Tossicità renale da Immune checkpoint inhibitors - Patrizia Giannatempo - Aiom
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Tossicità renale
da Immune
checkpoint
inhibitors
Patrizia Giannatempo
Fondazione IRCCS Istituto Nazionale
dei Tumori, Milano, Italy
Disclosures Co‐Investigator in IMvigor210, IMvigor211, CA209‐275, MK‐3475‐045, DANUBE trials

Typical patient with Typical clinical trial bladder cancer participant
Renal dysfunction is common in
patients with urothelial cancer
Proportion of patients deemed ineligible (i.e. creatine clarance
< 60 min/ml) by the Cockroft‐Gault formula by age group
Dash et al, Cancer, 2006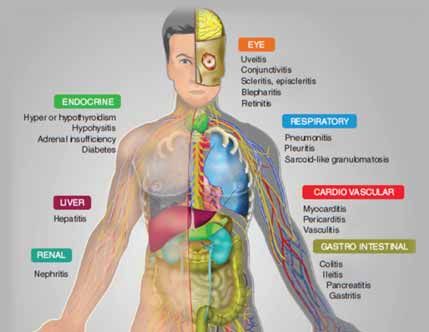
The burden of cancer is shifting to the
elderly
3.0
2.5 85
2.0
75–84
1.5
65–74
0.5 50–64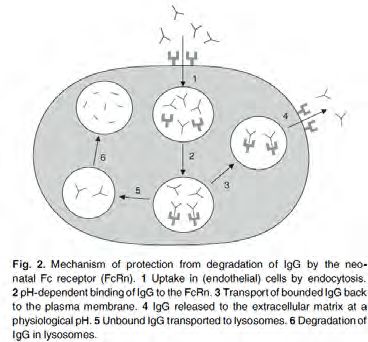
Immunotherapy
and
kidney failure
Metabolism and Elimination of
Therapeutic Monoclonal Antibodies
• mAbs are metabolized to peptides
and amino acids in several tissues,
by circulating reticuloendothelial
system (RES=macrophages and
monocytes)
• Antibodies and endogenous
immunoglobulins are protected
from degradation by binding to
protective receptors (the neonatal
Fc‐receptor [FcRn]), which explains
their long elimination half‐lives (up
Keizer RJ et al., Clin Pharma 2010
to 4 weeks). Tabrizi MA et al., DDT 2006
Lammerts van Bueren JJ et a., Cancer Res 2006
Duconge J et al., Drug Metab Pharmacokinet 2002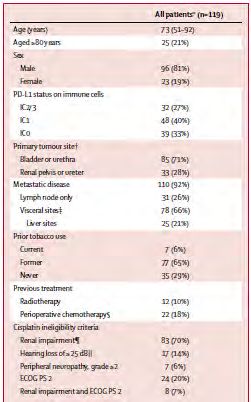
Pharmacokinetics of Therapeutic
Monoclonal Antibodies
• intracellular metabolism and be reduced to
small endogenous amino acids
• GFR 15 mL / min / 1.73 m (2) or higher has no
effect on the clearance compared to normal
renal function
Keizer RJ et al., Clin Pharma 2010
Tabrizi MA et al., DDT 2006
Lammerts van Bueren JJ et a., Cancer Res 2006
Duconge J et al., Drug Metab Pharmacokinet 2002
Quanto riportato in RCP
Nivolumab:
• Non sono state riscontrate differenze clinicamente
importanti nella clearance di nivolumab tra pazienti
con compromissione renale lieve(GFR < 90 e ≥ 60
mL/min/1,73 m2; n = 379) moderata (GFR < 60 e ≥
30 mL/min/1,73 m2; n = 179) e pazienti con
funzionalità renale normale.
• I dati su pazienti con compromissione renale severa
(GFR < 30 e ≥ 15 mL/min/1,73 m2; n = 2) sono
troppo limitati per poter trarre delle conclusioni in
questa popolazione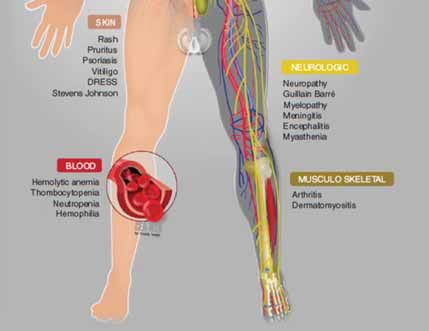
Quanto riportato in RCP
Pembrolizumab
“Non è necessario alcun aggiustamento della
dose nei pazienti con danno renale lieve o
moderato. KEYTRUDA non è stato studiato in
pazienti con danno renale graveImmunotherapy and renal
impairment
• Ipilimumab/Nivolumab/Pembrolizumab :
– Currently approved ICBs have not been evaluated
in patients with severe renal impairment
– No dose adjustment is recommended for patients
with mild or moderate renal impairment (i.e. ≥30
ml/min creatinine clearance)
• Clinical and pharmacokinetic data with pre‐
existing severe renal impairment are limitedUso compassionevole Atezolizumab
inel carcinoma uroteliale (II linea)
• …..
• …..
• …..
• Pazienti con adeguata funzionalità renale
• …..GFR>15 mL/min/1,73 m2Immune checkpoint
antibodies:
Renal toxicityCase Report
• 78‐year‐old man was hospitalized for acute kidney injury
• Metastatic (bone, lung and lymph nodes) melanoma was
diagnosed on February 2012
• Ipilimumab 10 mg/Kg every 3 weeks RT (6 Gys in 3
fractions on one axillarymetastatic lymph node)
• 5 days after the 2nd injection, the patient experienced
fatigue, anorexia, mild diarrhea and a grade 3 rashes.
Ipilimumab was discontinued.
• Body temperature = 38.5 °C
• blood pressure = 120/80 mm Hg
Izzedine H. et al.,Invest New Drugs 2014Case Report • Progressive renal failure was observed 1 week • Blood examination: – leucocytes 11,450/mm3 with eosinophils 2,300/mm3 – urine proteins (0.3 g in a 24 h collection) – 35.5 leucocytes per high‐power field – negative urinary cultures • Serum creatinine from 0.68 to 2.33 mg/dl (creatinine clearance 28 ml/min versus 84 ml/min at baseline) • Hepatitis B and C serology, anti‐nuclear antibody, antineutrophil cytplasmic antibodies (ANCAs) and antiglomerular basement antibodies were negative
Case Report
• Septic screening was negative, no volume depletion,
hemodynamic stress, nor administration of nephrotoxic
medications neither radio contrast, urinary Bence Jones
protein was negative.
• Renal ultrasound showed enlarged, swollen kidneys without
dilated pyelocaliceal cavities.
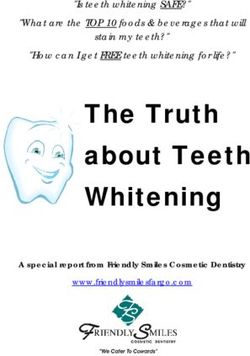
• A percutaneous renal biopsy was performed.
– Severe interstitial inflammation + edema + polynuclear
infiltration in glomerularCase Report • Oral prednisone at a dose of 1 mg/kg for 4 weeks, followed by fast tapering. • Serum creatinine level fell to 1.0 mg/dl over the next 2 weeks without dialysis and urinary leucocytes disappeared. • His rash had completely resolved and the rest of medical examination was within normal limits. • Staging showed a 40 % tumor reduction
Immuno‐related nephritis: symptoms
• Mainly asymptomatic laboratory findings
– Elevated creatinine and blood urea nitrogen (BUN)
levels
• Change in urine output, proteinuria, flank pain,
and edema may be symptoms of renal failure
• Fever may occur
• In some case + other immune‐related AE
• Appears much later, after 14–42 weeks on
immunotherapy Naidoo J,et al. Ann Oncol.2015
Kodner CM el al. Am Fam Physician 2003
Izzedine H et al. Invest New Drugs. 2014
Voskens CJ et al. Plos One 2013Differential diagnosis of immuno‐
related nephritis
• Acute deydration from fluid loss (eg. Diarrhea, CT‐
induced)
• Infection
• Physical obstruction
• Tumor progression in kidney and/or metastatic
disease
• Autoimmune disease (e.g LES, sarcoidosis)
• Vascular etiologies
• Metabolic abnormalities (e.g. diabetes)
Kodner CM et al.Am Fam Physician. 2003
Rahman M, et al. Am Fam Physician. 2012Differential diagnosis of immuno‐
related nephritis
• Infectious etiologies
– fever, chilling, nausea, vomiting, pos urine
cultures or viral serology
• Obstruction Hydronephrosis
• PD in kidney CT scan
• Autoimmune disease Ab (ANAs …)
• Vascular etiologies
– livedo reticularis, abdominal bruits, funduscopic
abnormalities
• Immuno‐related asymptomatic, mild proteinuria,
gradually increasing creatinine, rashDiagnosis of immuno‐related nephritis: • Clinical assessment (vital signs, hydratation status, hypotension …) • Laboratory finding: – GFR – Urinalysis – Complete blood count – Urine colture and viral serology (e.g.CMV, EBV) • Radiologic finding: – US and/or CT scans
Immuno checkpoint inhibitors and
Renal Failure
How many patients?
Ipilimumab Tremelimumab Nivolumab Pembro Atezo Durvalumab
Mechanism
CTLA‐4 CTLA‐4 PD‐1 PD‐L1 PD‐L1 PD‐L1
inhibitor inhibitor inhibitor inhibitor inhibitor inhibitor
Status FDA HL,
H&N, FDA H&N, FDA NSCLC,
FDA FDA
lung cancer, NSCLC, urothelial Under trial
melanoma mesothelioma
RCC, melanoma carcinoma
melanoma
Renal
failure
1 None 1‐3Patients (N = 350)
• Advanced urothelial
cancer Primary Endpoints
• No prior chemotherapy
Pembrolizumab
for metastatic disease 200 mg Q3W • ORR in all patients
• ECOG PS 0‐2 • ORR in patients with
• Ineligible for cisplatin PD‐L1–positive
based on ≥ 1 of the tumors
following:
– CrCl• Baseline characteristics:
– 70% (n= 83) pts with renal impairment
• GFR less than 60 mL/min and more than 30
mL/min
– 7%(n=8) pts with renal impairment + ECOG PS2
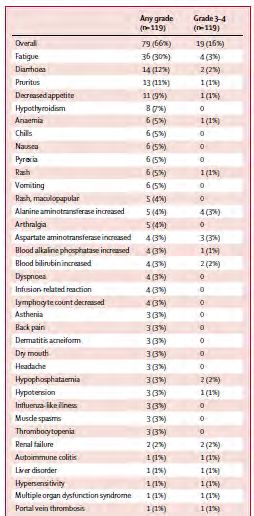
Treatment‐related adverse events:
Renal failure 2 (2%)Immune checkpoint inhibitors and Renal
Failure
How many patients?
• Durvalumab + Tremelimumab 2%
• Ipilumumab (lupus nephrititis or granulomatous
nephritis
• Nivolumab + platinum‐doublet chemo in NSCLC
phase I
Segal NH, et al. ESMO 2014.
Antonia S, et al. Lancet Oncol 2016.
Izzedine H, et al. Invest New Drugs 2014.
Thajudeen B, et al. AM J Ther 2015
Di Giacomo AM, et al. Cancer Immunol Immunother 2009.Treatment of immuno‐related
nephritis
• Steroids even for low‐grade events (Grade 2)
in order to prevent potential progression to
higher‐grade event
• Monitor:
– Routine urinalysis
– Elevated serum BUN and creatinine, GFR,
electrolyte imbalance, decrease in urine output,
proteinuriaImmuno‐related Nephritis Take home message • Most cases asymptomatically • Gradual increases in serum creatinine levels • Rule out other causes of elevated creatinine or acute failure • An early intervention can prevent worse or irreversible renal injury ‐‐ Steroids • Routine laboratory monitoring of kidney function at baseline, prior to each treatment, after treatment cessation
Thank you
patrizia.giannatempo@istitutotumori.mi.it
AIOM incontra SINYou can also read