Retina Pipeline? What's in the - Retina Today
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
NOV/DEC 2020 VOL. 15, NO. 8 | RETINATODAY.COM
What’s in the
Retina Pipeline?
Tracking the
treatments
of tomorrow.
THE LATEST FINDINGS FROM A LOOK AT FUTURE THERAPEUTICS THE PROMISE OF SUSTAINED-RELEASE
AMD TREATMENT TRIALS FOR DIABETIC RETINOPATHY POLYMER TECHNOLOGIES
1120RT_cover.indd 1 12/4/20 3:43 PM
This is
Laser-ablated micro-surface is designed to support
atraumatic ILM peel initiation1
Optimized grasping platform and angled tip closure
to help mitigate membrane shredding2
GRIESHABER® DSP IMPORTANT PRODUCT INFORMATION
Caution: Federal (USA) law restricts this device to sale by, or on the order of, a physician. Indications for Use: GRIESHABER® DSP instruments are a line of single-use
vitreoretinal microinstruments which are used in ophthalmic surgery, for cases either in the anterior or the posterior segment. The GRIESHABER® Advanced Backflush Handles
DSP are a family of instruments for fluid and gas handling in vitreoretinal surgery. Warnings and Precautions: • Potential risk from reuse or reprocessing GRIESHABER® DSP
instruments include: foreign particle introduction to the eye; reduced cutting or grasping performance; path leaks or obstruction resulting in reduced fluidics performance.
• Verify correct tip attachment, function and tip actuation before placing it into the eye for surgery. • For light fiber instruments: Minimize light intensity and duration of
exposure to the retina to reduce risk of retinal photic injury. The light fiber instruments are designed for use with an ALCON® illumination source. • Good clinical practice
dictates the testing for adequate irrigation and aspiration flow prior to entering the eye. If stream of fluid is weak or absent, good fluidics response will be jeopardized. • Use
appropriate pressure supply to ensure a stable IOP. • If unwanted tissue gets engaged to the aspiration port, it should be released by interrupting aspiration before moving
the instrument. Attention: Please refer to the product labeling for a complete listing of indications, warnings, and precautions.
Reference: 1. Data on File. Alcon Laboratories Inc; May 2018. 2. Data on File. Alcon Laboratories Inc; September 2017.
© 2018 Novartis 5/18 US-GUS-18-E-1175
US-GUS-18-E-1175 RT.indd 1 1/8/20 10:05 AM
This is
Designed to:
Enhance stability with a continuously open port and
CONSTELLATION® Vision System’s IOP compensation1
Reduce pulsatile traction with 20 000 cuts per minute
using 25+® and 27+® gauge probes*, 2,3
Improve vitreous flow4
Enable closer access to tissue plane with beveled tip5
*At similar single-blade flow rates
MIVS IMPORTANT PRODUCT INFORMATION
Caution: Federal law restricts this device to sale by, or on the order of, a physician. Indications for Use: The CONSTELLATION® Vision System is an ophthalmic microsurgical system that is indicated for both anterior segment (i.e., phacoemulsification and removal of
cataracts) and posterior segment (i.e., vitreoretinal) ophthalmic surgery. The ULTRAVIT® Vitrectomy Probe is indicated for vitreous cutting and aspiration, membrane cutting and aspiration, dissection of tissue and lens removal. The valved entry system is indicated for
scleral incision, canulae for posterior instrument access and venting of valved cannulae. The infusion cannula is indicated for posterior segment infusion of liquid or gas. Warnings and Precautions: • The infusion cannula is contraindicated for use of oil infusion. • Attach
only Alcon supplied products to console and cassette luer fittings. Improper usage or assembly could result in a potentially hazardous condition for the patient. Mismatch of surgical components and use of settings not specifically adjusted for a particular combination of
surgical components may affect system performance and create a patient hazard. Do not connect surgical components to the patient’s intravenous connections. • Each surgical equipment/component combination may require specific surgical setting adjustments. Ensure
that appropriate system settings are used with each product combination. Prior to initial use, contact your Alcon sales representative for in-service information. • Care should be taken when inserting sharp instruments through the valve of the Valved Trocar Cannula.
Cutting instrument such as vitreous cutters should not be actuated during insertion or removal to avoid cutting the valve membrane. Use the Valved Cannula Vent to vent fluids or gases as needed during injection of viscous oils or heavy liquids. • Visually confirm that
adequate air and liquid infusion flow occurs prior to attachment of infusion cannula to the eye. • Ensure proper placement of trocar cannulas to prevent sub-retinal infusion. • Leaking sclerotomies may lead to post operative hypotony. • Vitreous traction has been known to
create retinal tears and retinal detachments. • Minimize light intensity and duration of exposure to the retina to reduce the risk of retinal photic injury. ATTENTION: Please refer to the CONSTELLATION® Vision System Operators Manual for a complete listing of indications,
warnings and precautions.
References: 1. Irannejad A, Tambat S, Abulon DJK. Retropulsion and mass flow of 27-gauge vitrectomy probes: comparison of dual-blade/flat-tipped probes and single-blade/beveled probes. Poster presented at: 18th Congress of the European Society of Retina
Specialists; September 20–23, 2018; Vienna, Austria. 2. Alcon data on file. Alcon Laboratories, Inc; June 2018. 3. Alcon data on file. Alcon Laboratories, Inc; June 2018. 4. Alcon data on file. Alcon Laboratories, Inc; June 2018. 5. Alcon data on file. Alcon Laboratories,
Inc; May 2017.
©2019 Alcon 5/19 US-GAU-19-E-0842
US-GAU-19-E-0842 RT.indd 1 1/8/20 10:05 AM
EDITORIAL ADVISORY BOARD
CHIEF MEDICAL ASSOCIATE
Thomas Albini Pravin U. Dugel John W. Kitchens Elias Reichel
EDITOR MEDICAL EDITOR Miami, FL Phoenix, AZ Lexington, KY Boston, MA
Allen C. Ho Robert L. Avery J. Fernando Arevalo Jay S. Duker Derek Y. Kunimoto Carl D. Regillo
Philadelphia, PA Santa Barbara, CA Baltimore, MD Boston, MA Phoenix, AZ Philadelphia, PA
Carl C. Awh Jorge Fortun Baruch Kuppermann Kourous A. Rezaei
Nashville, TN Miami, FL Irvine, CA Chicago, IL
SECTION EDITORS G. William Aylward Thomas R. Friberg Rohit Ross Lakhanpal Philip J. Rosenfeld
RETINA PEARLS GLOBAL PERSPECTIVES London, UK Pittsburgh, PA Owings Mills, MD Miami, FL
Dean Eliott Albert J. Augustin Caroline R. Baumal Julia A. Haller Theodore Leng Steven D. Schwartz
Boston, MA Karlsruhe, Germany Boston, MA Philadelphia, PA Palo Alto, CA Los Angeles, CA
Ingrid U. Scott Ehab El Rayes Rubens Belfort Jr. Tarek S. Hassan Xiaoxin Li Carol L. Shields
Hershey, PA Cairo, Egypt São Paulo, Brazil Royal Oak, MI Beijing, China Philadelphia, PA
Audina M. Berrocal Jeffrey Heier Jordi M. Mones
Stanislao Rizzo Miami, FL Richard F. Spaide
BUSINESS MATTERS Boston, MA Barcelona, Spain New York, NY
Alan Ruby Florence, Italy María H. Berrocal
San Juan, Puerto Rico S.K. Steven Houston III Andrew A. Moshfeghi Ramin Tadayoni
Royal Oak, MI Lihteh Wu Lake Mary, FL Los Angeles, CA
David M. Brown Paris, France
San José, Costa Rica Jason Hsu Timothy G. Murray Sjakon George Tahija
MEDICAL RETINA Houston, TX
Jordana G. Fein FELLOWS’ FOCUS David S. Boyer Philadelphia, PA Miami, FL Jakarta, Indonesia
Fairfax, VA Michael J. Ammar Los Angeles, CA Michael Ip Anton Orlin Nadia Waheed
Philadelphia, PA Robison V. Paul Chan Los Angeles, CA New York, NJ Boston, MA
Heeral R. Shah Glenn J. Jaffe Yusuke Oshima
Chicago, IL George A. Williams
Joplin, MO Luv Patel Durham, NC Osaka, Japan Royal Oak, MI
Steve Charles
EYETUBE RETINA CHIEF
Philadelphia, PA Memphis, TN Kazuaki Kadonosono Kirk H. Packo Charles C. Wykoff
Michael A. Klufas Matthew R. Starr Allen Chiang Yokohama City, Japan Chicago, IL Houston, TX
Philadelphia, PA Philadelphia, PA Philadelphia, PA Peter K. Kaiser Jonathan L. Prenner Young Hee Yoon
David R. Chow Cleveland, OH New Brunswick, NJ Seoul, South Korea
VISUALLY SPEAKING Mississauga, Canada Richard S. Kaiser Aleksandra Rachitskaya
Manish Nagpal Kim Drenser Philadelphia, PA Cleveland, OH
Gujarat, India Royal Oak, MI Szilárd Kiss Ehsan Rahimy
New York, NY Palo Alto, CA
BUSINESS David Levine, Executive Vice President, Stephen Daily, Executive Editor, News
Digital & Custom Media +1 484 581 1871; sdaily@bmctoday.com
David Cox, President/Cofounder +1 609 933 6799; dlevine@bmctoday.com
+1 484 581 1814; dcox@bmctoday.com Cara Deming, Director, Special Projects
Laura O’Connor, Director, +1 484 581 1889; cdeming@bmctoday.com
Adam Krafczek Jr, Esq, Cofounder Market Analysis & Strategy
+1 484 581 1815; adam@bmctoday.com +1 484 581 1860; loconnor@bmctoday.com
Tamara Bogetti, MBA ART/PRODUCTION
Alvin Fu, Senior Director, Analytics & Technology
Executive Vice President/Group Publisher +1 484 581 1888; afu@bmctoday.com John Follo, Creative/Production Director
+1 714 878 0568; tbogetti@bmctoday.com +1 484 581 1811; jfollo@bmctoday.com
Janet Burk, Publisher Dominic Condo, Art/Production Director
+1 214 394 3551; jburk@bmctoday.com EDITORIAL +1 484 581 1834; dcondo@bmctoday.com
Gaynor Morrison, Rebecca Hepp, Editor-in-Chief Joe Benincasa, Digital Art Director
Vice President, Sales +1 484 581 1880; rhepp@bmctoday.com +1 484 581 1822; jbenincasa@bmctoday.com
+1 484 581 1836; gaynor@bmctoday.com Katie Herman, Associate Editor Rachel McHugh, Associate Art Director
Barbara Bandomir, Vice President, Operations +1 484 581 1897; kherman@bmctoday.com +1 484 581 1853; rmchugh@bmctoday.com
+1 484 581 1810; bbandomir@bmctoday.com Tim Donald, ELS, Consulting Editor
Camela Pastorius, CMP, Vice President, tdonald@bmctoday.com
Meetings & Events, Gillian McDermott, MA, Editor-in-Chief, Clinical
Bryn Mawr Communications Group Content, Anterior Segment
+1 484 581 1807; cpastorius@bmctoday.com +1 484 581 1812; gmcdermott@bmctoday.com
Retina Today (ISSN 1942-1257) © 2020 Bryn Mawr Communications LLC is published January/February, March, April, May/June, July/August, September, October, and November/December by Bryn Mawr Communications LLC,
1008 Upper Gulph Road, Wayne, PA 19087. Subscription is free to all applicable US retina physicians. All others, applicable subscription charges apply. For subscription information call +1 800 492 1267 (US only) or e-mail
retinatoday@bmctoday.com. Pending periodical postage paid at Wayne PA and additional entry offices. POSTMASTER Please send address changes to Bryn Mawr Communications LLC, 1008 Upper Gulph Road, Wayne, PA 19087. Bryn Mawr
Communications LLC provides certain customer contact data, which may include customer names, addresses, phone numbers and e-mail addresses, to third parties for promotional and/or marketing purposes. If you do not wish Bryn Mawr Communications
LLC to make your contact information available to third parties for any marketing purposes, please contact us at 800-492-1267 or e-mail us at retinatoday@bmctoday.com. This publication is intended for health care professionals and providers only. The
information contained in this publication, including text, graphics and images, is for informational purposes only and is not intended to be a substitute for professional medical advice. Bryn Mawr Communications LLC, via its Editors and the Publisher,
accepts no responsibility for any injury or damage to persons or property occasioned through the implementation of any ideas or use of any product described herein. While great care is taken by the Publisher and Editors to ensure that all information
is accurate, it is recommended that readers seek independent verification of advice on drug or other product usage, surgical techniques and clinical processes prior to their use. The opinions expressed in this publication are those of the authors and are
not attributable to the sponsors, the publication or the Editorial Board. References made in articles may indicate uses of medical equipment or drugs at dosages, for periods of time and in combinations not included in the current prescribing informa-
tion. Inclusion of advertising material in this publication, or in supplements thereof, does not constitute any representation or guarantee by Bryn Mawr Communications LLC of the quality of such products or of the claims made by the manufacturers.
© 2020 Bryn Mawr Communications LLC. All Rights Reserved. Reproduction in whole or in part without permission is strictly prohibited.
4 RETINA TODAY | NOVEMBER/DECEMBER 2020
1120RT_Edboard/Staff.indd 4 12/4/20 3:45 PM
Discover continuous
calm in uveitis
YUTIQ® (fluocinolone acetonide intravitreal implant) 0.18 mg:
• Proven to reduce uveitis recurrence at 6 and 12 months1*
[At 6 months–18% for YUTIQ and 79% for sham for study 1 and 22% for YUTIQ and 54% for sham for study 2 (P
YUTIQ™ (fluocinolone acetonide intravitreal implant) 0.18 mg, Table 1: Ocular Adverse Reactions Reported in ≥ 1% of Subject Eyes and
for intravitreal injection Non-Ocular Adverse Reactions Reported in ≥ 2% of Patients
Initial U.S. Approval: 1963
Ocular
BRIEF SUMMARY: Please see package insert for full prescribing information.
YUTIQ Sham Injection
1. INDICATIONS AND USAGE. YUTIQ™ (fluocinolone acetonide intravitreal
implant) 0.18 mg is indicated for the treatment of chronic non-infectious uveitis ADVERSE REACTIONS (N=226 Eyes) (N=94 Eyes)
affecting the posterior segment of the eye. n (%) n (%)
4. CONTRAINDICATIONS. 4.1. Ocular or Periocular Infections. YUTIQ is contra- Vitreous Hemorrhage 4 ( 2%) 0
indicated in patients with active or suspected ocular or periocular infections includ- Iridocyclitis 3 ( 1%) 7 ( 7%)
ing most viral disease of the cornea and conjunctiva including active epithelial
herpes simplex keratitis (dendritic keratitis), vaccinia, varicella, mycobacterial infec- Eye Inflammation 3 ( 1%) 2 ( 2%)
tions and fungal diseases. 4.2. Hypersensitivity. YUTIQ is contraindicated in Choroiditis 3 ( 1%) 1 ( 1%)
patients with known hypersensitivity to any components of this product.
Eye Irritation 3 ( 1%) 1 ( 1%)
5. WARNINGS AND PRECAUTIONS. 5.1. Intravitreal Injection-related Effects.
Intravitreal injections, including those with YUTIQ, have been associated with Visual Field Defect 3 ( 1%) 0
endophthalmitis, eye inflammation, increased or decreased intraocular pressure, Lacrimation Increased 3 ( 1%) 0
and choroidal or retinal detachments. Hypotony has been observed within 24 hours
of injection and has resolved within 2 weeks. Patients should be monitored follow- Non-ocular
ing the intravitreal injection [see Patient Counseling Information (17) in the full YUTIQ Sham Injection
prescribing information]. 5.2. Steroid-related Effects. Use of corticosteroids ADVERSE REACTIONS (N=214 Patients) (N=94 Patients)
including YUTIQ may produce posterior subcapsular cataracts, increased intraocu- n (%) n (%)
lar pressure and glaucoma. Use of corticosteroids may enhance the establishment
of secondary ocular infections due to bacteria, fungi, or viruses. Corticosteroids are Nasopharyngitis 10 ( 5%) 5 ( 5%)
not recommended to be used in patients with a history of ocular herpes simplex Hypertension 6 ( 3%) 1 ( 1%)
because of the potential for reactivation of the viral infection. 5.3. Risk of Implant Arthralgia 5 ( 2%) 1 ( 1%)
Migration. Patients in whom the posterior capsule of the lens is absent or has a
tear are at risk of implant migration into the anterior chamber. 1. Includes cataract, cataract subcapsular and lenticular opacities in study eyes
6. ADVERSE REACTIONS. 6.1. Clinical Studies Experience. Because clinical trials that were phakic at baseline. 113 of the 226 YUTIQ study eyes were phakic at
are conducted under widely varying conditions, adverse reaction rates observed in baseline; 56 of 94 sham-controlled study eyes were phakic at baseline.
the clinical trials of a drug cannot be directly compared to rates in the clinical trials
of another drug and may not reflect the rates observed in practice. Adverse reac- Table 2: Summary of Elevated IOP Related Adverse Reactions
tions associated with ophthalmic steroids including YUTIQ include cataract forma- YUTIQ Sham
tion and subsequent cataract surgery, elevated intraocular pressure, which may be ADVERSE REACTIONS (N=226 Eyes) (N=94 Eyes)
associated with optic nerve damage, visual acuity and field defects, secondary ocu- n (%) n (%)
lar infection from pathogens including herpes simplex, and perforation of the globe
where there is thinning of the cornea or sclera. Studies 1 and 2 were multicenter, IOP elevation ≥ 10 mmHg
50 (22%) 11 (12%)
randomized, sham injection-controlled, masked trials in which patients with non- from Baseline
infectious uveitis affecting the posterior segment of the eye were treated once with IOP elevation > 30 mmHg 28 (12%) 3 (3%)
either YUTIQ or sham injection, and then received standard care for the duration of
the study. Study 3 was a multicenter, randomized, masked trial in which patients Any IOP-lowering medication 98 (43%) 39 (41%)
with non-infectious uveitis affecting the posterior segment of the eye were all Any surgical intervention
treated once with YUTIQ, administered by one of two different applicators, and then 5 (2%) 2 (2%)
for elevated IOP
received standard care for the duration of the study. Table 1 summarizes data avail-
able from studies 1, 2 and 3 through 12 months for study eyes treated with YUTIQ Figure 1: Mean IOP During the Studies
(n=226) or sham injection (n=94). The most common ocular (study eye) and non-
ocular adverse reactions are shown in Table 1 and Table 2.
Table 1: Ocular Adverse Reactions Reported in ≥ 1% of Subject Eyes and
Non-Ocular Adverse Reactions Reported in ≥ 2% of Patients
Ocular
YUTIQ Sham Injection
ADVERSE REACTIONS (N=226 Eyes) (N=94 Eyes)
n (%) n (%)
Cataract1 63/113 (56%) 13/56 (23%)
Visual Acuity Reduced 33 ( 15%) 11 (12%)
Macular Edema 25 ( 11%) 33 (35%)
Uveitis 22 ( 10%) 33 (35%)
Conjunctival Hemorrhage 17 ( 8%) 5 ( 5%)
Eye Pain 17 ( 8%) 12 (13%) 8. USE IN SPECIFIC POPULATIONS. 8.1 Pregnancy. Risk Summary. Adequate and
well-controlled studies with YUTIQ have not been conducted in pregnant women to
Hypotony Of Eye 16 ( 7%) 1 ( 1%) inform drug associated risk. Animal reproduction studies have not been conducted
Anterior Chamber Inflammation 12 ( 5%) 6 ( 6%) with YUTIQ. It is not known whether YUTIQ can cause fetal harm when administered
to a pregnant woman or can affect reproduction capacity. Corticosteroids have been
Dry Eye 10 ( 4%) 3 ( 3%) shown to be teratogenic in laboratory animals when administered systemically at
Vitreous Opacities 9 ( 4%) 8 ( 9%) relatively low dosage levels. YUTIQ should be given to a pregnant woman only if the
Conjunctivitis 9 ( 4%) 5 ( 5%) potential benefit justifies the potential risk to the fetus. All pregnancies have a risk of
birth defect, loss, or other adverse outcomes. In the United States general population,
Posterior Capsule Opacification 8 ( 4%) 3 ( 3%) the estimated background risk of major birth defects and miscarriage in clinically rec-
Ocular Hyperemia 8 ( 4%) 7 ( 7%) ognized pregnancies is 2% to 4% and 15% to 20%, respectively. 8.2 Lactation. Risk
Summary. Systemically administered corticosteroids are present in human milk and
Vitreous Haze 7 ( 3%) 4 ( 4%) can suppress growth, interfere with endogenous corticosteroid production. Clinical or
Foreign Body Sensation In Eyes 7 ( 3%) 2 ( 2%) nonclinical lactation studies have not been conducted with YUTIQ. It is not known
Vitritis 6 ( 3%) 8 ( 9%) whether intravitreal treatment with YUTIQ could result in sufficient systemic absorp-
tion to produce detectable quantities of fluocinolone acetonide in human milk, or
Vitreous Floaters 6 ( 3%) 5 ( 5%) affect breastfed infants or milk production. The developmental and health benefits of
Eye Pruritus 6 ( 3%) 5 ( 5%) breastfeeding should be considered, along with the mother’s clinical need for YUTIQ
and any potential adverse effects on the breastfed child from YUTIQ. 8.4 Pediatric
Conjunctival Hyperemia 5 ( 2%) 2 ( 2%) Use. Safety and effectiveness of YUTIQ in pediatric patients have not been estab-
Ocular Discomfort 5 ( 2%) 1 ( 1%) lished. 8.5 Geriatric Use. No overall differences in safety or effectiveness have been
Macular Fibrosis 5 ( 2%) 2 ( 2%) observed between elderly and younger patients.
Glaucoma 4 ( 2%) 1 ( 1%)
Manufactured by:
Photopsia 4 ( 2%) 2 ( 2%) EyePoint Pharmaceuticals US, Inc., 480 Pleasant Street, Watertown, MA 02472 USA
(continued) Patented.
MEDICAL EDITORS’ PAGE
s
RECALIBRATING …
A
s we write this editorial for the last issue of Retina In addition, this issue contains ongoing Aspen Retinal
Today for 2020, we can’t help but look back on the Detachment Society coverage; a thought-provoking article
unprecedented year we’ve all experienced. It started on the importance of long-term inflammation control for
out like any other year: we were traveling to meet- patients with uveitis by Robert C. Wang, MD; a fascinating
ings, booking surgeries, accepting invitations to case of an extramacular dome-shaped elevation referred
lecture, writing our editorial for the January/February issue, for suspicion of circumscribed choroidal hemangioma; an
and offering input on topics and authors as we planned for exploration of how to build networks to screen for retinal
the March issue. By the time we began putting together disease in underserved areas; and an article by a group of
our April issue, the novel coronavirus had fully made itself doctors from Portugal who discuss how OCT angiography
known, and from then until our September issue we dedi- can reveal early changes in hydroxychloroquine therapy.
cated much of each issue to topics related to both retina Also, be sure to take in the beauty of the images in this
and COVID-19. issue’s Visually Speaking column on page 56, where Sham
The pandemic is far from over—we all know that. We Talati, MBBS, DO; Manish Nagpal, MBBS, MS, FRCS; and
also know that a vaccine seems to be on the horizon, but Navneet Mehrotra, MBBS, DNB, FRF, share the case of a
as retina specialists we can’t help with that. So we’ll let the patient with a choroidal mass. We’ve also brought back
epidemiologists and scientists diligently work on that. In our 5Q column, and in this issue you’ll get to know more
the meantime, we will do what we do best and cover time- about Retina Today contributor Brian C. Joondeph, MD,
ly topics, including COVID-19, in Retina Today. MPS, FACS.
In this issue, we take a look at the retina pipeline, As we close the book on 2020, we wish you all good
specifically early phase 1 and 2 studies exploring novel health and happiness, and we look forward to seeing you
targets in the treatment of diabetic macular edema and in 2021! n
AMD, later-stage trials for AMD, therapeutics for diabetic
retinopathy, and extended-release polymer technologies.
There are so many new agents, modalities, and technolo-
gies in clinical trials for the various conditions we treat,
it’s a refreshing reminder of the positive things happening ALLEN C. HO, MD ROBERT L. AVERY, MD
in the world. CHIEF MEDICAL EDITOR ASSOCIATE MEDICAL EDITOR
NOVEMBER/DECEMBER 2020 | RETINA TODAY 7
1120RT_Editorial.indd 7 12/4/20 3:46 PM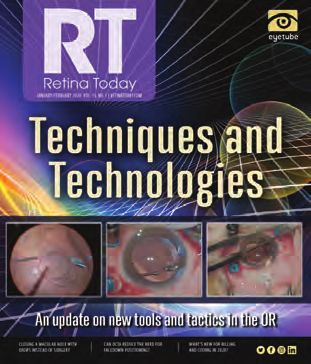
TABLE OF CONTENTS
Cover image credit: ©iStockphoto.com
What’s in the Retina Pipeline?
26 M
acular Research on the Move 34 T he AMD Pipeline: A Look at the Latest Results
By Fuad Makkouk, MD; Brian B. Berger, MD; and Grace Andres By Nika Bagherhi, MD; Allen Chiang, MD; Robert L. Avery, MD;
and Allen C. Ho, MD
30 A Timely Debut for Extended-Release Polymer Technologies 38 The Future Looks Bright: The Therapeutics Pipeline
By Michael Weaver, MS; Tremayne Koochin, BKIN; and Heeral Shah, MD; for Diabetic Retinopathy
Edited by Jordana G. Fein, MD By John Hinkle, MD, and Jason Hsu, MD
DEPARTMENTS
UP FRONTI 46 O CT Angiography Reveals Early Changes
7 Medical Editors’ Page With Hydroxychloroquine Therapy
10 Retina News By Diogo Lopes, MD; Tomás Loureiro, MD; Ana Rita Carreira, MD;
Ana Miranda, MD; Mafalda Pereira, MD; Inês Machado, MD; and
Nuno Campos, MD
MEETING MINUTESI
12 A RDS: Presentation by Philip J. Ferrone, MD
SPECIAL REPORTSI
Summarized by Abdallah Mahrous, MD
50 O phthalmic Presentations of Pituitary Adenoma
By Hanne Gehling, BS, and Kimberly M. Winges, MS
IMAGINGI
14 D ouble Trouble: A Tale of Two Intraocular Foreign Bodies
53 T he Winning Pitch Challenge:
By Remya Mareen Paulose DNB, FLVPEI, FICO, FAICO, and
Helping Innovators in the Trenches
Thomas Cherian, MS, FLVPEI
By Daniel Chao, MD, PhD
MEDICAL RETINAI
VISUALLY SPEAKINGI
16 L ong-Term Inflammation Control Benefits All Types of Uveitis
56 C horoidal Mass: Wading Through the Differentials
By Robert C. Wang, MD
By Sham Talati, MBBS, DO; Manish Nagpal, MBBS, MS, FRCS; and
Navneet Mehrotra, MBBS, DNB, FRF
OCULAR ONCOLOGYI
18 A Masquerader of Circumscribed Chroidal Hemangioma IN THE BACKI
By Ahmed Sheikh, MD; Philip W. Dockery, MD, MPH; and Carol L. Shields, MD
57 Ad Index
58 5Q with Brian C. Joondeph, MD, MPS
GLOBAL PERSPECTIVESI
43 L aying Foundations for International Retina Care
An interview with Eric D. Hansen, MD, and Christopher B. Komanski, MD;
By Benjamin J. Thomas, MD
8 RETINA TODAY | NOVEMBER/DECEMBER 2020
1120RT_TOC.indd 8 12/4/20 3:51 PM
FDA-approved TissueBlue is Ready for You. ™
Introducing
The ONLY FDA-approved selective stain for the ILM.
Easy open-and-inject application from a pre-filled,
sterile syringe.
CONFIDENCE OF SUPERIOR PURITY1 — FDA-approved, pharmaceutical-grade dye.
CONSISTENCY & CONVENIENCE — Pre-filled, sterile syringe eliminates need
to mix or source via compounding pharmacies.
PROVEN SAFETY* — Trusted for ILM staining in over 350,0002
procedures worldwide.
Confidence. Consistency. Convenience.
Visit tissueblue.com to learn more, request a sample†,
and receive further updates.
* Marketed as ILM Blue Outside US since 2010.
† Sample available to registered US physicians only. Samples subject to availability.
References
1. Data on file – Results of HPLC purity tests performed on samples of
compounded BBG dyes available in the U.S. 2. Total DORC Global Sales data
for ILM Blue since launch – available on file.
IMPORTANT INFORMATION ABOUT TISSUEBLUE™ Ask your patient about all the medicines they take, including prescription and over-
(Brilliant Blue G Ophthalmic Solution) 0.025% the-counter medicines, skin products, vitamins and herbal supplements.
BRIEF SUMMARY This summary contains important information about TISSUEBLUE™ WHAT ARE THE POSSIBLE SIDE EFFECTS OF TISSUEBLUE? Adverse reactions that
(TISH-OO-BLU) Solution. It is not meant to take the place of the full Prescribing have been reported in procedures that included the use of TISSUEBLUE™ have often
Information. Read this information carefully before you prescribe TISSUEBLUE. been associated with the surgical procedure. The complications include retinal
For full Prescribing Information and Patient Information please see package insert. (retinal break, tear, hemorrhage, and detachment) and cataracts.
WHAT IS TISSUEBLUE? TISSUEBLUE™ (Brilliant Blue G Ophthalmic Solution) 0.025% WHAT ARE THE INGREDIENTS IN TISSUEBLUE?
is a disclosing agent indicated to selectively stain the internal limiting membrane
Active Ingredient: Brilliant blue G
(ILM). The drug product will be administered by health care professionals only and
should never be given to patients to handle. Inactive Ingredients: Polyethylene glycol and buffered sodium chloride solution
(sodium chloride, sodium phosphate dibasic dodecahydrate, sodium phosphate
WHO IS TISSUEBLUE FOR? TISSUEBLUE™ is for use in patients who, at the
monobasic dihydrate, water for injection).
recommendation of their eye doctor or ophthalmic surgeon, could benefit from use
of the product when treating vitreoretinal conditions requiring removal of the ILM. WHERE SHOULD I GO FOR MORE INFORMATION ABOUT TISSUEBLUE? Go to
www.tissueblue.com or call 800-75-DUTCH or 603-778-6929.
WHAT WARNINGS AND PRECAUTIONS SHOULD I BE AWARE OF? Excess
TISSUEBLUE™ should be removed from the eye immediately after staining. When
using the syringe, surgeons or staff should make sure the plunger moves smoothly Dutch Ophthalmic, USA, 10 Continental Dr., Bldg. 1, Exeter, NH 03833, USA
before injecting the solution. dorc.eu | 800-75-DUTCH or 603-778-6929
tissueblue.com
RT NEWS NOVEMBER/DECEMBER 2020
V O L . 1 5 , N O . 8 | R E T I N AT O D AY. C O M
RETINAL OXIMETRY GIVES CLUES
TO CHOROIDAL MALIGNANCY
Noninvasive measurements taken with such as nevi, the authors pointed out. nous difference was 34.0% and 32.9%
a retinal oximeter detected differences in “Our study identifies a new param- (P = .18), respectively. In patients with
oxygenation in eyes with choroidal mela- eter that differs between [choroidal choroidal melanoma, mean ArtSat
noma that were not present in eyes with metastasis] and [choroidal nevus] (ie, was 94.8% and 93.2% (P = .006), mean
choroidal nevus, a recent study found. increased oxygen use),” the authors VenSat was 58.0% and 60.0% (P = .014),
Eyes with choroidal melanoma showed said. “Because the observed differences and mean arteriovenous difference was
increases in oxygen saturation in arteri- […] are small, this will currently not be 36.8% and 33.2% (P < .001), respectively.
oles (ArtSat) and decreased saturation in of use as a diagnostic criterion, but it “These changes [in eyes with mela-
venules (VenSat), leading to an increased demonstrates that melanoma-related noma] may be caused by inflamma-
arteriovenous difference that was not vascular alterations are present.” tion and a higher metabolism, with
seen in eyes with choroidal nevus, the In the study, retinal oximetry did larger oxygen consumption, leading to
study authors reported in Retina.1 not differ between the affected and altered blood flow and intraocular oxy-
Currently, fluorescein angiography, fellow eyes of patients with choroidal gen relocation,” the authors posited.
an invasive imaging method, is com- nevi; mean ArtSat was 94.5% and 94.2%
1. Brouwer NJ, Marinkovic M, Bleeker JC, et al. Retinal oximetry is altered in
monly used to help differentiate cho- (P = .56), mean VenSat was 60.5% and eyes with choroidal melanoma but not in eyes with choroidal nevi. Retina.
roidal metastasis from other lesions 61.3% (P = .35), and mean arteriove- 2020;40(11):2207-2221.
NEW CRISPR TECHNOLOGY AAO UPDATES
SHOWS PROMISE FOR TREATING CONTINUED IMPROVEMENT SEEN
INHERITED RETINAL DISEASES AT 1 YEAR WITH RPGR GENE THERAPY
Correcting mutations in the RPE65 gene using a novel An investigational gene therapy for the inherited retinal
gene editing technique, known as base editing, significantly disease X-linked retinitis pigmentosa was well tolerated and
restored retinal and visual function in mice with Leber con- demonstrated significant and sustained improvements in vision
genital amaurosis, researchers recently found. in a phase 1/2 trial, according to a presentation at the AAO 2020
“After receiving treatment, the mice in our study could Virtual Annual Meeting. The novel adeno-associated virus/reti-
discriminate visual changes in terms of direction, size, con- nitis pigmentosa GTPase regulator (AAV-RPGR) is being jointly
trast, and spatial and temporal frequency,” said Krzysztof developed by MeiraGTx and Janssen Pharmaceutical.
Palczewski, PhD, the Irving H. Leopold chair and a dis- “The continuous upward trend in efficacy we’ve observed
tinguished professor in the Gavin Herbert Eye Institute, through 1 year with this gene therapy is extremely promising
Department of Ophthalmology at the UCI School of as a potential way to halt the progression toward blindness
Medicine, in a press release. “These results are extremely in these patients,” said trial investigator Michel Michaelides,
encouraging and represent a major advance towards the BSc, MB, BS, MD (Res), FRCOphth, FACS, of Moorfields Eye
development of treatments for inherited retinal diseases.” Hospital and University College London, who presented
The preliminary data suggest that base editing can overcome 12-month data on the therapy at a late-breaking paper session.
initial gene therapy barriers, including unpredictable off-target The primary endpoint of the trial is safety, and secondary
mutations and low editing efficiency; in this study, the research- endpoints are assessing changes in visual function at prespeci-
ers were able to correct mutations precisely and predictably, fied timepoints after treatment. The ongoing trial includes three
explained first author Elliot Choi, an assistant specialist in the phases: dose escalation with low, intermediate, and high doses of
UCI Department of Ophthalmology, in the press release. AAV-RPGR; dose confirmation; and dose expansion. Statistically
10 RETINA TODAY | NOVEMBER/DECEMBER 2020
1120RT_News.indd 10 12/4/20 3:48 PMRT NEWS
s
significant differences in mean retinal sensitivity were observed prior intraocular inflammation (IOI) and/or prior RO in the
between treated and untreated eyes in the intermediate dose 12 months before that first injection, according to an analysis
cohort and in central visual field progression rate in the low and presented at the AAO meeting. Michael S. Ip, MD, presented
intermediate dose cohorts, Dr. Michaelides said. In the high dose the results at the meeting.
cohort, inflammation was evident in two of three adults, and The observed overall risk rate for RV or RO for all brolu-
measures of visual function were not improved. cizumab-treated patients in the registry was 0.46%, but risk
In tests of vision-guided mobility at 9 months, five of six increased to 3.97% in those with prior IOI and/or RO, the
patients demonstrated improvement in walk time for the database analysis found.
treated eye. In addition, in a post-hoc unmasked assessment of data
from the phase 3 HAWK and HARRIER trials presented by
Jeffrey S. Heier, MD, there was an observed trend toward
DATABASE ANALYSIS SHOWS increased incidence of RV or RO in patients with treatment-
emergent anti-drug antibodies.
PROGRESSION OF DRY AMD OVER 2 YEARS Further analyses of this data and additional data collection
Analysis of real-world clinical data from an AAO data- on this subject are ongoing, Novartis said in a press release
base showed significant disease progression over a 2-year recapping information presented at the AAO meeting.
period in more than 69,000 patients with geographic atro-
phy (GA), according to a presentation at the AAO meeting.
Patients with GA in one eye secondary to dry AMD were
more likely to develop new-onset wet AMD when wet
SAFETY ENDPOINTS MET
AMD had already been detected in their contralateral eye, IN PHASE 1 DRY AMD STUDY
the analysis found. An investigational treatment for dry AMD met all the pri-
“The data show that GA patients at their first encounter mary endpoints in a phase 1 clinical trial, with no treatment-
have useful vision that may be preserved if an effective related adverse events, according to a poster presentation at
treatment were available. The progressive loss of visual acu- the AAO meeting.
ity observed in this study over a 2-year period underscores In four ascending doses of a single intravitreal injection of
the urgent need for a therapy to slow disease progression,” GEM103 (Gemini Therapeutics) there were no dose-limiting
said Ehsan Rahimy, MD, who presented the findings at a toxicities, and all doses were well tolerated, according to pre-
late-breaking paper session. senter Arshad M. Khanani, MD, MA. In addition, visual acuity
The analysis of data from the AAO’s IRIS Registry was was generally maintained or improved in the majority of
conducted in collaboration with Apellis Pharmaceuticals, patients with advanced central GA in the open-label study.
the data analysis firm Verana Health, and the AAO. Apellis is Gemini is now evaluating GEM103 in the phase 2a
developing pegcetacoplan, a targeted C3 therapy currently in ReGAtta clinical trial, a multicenter, open-label, multiple-
phase 3 clinical studies in patients with GA. dose escalation study in patients with GA secondary to dry
At 12 months, progression from GA to new-onset wet AMD AMD, the company said in a press release.
was seen in 4.7% of patients with bilateral GA and 13.3% of
patients with wet AMD in the contralateral eye. At 24 months,
progression was seen in 8.2% and 21.6% of patients with bilat-
eral GA and wet AMD in the contralateral eye, respectively.
VITRECTOR HANDLE DESIGNED
Of note, a large proportion of patients with GA did not TO IMPROVE DEXTERITY
return for follow-up at 2 years. Of the patients potentially A new vitrector handle for use on Alcon’s vitrectomy plat-
eligible for inclusion in the analysis, only 40% had a 2-year form was introduced during the 2020 AAO Virtual Annual
follow-up visit. Meeting. The Finesse Reflex handle is designed to help sur-
geons move with ease, providing unrestricted movement
DATABASE PROVIDES INSIGHTS ON RISK and focused performance, according to the company.
Part of the Greishaber line of instrumentation for vit-
FACTORS FOR RETINAL VASCULITIS WITH reoretinal surgery, the handle provides improved surgical
dexterity with advanced ergonomic support and expanded
ANTI-VEGF AGENT extraocular working space during vitreoretinal surgery, the
In 12,000 patients identified in the AAO’s IRIS Registry, the company said in a press release before the meeting. The
highest observed risk for experiencing retinal vasculitis (RV) ultralight-weight handle features stiff 25- and 27-gauge
and/or retinal vascular occlusion (RO) in the 6 months after needle shafts for maneuverability and precision performance
first treatment with brolucizumab (Beovu, Novartis) was during ophthalmic surgery. n
NOVEMBER/DECEMBER 2020 | RETINA TODAY 11
1120RT_News.indd 11 12/4/20 3:48 PMs MEETING MINUTES
PEDIATRIC RETINAL DETACHMENTS
REQUIRE DIFFERENT STRATEGIES
Each year, the Aspen Retinal Detachment Society (ARDS) hears from a select group of highly distinguished speakers.
In several of our past meetings, we have made sure to reserve time on the podium to discuss pediatric retinal care.
ARDS leadership knows that most retina conferences give little attention to pediatric retina care. The reasons
are obvious: Pediatric retina is a sub-subspecialty of eye care, and dedicating valuable podium time on an other-
wise filled agenda to a discipline that only a small subset of attendees may practice could be unwise.
Still, we know our attendees. ARDS participants’ hunger for learning deeply about a number of subjects is not limited to the topics
that pertain most immediately to them and their practices. They’re polymaths. They know that rounding out their retina education
gives them a more holistic sense of the space. And hey, you never know when those pediatric retina pearls will come in handy.
Be sure to keep an eye on MedConfs.com for the latest updates about ARDS 2021 and our focus on an in-person meeting.
—Timothy G. Murray, MD, MBA
BEST APPROACHES FOR PEDIATRIC RETINAL DETACHMENTS
RD, and trauma are important to fetal vasculature (PFV) with central reti-
document. Pediatric examinations can nal stalk lines, or peripheral retinal folds
be made more challenging due to lack in retinopathy of prematurity (ROP).
of cooperation, difficulty with drop The short system has the advantage of
administration, and poor dilation. providing a trocar with no cannula.
Presentation by Philip J. Ferrone, MD For babies less than 1 year old, exami- Pediatric eye anatomy varies from
Summarized by Abdallah Mahrous, MD nation can be made easier by having that of adults. The pars plana–pars
At this year’s ARDS meeting, Philip the patient lie on a parent’s lap with the plicata complex extends on average
J. Ferrone, MD, provided a rundown of head by the knees and feet up to the for 1.87 mm posterior to the limbus
surgical considerations for pediatric reti- parent’s chest, while the parent helps at 40 weeks; therefore, introducing
nal detachments (RDs). He emphasized stabilize the baby by holding his or her the cannulas at 1 mm from the lim-
the important point that the anatomy head. For uncooperative children up to bus is appropriate for a term baby. By
of pediatric eyes is different from the 8 years of age, you can ask the parent 6 months, the pars plana–pars plicata
anatomy of adult eyes, and he discussed to bear-hug the child while an assis- complex extends for approximately
the best approaches to use in a variety tant holds the head and the physician 3 mm posterior to the limbus, so a
of presentations. This article summa- attempts to pry the eyelids open and trocar incision at 1.5 to 2.0 mm from
rizes portions of his presentation. examine. If this approach fails, examina- the limbus is appropriate for that age.
tion under anesthesia is often necessary. The eye’s anatomy continues to
HISTORY AND EXAMINATION TIPS Stickler detachments are often com- change with the child’s growth. The
Dr. Ferrone reported that pediatric plicated, with a redetachment rate of axial length increases by approximately
RDs have an incidence of 0.53 per 45% due to proliferative vitreoretinop- 1.5 mm during the first 12 weeks of
100,000, compared with an inci- athy (PVR). By contrast, non-Stickler life. The eye grows on average 2 mm
dence of 12 per 100,000 in the adult RDs often behave more like adult RDs over the first 2 years of life and then
population.1 Tractional RDs are even with more promising results. another 2 mm from 2 years to 5 years.
less common in children. RDs are Between 5 years and 15 years the eye
sometimes challenging to diagnose in SURGICAL APPROACHES typically grows another 3 mm. After
children, and they can present late or The standard Alcon kit for 25-gauge 15 years of age, there is typically no
with other signs such as strabismus. vitrectomy can often be used for com- significant growth.2 It is important
History is important, even in older mon pediatric RDs. Use of the special to take this progression into account
children—details such as a baby’s Alcon short 25-gauge instrumentation when scleral buckle surgery is con-
birth weight, a history of prematurity, can be helpful in cases such as microph- sidered and when you are placing
or a family history of eye disease or thalmic eyes, or eyes with persistent sclerotomy wounds.
12 RETINA TODAY | NOVEMBER/DECEMBER 2020
1120RT_Meeting Minutes_ARDS_Imaging_Paulose.indd 12 12/4/20 4:04 PMMEETING MINUTES
s
Eyetube Meeting Coverage at Aspen Retinal Detachment Society
Each year, the Society invites Eyetube to cover selected talks from the year’s agenda.
ARTIFICIAL INTELLIGENCE AND PEDIATRIC RETINA SUBRETINAL GENE THERAPY
R.V. Paul Chan, MD, discusses how applying AI to pediatric patients aids in Christina Weng, MD, MBA, gives insight into ongoing subretinal gene therapy
diagnosing conditions such as plus disease by characterizing and monitoring pipeline candidates, specifically voretigene neparvovec for patients with a
disease activity. mutation of the RPE65 gene.
BIT.LY/ARDSCHAN BIT.LY/ARDSWENG
BEST APPROACHES FOR PEDIATRIC RD NEUROPROTECTION FOR THE TREATMENT OF THE RETINA
Philip J. Ferrone, MD, discusses how to properly care for and diagnose pediatric Baruch Kuppermann, MD, PhD, discusses unmet needs in conditions such
patients. Dr. Ferrone discusses how fundus autofluorescence, OCT, and other as retinal detachment, geographic atrophy, and dry AMD and what the right
in-office imaging modalities can be used to obtain the best and most accurate pathway may be for neural protection and enhancement.
imaging results.
BIT.LY/ARDSFERRONE BIT.LY/ARDSKUPPERMANN
Want to see the whole video collection? Head to bit.ly/ARDS2020.
CASE-BY-CASE CONSIDERATIONS these RDs often requires time and lasered. If not treated, these areas can
Pediatric RDs should be approached patience. They might require multiple lead to dense preretinal proliferation
on a case-by-case basis. Retinal dialysis surgeries, with relaxing retinectomies with high-ridged retinal folds. The folds
should preferably be buckled using a and silicone oil. must be carefully dissected, taking care
low and broad approach, as opposed Familial exudative vitreoretinopathy not to create any retinal breaks, which
to a high and narrow one. Stickler (FEVR) may present with a normal would be very difficult to repair.
detachments, as previously men- appearing fundus, but fluorescein Mutations in KIF11 can cause micro-
tioned, are highly proliferative with angiography can reveal large areas of cephaly, microphthalmia, and con-
high redetachment rates. Addressing peripheral nonperfusion that can be (Continued on page 15)
NOVEMBER/DECEMBER 2020 | RETINA TODAY 13
1120RT_Meeting Minutes_ARDS_Imaging_Paulose.indd 13 12/4/20 4:04 PMs IMAGING
DOUBLE TROUBLE: A TALE OF TWO
INTRAOCULAR FOREIGN BODIES
Imaging might be wise, even when one object is clearly visible.
BY REMYA MAREEN PAULOSE, MBBS, DNB, FLVPEI, FICO, FAICO, AND
THOMAS CHERIAN, MS, FLVPEI
I
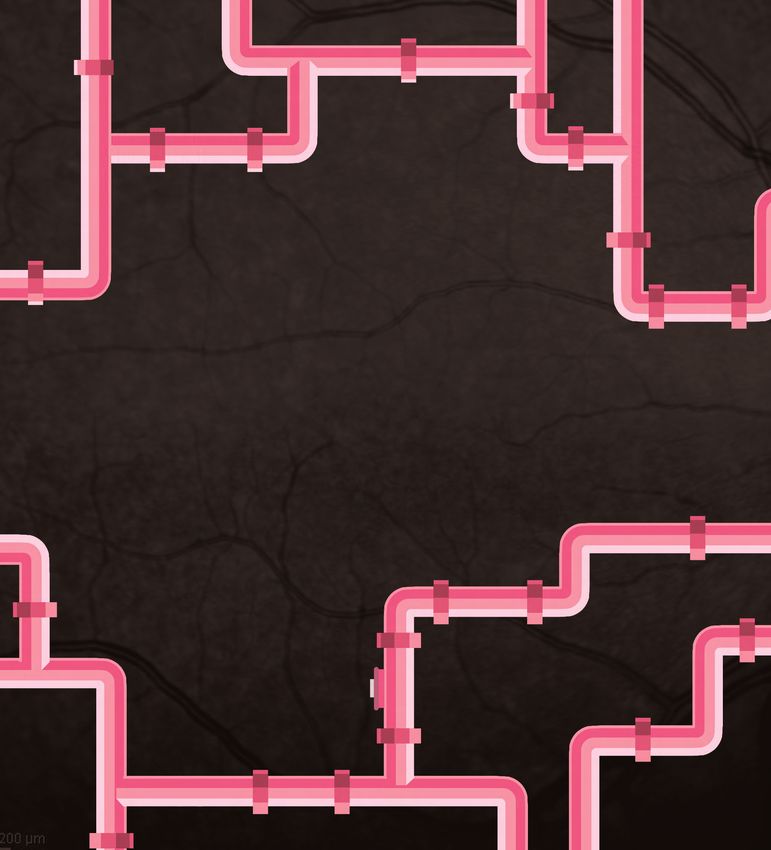
ntraocular foreign body (IOFB) injuries may result in a wide CASE
range of pathology and visual outcomes. Metallic IOFBs are A healthy 24-year-old man presented urgently with a
often associated with high velocity, and once they penetrate penetrating corneoscleral injury of the right eye following a
the cornea, they tend to enter the posterior segment.1-3 reported history of a high-velocity projectile resulting from
Additionally, IOFBs may present with varied clinical aspects hammering a nail. He complained of poor vision, pain, and
that may limit their detection, and symptoms may only redness in the right eye.
become apparent after a prolonged period of time. His visual acuity was light perception in the right eye and
However, in cases of visible IOFB, there are no clear guide- 20/20 in the left. In the right eye, the conjunctiva was con-
lines regarding the need for additional imaging. gested with a full thickness corneoscleral tear at 4 o’clock,
This report describes a unique case of a single penetrating extending 3 mm onto the cornea and 5 mm radially onto the
wound with two metallic IOFBs, one of which would have sclera. The anterior chamber was shallow, and the pupil was
been overlooked on a cursory clinical examination. It high- mid-dilated with a relative afferent pupillary defect. Although
lights the need for suspicion of additional foreign bodies even a rosette cataract was present, the fundus could be visualized,
if one IOFB is clinically evident. showing a metallic IOFB embedded on the retina inferonasally
A B
C D
Figure: Fundus imaging reveals a large macular tear caused by a high-velocity impact (A). Note the large visible metallic IOFB on the inferonasal retina (B). A second IOFB, hidden in
the inferonasal periphery, was localized with the help of a CT scan (C); the CT scan helped to localize the anterior smaller foreign body (left), while the larger foreign body is visible
in a posterior scan (right). The larger visible foreign body was brought into the anterior chamber (left), and the smaller anterior foreign body in the periphery was localized with
scleral indentation (right) (D).
14 RETINA TODAY | NOVEMBER/DECEMBER 2020
1120RT_Meeting Minutes_ARDS_Imaging_Paulose.indd 14 12/7/20 9:20 AMIMAGING MEETING MINUTES
s
s
(Figure, A). The macula showed a large retinal tear with an (Continued from page 13)
overlying hemorrhage (Figure, B). genital retinal folds. Fluorescein studies may show peripheral
The patient underwent fundus photography and emer- nonperfusion as well. Retinal folds can sometimes have stalks
gency CT scan as per institution protocol. To our surprise, that connect to the lens. The preferred surgical approach in
CT imaging revealed two separate IOFBs in the inferonasal these eyes is to use the short 25-gauge instruments, cutting
aspect of the right eye (Figure, C). the stalk anteriorly to free up the retina and letting it settle
The patient was scheduled for emergency 25-gauge pars back down to a more normal anatomy, then approaching
plana vitrectomy and pars plana lensectomy with anterior the rest of the retinal folds.
capsulotomy. Posterior vitreous detachment nasally helped to Optic pit RDs can sometimes self-resolve if given time;
avoid the extension of the macular tear. After vitrectomy, the however, in cases that require surgery it is recommended
larger of the two foreign bodies was removed through a clear to remove the vitreous stalk that goes right into the optic
corneal incision, while a thorough search with scleral indenta- pit, followed by application of light intraoperative laser
tion localized the second IOFB in the peripheral retina close to around the pit.
the ora (Figure, D). The second one was removed in a similar In Coats disease, the pathognomonic telangiectatic
manner. Cryotherapy was applied to the peripheral break, fol- vessels are often accompanied by RDs. In these eyes, it is
lowed by silicone oil tamponade. After silicone oil removal at better to drain the subretinal fluid externally and apply
3 months postoperatively, visual acuity improved to counting extensive laser to the telangiectatic vessels; this might not
fingers at 3 m with attached retina and scarring at the macula. provide ideal results but will preserve any vision possible.
Colobomas can present with very challenging RDs.
DISCUSSION Silicone oil is preferred in these eyes, but even with oil
The identification of an additional foreign body can be chal- there are often redetachments due to the complexity of
lenging when the level of suspicion is low, as can be the case the retinal layers in the coloboma. Platelet-rich plasma can
when one IOFB is clinically visible. General consensus is lacking be helpful in these cases.
regarding the need for imaging in cases with visible IOFB.
In one interventional case series of 69 eyes with IOFBs, CONCLUSION
17 eyes had no imaging when the IOFB was easily visualized.1 Pediatric RDs are different from RDs in adults.
The researchers also reported that two eyes had an additional Children’s eyes have a different anatomy that requires
IOFB identified on radiological evaluation. Thus, the authors modification of surgical approaches. With the correct
recommended radiologic imaging even when an IOFB is approach and patience, excellent visual and anatomic
clearly visible on clinical examination. A retrospective review results are still possible. n
of imaging techniques in IOFB cases demonstrated the superi-
1. Nuzzi R, Lavia C, Spinetta R. Paediatric retinal detachment: a review. Int J Ophthalmol. 2017;10(10):1592-1603.
ority of CT scan over other methods.4 2. Maldonado RS, Izatt JA, Sarin N, et al. Optimizing hand-held spectral domain optical coherence tomography imaging for
To the best of our knowledge, this is a unique report of two neonates, infants, and children. Invest Ophthalmol Vis Sci. 2010;51(5):2678-85.
metallic IOFBs from a single entry site caused by a hammering
accident. I speculate that the force of the IOFB’s impact on
the macula may have caused the IOFB to split in two inside CORRESPONDING AUTHOR ABDALLAH MAHROUS, MD
the eye. This case highlights the need for suspicion and imag- nV itreo-Retinal Surgery Fellow, Weill Cornell Medicine, New York
ing for additional IOFBs in the event of high velocity projectile n a mahrus89@gmail.com
injuries, even when one IOFB is clinically evident. n nF inancial disclosure: None
1. Woodcock MG, Scott RA, Huntbach J, Kirkby GR. Mass and shape as factors in intraocular foreign body injuries. Ophthalmology. 2006;113(12):2262-2269.
2. Roper-Hall MJ. Review of 555 cases of intra-ocular foreign body with special reference to prognosis. Br J Ophthalmol. 1954;38:65-99.
PHILIP J. FERRONE, MD
3. Percival SP. A decade of intraocular foreign bodies. Br J Ophthalmol. 1972;56:454-461. nR etinal Surgeon, Long Island Vitreoretinal Consultants, Great Neck, New York
4. Nie S, Wang Z, Liu W, Liang X. Clinical application of X-ray, B-scan, and CT in the diagnosis of ocular foreign bodies. Eye Sci. 2013;28(1):11-4. nF inancial disclosure: None acknowledged
THOMAS CHERIAN, MS, FLVPEI
n Vitreoretinal Consultant, Little Flower Hospital and Research Center, Angamaly, Kerala, India
n Financial disclosure: None
REMYA MAREEN PAULOSE, MBBS, DNB, FLVPEI, FICO, FAICO
n Vitreoretinal Consultant, Little Flower Hospital and Research Center, Angamaly, Kerala, India
n r emyapaulose@gmail.com
n Financial disclosure: None
NOVEMBER/DECEMBER 2020 | RETINA TODAY 15
1120RT_Meeting Minutes_ARDS_Imaging_Paulose.indd 15 12/4/20 4:05 PMs MEDICAL RETINA
LONG-TERM INFLAMMATION CONTROL
BENEFITS ALL TYPES OF UVEITIS
Preventing flare-ups is essential in the pandemic era.
BY ROBERT C. WANG, MD
U
veitis is a multifaceted disease dose of steroid. with systemic methotrexate and had
that strikes in different ways, but As the following case studies illus- been using topical prednisolone ace-
the goal of treatment is always trate, a thorough evaluation of the tate in the right eye for the 2 months
the same: to achieve quiescence patient’s clinical presentation and medi- before presentation (Figure 1).
with the fewest possible side cal history guide the development of a
effects. Whether a patient presents well-suited uveitis treatment regimen, Treatment Course
with iritis, panuveitis, or uveitis with and frequent monitoring makes it pos- I started the patient on topical
systemic disease association, the retina sible to change course when necessary. 0.05% difluprednate ophthalmic emul-
specialist’s objective is to eradicate sion (Durezol, Alcon) as a bridge to
vision-threatening inflammation and CASE 1: ANTERIOR UVEITIS initiation of systemic adalimumab
quell potential flares. To that end, we Presentation (Humira, AbbVie). With the topical
have an increasingly sophisticated arse- A 9-year-old White child was treatment, the CME improved greatly,
nal of tools from which to choose. brought to the clinic for evaluation although the patient developed a mild
By the time patients with noninfec- and treatment. The patient had a his- steroid-induced IOP response, with
tious uveitis reach my clinic, they have tory of psoriatic arthritis and decreased elevation to 27 mm Hg.
typically been treated unsuccessfully vision in her right eye. She presented I replaced the difluprednate with
with oral steroids and are then candi- with rebound iritis and worsening 0.5% loteprednol etabonate ophthal-
dates for systemic immunosuppres- vision. The most common causes of mic suspension (Lotemax, Bausch
sives or intraocular corticosteroids. vision loss in pediatric patients with + Lomb) and gradually tapered
Options at this point include the bio- anterior uveitis are cataract, band kera- the loteprednol to one drop daily.
erodible 0.7 mg dexamethasone intra- topathy, glaucoma, and cystoid macu- Adalimumab was started 2 weeks
vitreal implant (Ozurdex, Allergan); the lar edema (CME). after the loteprednol taper, result-
surgically placed 0.59 mg fluocinolone On presentation, the patient’s VA ing in resolution of most of the CME.
acetonide intravitreal implant (Retisert, was 20/40 OD and 20/20 OS, and OCT The patient’s IOP returned to normal
Bausch + Lomb); and the inject- documented CME in the right eye. The (11 mm Hg) and visual acuity stabilized
able 0.18 mg fluocinolone acetonide patient had been treated on and off at 20/25 (Figure 2).
intravitreal implant (Yutiq, EyePoint
Pharmaceuticals).
When appropriate, I am partial to AT A GLANCE
the newest option, the 0.18 mg fluocin-
olone acetonide intravitreal implant, T he goal of uveitis treatment is to achieve quiescence with the fewest
s
because it is a low-dose implant that possible side effects.
lasts up to 3 years. I’ve treated many
patients with it who have then expe- A number of implantable posterior segment steroid options exist for
s
rienced long-term quiescence and few
side effects. The 0.59 mg fluocinolone
local control of inflammation.
acetonide intravitreal implant is also
Ongoing coverage is a chief advantage of an implantable corticosteroid.
s
an excellent option, but it requires sur-
gical placement and delivers a higher
16 RETINA TODAY | NOVEMBER/DECEMBER 2020
1120RT_MedicalRetina_Oncology.indd 16 12/4/20 4:09 PMMEDICAL RETINA
s
Figure 1. The Case 1 patient’s OCT shows CME secondary to chronic iritis in the right eye (left panels), normal left eye.
Figure 2. The Case 1 patient’s OCT demonstrates resolution of CME in the right eye.
Current Status At that point, it was clear to me that the patient’s disease
Ten months after initiation of adalimumab, the patient’s would continue to flare without a move to local therapy. I placed
visual acuity remains 20/25 OD and 20/20 OS with normal a 0.7 mg dexamethasone intravitreal implant in the vitreous,
IOP and no recurrence of inflammation or CME. after which the inflammation improved rapidly. This implant is
expected to last up to 6 months, but I often find that its efficacy
CASE 2: PANUVEITIS wanes by about month 3, and pharmacokinetic data supports
Presentation that observation.2
A 72-year-old White woman presented with panuveitis I discussed with the patient the possibility of implanting
secondary to birdshot chorioretinopathy positive for histo- the 0.59 mg fluocinolone acetonide intravitreal implant,
compatibility leukocyte antigen (HLA)-A29. Birdshot cho- but the patient was concerned about a higher incidence of
rioretinopathy is a rare form of chronic bilateral posterior glaucoma with this treatment in patients with birdshot cho-
uveitis. Despite its distinctive clinical phenotype and associa- rioretinopathy.3 In addition, the anticipated out-of-pocket
tion with HLA-A29, delays in diagnosis and treatment are cost was beyond her means. Instead, she elected to repeat
common, sometimes resulting in significant visual loss.1 the dexamethasone implant every 3 months for nine more
treatments.
Treatment Course The 0.18 mg fluocinolone acetonide intravitreal implant sub-
Because birdshot chorioretinopathy is thought to have an sequently became available. The patient was amenable to trying
autoimmune etiology, therapy aims to regulate the body’s it when I explained that it would be implanted in an outpatient
immune response. I started the patient on oral prednisone procedure under topical anesthesia, that it would last for 3 years,
and 50 mg of the antimetabolite azathioprine (Imuran, and that the reimbursement would be favorable.
GlaxoSmithKline) three times daily. I began a taper of the
oral steroids, and the patient achieved quiescence, but Current Status
4 months later she developed a recurrence of inflammation. I placed the 0.18 mg fluocinolone acetonide intravitreal
At that time, I initiated a pulse of oral steroids, which implant bilaterally in December 2019. Since then, her eyes
calmed the inflammation, and I prescribed 150 mg of aza- have remained quiet with no other therapy needed.
thioprine and 5 mg of prednisone daily for maintenance
therapy. However, she again developed a flare 3 months later. CASE 3: UVEITIS WITH SYSTEMIC ASSOCIATION
We attempted to enroll her in a clinical trial of adalimumab, Presentation
but the study had reached its closeout date. I consulted with A 74-year-old White man presented with bilateral
rheumatology, intending to initiate systemic biologic thera- nyctalopia and vision loss. The patient had a history of
py. With no other systemic diagnosis, however, the patient’s autoimmune neuropathy predominantly affecting his right
insurance carrier would not approve any therapy. leg and, to a lesser degree, his left leg and both hands. He also
I increased the dose of azathioprine to 200 mg daily, but had hearing loss, with cochlear implants bilaterally, and he
the patient still demonstrated inflammation on exam. Next, I was being treated with azathioprine for Sjögren syndrome. On
switched her to a daily regimen of 3,000 mg of mycophenolate examination, he had 20/20 VA OU and normal retina findings
mofetil (CellCept, Genentech) and initiated another steroid but very constricted visual fields bilaterally.
pulse. Despite the switch, the inflammation flared once again. (Continued on page 21)
NOVEMBER/DECEMBER 2020 | RETINA TODAY 17
1120RT_MedicalRetina_Oncology.indd 17 12/4/20 4:09 PMYou can also read