High-Yield Cognitive Behavioural Therapy Techniques for Persons with Psychotic Symptoms CBT of delusions & negative symptoms - Friday, August 13 ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

High-Yield Cognitive
Behavioural Therapy
Techniques for Persons with
Psychotic Symptoms
CBT of delusions & negative
symptoms
Friday, August 13, 1-4 p.m.
How can we make sense
of delusion?
Some basic theory…..

A delusion is a false belief out of
keeping with educational, social
and cultural background. It is
held with extreme conviction
and is not amenable to reason.
Simms
It is a waste of time to argue
with the deluded patient
Hamilton
Neither previous experience nor
compelling counter-arguments
can shake the certainty of the
delusion
Scharfetter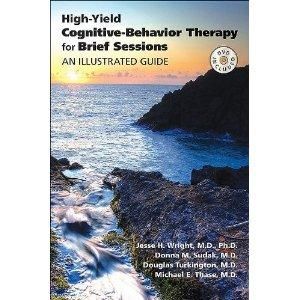
“Don‟t talk to the patient about
their hallucinations and
delusions…..on the contrary the
patient should be encouraged to
ignore them”
Fish
A delusion is a belief which may
be false and at the extreme end
of consensual agreement, it can
be culture dystonic but may be
amenable to reason
Turkington et al, 1997.
Cognitive vulnerabilities to delusion formation • Theory of Mind deficits • Attributional Style • Jumping to conclusions • Certification • Specific schema vulnerabilities.
Types of Delusions (form) • Secondary delusion • Delusional perception • Delusions of reference • Delusional memory • Multiple linked delusions • Primary systematised delusion
Delusional content Culture syntonic • Spain 50% religion; 40% computers etc) • Italy 50 % religion; 30% mafia etc • UK 20% religion; 50% microchips etc • China 50% spirits of ancestors 50% erotomanic, jealous • West Africa: 50% witchcraft
CBT models of delusion • “Normal” • Jumping to Conclusions (type I) • Systematised delusion linked to trauma (type IIa) • System linked to hot cognitions (type IIb)
CBT for delusions The early stages…
Taping sessions • Avoid if patient too paranoid. • Excellent osmotic homework. • Something to take from the session. • Use for supervision.
Simple delusions • Be friendly • Ask peripheral questions • Gather pertinent general information • Ask Socratic Questions • Introduce doubt • Generate alternative explanations • Draw a pie chart
Simple delusions • Do an easy behavioural experiment • Follow up with a more challenging experiment • Redraw the pie chart • Support the patient in the new belief
Therapeutic Relationship
• Clinician should be curious, relaxed,
friendly, honest & respectful..needs to
have enough
• Personal disclosure can be used
– Personal experience of using CBT to
overcome a phobia of public speaking
– Doctors hearing the telephone ringing when
it isn't
– Doctors thinking that the hospital managers
are persecuting themBe friendly • Could it be true..or partly true? • Curiosity and respect. • Ready to validate true statements • Open to persuasion • Open to the evidence • Normalise
“The aliens might do
something”Evidence • The immensity of space • Space is curved • Worm holes/ black holes • Cultural devastation • Proton accelerator experiments • Synchronicity
Suspicious Minds • “People are talking about me” • “There is a conspiracy against me” • “That item on the radio / TV might have referred to me” • “I had something to do with that crime / accident” • “That police car is waiting for me” • “I have been singled out for bad treatment” • “That memo which went around the office is mostly about me”
ParanoidThoughts.com
People who cope better… • Keep the thoughts in proportion “don‟t catastrophise..” • Keep a distance on the paranoid thoughts so as to be emotionally neutral about them • Talk to others about them • Have more self esteem
What will you say to be word perfect and accurate? • “people are watching me”
Peripheral Questions for
Delusions
• How did this all start?
• What were you doing/ feeling ?
• How did he/ she behave?
• What was he/ she wearing?
• How would such a device be
operated?
• How many people would that take?Example David • David believed that a satellite was taking the thoughts out of his mind and broadcasting them. • He was preoccupied and distressed. He had auditory hallucinations, social withdrawal and poor self care.
Peripheral questions
Working with a delusion • “I am ugly”
What are the parameters of
ugliness?
• Prettiness
• Nice eyes
• Nice hair
• Complexion
• Self care
• Choice of jewellery
• Choice of clothing
• Nice smellCan you design an easy behavioural experiment?
Go back to the start of the
delusion.
• Inductive questioning
• Imagery
• Role play
– May lead to schema activation –
distress in 30%
– Integrative experience in 70%
– Should give hints to functionality of
particular symptoms and start to
clarify themes in psychotic contentBehavioural experiments
Illustrative Example • Patient believes that there are evil entities „shadows‟ in her house which can take you over (100% conviction) • Whenever people‟s eyes go pinpoint they have been possessed. • Refuses to look in people‟s eyes, imagines a crucifix and pinches herself.
Patient and therapist watched the film
Breakfast at Tiffanies
brightness
shadows
emotion
grit
Re-rate original
belief and emotion
in light of
alternativeCan you design the next
experiment?DVD clips of behavioural experiments for delusion
Can you design 2 stage experiments
for these delusions?
• I am emitting a foul smell
• My bones are radioactive
• A satellite is burning my genitals
• My flatmates are poisoning my
food
• Fat, bald mafia men are following
me.
• A demon is talking to me and is all
powerful.Grandiose Delusions
Case study guide to CBT of
Psychosis (Wiley) 2002.
• Multi-disciplinary
use of CBT
• Training issues
• Supervision
• Implementation
• More detailed
case reports
• RoadblocksCognitive Therapy of
Schizophrenia 2005 (Guilford)
• Full therapy manual.
• Assessment
• Formulation
• Schema techniques
• Subgroup and
symptom
applications.
• Detailed case
studies.
• Evidence base.“Don‟t talk to the patient about their
hallucinations and delusions…..on
the contrary the patient should be
encouraged to ignore them”
FishWhat are negative symptoms? • Affective flattening: difficulty in communicating or expressing emotion. • Alogia: slowness to respond, and not much to say. • Avolition: Get up and go has gone, little motivation. • Anhedonia: Unable to get pleasure from anything. • Attention deficits: poor concentration/memory • Social Withdrawal
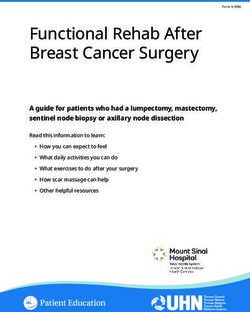
Negative Symptoms and Side Effects
From Lewander, T. (1994) Neuroleptics and the neuroleptic induced deficit syndrome. Acta Psychiatrica Scandinavica 89 (suppl. 380): 8-13
Psychological Neuroleptic Side Negative Symptom
State Effect
Vigilance Drowsiness Attentional Impairment
„Will‟ Apathy Apathy
Lack of energy Lack of Purpose.
„Weak, Tired‟
Mood Flat Affect Affective Blunting
Indifference Restrictive affect
Emotional Lack of Feeling Reduced emotional
Responsiveness Dysphoria range
„Dead inside‟
Motivation Reduced drive Asociality
Reduced initiative Reduced curiosityPossible Explanations for Negative
Symptoms
Affective Flattening Shock or demoralisation following a
potential trauma or difficult time.
Alogia Reaction to criticism or bullying.
Avolition Driven to standstill from high pressure
and failing to meet expectations.
Anhedonia Hopeless, numb and demoralized
Social Withdrawal Keeping stress to a minimum, lower
overstimulation (i.e. Diurnal variation)
Attention Deficit Over-stimulated causing poor
concentration and attentionPotential Losses in Schizophrenia • Loss of identity as a healthy, functioning person • Loss of control • Loss of job and income • Loss of structure to the day. • Loss of friends / relationship break up. • Loss of aspirations. • Loss of social status. • LOSS OF HOPE!
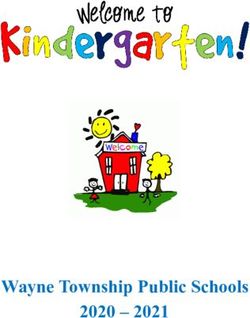
Vicious cycle following job loss
I‟ll never be
employed again
Mood worsens. Mood: sad, shame
Self care goes downhill
Behavior: Withdraws,
Increased voices avoids friends
No distraction, Dwells
on thoughts, reduced
opportunity for positive
events in lifePractical Solutions • Side effect monitoring – including base line measures (e.g. LUNSERS) will highlight the impact of medication on „negative symptoms‟. • Sensitively deal with secondary gains. • Behavioural Activation • Deal with associated cognitions • Family work
Interventions with Depression
Cognitive
Interventions
Behavioral
Interventions
Severe Depression
Mild DepressionActivity Schedule
Instructions: Please write in each box for every of hour of the day:
Activity, Achievement (A=0-10), Mood (M=0-10) and Pleasure (P=0-10)
Time Monday Tuesday Wednesda Thursda Friday Saturd Sunday
y y ay
6-7am
7-8am
8-9am
9-10am
10-
11am
11-
12pmPoints for Monitoring Activity • Fill in activities as you go through the day (as frequently as possible). • You are always doing something (even if it‟s sitting looking out of the window – that‟s doing something) • Rate each activity on a scale of 0 – 10 for pleasure/enjoyment and mastery/achievement (P scores and M Scores)
Why monitor activities? • Provides data on the client‟s current level of activity • Demonstrates the relationship between mood and activity • Identifies activities that occur too frequently (e.g. staying in bed ruminating for long periods) • Identifies activities that do not occur frequently enough (e.g. engaging in pleasurable activities) • Establishes what activities give highest and lowest mastery and pleasure ratings • Allows the therapist and client to test thoughts like „I don‟t do anything‟ which may or may not be the case • Tests thoughts such as „no matter what I do, it makes no difference to how I feel‟. • Highlights any excessively high standards held by the patient that are getting in the way of their ability to give themselves credit for completing tasks made more difficult because of the depression
Scheduling Activities • Aim to increase activity, re-establish routine and to maximise levels of mastery and pleasure • Alleviate clients‟ difficulties with indecision and procrastination • Emphasis is always on attempting the planned activity and not on its successful completion • Write a plan of activities for the coming week (may require help at first).
Scheduling Activities • Plan both pleasurable and mastery based activities (from previous schedule) • Allow flexibility • Rate each activity as before. (A, P, M) • Look at predictions • Identify cognitions that may be getting in the way and explore these.
Grading Tasks • Aim is to gradually re-establish routine • Maximise the chance of success • Specify time limits rather than aiming for completion of the full task • Level of difficulty of the task can also be graded • Start small: e.g. go to bed rather than sleep on sofa, 10 minute walk, read one article in a newspaper etc • Work to re-establish social contacts, daily chores etc.
Cognitive Systemic Considerations
Adam’s Behaviour Parents’ Interpretation
Staying in bedroom a lot, He’s so lazy,
sleeping long hours. He’s just not trying
Adam’s Interpretation Parents’ Behaviour
They’re not bothered about Nag him
me at all. No one cares Tell him he’s lazy and a wasted
of spaceCognitive Systemic Considerations
Adam’s Behaviour Parents’ Interpretation
Staying in bedroom a lot, Schizophrenia has changed
sleeping long hours. Adam, he’s so poorly now.
Adam’s Interpretation Parents’ Behaviour
Every one has given up on Leave him alone
me, feels like my life is over Don’t encourage him to
engage in more activitiesDVD of CBT for thought
disorderAdherence CBT • Shared control of prescribing. • Normalising/ personal disclosure • Health belief model • Word perfect accuracy on mechanism of action and outcome • Relapse and recovery • Stigma reduction
CBT techniques for adherence • Attitudes to medication taking “I am not a pill person” • Schemas which interfere with compliance:- approval, control, achievement, entitlement • Relapse prevention • How does it work?.....salience and tranquillisation….
DVD of CBT for adherence
Staying Well • Relapse Signature • Coping Cards • Action Plan • Getting Carers on Board • Attitudinal Change • Advance Directives • Sleep Hygiene and Managing Anxiety
www.theinsightpartnership.co.uk
You can also read