Integrating Physical & Mental Health in Surrey - The King's Fund
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
13/03/2017
Integrating Physical & Mental
Health in Surrey
The King’s Fund ‐ Presentation
10 March 2017
Dr Helen Rostill
Director of Innovation, Development and Therapies
Surrey and Borders Partnership NHS Foundation Trust
Sue Robertson
Head of Collaborative Programmes and Partnership
NHS North West Surrey Clinical Commissioning Group
Surrey has three STP Footprints
1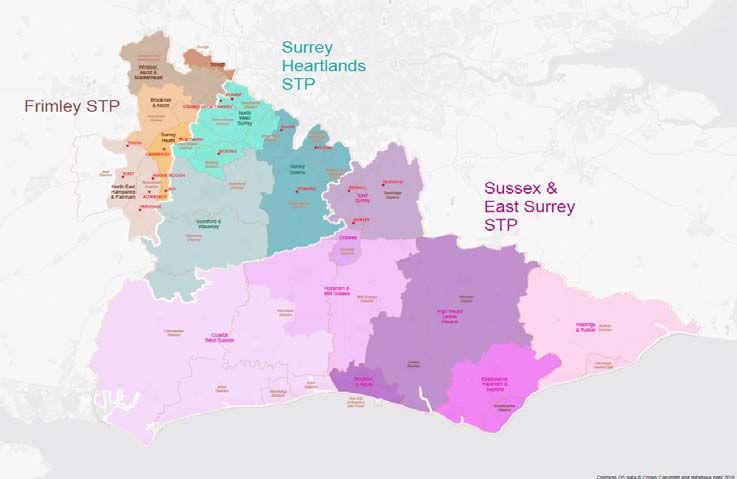
13/03/2017
Approaches to integrating care in Surrey
• National initiatives and models:
– NW Hampshire and Farnham Vanguard
– Innovation: Technology Integrated Health
Management (TIHM)– Internet of Things Test Bed
• Locality hubs and integrated care models –
Surrey Heartlands STP, incl. Epsom Health & Care
and NHSI Guildford and Waverley
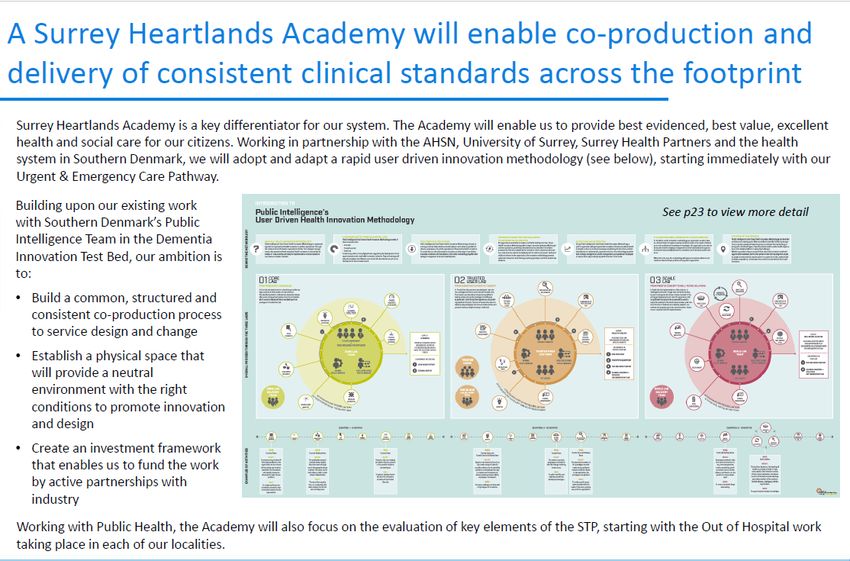
• Surrey Heartlands Academy
• Mental‐Physical health integration in primary
care – developing our approach within the STP
Integrated Care
National Initiatives and
Models
2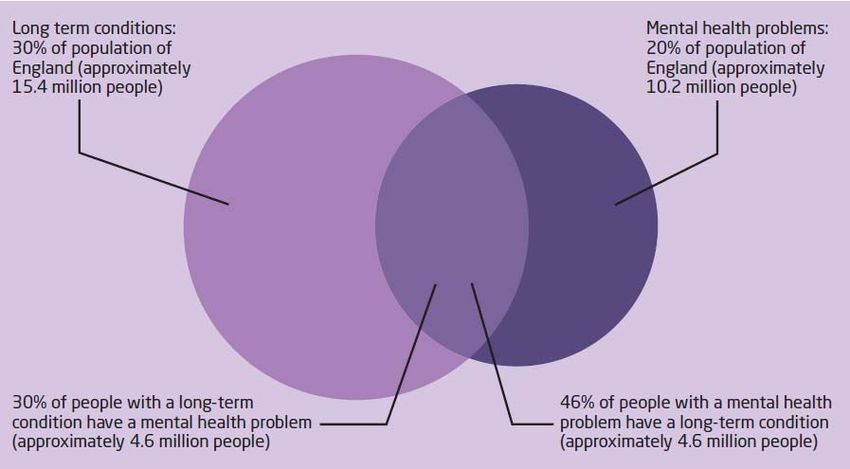
13/03/2017
Primary and Acute Care System
3
13/03/2017
Who we are – local context
Our partnership
Salus Medical Services Ltd –
(24 Member Practices)
Local third sector partners
North East Hampshire and Farnham Vanguard
4
13/03/2017
A shared vision to improve health and wellbeing
OUR VISION
Our vision is that local people are supported
to improve their own health and wellbeing,
and that when people are ill or need support,
they receive the best possible joined up care
North East Hampshire and Farnham Vanguard
Secondary Care Our programme
Highlights
Designed by care
professionals and local
people
A new model
of care
A new A new
commissioning provider model
model
Commissioners pooling Providers collaborating
budgets and aligning to manage population
incentives health
North East Hampshire and Farnham Vanguard
5
13/03/2017
Model of care implementation
System wide Primary care at scale
prevention
and self care
New partnerships for acute
care in the community
North East Hampshire and Farnham Vanguard
6
13/03/2017
Patient reported Outcome Measures
Frimley STP Footprint
7
13/03/2017
Vanguard lessons and latest
• Progress is slow – our key learning it that it
takes time to transform a system
• Our system leaders are working well together
and experimenting as an “accountable care
system board”
• PROMS and PREMS indicate improved
outcomes and experience.
• Most acute system metrics not showing
improvement yet
Innovation
IoT Test Bed
8
13/03/2017
Technology Integrated Health Management
Internet of Things Test Bed
Test Bed Objectives
• Improve health and care outcomes for people with dementia and
their carers, enabling people to stay at home longer, reduce hospital
bed days and postpone/delay nursing home care
• Test interoperable combinations of technologies combined into an
Internet of Things
• Drive change in workforce practice and cascade learning into the
care pathway
• Ultimately to deliver improved care at lower cost
9
13/03/2017
Innovation Partners
Eight companies with 20 devices and services, including monitors, motion sensors,
apps, hubs, virtual assistants, location devices and wearables
Locality Hubs and Integrated
Care Models
Progress, Pitfalls and Learning…..
1013/03/2017
Locality Hub – conceptual model (one‐stop‐shop)
A physical building next to a community hospital providing an integrated frailty service for
people & their carers with all locality GP practices and services operating in a network
X
Locality Hub
Assessment, Care Coordination & Care Planning
Hub out‐reach
Adherence & Persistence
Place of residence
e.g. Adaptive Environment & Assistive Tech. Hospital
• Home
• Nursing Home
• Residential Home
Medical Monitoring & Testing
Transport
• Extra Care Housing Medication Management
Self Care
Carers, Family, Friends & Community Support
Care packages
Emotional Resilience
Transitions
Support services Hub out‐reach into
People are referred to the Hub
hospital to proactively pull
from local services based on flags Diagnostics people through the urgent
for high risk & formal screening at
care system
GP surgeries Pharmacy
Locality Network: GP Practices, Community & Social Services, Mental Health, Borough Council & Voluntary Sector
Multi‐disciplinary Team working
A multi‐disciplinary team approach supports people in the Hub
Locality Hub
Associate Community Locality hub manager Social Care Mental Health
Practitioner Matron Specialist Specialist
Social Care Community
Specialist Specialist
Worker Mental Health
Geriatricians Nurses
Nurse
Therapist Other specialists as
Pharmacist Wellbeing Co‐ required
ordinators
Practice Nurse Person’s GP
(MDT attendees may flex depending on patient need)
1113/03/2017
NW Surrey Integrated Health & Care – Logic Model
Context: The Five Year Forward View, a growing elderly population with long term conditions and multi‐morbidities will exert pressures on the system and on informal unpaid carers.
Rationale: NW Surrey has 15,000 frail elderly, or at significant short term risk of becoming frail. Each complex patient averages seven inpatient admissions per year. Audits show that half of inpatient stays on
medical units were avoidable and 29% did not meet the criteria for acute care admission; 30% spent at least half of their stay waiting to be discharged. Our vision is to create a coherent health & care system
delivering the best possible outcomes with a highly effective acute trust working alongside a primary care‐led integrated out of hospital service wrapped around the community. This will promote independence,
physical and mental health and deliver better value for money.
Inputs Activities Outputs Outcomes
Efficiency Metrics
• The people and financial resources & • Access to Bedser integrated care hub • MDT’s in all 3 Localities focused on • Reduction in A&E visits
leadership capacity of commissioners Woking ‐ local experience care for the 15,000 patients with • Reduction in non elective admissions
and providers of health and care for • Integrated patient‐centric frailty service highest risk & need seven days a week • Reduced bed days/LOS
local people: NW Surrey CCG, Ashford operating in a single network in • Robust care coordination by named • Reduced re‐admission
& St. Peter’s Hospitals, Surrey County Integrated teams staff. • Reduction in admissions to nursing
• Single Point of Access for referrals and care homes
Council, GP Practices (, Thames Medical • Hubs based around physical buildings • Reduction in social care packages
14, SASSE 13, Woking 13), Surrey & • Uses risk stratification to identify those • Rapid Response available in the
• Maintaining people at home for
Borders Partnership Trust, Surrey Age with the most complex needs community for patients at immediate >91days post discharge
UK, Surrey CC, Virgincare, Elmbridge, • Consultants providing direct clinical risk of admission • Increase in identification & treatment
Woking, Spelthorne & Runnymede input to manage patients with complex • Activity measures of people with dementia
Borough Councils needs at home • Extended access 8 – 8 • Reduced annual costs of head of
• Better Care Fund • Assessment, care coordination, shared • Regular well attended MDT meetings population
of a core team of health & social care • No of IBIS registered Hub patients
• Service user and carer representatives care planning and care record utilising • 999 calls matched to IBIS patients.
Volunteers from colleges, universities ‘7 elements care plan’ staff & extended team of specialist &
• IBIS: Hear & Treat, See & Treat, See &
and/or user representative groups • Provides proactive and reactive care with voluntary input Convey.
focus on prevention • Access to a shared care record • IBIS Conveyance Rate, Conveyance
• Discharge to Assess model • Governance arrangements between Avoided, Admissions Avoided.
• Provides opportunities for socialisation organisations enabling population Care & Quality Metrics
& engagement activities – groupwork health management • Improved personal wellbeing
• Estate that is fit for purpose & well • Increased confidence of people to
and community based, including take responsibility for own health
provision of hot meals, exercise classes utilised.
• Improved experience of care
& social activities. • Clinical teams and leaders undertaking (patients & carers)
• Standardised multidisciplinary care, team development • Improved staff satisfaction, staff
evidence based individualised tasks and confidence and staff
activities, utilising self‐management recommendation
concepts which maximise health and Health & Wellbeing Metrics
• Improved mental & physical
help maintain independence and outcomes (mobility, daily living,
functioning. cognition & mood)
• Inclusion of carers and volunteers
• Provision of transport.
• Utilises technology to enable remote
communication for staff and patients &
telehealth interventions.
Evaluation (Surrey Heartlands Academy)
1213/03/2017
Progress in North West Surrey
• North West Surrey CCG launched the Woking ‘Bedser’
Hub – the first of three multiagency health and social
care multi‐agency hubs aimed at providing integrated
care for frail older residents with co‐morbidities to help
them live healthy and independent lives for as long as
possible.
• The Hub is staffed by health and social care providers
who give comprehensive mental and physical health
assessments, diagnostics, treatment interventions and
follow up care.
Outcomes to date
• Since the Hub opened in December 2015, there
has been a 1.3% reduction in non‐elective
admissions across all patients over the age of 75
registered to Woking practices, compared with an
increase in activity in the other two localities.
• Whilst A&E attendances for the over 75s have
risen across all three localities, the percentage
increase for the Woking population was 1.2%,
compared to 4.5% and 12.3% for the other two
localities without hubs.
1313/03/2017
Challenges Why Mitigation
Activity slower than expected, Some patients refused to attend Eligibility criteria expanded
cohort not identifying as many as they were ‘too well.’ WBC contracted as ‘Data Processors’ acting on behalf of GP
patients as the original model GPs slow to refer Practices allowing them to directly contact cohort patients
identified Hub capacity insufficient to prior to explicit consent being obtained
provide an outreach service to Procedures agreed for patients accessing the D2A scheme
care homes (early supported discharge), A&E, wards and specialist
nurses to refer into Hub; Future integration of care home
team with Hub team
Patient assessments taking Staff were not familiar with the Workshop held with staff to ensure clarity of roles.
longer than originally documentation and there was Assessment procedure being reviewed to reduce
planned, resulting in some duplication of work duplication, following which appointment times will be re‐
increased impact on Hub evaluated.
activity
Reactive service not yet Unable to recruit suitably Training and peer support arranged for existing GPs to take
established qualified lead GP on the role
Financial constraints Lead ASPH consultant identified to support the service
Unable to provide patients Patients found it too tiring to see Patients are now brought in to see professionals over two
with all services on one single everyone on a single visit visits
visit Physiotherapy and OT are provided as outreach as found to
be more effective in patients own home
ChenMed model: patients stay Patients didn’t like being left Patients return to the waiting room between appointments,
in one room while the alone, and it was difficult to with one member of staff supervising them.
professionals move about ensure adequate supervision
The provision of regular Voluntary sector slow to engage Continuing to provide creative seated dance, reviewing
activities is limited due to increasing demands on options for other activities
their time
Epsom Health and Care (EHC)
1413/03/2017
Roadmap for EHCforservice
Roadmap EHC serviceprovision April
provision for April 2017‐2018
2017‐2018
Accountable
Care Epsom Health and Care Whole
System Service:
• Co-located
April Budget:
£12.3m • Transformed reablement /
rehabilitation service
2018 • Integrated bed base
• Fully integrated teams
• Integrated management
structure
Neighbourhood
development
Epsom Health
and Care Epsom Health
Stroke and Care
service: Cardiology
• Integrated service
ward
• Enhanced Legally
discharge binging Epsom Health
Consortium and Care
Epsom
Agreement @home service
Health and
Budget:
Care
£3.7m
Integrated GP
in A&E
service April 2017
NHS Improvement – Guildford and
Waverley exploratory project
• Take the area as proof of concept– identify initial metrics of system efficiency
and productivity which can be applied in other systems
• Enable local partners to realign and re‐embed productive relationships for
local long‐run change to be self‐sustaining
• Potential for whole system transformation – health and social care
• Focus on:
1. Frail Elderly and long term conditions (over 65s with co‐morbidities)
2. Dementia and older people in acute, and pathway to community
3. Working age adult psychiatric liaison and acute interface
4. Working age Long Term Conditions
30
1513/03/2017
Learning from our integrated care
experiences
Challenges
• Fragmentation locally and nationally
• Variance
• Established ways of working and commissioning services
• Transformation can destabilise the system and lead to unmitigated risks
• Information sharing
Benefits
• Meeting local need
• Improving access
• Improving patient outcomes and experience
• Building relationships and understanding each others’ roles/business
Learning From Experience
• Relationships are at the core of success
• Collaboration not competition
• Willingness to think differently and
experiment
• Transparent conversations
• Holding onto what we do well
• Recognising that change is hard and takes
time
1613/03/2017
Surrey Heartlands
Academy
1713/03/2017
Surrey Heartlands STP
Mental Health
Mandate:
Integration
Our approach – overview of initiatives
Initiative Outcomes and benefits How will we achieve this
Operating System: • Co‐design a Surrey Heartlands coordinated model/system for mental health, learning disabilities & dementia
• Better coordination of heath & social care system (‘no wrong door’) approach across all • Continue to develop a one person, one assessment, one plan approach
model for ages & abilities to improve experience of citizens within the footprint • Develop SPA & core assessment process
Mental Health ‐ • Standardised interface processes/SOP’s • Establish a common governance framework
• Evidence joint assessment & care planning, escalation plans & shared understanding of risk. • Embed Digital Road Map
within the Outcomes:
wider system • Reduced variation through delivery of evidence based NICE compliant pathways.
• Outcome‐focused, intelligent & data driven commissioning
Prevention: • Citizens will be better equipped to participate in co‐designing services. • Establish Surrey Heartlands Wellbeing prescribing model
• Citizens will be encouraged and helped to make healthier choices to achieve positive long‐ • Develop a series of engagement events to explore engagement & leadership concepts – bit undefined. Is it
Citizen Led term behaviour change and adopt different approaches to self‐care and mental health to co‐design self‐management options This is about working with local citizens to look at how we can
Health & Social prevention strategies. empower them to get more involved in looking after their mental health.
• Ensure good mental Health messaging is embedded into self care initiatives & healthy lifestyle campaigns –
Care • Implement Making Every Contact Count
• Develop Virtual Wellbeing Centre
Increase access • Increased access to: Further develop/co‐design coherent & consistent models of care that span the Surrey Heartlands system:
• IAPT services by 25% by creating better interfaces for those with LTCs • Recovery College combining physical and mental health
to early • completion of IAPT treatment • Primary Care (Team around the Practice)
intervention • specialist perinatal services • IAPT expansion to LTC’s, MUS, Common MH and SMI to improve access rates
• eating disorder services • Extend eating Disorder services inc. children
• 50% of those diagnosed with first episode psychosis get access to evidence • EiIP services meeting national targets
based EiIP packages of care within 2 weeks • Employment services e.g. IPS
• early detection & assessment to physical care (SMI &LD) • Review & expand health psychology in acute hospitals
• Employment for people with SMI • Develop a resource e.g. Lester model to enhance physical health care SMI.
• Trauma services • Develop NICE compliant care pathways/outcomes based models
• Learning from the Technology Integrated Health Management
Managing crisis • More connected networks of services to manage crisis and lead to system efficiencies, • Implement SPA 24/7 Crisis Care (no wrong door – interfaces with children’s pathways HOPE)
reducing: • Evaluate & expand innovative models of care: e.g. Safe Haven
well • admissions to acute MH care • Review existing model, define & scope enhanced model ( to include children & LD) of Psychiatric Liaison in 3
• A&E visits footprint acute hospitals to assess against Core 24.
• lengths of stay –acute care • Gap analysis ‐ review/expand CRHTT to provide intensive home treatment 24/7
• use of SECAM • Expand Carers Support/Healios approach
• And more appropriate use of S136 • Expand model of MH staff in police call centres
• 10% Reduction in suicides • New MH Hospital site expansion
• Increase access to psychiatric liaison • Implement a suicide prevention initiative
• Complete the second hospital for acute MH admissions
• Optimise use of Estates
Dependency: • Increased capability across physical & mental health workforce in recognising MH • Develop eLearning package and Embed MH Training into all standard induction processes across the system
issues/mind body connect for all new starters
Workforce • Improved wellbeing of the workforce • Scope what is already being offered e.g. through Health Ed. England, Public Health etc.
capability and • Develop ‘Wellbeing of the Workforce’ sessions & deliver through Recovery College
• Sponsor GP’s to undertake Accredited Diploma in MH
wellbeing • All organisations to sign up to Wheel of Wellbeing
1813/03/2017
Latest STP Workshop
• 180+ attendees from public, private and
voluntary sector health and social care providers,
commissioners and partner agencies on 7 March
2017
• Our focus on Primary Care: Team around the
Practice
• Checking with partners: what’s working well,
challenges and ideas/solutions
• Challenges and ideas significantly outnumbered
what’s working well!
The overlap between long term conditions & MH
problems
1913/03/2017
Mental health workshop: what people told us
Working well Challenges Ideas/Solutions
Crisis support improving, CPD for GPs, practice staff Enhanced professional
e.g. Safe Havens and other health/care training in mental health
professionals in mental
health
Mindsight Surrey CAMHS Navigating the system and Enhanced use of
model and pooled budgets care continuity technology – e.g. virtual
support for GPs
IAPT self‐referral Early identification of Team around the person
mental health problems and whole family approach
Voluntary sector Stigma Social prescribing and time
involvement, e.g. banking – community
Community Connections activation
Co‐morbidities and Improved signposting and
pigeonholing by ‘condition’ service directories
Ongoing service user
consultation and co‐design
20You can also read