2021 Primary Care Symposium Cardiometabolic Panel Discussion - James Smith MD Coastal Cardiology
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

2021 Primary Care Symposium
Cardiometabolic Panel Discussion
James Smith MD
Coastal Cardiology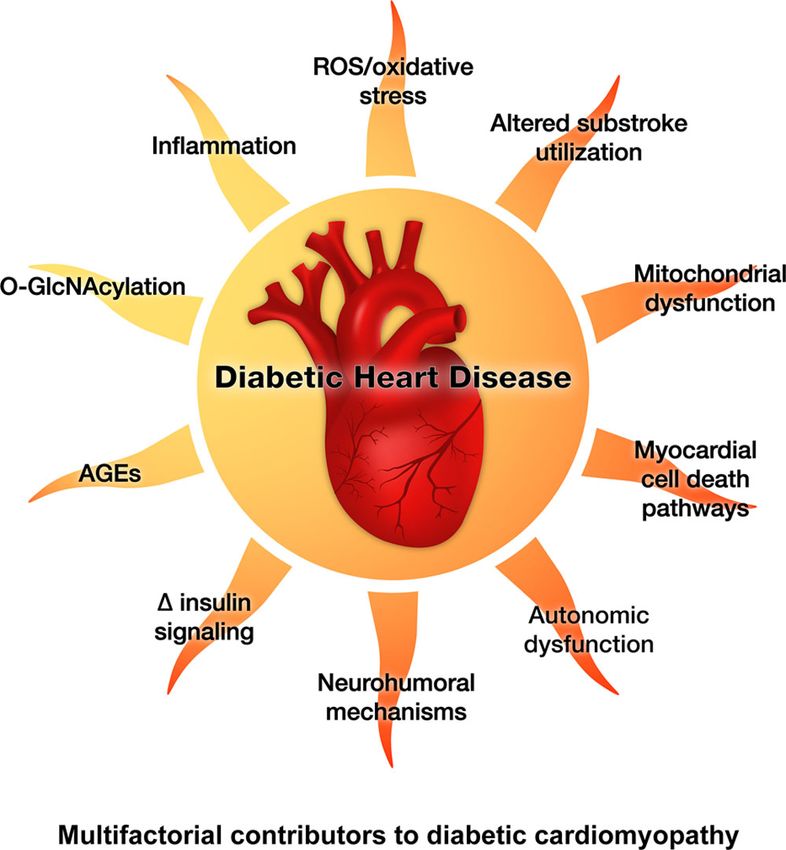
Prevalence • 425 million people worldwide • In 2010 the International Diabetes Federation prediction was “430 million by 2030”
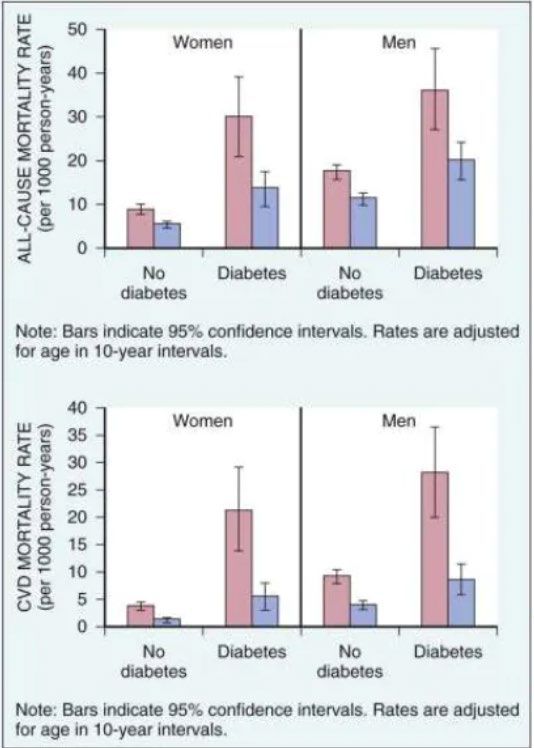
• Compared with non-diabetics, patients with diabetes have a twofold to fourfold increased risk for development and dying of CHD
More than just CHD • Twofold increase in stroke risk compared to non-diabetics • Sixfold increased risk for adverse outcomes after stroke • 1/3 of all patients with symptomatic PAD • Accounts for roughly 50% of all lower extremity amputations
More than just CHD
• Two to fivefold increased risk for heart
failure
• HFrEF
• HFpEF
• Worse outcomes
• Multifactorial
• Ischemic, metabolic, functional
myocardial perturbations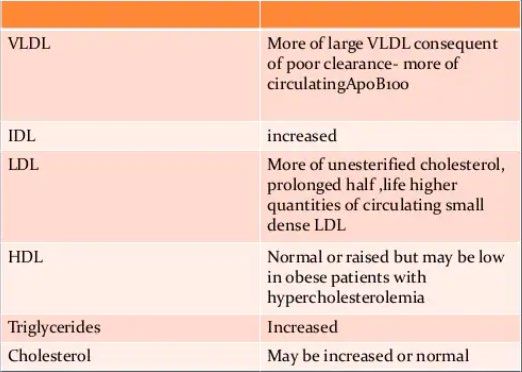
Lesion morphology • In atherectomy specimens of coronary cell rich areas, the extent of the necrotic plaque core, calcification and thrombus were increased in diabetics • Associated with formation of vulnerable plaques and plaque rupture • Post mortem studies demonstrate increased frequency of healed ruptures in patients with DM2 who died from acute coronary events
CAD • DM is considered a CAD equivalent • For patients with known CAD and diabetes, the rates of death approach 45% over 7 years • 75% over 10 years
Myocardial infarction • 50% are dead 5 years after an MI • 1 month mortality rate is 58% higher in diabetics than non-diabetics • The SHOCK (Should we emergently revascularize Occluded Coronaries for cardiogenic shock) trial found a 36% increase in death for diabetic patients with cardiogenic shock from MI
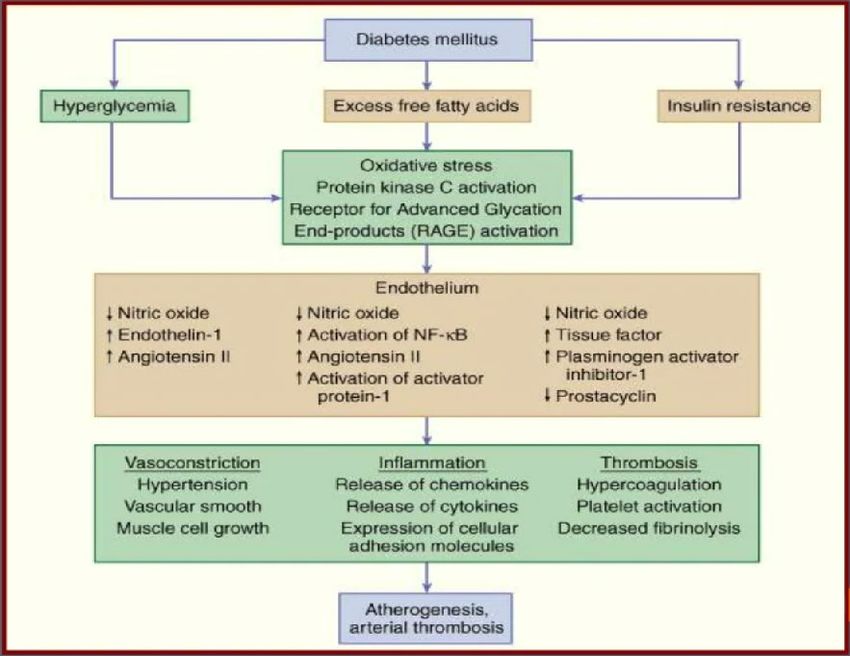
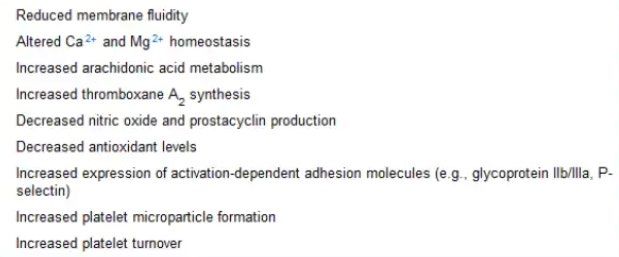
Platelet abnormalities
Clotting • Imbalance in the coagulation and fibrinolytic cascades that supports clot formation and stability • Increases plasminogen activator inhibitor type 1 (PAI-1) levels impairing fibrinolytic capacity in atherosclerotic lesions • Increases the expression of tissue factor and levels of plasma coagulation factors • Decreases levels of endogenous anticoagulants
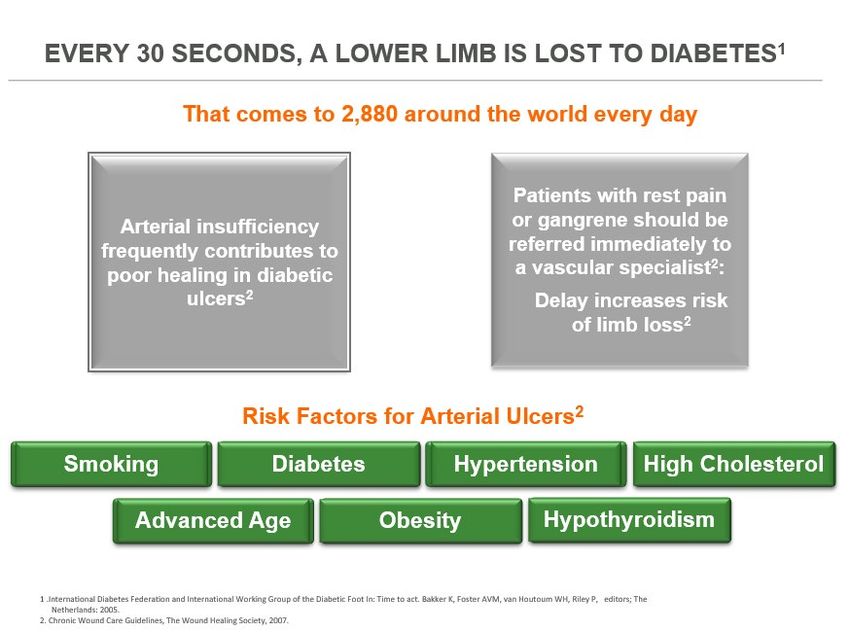
PAD • DM increases incidence and severity of limb ischemic two to fourfold • Often affects distal limb vessels – tibial and peroneal arteries which limits the potential for collateral vessel development • May present with absent pedal pulses, diminished ABIs, claudication, non-healing ulcers, rest pain, cramping pain, numbness • MAY BE SILENT
Disparities • In the Framingham cohort, the presence of diabetes increased the frequency of intermittent claudication by more than 3-fold in men and more than 8-fold in women • Most common cause of nontraumatic amputations in the US • 1 in 20 Americans over 50 have PAD • 1 in 3 diabetics over 50
Amputations • 54% of patients undergo amputations without being assessed by angiograms • Amputation rates decrease as revascularization increases
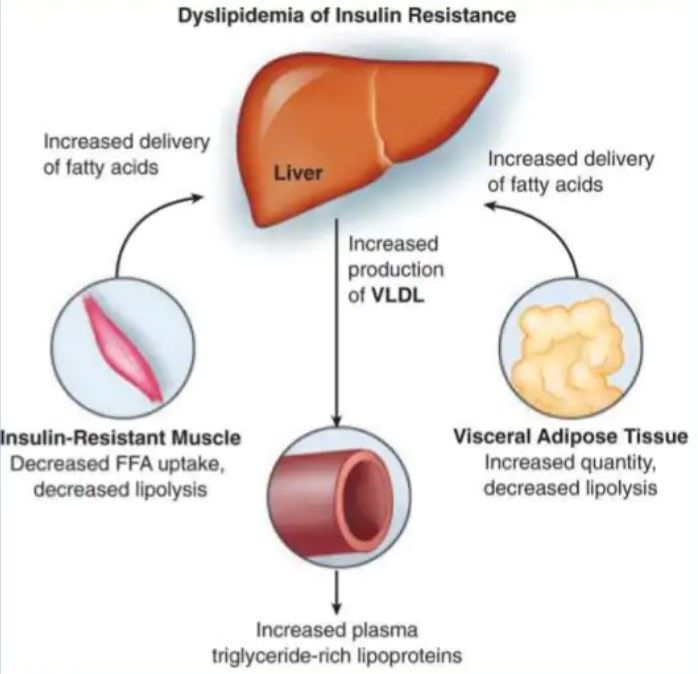
Diabetic Dyslipidemia
Lipid and lipoprotein abnormalities in NIDDM
Lipid and lipoprotein abnormalities in IDDM
Lipid Management—Lifestyle Intervention • Lifestyle modification focusing on weight loss (if indicated); application of a Mediterranean style or Dietary Approaches to Stop Hypertension (DASH) eating pattern; reduction of saturated fat and trans fat; increase of dietary n-3 fatty acids, viscous fiber, and plant stanols/sterols intake; and increased physical activity should be recommended to improve the lipid profile and reduce the risk of developing atherosclerotic cardiovascular disease in patients with diabetes • Intensify lifestyle therapy and optimize glycemic control for patients with elevated triglyceride levels (≥150 mg/dL [1.7 mmol/L]) and/or low HDL cholesterol (
Monitoring with Lipid Panel • In adults not taking statins or other lipid-lowering therapy, it is reasonable to obtain a lipid profile at the time of diabetes diagnosis, at an initial medical evaluation, and every 5 years thereafter if under the age of 40 years, or more frequently if indicated. • Obtain a lipid profile at initiation of statins or other lipid lowering therapy, 4–12 weeks after initiation or a change in dose, and annually thereafter as it may help to monitor the response to therapy and inform medication adherence.
Statin Treatment—Primary Prevention • For patients with diabetes aged 40–75 years without atherosclerotic cardiovascular disease, use moderate-intensity statin therapy in addition to lifestyle therapy. • For patients with diabetes aged 20–39 years with additional atherosclerotic cardiovascular disease risk factors, it maybe reasonable to initiate statin therapy in addition to lifestyle therapy. • In patients with diabetes at higher risk, especially those with multiple atherosclerotic cardiovascular disease risk factors or aged 50–70 years, it is reasonable to use high-intensity statin therapy. • In adults with diabetes and 10-year ASCVD risk of 20% or higher, it may be reasonable to add ezetimibe to maximally tolerated statin therapy to reduce LDL cholesterol levels by 50% or more.
Statin Treatment—Secondary Prevention • For patients of all ages with diabetes and atherosclerotic cardiovasculardisease, high intensity statin therapy should be added to lifestyle therapy. • For patients with diabetes and atherosclerotic cardiovascular disease considered very high risk using specific criteria, if LDL cholesterol is ≥70 mg/dL on maximally tolerated statin dose, consider adding additional LDL-lowering therapy (such as ezetimibe or PCSK9 inhibitor). • For patients who do not tolerate the intended intensity, the maximally tolerated statin dose should be used.
Statin Treatment Intensity
Overwhelming benefit for the use of statins
Residual risk • 65-70% of events occur in the setting of statins
Lower is better
• The LDL hypothesis
• 2004 PROVE-IT
• Significantly reduced CVD events following MI with high-dose atorva vs. prava
• As early as 1995 Cholesterol Treatment Trialists began publishing
meta-analyses based on the statin trials
• In 2005 (based on 14 trials at the time) they reported that on average, a
reduction of 1 mmol per liter (38.7 mg per deciliter) in LDL cholesterol levels
yields a consistent 23% reduction in the risk of major coronary events over 5
yearsLower is better?
• 2008 ENHANCE trial
• Failed to show the addition of ezetimibe in carotid intimal medial thickness
despite a reduction in LDL
• Several negative trials using combination lipid therapy despite
lowering LDL in many cases
• The statin hypothesis
• Pleiotropic effects of statins including:
• Amelioration of endothelial dysfunction
• Enhancing stability of atherosclerotic plaques
• Increased nitric oxide bioavailability
• Anti-oxidant properties
• Anti-inflammationLower is Better! • Published in 2015 • Simvastatin 40mg vs simvastatin 40mg + ezetimibe 10mg in patients who had been hospitalized in the preceeding 10 days with acute coronary syndrome • Lowered LDL cholesterol by approximately 24% • First outcome trial of a non-statin to show benefit with further LDL reduction
What is PCSK-9? • Pro-protein convertase subtilisin-like kexin type 9 • A secreted protease which is a 692 amino acid mature protein, consisting of 3 domains: prodomain, catalytic, and C-terminal • Primarily expressed in liver, intestine and kidney • Rapid turnover in plasma (
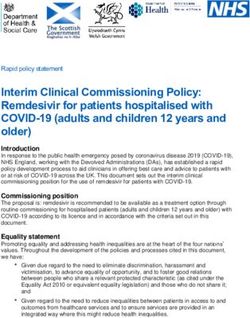
Discovery of PCSK-9 • Identified in 2003 at the Necker-Enfants Malades Hospital in Paris. • Gain-of-function mutations were identified in two French families (HC92 and HC60) who presented with severely elevated LDL-C levels and were diagnosed with autosomal dominant hypercholesterolemia • It was determined with linkage analysis that these patients had PCSk9 gain- of-function mutations on chromosome 1 which results in increased expression of the PCSK9 protein, increased serum LDL-C, and the expression of the FH phenotype. • Further investigation with animal models revealed that overexpression of the PCSK9 gene results in a dropout in the LDLR and a subsequent increase in LDL-C levels proving the relationship between the two.
Figure 1. Pedigree of family HC92 and genetic analysis with markers spanning the 1p34.1−p32 region. Affected individuals present with a history of tendon xanthomas (individuals HC92-II-7 and HC92-III-3), coronary heart disease, early myocardial infarction (individuals HC92-II-2 and HC92-II-6) and stroke (individual HC92-II-4). Filled bars indicate the mutated allele. Age (in years) at lipid measurement, total cholesterol (TC) and low- density lipoprotein cholesterol (LDL-C; in g per liter; untreated values for affected individuals) are given.
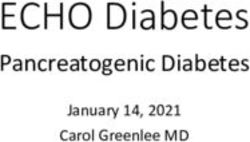
Mean LDL-C levels in patients with GOF PCSK9 Mutations
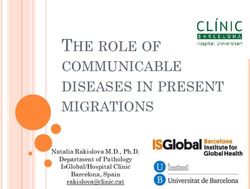
Loss of Function • The hypothesis originated that if gain of function of PCSK9 is associate with elevated levels of LDL-C and CHD, then loss of function of PCSK9 is associated with low LDL-C levels • This was affirmed by the Dallas Heart study in 2004 that evaluated a diverse population (50% African Americans) in which two nonsense mutations (Y142X and C679X) were identified in PCSK9 among African Americans with 40% lower LDL-C levels. • Subsequently, PCSK9 was sequenced in the Atherosclerosis Risk in Communities (ARIC) study participants which found that 2.6% of 3363 African American subjects had similar PCSK9 nonsense mutations (Y142X and C679X). • These mutant carriers had a 28% LDL-C reduction and an 88% reduction in coronary events over a 15-year observation period • 3.2% of white subjects had the PCSK9R46L sequence variant, which was associated with a 15% reduction in mean LDL-C and a 47% reduction in CHD • In 2005, a PCSK9 knockout (KO) mice model also showed decreased levels of cholesterol
Mean LDL-C levels in patients with LOF PCSK9 mutations
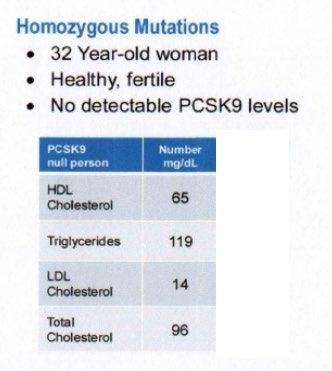
Loss of function homozygous mutation case reports • 32 year old Caucasian woman had no measurable PCSK9 and a LDL-C of 14 (Am J Hum Genet. 2006;79: 514-523) • 21 year old Zimbabwean woman had no measurable PCSK9 and a LDL-C of 15 (Atherosclerosis. 2007;193: 445-448) • 49 year old French male had no detectable PCSK9 levels and a LDL-C of 16 (Arterioscler Thromb Vasc Biol. 2009;29:2192-2197)
Regression?
Treatment of Other Lipoprotein Fractions or Targets • In patients with atherosclerotic cardiovascular disease or other cardiovascular risk factors on a statin with controlled LDL cholesterol but elevated triglycerides (135–499 mg/dL), the addition of icosapent ethyl can be considered to reduce cardiovascular risk .
Lipoprotein(a) • “We recommend screening for elevated Lp(a) in those at intermediate or high CVD/CHD risk, a desirable level
Inflammation
• Proinflammatory HDL
• During states of inflammation HDL can be converted to proinflammatory HDL
which promotes LDL oxidation
• McMahon et al. found that >85% of patients with SLE and carotid plaques had
measurable piHDL, compared with around 40% of those without detectable
plaques
• Oxidative stress
• an excess of ROS not counterbalanced by an adequate antioxidant defense
system is associated with accelerated atherosclerosis in the general
population
• Increased oxidative stress has been identified in patients with SLE, and is
often elevated independent of disease activitySCAI Statement on Meta-Analysis of Elective Coronary Revascularization vs. Medical Therapy Alone • A rigorous meta-analysis of randomized clinical trials (RCTs) that compared the effects of medical therapies alone with medical therapies plus revascularization in patients with stable ischemic heart disease (SIHD) was presented at EuroPCR on May 18, 2021. • concluded that adding revascularization was associated with a statistically important reduction in cardiovascular death associated with a statistically important reduction in spontaneous myocardial infarction (MI) • Syntax, Bari2D, FAME, ischemia, courage
You can also read