.47 4-10
Gianyar 1.62 1-3 3.69 2-7 7.36 4-10 7.6 4-10
Denpasar 1.82 1-3 3.91 3.5 7.43 4-10 7.3 2-10
Badung 1.77 1-4 3.38 2-6 6.36 3-9.3 8.05 6-9.25
Klungkung 1.11 1-2 2.33 1-3 7.5 6-9 7.56 5-9
Karangasem 1.08 1-2 2 1-3 6.65 2.5-9 7.54 2.5-9
* Average number of visits to complete validation in one PHC was calculated by the study coordinator. This number was
summed and divided by the total number of participating PHCs in each district
** Average (days) validation per child was calculated by the study coordinator by estimating the total number of days to
complete validation per PHC
*** Completeness and cooperativeness were scored by the study coordinator who visited the PHCs, scores range from 1 =
very poor and 10 = very good. The scores for each PHC were summed and divided by the number of participating PHCs
to obtain an average score for each district
1.10 DATA MANAGEMENT
Completed Epi-collect questionnaires were uploaded to the Epi-collect server and backed up
regularly. The paper control forms were returned to the researcher for checking and then
passed to the data manager for data processing. The questionnaires employed coded, closed-
ended questions and the Epi-system had been set up to minimize missing data. The data
manager carried out the data processing, and the data were returned to the researcher in the
10form of Excel files. The research team examined the data, crosschecked it with the researcher,
and cleaned it before analysis. The Excel data was then imported to STATA and analyzed using
STATA version 12.
In terms of data analysis, a local statistician, WHO Indonesia, WHO Headquarters Geneva, and
the WHO Regional Office were consulted on several occasions. To decrease bias due to
sampling design and non-response, the data were weighted at the district-level analysis, and
post-stratification weighting was applied in data analysis at the provincial level (Annex 11).
1.11 RESPONSE RATE & WEIGHTING
The JEIC survey was designed to produce estimates at the district and province levels. Table 3
summarizes characteristics of the clusters in the JEIC survey. In general, 7 of the 9 districts were
successfully sampled for the household survey. However, in one district (comprised of 4
selected sub-villages), one village head refused our request for a list of households while in
another district, one cluster could not be visited due to a prolonged religious ceremony.
Substitution of these clusters was not possible because of the time-consuming nature of
arranging permission (as detailed above). In general, the percentage of clusters with eligible
subjects was high, apart from those in Denpasar.
Table 3. Characteristics of Survey Clusters
Description of Selected Cluster
Total Total
Districts Cluster with eligible
Clusters Villages Planned Surveyed
subjects
F F % F %
Bali province 4,450 667 441 436 98.9 431 98.8
Tabanan 792 130 40 40 100.0 40 100.0
Gianyar 565 70 40 40 100.0 40 100.0
Denpasar 442 43 91 87 95.6* 85 97.7
Badung 553 52 62 62 100.0 61 98.4
Klungkung 285 55 30 30 100.0 29 96.7
Karangasem 570 65 47 46 97.9** 46 100.0
Bangli 353 63 30 30 100.0 30 100.0
Buleleng 620 138 71 71 100.0 71 100.0
Jembrana 270 51 30 30 100.0 29 96.7
For individual interviews, participation rates varied among districts. From a total of 5,733
households targeted for sampling, 5,630 (98.2%) households were actually visited, of which,
2,290 (40.67%) of households were eligible for inclusion. Of these households, 2,075 (94.62%)
were successfully interviewed, where 118 (5.6%) refused to participate, and 97 (4.67%) were
re-visited and found no to be at home or were not re-visited. The main reason people cited for
not participating was being busy (>60%), and particularly with religious ceremonies. It is
noteworthy to mention that the surveys accidentally [G1] coincided with auspicious days for
traditional/religious ceremonies across the whole of Bali. Households that could not be
identified for the existence of eligible children were considered as missing. This yielded a
11You can also read

















































