Health Systems Analysis: Colombia Case Study - Lancet Commission on Global Access to Palliative Care and Pain Control
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Lancet Commission on Global Access
to Palliative Care and Pain Control
Health Systems Analysis:
Colombia Case Study
December 2016
Not for Citation or Circulation
Colombian Context Socio-economic: – Upper-middle income – Stable economic growth (~3% GDP annual) – Stark inequalities, Gini index = 0.53 Demographic: – Population: 48.2 million – Aging population (>60 expected to triple by 2050 to 27%) Epidemiological: – NCD burden on the rise (83% total burden of disease) – High burden of injuries, interpersonal violence, chronic pain
Health System Overview
Ley 100 (1993) introduced a universal health insurance scheme for all
citizens
– Coverage increased from 24% to 97%
– OOP spending decreased from 52% to 15%
– Resulted in financial protection from CHE, improved access to
services (mostly benefitting the poor)
– Contributory Regime covers workers with monthly income,
financed by mandatory payroll tax contributions
– Subsidized Regime covers poor/unemployed, financed by national
and local govt tax revenues and a payroll tax “solidarity
contribution” subsidy from the contributory regime
– Both now cover same benefits, Plan Obliatorio de Salud (POS),
but inequalities persist, particularly in quality of services
Impressive reform, but not UHC without palliative care or pain control
Colombian Context
Colombian Context – Low quality of death index (EIU) – 1 of only 4 countries to legalize euthanasia
Plan Decenal de Salud
Pública
10-year Public Health Plan, (2012-2021)
– Conceptual model based on social determinants of health
– Large focus on NCDs
– Differential approaches for specific population groups
– Includes PC (to organize and guarantee coverage of PC services and
opioids) as part of strategy for aging population
Ley Estatutaria de Salud
Statutory Health Law (2015)
– Guarantees fundamental right to health for all citizens
– Establishes link between the right to health and essential public
health interventions that aim to address social determinants
– Presents a model for integrated healthcare delivery,
Modelo de Atención Integral en Salud (MIAS):
Source: MSPS Colombia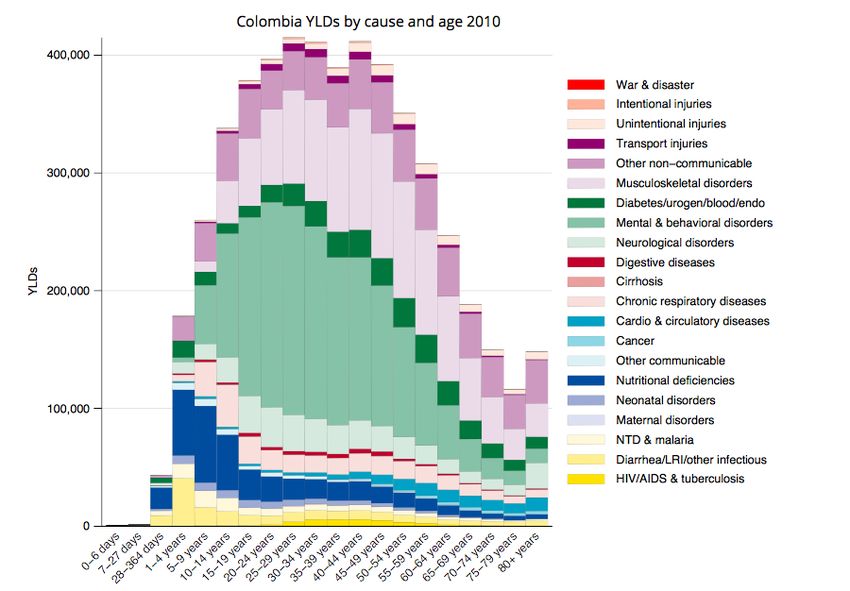
Palliative Care in Colombia
History of PC in Colombia:
1980s: first pain control/PC clinic and hospices were established
1990s: PC program at National Cancer Institute initiated, PC associations
begin forming, work begins in opioid accessibility, PC education and
specialization programs
2000s: Decentralization of opioid procurement, restrictive prescription laws
are modified
2010: Most opioids added to Mandatory Benefits Plan, first national law
incorporating palliative care is passed (cancer care)
Sandra Ceballos Law (Law 1384 of 2010)
– Guarantees PC as part of the comprehensive management of patients with cancer
and their families
– PC aimed at improving the quality of life of patients and cancer survivors and their
caregivers
– Law mandates provision of palliative care and pain relief at different levels of
complexity for cancer patients, and ensure access and availability of opioids in the
country
Palliative Care in Colombia
PCPC Status (as of 2012)
• Opioid availability
– Each state in Colombia now has at least one pharmacy that dispenses opioids 24/7
– Additional opioids (methadone, hydromorphone, and morphine solution) are all
included in Mandatory Benefits Plan available at no cost to patients
– Allowable length of opioid prescriptions extended from 1 week to 30 days
– Limited availability in rural areas due to operational barriers in procurement process
• Access to PC services
– All citizens under CR or SR have right to PC services, but many services still
linked/restricted to cancer patients. Other diseases have less PC coverage.
– Hardly any PC services available outside major cities.
• Education
– Palliative care training is mandatory in only ~5% of medical schools
• Research
– 4 PC research groups in the country
– International collaborations w/ ALCP and IAHPC
• National Guidelines
– Health and educational institutions have partnered with NGOs to advise MOH/Senate
New Palliative Care Legislation
Colombian Palliative Care Law (Law 1733 of 2014)
– Guarantees the right of patients with terminal, chronic,
degenerative and irreversible conditions to palliative care
services, to improve the quality of life of the patients and families
through an integrated treatment of pain and other physical,
emotional, social and spiritual symptoms, according to clinical
guidelines establish by MSPS
– Outlines the obligations of the health system and the
government:
• To offer palliative care services with equity and quality in all levels of
care throughout the country;
• To educate health professionals; and
• To ensure availability of opioid medication 24/7New Palliative Care Legislation
Colombian Palliative Care Law (Law 1733 of 2014)
Ongoing implementation work:
MSPS:
– Defining CPG, protocols, national plan for PC
• Instiituto de Evaluación Tecnológica en Salud published CPG in
2016
• MSPS currently working on integrated national PC plan with INC
• In April 2016, MSPS circulated instructions to EPS on minimum PC
service requirements
– Formalizing accreditations of services, certification
Active civil society and PC associations:
• writing guidelines
• designing programs to include PC in all levels of medical education
• following implementation of law, monitoring and collecting data on
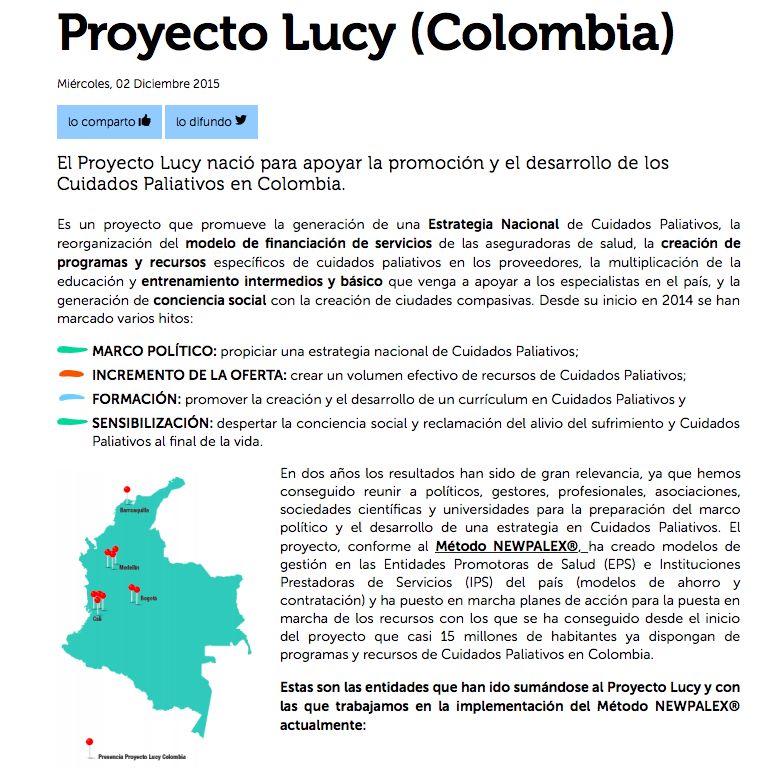
PC status in the countryProyecto Lucy
2014 2015 2016
No. of HMOs with 1 3 6
PC coverage
No of Insured in 2 MM 6 MM 10 MM
HMOs with PC
programs
No of Institutions 10 20 30
providing PC
services
No of patients 4.000 10,000 25,000
treatedProyecto Piloto: ITES
• “Iniciativa Transformando El Sistema” con el fin de fomentar la integración
del CP en el currículo de pregrado en ciencias de la salud en
Latinoamérica.
• Inicio del proyecto: solo 3/57 facultades de medicina y 0/37 facultades de
enfermería incluía CP en el currículo de pregrado.
• Se visitaron 6 universidades para evaluar el interés y potencial inclusión del
CP en los currículos de pregrado.
• Se hicieron talleres para determinar en consenso las competencias en CP
a nivel nacional en el pregrado y para la capacitación de docentesKey Challenges
Stewardship and governance:
• Lack of accountability (no reporting or monitoring mechanisms in place for
PC)
Financing:
• MSPS has yet to define basic essential PC package for inclusion in POS
Service Delivery:
• Isolated PC service provision and unequal access (supply and quality)
• Lack of medicines and human resources in rural and dispersed areas
• Operational barriers in decentralized opioid procurement system/supply
chain
Resource management:
• Continuing to expand PC education at undergraduate and postgraduate
levels, training of physicians to address specific needs of PC patientsOutlook for PCPC in Colombia
Policies for better Policies for better
healthcare health
Sandra Ceballos Law (2010) 10-year Public Health Plan (2012-2021)
Colombian Palliative Care Law (2014) Statutory Health Law (2015) + MIAS
Active
civil society Integrated/Universal
Palliative Care
CoverageKey Lessons Learned
1. The strong, evidence-based advocacy undertaken by PC
professional groups/civil society since the 1990s has been
the driving force behind PCPC provision reform, and will
continue to play a major role in the integration of PC into
UHC.
2. Integrated, comprehensive health model initiatives (MIAS)
provide key platforms on which to embed PC.
3. Lack of defined package of PC services is a significant
barrier.
4. National PC policy plans and frameworks need to be
developed and operationalized to achieve universality.You can also read

















































