Women with schizophrenia: what risk issues need to be considered in the perinatal period?
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Women with
schizophrenia:
what risk issues need to be
considered in the perinatal period?
Liz McDonald
January 2021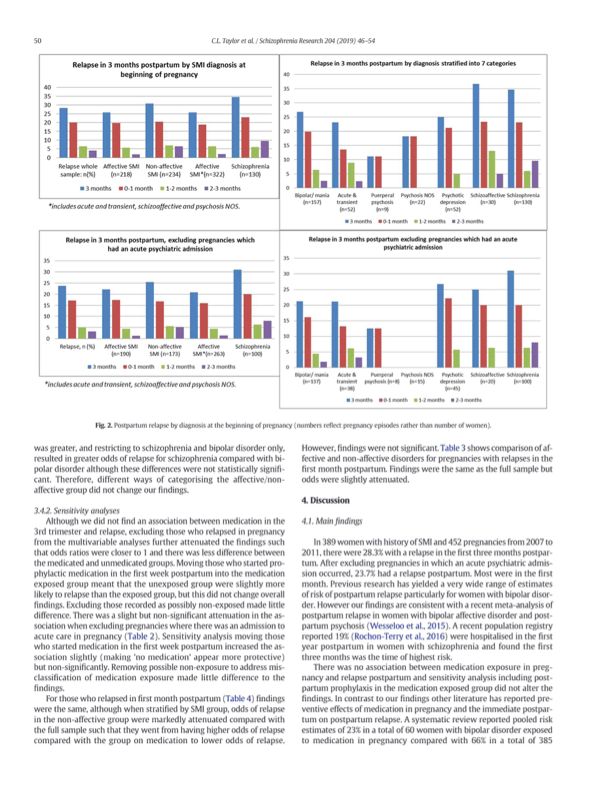
• Be though9ul about all women of childbearing age • Pre-concepAon counselling • Consider their sexual health, sexual acAvity, contracepAon, plans for pregnancy throughout contact • Pregnancy tests – do them!! Preconcep(on Toolkit www.healthylondon.org/resource/best-prac(ce-toolkit- for-providing-family-planning-advice-to-women-with-a- mental-illness/ Preconcep(on Interven(ons and Resources for Women with Serious Mental Illness: A Rapid Review. PHE 2020

The good physician treats the disease;
the great physician treats the patient
who has the disease.
William Osler 1849-1919
Question to the group What are the gender differences in schizophrenia that we have to consider?
Understand the gender differences
• Gender differences more apparent in younger women.
Psychosocial outcome ul8mately equal.
• Longer pre-psycho8c prodrome
• Longer diagnos8c delay
• More familial
• More schizoaffec8ve diagnoses
• Higher rates of comorbidity with other mental health
problems, (including depression, personality disorders, ea8ng
disorders and anxiety disorders)
• More self-harm and suicide aFempts (8.2% v 5.9%) though
less completed suicide. Suicide rate of 6% spread over 20
years.
• Differences in symptomatology
• Neuro-modulatory role of oestrogen
• Sex differences in pharmokine8cs, liver enzymes, renal
elimina8on and dopamine D2 receptor occupancy – eg lower
doses of Olanzapine and Clozapine
Sommer et al 2020 Seeman 2018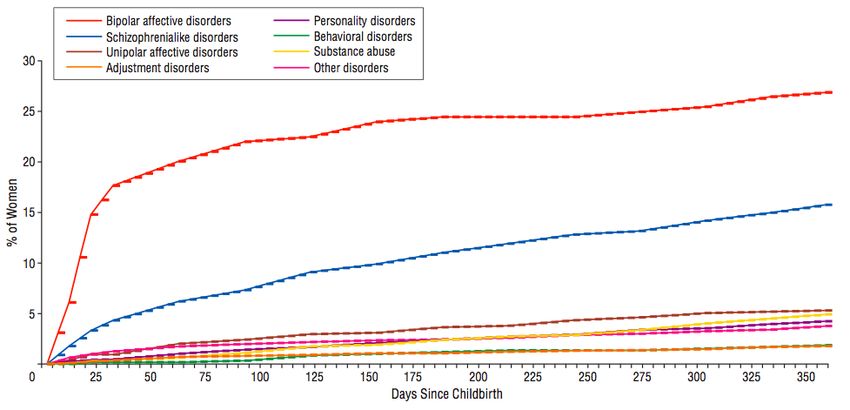
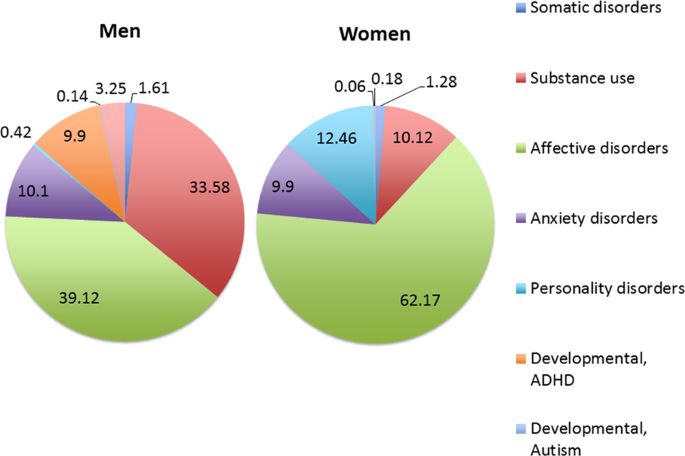
Gender difference of age of Last recorded non-psychotic disorder before hospitalisation for SSD, for those who had at onset less than previously least one prior hospitalisation. N=7,142 women, n=9006 men. Sommer et al, npj Schizophrenia, 2019 thought Eran7 et al, 2012

Last recorded non-psychotic disorder before hospitalisation for SSD, for those who had at least one prior hospitalisation. N=7,142 women, n=9006 men. Finnish register Sommer et al, npj Schizophrenia, 2019
Don’t forget that diagnoses can change over time and that there are very high rates of psychiatric co-morbidities in women with mental disorders.
Residual symptoms impair func3on and increase risk Do not undertreat or offer less effec3ve medica3on
Individuals with schizophrenia have a 2–3 fold increased standardised mortality ra@o- a sobering fact aptly described as ‘the scandal of premature mortality’. Thornicro( 2011
General health • More migraine, thyroid dysfunc8on, auto-immune disorders, tardive dyskinesia • Diet – malnourished with eg lack of folate, Fe, Calcium • Low Vit D • Lack of physical ac8vity, smoking, alcohol and other substances • Preventa8ve care: breast checks, cervical screening, dental care • Health consequences of weight gain, such as hypertension, diabetes, and heart disease. • Non-aFendance at appointments • Delay in diagnosis • Sub-op8mal treatment • Earlier death with more deaths from cancer
Gestational diabetes:
Oral glucose tolerance test at 24–28/40 in all
women taking antipsychotic medication in
pregnancy
1. NaEonal InsEtute
of Health and Care
Excellence (2014)
Clinical PracEce
Guideline 192
2. NaEonal InsEtute
for Health and Care
Excellence (2008)
Diabetes in
pregnancy. Clinical
PracEce Guideline 63.Women with schizophrenia Trauma Abuse Vic@misa@on S@gma Perpetra@on of violence
Schizophrenia: risk of relapse rises throughout the first postnatal year and is of a lower magnitude than that associated with BPAD. Munk-Olsen et al., 2006; Munk-Olsen et al.,2009 Risk is significantly increased if: • there is an admission in pregnancy • prior severity of illness • older (>35) • there is partner psychopathology • low socio-economic status • inconsistent MH care provider • Not having US scans pre-20/40 • discontinuing medication • overwhelming levels of stress, unique psychological, emotional and social pressures of becoming a mother including increased contact with health and social care professionals, disruption of routine • cognitive demands may also contribute to the increased rates of breakdown. • consistently documented that women with schizophrenia are at high risk of admission in pregnancy and postpartum and that early postpartum is the highest risk for admission across the whole perinatal period Vigod et al 2016
• n=389 hx of SMI Individual circumstances of the
• 452 pregnancies 2007-2011 woman matter:
• 28.3% relapsed in first 3/12 PP Recency of last admission and
admission in 2 years before
• 23.7% relapsed if no admission pregnancy
in pregnancy
Non-affective SMI – higher odds
• NO association with meds in late of relapse
pregnancy
Taylor et al, Schiz Res, 2019Prescribing for women: get more side-effects and more likely to report
them as being serious
• Physical aVrac@veness
• Femininity
• Health and well-being: weight gain, metabolic
syndrome, blurred vision, headache
• Emo@onal/ Psychological: general ‘dulling’,
sleepiness, poor concentra9on, fa9gue, lack of
emo9onal responsivity and availability, reduced
spontaneity, reduced affec9ve expression
• Social: s9gma, impairment of occupa9onal
func9on, impact on parental and caring roles and
responsibili9esPregnancy • ⬇ gastric emptying • ⬆ gastric ph • ⬆ cardiac output • ⬆ GFR • ⬆ body water • ⬆ body fat • ⬇ cytochrome P450 1A2 in 2nd and 3rd trimester
Careful risk-benefit analysis required regarding medica7on in pregnancy. Do not assume it is be
Neonatal outcome • Lower mean birth weight 15.8% • Pre-term birth 10.2% • NICU admission 24.3% • Link with episode of illness in pregnancy Boukakiou et al, 2019
Neonatal outcome Among infants of women with schizophrenia risk was higher: prematurity (11.4% vs. 6.9%) Apgar score < 8 at 1 (19.0% vs. 12.8%)and 5 min (5.6% vs. 3.0%) Smoking, fourfold more common among women with schizophrenia, was the variable that explained the greatest propor7on of the elevated aRR for prematurity (9.9%), SGA (28.7%), and Apgar < 8 at 1 and 5 min (9.8%, 5.6%). Illicit substance use, certain reproduc7ve history variables, and pregnancy complica7ons also contributed to the elevated aRR for preterm birth. • Conclusions: Elevated risks of preterm birth, SGA, and low Apgar scores in infants of women with schizophrenia are partly explained by poten7ally modifiable factors such as smoking and illicit drug use, sugges7ng opportuni7es for targeted interven7on. • Maternal schizophrenia and adverse birth outcomes: what mediates the risk? Vigod et al 2020
• The presence of schizophrenia is linked to poor socio- economic status, unwanted and unplanned pregnancy, lack of partner support, co-morbid illicit substance abuse, and poor nutri@on. These factors have been associated with poor prenatal care and pregnancy outcomes, independent of the presence of schizophrenia. • Gesta@onal diabetes, prematurity, IUGR – increase the risk of schizophrenia in exposed infants irrespec@ve of gene@c suscep@bility • SCZ – less antenatal care, higher rates of complica@ons • Improved antenatal care reduces adverse outcomes Lin 2009
Culture and ethnicity • Black BriDsh women are five Dmes more likely to die in childbirth than White BriDsh women (2018 MBRRACE- UK) • Black babies have a 121% increased risk of being sDllborn and a 50% increased risk of neonatal death compared to white babies (Government response to a pe
Focus on poten@ally reversible risk factors:
• Keep weight down
• Healthy diet, supplements, exercise
• Lowest effec@ve dose of AP
• Abstain from cigareVes, alcohol, other
substances
• Rapid treatment of infec@on and
inflamma@on
• Avoidance of stress
• Housing and other socio-economic issues
• Be not only gender-aware but also age-
awareHow do symptoms in
women with schizophrenia
affect maternal func3on?
Breakout groupsSymptoms: affect maternal sensitivity, responsiveness and competence
• Affec7ve symptoms
• When depressed have more nega7ve symptoms and aVempt suicide
• Anxiety
• Inappropriate and blunted affect
• Anhedonia
• Fa7gue
• Overt hos7lity
• Illogical thinking
• Domina7ng
• Sexual, jealousy, roman7c and soma7c delusions
• Emo7onal delusions
• Persecutory delusions: partner/family/infant/children
• Delusions that the birth did not occur, that the baby is dead, defec7ve, not
a real baby
• Lack of insight
• Need for solitudeWomen with schizophrenia may have varying degree of cognitive impairment, including: • Difficulties understanding information • Memory problems • Reduced concentration, attention, verbal memory • Impaired executive function • Unable to organise time effectively • Difficulties in prioritising and planning tasks • Difficulty discerning non-verbal cues • Recognising affects from facial expressions
Mutual social interac@ons with infants Misinterpre@ng the infant’s cues Touching and playing less with the infant Intrusive, insensi@ve, inappropriate interac@ons Difficulty dis@nguishing own needs from those of the infant May pose risks to their child’s development Gamer et al 1976
Planning pregnancy
• 1, 565 women with schizophrenia and 924,657 women
without who had at least one live birth during the study
period
• women with schizophrenia were younger (6.2% age 18-19
years, vs. 3.6%),
• lower income (38.7% in the lowest income quinGle, vs.
21.3%),
• had more stable (41.1% vs. 27.3%) and unstable chronic
medical condiGons (24.2% vs. 13.2%),
• had higher rates of substance use disorders (27.0% vs.
2.1%)
• 99 (6.3%) women with schizophrenia had a repeat
pregnancy within 12 months, compared to 36,065 (3.9%)
without schizophrenia
Gupta et al 2019How can mental health
teams best support women
of childbearing potential?
Breakout
groups• Educa&on re sexual health – contracep&on, infec&ons, pregnancy • Support access to family planning and maternity services • Understand her values and beliefs about femininity, pregnancy, motherhood, rela&onships, abuse • Maintaining capacity eg treat the illness, support problem-solving development • Don’t be afraid to support the protec&on of women when they are very vulnerable eg acute in-pa7ents, vic7ms of abuse
Principles of managing women with schizophrenia in the perinatal period • Understand the individual woman: who is she? what are her concerns? • Think about the partner, family and infant • Get the diagnosis right • Know her previous history and risks • What is her experience of illness, treatment and care, pregnancy, parenthood? • Ensure ease of access to both maternity and mental health care and prompt and effec
What are the risk issues?
Risk to her physical health due to pregnancy and
Risk to her mental health childbirth
• Untreated illness Risk to the fetus/infant
• Isolation/poor social support • MedicaEon
• Overwhelmed by challenges associated with having to negotiate • Untreated illness
with several teams and agencies • Specific symptoms
• Culture • LimitaEons to parenEng capacity and funcEon
• Stigma Risk to her future well-being
• Fear
• Grief
Risk from her her mental illness
• Symptoms
• Medication
• Impact on physical health
• Impact on her socioeconomic situation and environment
• Effects of non-disclosure/ poor engagement/ lack of insightYou can also read