Pediatric Anxiety Disorders - John T. Walkup, MD Pritzker Department of Psychiatry & Behavioral Health - Landspitali
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Pediatric Anxiety Disorders
John T. Walkup, MD
Pritzker Department of Psychiatry
& Behavioral Health
Disclosures
Advisory Research
Source Honoraria Royalties
Board Support
Anxiety Disorders
Association of X
America
Guilford Press X
Oxford University
Press X
Wolters Kluwer X
Tourette Association X X
Trichotillomania
Learning Center X
Objectives At the conclusion of this presentation the participant will: 1. define the barriers to identify and treat the childhood onset anxiety disorders. 2. discuss the suicidal behavior and mania risk of antidepressants in children and adolescents 3. discuss the role of family factors in the successful treatment of children with anxiety disorders. 4. discuss the relative ages of onset for the major psychiatric problems in children and adolescents
Overview § We have very good treatments for the childhood anxiety disorders § Medications (antidepressants) and CBT are effective, § The evidence base is deep, yet.. anxiety disorders are under diagnosed and under treated § Thus, the identification of anxiety and effective treatment requires special knowledge and attitudes which is the focus of today presentation § So what is going on? § The Fundamentals § Suicide and mania hot topics
Introduction - § The Fundamentals § The Anxiety Disorders § Effective medications § Adverse effects § Integration with evidenced based psychotherapy § Hot topics
The Anxiety Disorders
‘Anxiety disorders aren’t just bad normal anxiety” § Dimensional vs categorical view of anxiety § Normal anxiety § Predictable triggers (they make everyone anxious) § Proportionate reaction § Can happen anytime in development § Can be severe and chronic § Pathological § Triggers are normative experiences § Excessive, disproportionate reaction § Predictable age of onset – SAD, SoAD, GAD ages 6-12; § Panic – late adolescence § Highly stereotyped across anxious individuals
Specific Phobia § Animals, insects etc. § Environmental - thunder, water, heights § Blood, injection or other suspected painful event § Situational - tunnels, bridges, elevators § 70% have another anxiety disorder
Separation Anxiety Disorder § Excessive concern regarding separation from home or from attachment figures § Bad things happening to parent and or child § Cannot be alone § Avoidance S, M, L, XL, XXL § Difficulty falling asleep or sleeping with loved ones § Physical aches and pains § Accommodation by adults S, M, L, XL, XXL § Impairment or distress § Can diagnose over age 18 years § Duration of 6 months
Generalized Anxiety Disorder § Excessive worry and apprehensiveness § Restless, keyed-up or on edge. § Fatigued at end of school day § Concentration problems “choking on tests” § Sleep problems (falling asleep) § Tense and irritable § Unable to control the worry § Impairment or distress
Social Anxiety Disorder § Fear of social or performance situations § Specific § Generalized § “slow to warm up” socially § anxious about being with other people § reticent to talk in social settings (short answers, soft spoken) § self-conscious and anticipate being embarrassed § anticipate that others will judge them § worry before an event where other people will be § avoid places where there are other people § blush, sweat, or tremble around other people § feel nauseous or sick to their stomach when with other people § depersonalize or derealize when with other people
Selective Mutism § Young children § Ability to speak § Not speaking in social situations § Not part of another disorder § Mild variant (single words, soft spoken)
Acute Stress Disorder § True stressful event – life threatening § Re-experiencing the event § Avoidance and numbing § Increased arousal § Negative thoughts, feelings and moods § Time limited
Post-traumatic Stress Disorder § True stressful event – life threatening § Re-experiencing the event § Avoidance and numbing § Increased arousal § Negative thoughts, feelings and moods § Risks for enduring symptoms § Pre-existing or genetic risk for mental disorder § Proximity § Post-traumatic environment § Stuck in unhelpful narrative about trauma
Panic Disorder § Attacks of anxiety (Physical Symptoms) § Heart rate, pounding heart, palpitations § Hyperventilation, shortness of breath § Choking sensation § Chest discomfort or pain § Abdominal pain § Some psychological symptoms § Worry about the next one § Avoidance behavior related to the attacks § Agoraphobia….
Obsessive Compulsive Disorder § Prominent obsessions or compulsions § Dirt, germs, or other contamination § Ordering and arranging § Checking § Repetitive acts § Impairing or time consuming
Infection-triggered
Childhood Onset Conditions
§ Neuropsychiatric disorders associated* with
infections
§ PANDAS (Strep)
§ PANS (acute onset with other infectious agents)Characteristics Common to All
Anxiety Disorders
§ Hypervigilance
§ Reactivity to novel situations
§ Biased interpretation of experiences as
threatening
§ Avoidance coping
§ Catastrophic reactions
§ Parental accommodation
§ Midline physical symptomsTension headache
Dizziness
“Lump in the throat” Perioral tingling
Can’t swallow pills (hyperventilation)
Worry about gagging,
“Can’t catch his/her breath”
choking, swallowing, and
Shortness of breath,
vomiting
Chest pain hyperventilating
Abdominal pain
Bowel and bladder
Tingling in finger tips
urgency
(hyperventilation)
Figure outline attributed
to Servier Medical Art, Thanks to Sarah Hellwege for putting
modified by addition of the slide together
anxiety symptoms and
midline.Anxiety is not a great term § Home sickness (separation) § “Worry worts” (generalized) § Self-conscious or shyness (social anx) § Excessive interpersonal sensitivity (all) § Fear (all) § Apprehension (all) § Dread (generalized) § Worry (all) § “Stressed out “
Ages of Onset Risk § ASDs – 0-3 years or later for mild § ADHD - 4-7 or later for mild, but differential is broader § Anxiety – 6-12 years § Depression – 13-16 years § Bipolar and psychosis - > 16 years § Panic Disorder 16-25 years § Disruptive behavior – almost anytime
Assessment Strategies § Global scales with anxiety subscales § Child Behavior Checklist § Behavioral Assessment System for Children § MASC § SCARED § Child version § Search on “U Pitt SCARED” § Parent on child version § Search on U Pitt SCARED § Adult SCAARED
Epidemiology § Very common up to 8-10% of kids § Up to 25% of adults § Under diagnosed § Under treated § Probably the most common childhood disorder and the prepubertal disorder associated with changes in mood and emotion regulation
Environment and Genetics § Genetic vulnerability (twin studies) § Anxiety is self-perpetuating § Avoidance results in temporary relief § Perfectionism is highly valued § Anxiety is “contagious” § Parental attention to the anxious child § Parental support for avoidance § Catastrophic reactions shape relationships
Everyone has anxiety but no one recognizes it as a meaningful condition and clinicians are unlikely to take it seriously and treat it. Why?
Under-recognized and Under-treated § Extremely common, so considered “normal” § Very early onset, so considered a temperamental or personality trait § Triggered affective illness, if not triggered can appear ”well” § Not considered a serious condition § Lack of knowledge re: course of illness/impairment § Evidence base established in 2009 § Only FDA approved med in 2015 § Advocacy/awareness efforts are a recent phenomena § Treatment barriers § Overlapping syndromes
It is just a phase…. § Anxiety Disorders begin very early § When untreated they can evolve and impair across the lifespan § Childhood anxiety to Panic Disorder § Childhood anxiety to Depression and Bipolar Disorder § Childhood anxiety to complex impairment § Accumulated disability § Maladaptive behaviors § Some symptoms meet the ‘just a phase’ definition
Course of Anxiety § Onset in childhood -“Prepubertal affective illness” § Adolescence - symptoms + accumulated disability § Intense symptoms “burn out” ….. sometimes § Generalized anxiety § Poor adaptation and coping – easily flooded and overwhelmed by typical life and developmental expectations § Some morph to depression § School drop out (fade away) § Young adulthood – symptoms + failure in major roles § Work inhibition § Fail to leave home or stay in college § Evolution into panic disorder § Evolution to recurrent depression and risk for bipolar disorder § Substance abuse
Anxiety and Personality Disorders 1) Distorted thinking patterns 2) Problematic emotional responses 3) Over- or under-regulated impulse control 4) Interpersonal difficulties § Borderline Personality Disorder § Avoidant Personality Disorder § Dependent Personality Disorder § Obsessive Compulsive Personality Disorder § Schizoid Personality Disorder
Implications of Anxiety Course on
Treatment
§ Three potential treatment targets
§ Anxiety symptoms – anxiety, distress tolerance
§ CBT and Medication
§ Accumulated disability – poor adaptation and coping
§ Life skills training
§ Maladaptive behaviors – suicidal and self injurious
behavior and substance misuse
§ Behavioral treatmentsTreatment Barriers § Anxiety starts early and easily missed § Overlapping syndromes § Symptom patterns evolve and thus, confuse § Fear – patients, parents, providers § Misinformation § Scientific – not a serious mental health condition § Mass Media – trivializing by generalizing § Stigma § Disorders § Treaters § Treatments
Overlapping Syndromes § ASD § ADHD § Depression § Somatic symptom disorders § Personality disorders § Bipolar disorder § Psychosis § Medical problems
The implication of identifying and
treating the childhood anxiety disorders
ADHD ANX Depression
AS
Ps
D
ych
os
is
ADHD Anxiety Depression
Ps
AS
ych
D
os
isOverlapping Syndromes § ASD § ADHD § Depression § Somatic symptom disorders § Personality disorders § Bipolar disorder § Psychosis § Physical symptoms
Tension headache
Dizziness
“Lump in the throat” Perioral tingling
Can’t swallow pills (hyperventilation)
Worry about gagging,
“Can’t catch his/her breath”
choking, swallowing, and
Shortness of breath,
vomiting
Chest pain hyperventilating
Abdominal pain
Bowel and bladder
Tingling in finger tips
urgency
(hyperventilation)
Figure outline attributed
to Servier Medical Art, Thanks to Sarah Hellwege for putting
modified by addition of the slide together
anxiety symptoms and
midline.The Fundamentals of Anxiety
Treatment
§ Evidence base for children established in 2008
(Walkup et al., 2008)
§ Combination treatment most effective - 80% response
rate
§ SSRIs and CBT are both effective – 55-60%
§ Placebo response rate is less than 25%
§ Outcomes more clearly positive than for teen
depression
§ Only 1 med with FDA indication for non-OCD
anxiety disorders – duloxetine (Strawn 2015)Antidepressant Efficacy for Non-OCD
Anxiety Disorders
§ SAD, GAD and SoP
§ Fluvoxamine – RUPP, 2001
§ Fluoxetine – Birmaher et al, 2003
§ CAMS – Walkup et al, 2008
§ SoP
§ Paroxetine - Wagner et al, 2004
§ Fluoxetine - Beidel et al 2007
§ Venlafaxine - March et al, 2007
§ GAD
§ Sertraline - Rynn et al., 2001
§ Venlafaxine, Rynn et al., 2007
§ Duloxetine, Strawn et al 2015
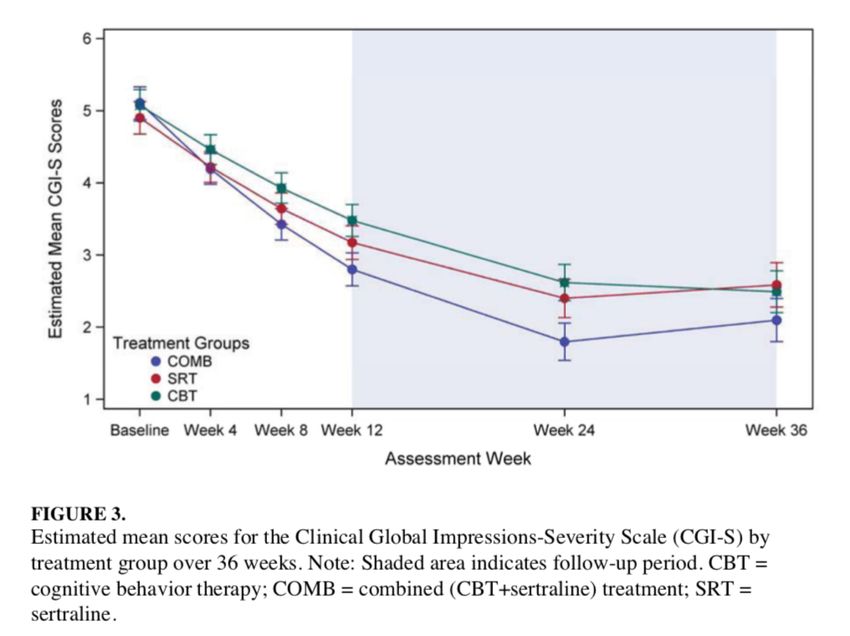
§ Buspirone in GAD, Strawn et al 2015 (huge placebo response)Long Term Treatment § CAMS long term data § >80% maintained response at 24 and 36 week time points § Combined continue to be better than the monotherapies § Participants on medication pursued more concomitant psychosocial treatment than those in combined and CBT. § CAMELS § 46% were in remission for a mean of 6 years § Those who achieved remission in the acute phase were more likely to be in remission at long term follow up § 48% of acute phase responders relapsed during the follow-up. § The challenges of long term studies § Remission rates
39
40
41
42
How many in CBT went onto meds
49/139 Remitted
12/139 kids started
Med
43If your not better why wouldn’t
you explore more treatment?
44Antidepressant USA FDA Approvals § Approved for OCD § Clomipramine > 10 yrs § Fluvoxamine > 8 yrs § Sertraline > 6 yrs § Fluoxetine > 7 yrs § Approved for Depression § Fluoxetine > 8 yrs § Escitalopram > 12 yrs § Approved for Non-OCD Anxiety § Duloxetine > 7 yrs GAD
Dosing of Antidepressants with
Efficacy for Anxiety
§ Use clinical trials for timing of dose changes for
‘maximum safe doses’
§ Fluoxetine up to 40 mg by week 12 (TADS, 2004)
§ Fluvoxamine 100-150 mg by week 10 (RUPP, 2001)
§ Sertraline 100-150 mg by week 8 (CAMS, 2009)
§ Paroxetine 40-50 mg by week 10 (Geller, 2004)
§ Citalopram 40 mg* (Uchida M, et al. J Clin Psychopharmacol. 2017
Jun;37(3):359-362.)
§ Escitalopram 20 mg (Wagner, 2006; Emslie, 2009)
§ Duloxetine 60-120 mg (Strawn, 2015)
§ What about other meds?Refractory Anxiety § Pharmacological augmentation § Serotonin agonists § Antipsychotics § Dopamine agonists § Re-assess for more intensive behavioral interventions § Familial factors § Functional assessment
Family Factors Peris et al., 2009 § The Resistant Triad § High conflict § Low cohesion § High blame § Watch for how behavior change will be accepted in the family.
Function-Based Assessment § Assess and address antecedents and consequences § Provoking experiences – triggers § Intrapsychic reward (+) and relief (-) § Interpersonal consequences § Positive reinforcement – active rewards § Negative reinforcement – escape consequences
Types of Reinforcement and
Related Treatment Options
Positive Negative
Reinforcement Reinforcement
Internally Provides
Relieves distress
Reinforcing gratification
Interpersonally Attention and Avoidance
Reinforcing support AccommodationTypes of Reinforcement and
Related Treatment Options
Positive Negative
Reinforcement Reinforcement
Provides
Internally gratification Relieves distress
Reinforcing (Raise the cost) (ERP)
Attention and
Avoidance
support
Interpersonally Accomodation
(Redirect
Reinforcing (Re-engage,
parents and
not escape)
others)Antidepressants Cause Mania etc § Activation is common 10-15% § Early in course or after dose change – think diphenhydramine § Younger kids § “Minimal brain dysfunction” § Bipolar switches uncommon
Suicidality – Benefit/Risk
§ % Difference for Efficacy
§ MDD - 11.0% = NNT of 10 (3 for NIH Studies)
§ OCD - 19.8% = NNT of 5
§ Non-OCD anxiety disorders - 37.1% = NNT of 3
§ % Difference for Suicidality
§ 1-2% = NNH 50-100 (Hammad et al., 2006)
§ 0.7% = NNH 143 (Bridge et al., 2007)
§ But not for individual disorders
§ MDD - 0.9%; NNH ~100
§ OCD - 0.5%; NNH ~200
§ non-OCD anxiety disorders - 0.7% ; NNH ~140
Bridge et al., 2007Suicidality – Benefit/Risk
§ % Difference for Efficacy
§ MDD - 11.0% = NNT of 10 (3 for NIH Studies)
§ OCD - 19.8% = NNT of 5
§ Non-OCD anxiety disorders - 37.1% = NNT of 3
§ % Difference for Suicidality
§ 1-2% = NNH 50-100 (Hammad et al., 2006)
§ 0.7% = NNH 143 (Bridge et al., 2007)
§ But not for individual disorders
§ MDD - 0.9%; NNH ~100
§ OCD - 0.5%; NNH ~200
§ non-OCD anxiety disorders - 0.7% ; NNH ~140
Bridge et al., 2007Antidepressant Trials § 2 NIMH-funded § Demonstrated efficacy § Low placebo response rates § Many quality indicators § 17+ industry-funded (FDAMA) § Multiple sites § High placebo response rates § No quality indicators § FDAMA exclusivity § No investment in outcome
Number
Exclusivity
Response Placebo of Sites &
Data Source Medication Duration Children Active% Granted
Assessment % (Participa
Nov 201634
nts)
NIMH Studies
Emslie et al., 199715 Fluoxetine 8 weeks GGI-I Yes 56% 33% 1(96)
TADS, 20049 Fluoxetine 12 weeks CGI-I No 61 35 13(439)*
Yes
IINDUSTRY Studies
Emslie et al., 200219 Fluoxetine 8 weeks CGI-I Yes 65 53 15(219)
Keller et al., 200120 Paroxetine 8 weeks CGI-I No 66 48 12(275)*
Berard et al., 200621 Paroxetine 12 weeks CGI-I Yes 69 57 33(286) Yes
Emslie et al., 200622 Paroxetine 8 weeks CGI-I Yes 49 46 40(206)
Wagner et al., 200323 Sertraline 10 weeks CDRS Yes 69 59 53(376) Yes
Wagner et al., 200424 Citalopram 8 weeks CGI-I Yes 47 45 21(178)
von Knorring et al., Yes, single
Citalopram 12 weeks Kiddie-SADS-P No 60 61 31(244) exclusivity
200625
for both
Wagner et al., 200626 Escitalopram 8 weeks CGI-I Yes 63 62 25(264)
medications
Emslie et al., 200927 Escitalopram 8 weeks CGI-I No 64 53 40(312)
Emslie et al., 200728 Venlafaxine XR 8 weeks CGI-I Yes 61 52 50(367) Yes
Atkinson et al., 201428 Duloxetine 10 weeks CDRS Yes 67 63 65 (337)*
Yes
Emslie et al., 201430 Duloxetine 10 weeks △CDRS-R >50% Yes 69 60 60 (463)*
Delbello et al., 201431 Selegiline 12 weeks CGI-I No 59 59 26(308) No
CN104-14132 Nefazodone 8 weeks CGI-I No 63 44 15(206)
Yes
CN104-18732 Nefazodone 8 weeks △CDRS-R Yes >30%↓ >30%↓ 28(317)
15/17
No between group
003-04533 Mirtazapine 8 weeks CDRS-R Raw Score Yes (126/153)* No
difference
*
Walkup, 2017‘We don’t have long term safety data...” § Long-term comparison of affected individuals on drug vs placebo. Or…. ‘We don’t know what treatment is best for whom” § Need very large samples to find moderators § When treatments are good for a respectable sampling frame you wont find moderators ‘We don’t don’t know how best to start treatment” § Need very large samples to do sequence studies, especially if the first step in treatment is good… rerandomize non- responders
Summary § Anxiety disorders start very early § Under-recognized and under-treated § Identifying anxiety is the place to start! § Understanding the Hot Topics is critical to understanding the literature and sophisticated treatment. § Complex treatments for refractory anxiety § For refractory anxiety think… § Medication augmentation strategies § Functional assessment and family involvement
You can also read