HARRY WINKLER Director, section of Endourology Kidney stone center - Dept.of Urology - Med
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Alpha blockers have no
role in renal colic
HARRY WINKLER
Director, section of Endourology
Kidney stone center
Dept.of Urology
‘Sheba’ Medical Center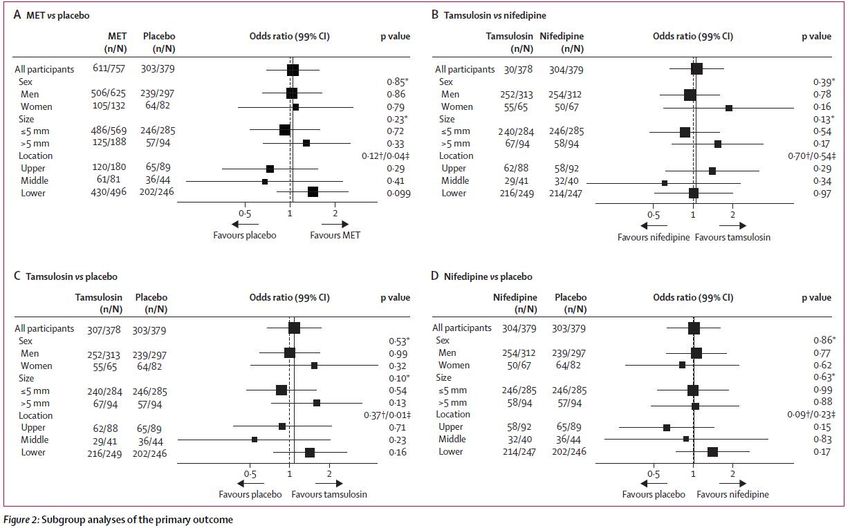
Financial and Other Disclosures
Off-label use of drugs, devices, or other agents: None
including our local regulatory agency
Data from IRB-approved human research is not presented
I have the following financial interests or
Disclosure code
relationships to disclose:
No financial relationships N
2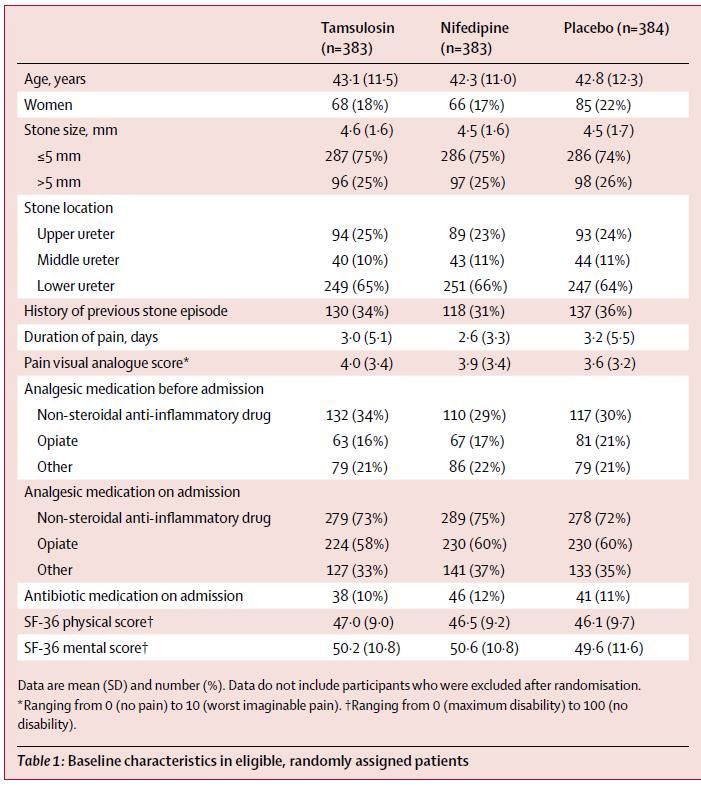
Tamsulosin, which is a selective α1A/α1D-adrenergic
receptor antagonist, has been widely studied in the
context of MET for patients with distal ureteric
stones smaller than 10 mm.
It has been proved that tamsulosin increases stone
expulsion rates, decreases pain, reduces mean time to
stone expulsion and decreases analgesic usage when
compared with placebo
Can J Urol 2010; 17:5178–83
Urology 2010;75: 4–7
MEDICAL EXPULSIVE THERAPY ( met ) HAS BECOME AN ESTABLISHED METHOD OF TREATMENT.
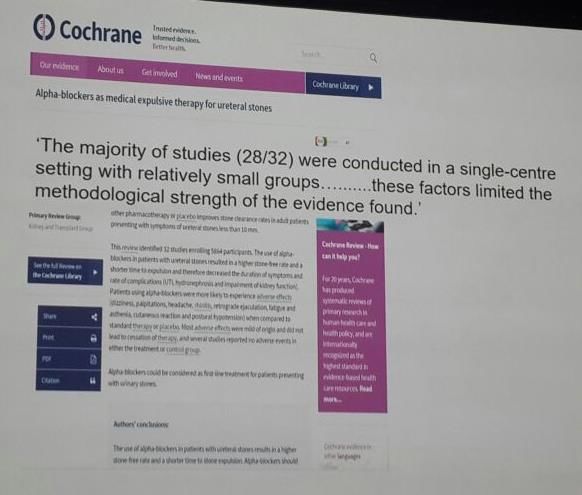
Thirty-two studies (5864 participants). The stone-free rates were significantly higher in the alpha-blocker group (RR 1.48, 95% CI 1.33 to 1.64) when compared to standard therapy. Stone expulsion time was 2.91 days shorter with the use of alpha blockers (MD -2.91, 95% CI -4.00 to -1.81).
2014 Cochrane - Study limitations Included many heterogeneous trials Most studies have a relatively small number of patients, performed in a single-centre, with variable methodological quality. In ONLY 7/32 studies patients and doctors were both blinded. Two studies described incomplete data Proximal and mid-ureteral stones were assessed in only three studies ( 3/32 ) A large-scale, placebo-controlled (multicenter RCT may be needed to draw final conclusions concerning the role of alpha-blockers in all ureteral stones.
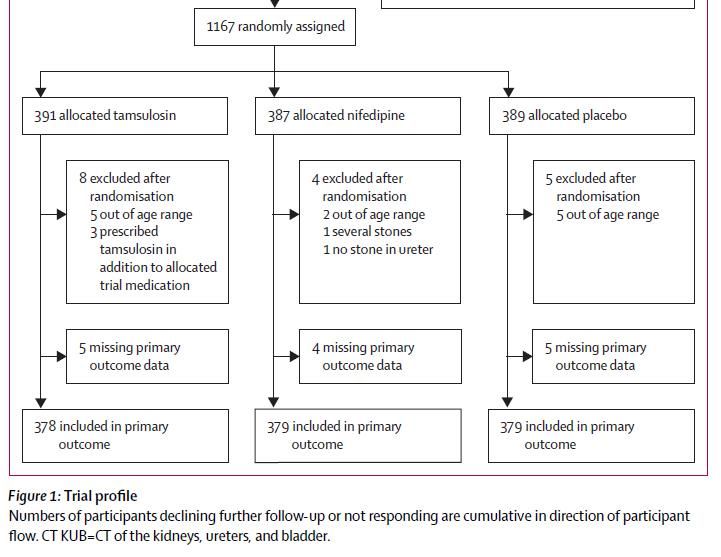
24 centers in the UK Lancet 2015; 386: 341–49 1167 participants
Medical Expulsive Therapy for Ureteral Stones:
No Better Than Placebo
bruce soloway, reviewing Pickard R et al. Lancet 2015 May 18
Researchers in the U.K. enrolled 1136 symptomatic adults,
each with a single ureteral stoneComment :( LANCET)
This trial, designed to reflect current recommendations
and clinical practice
Definitively demonstrates the ineffectiveness of
medical expulsive therapy for ureteral stones
Reaffirms the essential importance of large, well-
designed, randomized trials for assessing clinical
interventions and formulating treatment guidelines
Bruce Soloway, NEJM journal watch“…This may change future guidance on MET”…
Efficacy and Safety of Tamsulosin in Medical Expulsive Therapy for Distal Ureteral Stones with Renal Colic: A Multicenter, Randomized, Double-blind, Placebo-controlled Trial Zhangqun Ye et al. Eur Urol 73 ( 2018 ) 385– 391
The primary end point was the stone expulsion rate, defined as stone expulsion, confirmed by negative findings on CT, over the 28-d
tamsulosin significantly facilitates the passage of distal ureteral stones and relieves renal colic. Tamsulosin provides a superior expulsion rate for stones >5 mm, but does not show any difference from placebo for stones ≤5 mm.
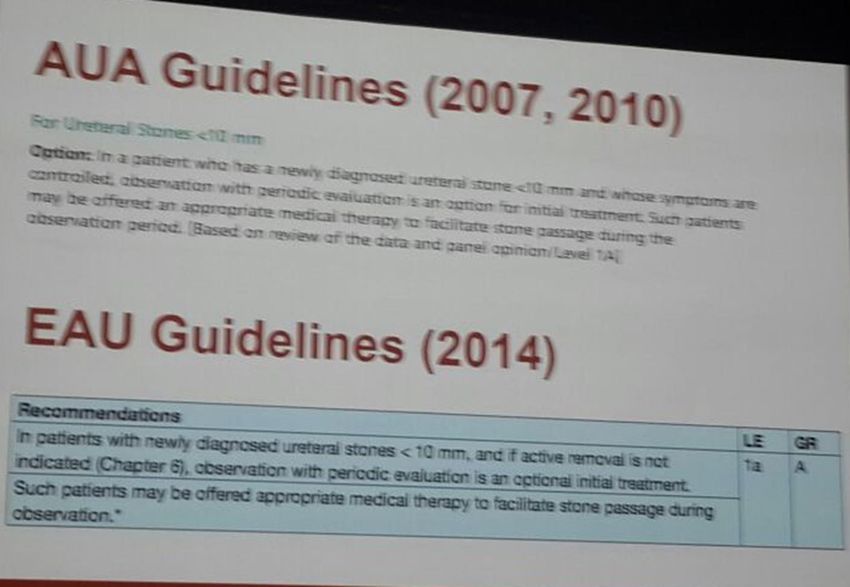
Contemporary Management of Stone Disease:
The New EAU Urolithiasis Guidelines
Matthew Bultitude et al. EUR UROL, 6 9 ( 2 0 1 6 ) 4 8 3 – 4 8
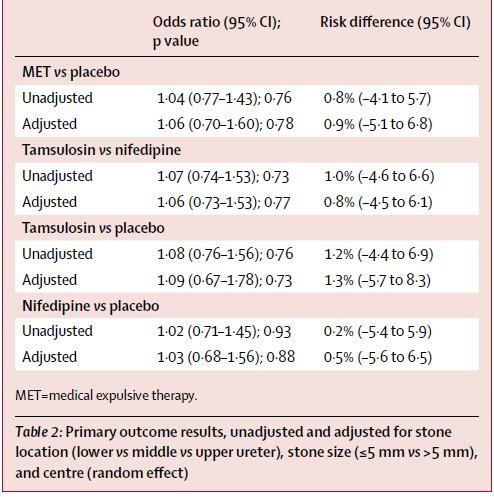
A randomised multicentre placebo-controlled trial of 1167 pts.
“this is a single trial, it had more patients
than the meta analysis data, and significant
weight needs to be given to this paper when
deciding whether to continue to offer MET
for ureteric stones”.
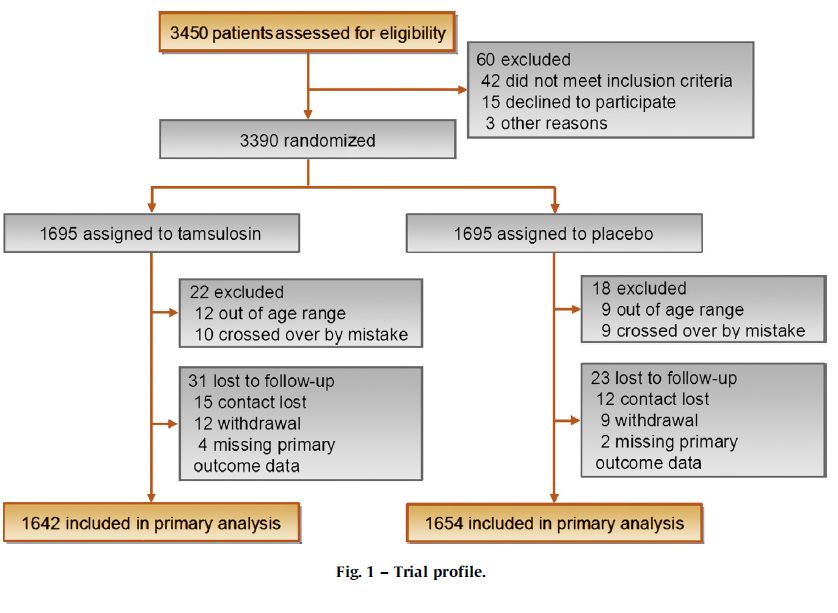
Pickard R, et al. Lancet 2015;386:341–9Effect of Tamsulosin on Passage of Symptomatic Ureteral Stones : A Randomized Clinical Trial Andrew C. Meltzer , JAMA Internal Medicine , June 18, 2018. a multicenter, randomized, double-blind, placebo controlled clinical trial among emergency department patients The Study of Tamsulosin for Urolithiasis in the Emergency Department (STONE)
Phase 1 : 2008 to 2009 ------109 pts. single site Phase 2 : 2013 to 2016 at 6 emergency department---------403 pts. Total – 512 pts. Symptomatic ureteral stones determined by NCCT Size < 9 mm in diameter Follow-up CT scan after the 28-day treatment period The primary outcome : passage of stone within 28 days after randomization, as determined by the participant’s visualization or physical capture of the stone
Use of medical expulsive therapy in ED - 15% to 55%. Ganesan V, J Urol. .196:1467-1470;2016 Our findings agree with those of 2 recent large multi site clinical trials conducted in the United kingdom Pickard R, Lancet. 2015;386(9991):341-349.(SUSPEND) theAustralian study, 403 patientswith distal ureteral stones 10 mm or less in diameter were enrolled in 5 emergency departments and randomized to either tamsulosin or placebo. Furyk JS, Ann Emerg Med. 2016;67(1):86-95.e2. No difference was detected between treatment groups in the overall rate of urinary stone passage after 28 days of therapy.
Strengths of the study Recruited from emergency departments Overall , diverse sample with respect to race , making results more generalizable. A high rate of ascertainment of the primary outcome, having contacted 97.1% of study participants A high rate of adherence to the study medication A broad range of secondary outcomes Follow-up CT scan in most of our phase 2 Included all patients who had stones in any part of the ureter to increase the generalizability of our study.
Conclusions Stone passage rates were 50% in the tamsulosin group and 47% in the placebo group (relative risk, 1.05; 95.8% CI, 0.87-1.27; P = .60) Our findings do not support the use of tamsulosin for symptomatic urinary stones smaller than 9 mm Although tamsulosin may still play a role in medical expulsive therapy for larger stones, guidelines that recommend tamsulosin for ureteral stones may need to be revised
The new 2016 EAU guidelines on MET
The EAU Recommendations in 2016 have been downgraded to grade C A potential benefit of MET (a-blockers) is most likely for distal ureteral stones >5 mm The question is whether to base treatment decisions on meta- analyses composed of single-center, small, mainly low-quality trials favoring MET or on a few large high quality trials with findings of no significant effect.
Medical Expulsive Therapy for Distal Ureteral Stones:
The Verdict is In
Philipp Dahm et al. EUR UROL 73 ( 2018 ) 39 2– 39 3
Treatment is effective in patients with larger stones in the lower
ureter
No further trials are required
In many countries, CT imaging of patients is not the norm.
The trade-off for MET may be less clear cut
Most stones presenting at the distal ureter are small in size
Remains unclear is the effectiveness of MET for stones in the
proximal and mid ureterIt is important to inform patients about the possible but
as yet unproven benefit using a-blockers as well as their
off-label use and possible side effects !!
THANK YOU !You can also read