Dementia Strategy 2018 2020 - Health in Wales
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Dementia Strategy 2018 - 2020

Table of Contents
1.0 Introductory Statement and Strategic Aim ........................................................ 3
2.0 What is dementia? ............................................................................................ 4
2.1 Service demand ............................................................................................ 5
3.0 Our approach ................................................................................................... 6
4.0 What people wanted us to know ....................................................................... 6
5.0 A shared vision ................................................................................................. 8
6.0 Shared priorities ............................................................................................... 9
Priority 1 .................................................................................................................. 9
Priority 2 .................................................................................................................. 9
Priority 3 ................................................................................................................ 10
Priority 4 ................................................................................................................ 11
Priority 5 ................................................................................................................ 11
Priority 6 ................................................................................................................ 11
7.0 Making this happen ........................................................................................ 13
8.0 How will we know if the strategy is making a difference? ............................... 13
9.0 Summary ........................................................................................................ 16
Appendix I - List of contributions and consultations ................................................. 17
Appendix II - Pledges Made ..................................................................................... 18
Appendix III - Key Performance Indicators ............................................................... 19
2
Version 1.03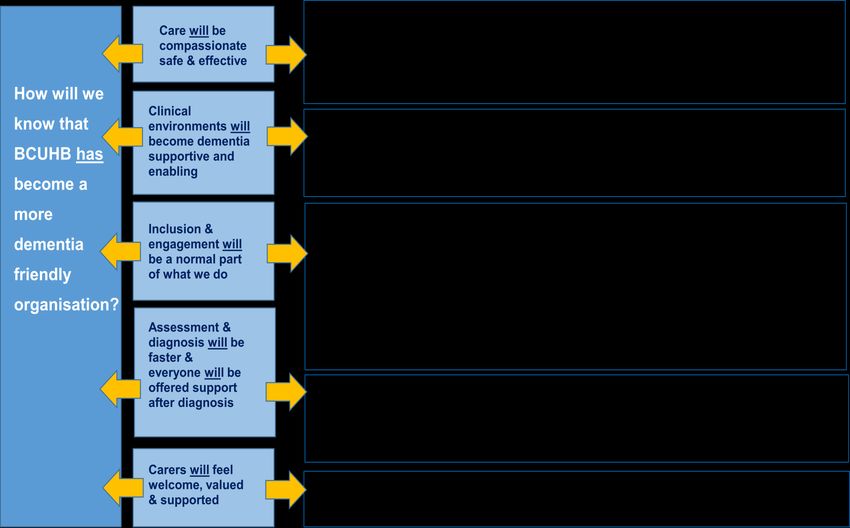
DementiaStrategy forBetsi Cadwaladr University Health Board 2018
- 2020
1.0 Introductory Statement and Strategic Aim
Every aspect of Betsi Cadwaladr University Health Board (BCUHB), encompassing
Primary, Community Secondary and Mental Health Care, is committed to the
delivery of high quality, person-centred care to people identified or assessed as
having known or suspected dementia and those affected by it.
While the BCUHB Dementia Strategy has taken account of the proposals for the
National Plan this has only recently been published. We will therefore continue to
work with our partners to review and refresh it and will revise it to take account of the
National Plan.
The BCUHB Dementia Strategy reflects the Dementia Strategic Action Plan for
Wales1 by;
Supporting a local emphasis for the commitment to creating ‘dementia
supportive communities’ within our organisation
Respecting the voice of people affected by dementia
Consulting and listening to the people who access our services
Ensuring services available are accessible and responsive to the needs of the
community we serve
Ensuring that people with dementia are included in activities and their carers
supported
The BCUHB Dementia Strategy is based upon best practice and national guidance.
It also complements the BCUHB Quality Improvement Strategy in its objective to
provide services which are safe, effective and caring.
The Health Board acknowledges that prevention of Dementia is an important
consideration and risk reduction and health promotion and recent evidence shows
that there are steps that people can take across their life course to reduce their risk
of developing dementia, to delay onset or slow deterioration following diagnosis.
The lifestyle steps focus on remaining active (physically and socially), checking your
health regularly, trying new things, not smoking, only drinking alcohol within the
recommended guidelines and maintaining a healthy weight.
With the implementation of the actions identified within this document, BCUHBaims
to improve the experience of all people living with dementia who access health
services. We will do this by recognising and acknowledging the universalrights of
those affectedand making dementia care safe, compassionate and based on best
evidence. The strategy also intends to facilitate the greater inclusion of individuals,
1 Currently in draft
3
Version 1.03families and carers, in the shaping of the care that we provide. It is recognised that it
is the responsibility of every member of health board staff to promote the principles
in this document to facilitate and deliver the highest standard of care.
This strategy has been informed by a number of individuals, organisations and
professionals (Appendix I) who have the experience and expertise to advise and
guide the Health Board as it makes meaningful change. This includes people living
with dementia their relatives and carers as we recognise that they are most affected
by dementia.
2.0 What is dementia?
The term ‘dementia’ describes a set of physical illnesses affecting the brain and its
functioning. Whilst there are many types of dementia the most common is
Alzheimer’s disease followed closely by the vascular dementias, together these
account for around 80 – 90% of all dementias. Dementia presents as a collection of
common signs and symptoms which affect much more than just memory2.
The person may have difficulty with thinking, with judgement, with concentration, with
communication, with being as independent as he or she wishes and may experience
problems with hearing or vision. Whilst these changes are often small to start with
they will increasingly make life difficult for that person and their journey will
progressthrough mild, moderate and severe stages. In the moderate stage those
affected require most support as the daily challenges increase and previous ways of
coping become less effective.
Some of those challenges are related to damage to the brain itself and the type of
dementia a person has is mostly related to which parts of the brain have been
affected. However, to truly understand dementia it must be acknowledged that this is
but one aspect as each person diagnosed with dementia is as unique as each reader
of this document and each person’s personality, biography, health, spirituality and
social networks are important in understanding how they are affected by dementia.
Younger people (those below the age of 65 years), at the point of diagnosis, are
more likely to: still be in work; have dependent children; have significant financial
commitments; and may well be caring for older parents or relatives. The illnesses
themselves can present differently and the rarer types of dementia may be more
common in younger people. In addition to the same signs and symptoms of older
people diagnosed with dementia, younger people are more likely to have problems
with mobility and balance, with speech and language and with making sense of
vision.
Whilst the word ‘dementia’ is often heard it is not yet fully understood by all. Often as
a consequence of misunderstanding or lack of awareness people who have
dementia find themselves stigmatised, discriminated against or disadvantaged in
some way. Through this strategy and the priorities set out later we aim to increase
awareness, reduce stigma, include people with dementia and empower our staff to
2 Older People’s Commissioner for Wales. 2015. Dementia: more than just memory loss.
4
Version 1.03play their part in supporting the places where they live to become dementia friendly
communities.
2.1 Service demand
Currently there are almost 11,000 people in North Wales who are living with
dementia or varying age. This one in fifteen people over the age of 65 years will
have a diagnosis of dementia. As the age of the general population increases the
numbers of those affected by dementia will also increase throughout the first part of
this century and, by 2031, it is anticipated that there will be almost sixteen thousand.
This change will not be evenly distributed as shown in Chart 1.
Chart 1
New cases of dementia in North Wales 2014 to 2031
3000
2500
2000
1500
1000
500
0
2014-21 2021-26 2026-31
Wrexham/Flintshire Conwy/Denbighsire Gwynedd/Anglesey N. Wales
During the period this strategy covers the number of predicted new cases of
dementia will be around 7% which is equivalent to another 781 people. However by
2031 that increases to 18% or 5,240 more people affected by dementia than there
were in 2016.
Regardless of population change and increased demand BCUHB recognises that it
cannot allow universal rights to go unidentified and that we have a statutory duty to
ensure that health care needs do not go unmet. This, aligned with the anticipated
sharp increase in diagnosis, further emphasises the pace required to deliver the
5
Version 1.03improvements now by changing culture, systems and processes. It is also
acknowledged that BCUHB needs to work in partnership with others to best meet the
total needs of anyone living with or affected by dementia.
3.0 Our approach
It has been highlighted3 that the experience of dementia care has not always been
good and isoften one of contrasts and inconsistencies. In developing this strategy
we have reflected on users stories of real experiences, both positive and negative, to
help inform our priorities. A clear message that the strategy should be ‘real and
demonstrably measurable’ was heard. As a result this strategy is a living document
that is supported by a framework for meaningful improvement.
This strategy has been written in partnership with our Dementia Ambassador and
informed by a wide group of stakeholders. That has enabled us to get the tone and
language right because these things are important for people affected by dementia.
We have followed appropriate guidelines on the language used to describe dementia
and those affected by it4.
We recognise that the voices of those living with dementia and in particular their
families have often not been heard. BCUHB as an organisation has had to learn, not
only to listen, but to truly hear what people have said. Everything we have heard
throughout this consultation has been valued and considered in producing this
strategy.
In moving forward against our objectives we recognise that we must be transparent
and visible to those who use our services, and to our staff. This strategy includesan
assurance mechanism for improvement to be planned, monitored and reported
annually across the next two years. Importantly a number of pledges are made for all
age groups and these are shown at Appendix II. The progress against key
measures will be monitored via our internal governance processes.
4.0 What people wanted us to know
We wanted to know what was important, what matters to people and what we
needed to change. What we were told has been captured in the words of our
dementia strategy ambassador amongst others.
Chris Roberts – Dementia Ambassador
By making small changes we can make a big difference. I’d like you to think about
the changes that you can make to be more dementia friendly. Together we can
create places where people like me are understood, accepted and where we can feel
3 ‘One Simple Thing’ improving NHS Services for people living with dementia. The Board of
Community Health Councils 2017
4
Dementia words matter - DEEP (Dementia Engagement and Empowerment Project) and the
Dementia Action Alliance 2014
6
Version 1.03involved and supported. A place where we feel like we are enabled and empowered
to make decisions about our lives, where we are included, involved and given choice
and control over our day to day life”.
We agree with that and we see hospitals and other spaces where health care is
provided as being those places. They are not built by bricks and mortar alone but are
founded upon our beliefs, attitudes and values. We aim through this strategy to
emphasise the importance of such things and ask all our staff to look to the changes
they can make to become more dementia aware and friendly.
Teresa Davies – living with dementia
“I try to live as much of a full life as I can but it is hard and often people don’t see me
as a person, sometimes treat me like I am not there”.
We do not want people living with and affected by dementia to feel like this. Our
strategy will help people to feel more visibility, to find they have voices that are heard
and to be regarded as people who are valued and supported.
Emyr Williams, son, carer and community mental health nurse BCUHB, Conwy
"I became a carer for my mother following the sudden death of my father. I found
myself attempting to cope with a full time job, my own personal grief and a new
unexpected and challenging role as a carer. I never applied for the role, and its
associated responsibilities, and consequently felt very inadequate and under
qualified to carry out all the duties involved”.
Another carer commented
“When a diagnosis is given, it is given to the whole family. We all became carers. Me
and our children (our youngest was fourteen).
We strongly believe that carers and families must be supported to understand what
dementia is and how individuals may be affected by it. To facilitate this ambition
carers will need to have access to sensitive and timely signposting towards the
support that is most effective and meaningful for them. There is a real opportunity for
mutual learning and we acknowledge that very often carers are in the best position to
inform staff about the uniqueness of the person receiving care. This helps clinical
staff to better understand how the individuals needs can be best met. To enable this
the carer must be fully included and consulted about the care that is provided 5.
A daughter comments on attending the emergency department
5
Unless the person with dementia retains mental capacity and does not wish this to be the case.
7
Version 1.03“When we arrived at the hospital mum was not only in pain but was becoming very
anxious. There were lots of people waiting to be seen and we ended up being stuck
there for more than four hours. Mum was frustrated and started singing and
shouting. Other people were looking at her and some were sniggering”.
We understand that places like the emergency departments can be really difficult for
many people to attend but it is worse for those who are affected by dementia.
Through this strategy we will be acting to ensure that the emotional and
psychological needs of people with dementia are given as much priority as the
physical health problem that has brought them into hospital. We will introduce a ‘fast-
track ’dementia friendly triage, initiate better ways to support people whilst they are
in those departments and work to get as many people as possible back to their
homes as soon as we are able.
A Welsh speaking Carer says
“My husband prefers to speak in his first language. Being able to communicate with
others in your own language whilst you are in hospital is so important. We are lucky
that we have nurses who can speak Welsh and this has really benefitted the quality
of care my husband has received”.
We are proud to be part of a bi-lingual nation. We know from our own audit work how
much people affected by dementia value being able to receive health care and
consultations through their preferred language and how disadvantaged they feel
when this is not possible. We are committed to providing services bilingually and
acknowledge that some groups have even greater need to receive services in their
first language. BCUHB recognises the importance of actively offering services in
Welsh 6 as an integral element of care. This ensures that we maintain professional
and statutory standards whilst fully responding to the language needs of individuals.
5.0 A shared vision
BCUHB works to a set of shared values that alongside this strategy will support its
ambition in becoming a ‘dementia friendly organisation’7. Over the nextthree years
BCUHB will continue to work towards changing systems and processesto enhance
and support improved dementia care.
We see the future as one in which those who are diagnosed with dementia, who
support them, can feel confident that not only will they experience compassionate,
safe and professional care but that they have, as a right, real opportunities to shape
and be more involved in that care. It is a future which will be based not just on
partnerships but on respect for human rights, protection by law, transparency and
engagement.
6
Office of the Welsh Language Commissioner.
7
As recognised through the Alzheimer’s Society dementia friendly organisations programme
8
Version 1.036.0 Shared priorities
Figure 1. Our shared priorities
Priority 1– Safeguarding vulnerable people in our care
The Health Boards Director of Nursing & Midwifery has executive responsibility for
Safeguarding. As a dementia friendly health care organisation we will safeguard
vulnerable people in our care. Safe care is one of the cornerstone values in our
Quality Improvement Strategy and must be reflected through the attitudes, values,
behaviour and practice of all BCUHB staff who have contact with people affected by
dementia. To assure this we will be committed to safeguarding people from harm
and to improve the well-being of patients by empowering staff to act and work
collaboratively to achieve the best outcomes for individuals. We will protect people
from harm related to unnecessary medical intervention or prescribing. The use of
anti-psychotic medications will be managed through prescribing guidelines that
promote the involvement of the family in decision making and, we will promote
prudent health care particularly to prevent unnecessary distress. We will look
towards how the concept of the ‘wrap around’ team8 can be introduced to help
people receive more care at home as an alternative to hospital admission.
Priority 2– Deliver safe, effective and compassionate care
Effective care is a strand of our Quality Improvement Strategy and the BCUHB
approach to dementia (Figure 2 below) has been based on recognised best practice
8
National Dementia Action Plan for Wales 2018
9
Version 1.03and National guidelines. The approach applies to all health care settings and will
ensure the delivery of person centred care throughout all levels of the organisation.
Learn more
Deliver safe Know the about
Welcome and dementia and
effective and person
include families apply your
compassionate as well as
and carers learning
care to all the patient
Think pain,
anxiety or Think about
Think about Think
infection as your care
your Safeguarding
the cause of environment
communication and Act
behaviour
change
Figure 2. The BCUHB approach to Dementia
We will support our clinical staff to incorporate the principles into their individual
everyday practice, by ensuring that awareness training becomes a fundamental part
of induction, with higher levels of training for relevant staff.
To enable this, the Health Board will underpin the model with the necessary training
and education resources. All dementia training will be opened up to carers and
families of those affected and increasingly we will see this group leading the training
and education of staff as they bring their experience to share with others. Those in
leadership positions in relevant wards and clinical teams will incorporate this model
into supervision and identify local champions who actively engage within a dementia
community of practice.
Priority 3– Carers will feel welcomed, valued and supported
People diagnosed with dementia are at the heart of this strategy but we must never
forget the contribution made by carers. There are countless numbers of wives,
husbands, partners, sons, daughters, friends and neighbours who give of their time
and health to support people through the challenges that dementia brings.
10
Version 1.03This Dementia Strategy is clear that we have a priority to ensure that carers are
respected and made welcome in any health care setting. To ensure that in our
hospitals we fully endorse ‘John’s Campaign’ and will have this in place on every
ward. We believe that right from the start carers must be fully involved and consulted
about the care that is to be provided. To help support this we will work with the third
sector to identify and overcome barriers to inclusion and, we will better utilise the
good work already undertaken by our service user experience team to bring together
carers and create networks. The training currently offered will be built upon and
carers will have an opportunity to inform, input and participate as appropriate into the
programme. We will maintain the independent advocacy available and seek ways to
build upon that.
Priority 4– Inclusion and engagement around dementia care will be
a natural part of what we all do
Our most important stakeholders are the people that we as an organisation exist to
serve. We will establish an external reference group to both advise on our progress
and enable our services to improve responsively. We will ensure that we address
issues of rurality and that a Welsh language offer is available.
We will launch our dementia feedback tooolkit that will involve carers as early as
possible and will set out the full range of ways in which we can give a stronger voice
to everyone affected by dementia.We will work across organisational boundaries by
collaborating more closely with partner agencies.
Priority 5– All healthcare environments will be dementia supportive
and enabling
We will commit to ensuring all refurbishment and new build projects across the
health board meet the 2016 National standards outlining what a dementia supportive
and enabling environment looks like. We will develop a ‘best environment ward’
template to demonstrate our future ambitions.
Additionally we will ensure that our services work in the way recommended by the
‘Well Organised Workspace” programme. This is an approach to simplify the
workplace and reduce waste by having everything in the right place, at the right time,
ready to go and through this enable provision of safer care for our patients.
Priority 6– There will be timely access to assessment for dementia
and once the diagnosis has been made there will be meaningful
support
Waiting for the assessment process to start can be a difficult and anxious time. We
will act to significantly improve upon the six week target set by the Memory Services
National Accreditation Programme. This means that we will offer meaningful
assessment to be commenced within 28 days of the referral being received.
11
Version 1.03Due to clinical complexity it can take longer for an accurate diagnosis of dementia to
be made. When this happens we commit to clearly communicating with the person
who is being assessed with an opportunity given to fully discuss this.
Whilst across North Wales a standard offer of support after diagnosis is welcome we
also recognise the value of peer support and facilitate this. This willmean individuals
and families can meet with others who have been or are living the same experience.
Additionally we will ensure that evidence based psychological interventions are more
accessible. This will include training a number of staff to deliver these where
appropriate and will incorporate Cognitive Stimulation Therapy and making ‘Coping
with Caring and Loss’ groups available to carers from across the Health Board.
In particular we will work with those affected by a young onset dementia to determine
the improvements in services that are required to better support, enable and
empower this group in an age appropriate and meaningful way.
12
Version 1.037.0 Making this happen
People we have engaged with have told us what is important to them and have also
stated that given the impact of dementia on every part of a person’s life, this strategy
must have a broad purpose and a far reach for BCUHB to become a more ‘dementia
friendly organisation’. The driver diagram (see Figure 3) sets out the areas of work
we will address in the three years of this Dementia Strategy to achieve that.
8.0 How will we know if the strategy is making a
difference?
Supporting the strategy will be a comprehensive improvement plan and progress will
be monitored via the BCUHB quality governance framework. This will include
definable measures of success through which we can assess and openly share our
progress. Throughout each year we will be discussing progress with our external
reference group, with the North Wales Community Health Council and, with the
Alzheimer’s Society in Wales as our aspirations towards becoming a more dementia
friendly organisation are monitored. For the wider population we will publish an
annual progress report, with opportunities throughout to evaluate the impact of the
implementation and ask stakeholders; ‘How are we doing?‘Appendix III provides
performance indicators through which we will also be able to assess our progress
13
Version 1.03Figure 3.Making this happen – driver diagram
• Specialist practitioners for safeguarding in dementia and learning disabilities
Safeguarding • Training will be more accessible to staff, this will include best practice,
will be at the Deprivation of Liberty and the Mental Health Act.
heart of what we • Championing the approach that safeguarding is everyone’s business.
do • Sharing good practice and safeguarding learning across the organisation.
• Valuing equality and diversity through person centred approaches to care.
BCUHB will Launch the BCUHB model for dementia care and the delirium improvement
measure.
become a Prevent clinically unnecessary moves between wards.
Care will be Align dementia training to the All Wales ‘Good Works’ framework ; train all
more compassionate, staff to better understand dementia and involve those affected by dementia in
safe & effective training.
dementia Develop robust audit programme for dementia care.
Assure dignified end of life care.
friendly Promote zero tolerance on language that negatively positions those affected
by dementia.
organisation
• Go beyond the principles of John’s Campaign and embed the values in all of
Carers will feel our services. .
welcome, valued
• Include the carer in all discussions about care and treatment.
& supported
• Incorporate National quality standards about carer expectations into the
delivery of care across BCUHB
14
Version 1.03• Inclusion and engagement will be a fundamental strand of how we implement this strategy
Inclusion & • Establish an external expert reference group comprised of people living with dementia to
engagement
will be a advise and evaluate on strategy progress.
normal part of • Work jointly with others to better understand issues related to rurality and dementia.
what we do • Ensure the Welsh language active offer is prominent in dementia care
• Seek to connect with minority and seldom heard groups to better understand and address
unmet need
BCUHB will • Introduce a BCUHB dementia feedback toolkit and involve carers as early as possible in
all episodes of care
become a • Work with external organisations to seek opinion on service development and wherever
possible to jointly provide services.
more Clinical
environments
dementia • Apply National policy standards to new build and refurbishment projects and undertake
will become
dementia assessment of all clinical environments to identify variance to standard.
friendly supportive and
enabling
organisation
• Introduce an effective model for mental health liaison services
• Develop the dementia pathway from primary care through to secondary care
Assessment &
diagnosis will • Memory Services to commence substantive assessment within 28 days of referral.
be faster & • Implement new processes to ensure fast tracking through Emergency and Out-Patient
everyone will
be offered departments
support after • Engage with and commission appropriate third sector organisations to introduce peer
diagnosis
support after diagnosis and introduce the ‘coping with caring and loss’ intervention for
carers.
• Effectively communicate (verbally and in writing) with the person concerned and their carer
the diagnosis that is made.
15
Version 1.039.0 Summary
‘Nothing about us without all of us’
Facing the challenges that dementia brings is hard enough without feeling that those
who offer care do not fully understand the experience or engage enough. To respect
that the whole of BCUHB as an organisation will work together toward the common
goal of becoming a more dementia friendly organisation that provides safe, effective
and compassionate care in a fully inclusive way.
This Dementia Strategy has outlined the BCUHB aims to improve the experience of
health care for people living with and affected by dementia in North Wales. In order
to do this, there has been consultation and engagement with a large number of
people whose lives are affected in some way by the presence of dementia. BCUHB
aims to become a more ‘dementia friendly organisation’ and will achieve that by
acting to deliver care that is safe, effective and compassionate. A number of pledges
to support delivery of this strategy have been made with a commitment that BCUHB
will publish an annual report on progress alongside an incremental plan for
improvement.
CONFIDE NTIAL D RAFT
16
Version 1.03Appendix I - List of contributions and consultations
Alzheimer’s Society Cymru
Tawel Fan Families Group
Flintshire Local Authority
North Wales Community Health Council
North Wales Adult Social Service Heads
‘Men in sheds’ – Llanrwst
Conwy Community Big Voice Project
Anglesey Community Big Voice Project
TIDE – ‘Together in Dementia Everyday’ – represented by Ruth Eley, Director, The
Life Story Network
DEEP – Dementia Engagement and Empowerment Project – represented by Chris
Roberts
North Wales Hospices – represented by Iain Mitchell, CEO St. Kentigern’s Hospice
School of Health Care Sciences, Bangor University
CONFIDE NTIAL D RAFT
John’s Campaign – represented by Julia Jones, co-founder of John’s Campaign
People living with or affected by dementia attending ‘Dementia Education and
Inclusion Meet-up Event’ 24th to 25th November 2015, Llandudno
People living with or affected by dementia attending ‘Dementia Education and
Inclusion Meet-up Event’ 22nd to 23rdNovember 2016, Llandudno
People living with or affected by young onset dementia attending ‘Mental Health
Summit’ 13th January 2017, Llandudno
Head of Psychology Services, BCUHB
17
Version 1.03Appendix II - Pledges Made
CONFIDE NTIAL D RAFT
18
Version 1.03Appendix III - Key Performance Indicators
CONFIDE NTIAL D RAFT
19
Version 1.03CONFIDE NTIAL D RAFT
20
Version 1.03You can also read