Anticoagulant on COVID-19 Associated Coagulopathy (Penggunaan Antikoagulan pada Tatalaksana Covid-19) - Agus Subagjo MD, M Yusuf A MD, Irma ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Anticoagulant on COVID-19 Associated Coagulopathy
(Penggunaan Antikoagulan pada Tatalaksana Covid-19)
Agus Subagjo MD, M Yusuf A MD, Irma Maghfirah MD
Department of Cardiology and Vascular Medicine
Universitas Airlangga-Dr. Soetomo General Hospital
The Guidelines
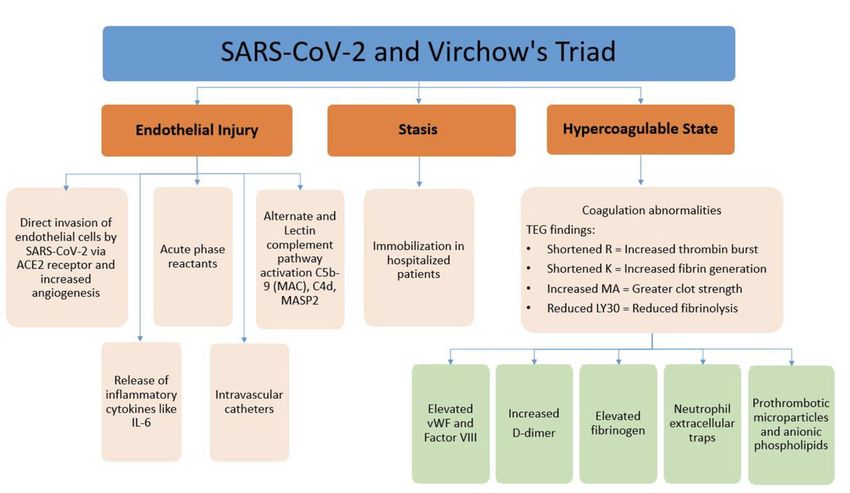
Pathogenesis of Hypercoagulability
in COVID-19
Incompletely Understood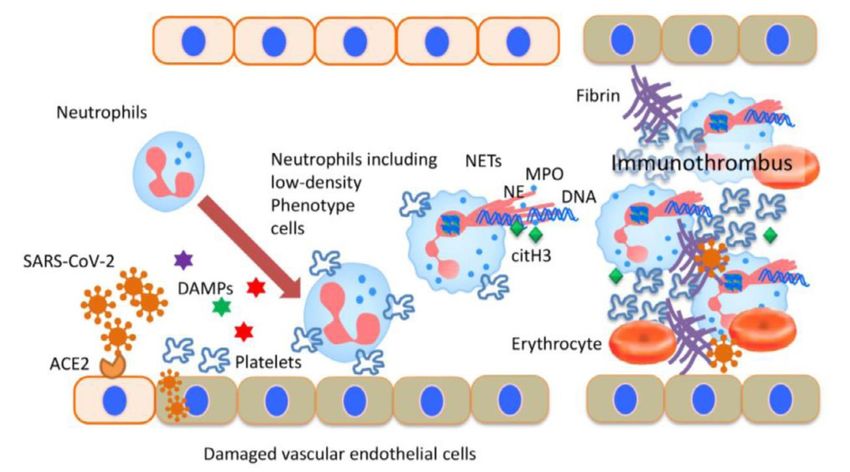
American Journal of Cardiovascular Drugs, 2020: 20(5), pp.393–403.

Immunothrombosis or Thromboinflammation in COVID-19
EBioMedicine 59 (2020) 102942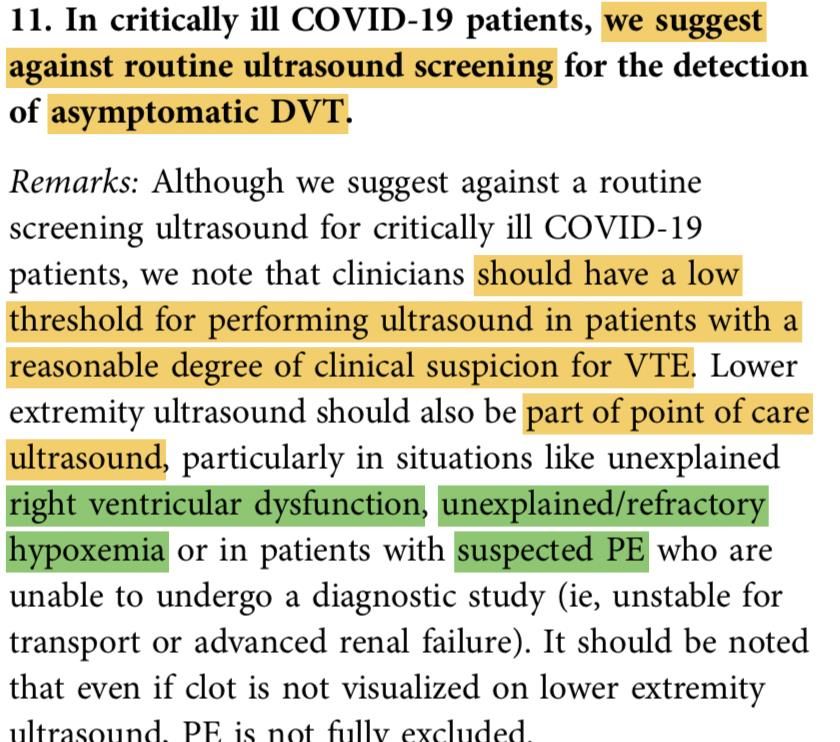
Mr. Potter, 48 yo with HTN and Hyperlipidemia, came to ER with 2 day history of
shortness of breath (SOB) alongwith fever (T 38.5). No bilateral leg swelling. CxR
shows bilateral pneumonia, Rapid test Non reactive, CT scan thorax showed
Ground Glass Appearance (GGO). SWAB PCR no data yet. D Dimer level 1400
ng/ml. BGA showed type 1 respiratory failure. Patient was then admitted to ICU.
You’ve been consulted regarding anticoagulant on this patient. Which one could
be the best option?
a. Hold anticoagulant, patient wasn’t confirmed as COVID yet
b. Do VTE risk assessment, consider giving anticoagulant if VTE score was high
c. Consider anticoagulant IV
d. Perform Duplex ultrasound considering abnormal D dimer, treat with
anticoagulant if thrombus was detected
1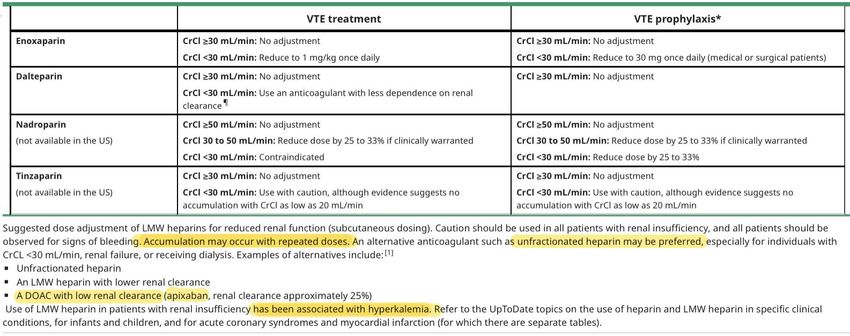
Should acutely ill hospitalized patients
receive VTE Prophylaxis ?
Unless Contraindicated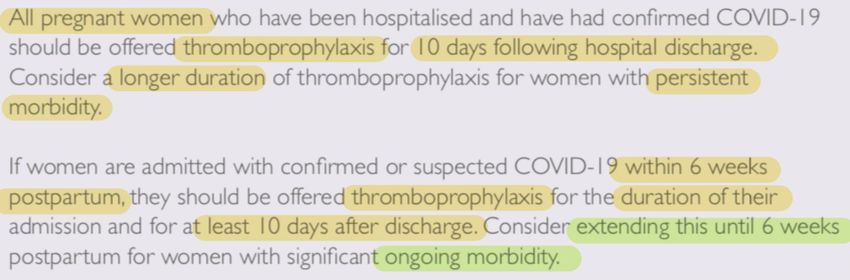
Journal of Thrombosis and Thrombolysis (2020) 50:72–81 blood® 4 JUNE 2020 | VOLUME 135, NUMBER 23
doi:10.1093/ehjcvp/pvaa036. European Heart Journal J Am Coll Cardiol 2020;75:2950–73
Reasons Why
• Pneumonia > considered as risk factors for VTE
• Others Risk Factors found in Px with Covid-19 :
- High Risk : Hospitalized for AF or Acute Heart failure
- Moderate Risk : central venous lines, Congestive HF,
Respiratory Failure
- Low Risk : Bed Rest > 3 days, DM, HT, Increasing age,
obesity, pregnancy
European Heart Journal (2020) 41, 543603 Journal of Thrombosis and Thrombolysis (2020) 50:72–81Reasons Why
• The pathogenesis of hypercoagulability in COVID-19 is incompletely
understood
• Predominant coagulation abnormalities in patients with COVID-19
suggest a hypercoagulable state and are consistent with uncontrolled
clinical observations of an increased risk of venous thromboembolism
COVID-19-associated coagulopathy (CAC)STUDIES Why
Reasons
Study in China > VTE incidence 25%
vs 5-15% (COVID VS not COVID)
Italy > Thromboembolic events
7.7%, cumulative rate 21%
Netherlands > PE in COVID 13.6% despite
on pharmacologic prophylaxis
Journal of Thrombosis and Thrombolysis (2020) 50:72–81What are the Contraindication for VTE
Prophylaxis ?
Common SenseISTH-IG
If Contraindicated SCC-ISTH
Mr. Ronald Weasley, 53 yo with confirmed COVID-19 was admitted to Intensive
care unit for a couple days. He was intubated, no swelling on extremities. D Dimer
level 1400 ng/ml. No data on fibrinogen. CRP was elevated. RFT within normal
limit.
You’ve been consulted regarding the anticoagulant regiment should be given to
this patient. Which one could be the best option?
a. Prophylaxis dose of LMWH
b. Intensified dose of enoxaparin
c. Heparin drip loading 80 IU continued by 18 iu/kg/hour
d. Duplex ultrasound considering abnormal D dimer, consider anticoagulant if
thrombus was detected
2Mr. Tom Riddle, 78 yo with HTN and Hyperlipidemia, was brought to ER 48 hrs
ago, with 2 day history of SOB and fever (T 38.5). D dimer level was 980 ng/ml.
Swab PCR (+). Over the past 48 hrs, he has worsened, he remained febrile, CRP
and D-dimer increased to 1656 ng/ml. He was treated w/ prophylactic
anticoagulant on admission. CTA showed no evidence of DVT or PE. Now that he
has worsened, what was your decision regarding anticoagulant dose intensity of
the patient?
a. Continue prophylactic anticoagulation during hospitalization
b. Re-assess VTE risk score, perform serial D-dimer to determine anticoagulant
dose
c. Consider therapeutic dose anticoagulant IV
d. Perform Duplex ultrasound considering abnormal D dimer, treat with
anticoagulant if thrombus was detected
3Mr. Dudley, 78 yo with HTN and Hyperlipidemia, was brought to ER 48 hrs ago,
with 2 day history of SOB and fever (T 38.5). D dimer level was 980 ng/ml. Swab
PCR (+). Over the past 48 hrs, he has worsened, he remained febrile, CRP and D-
dimer increased to 1656 ng/ml. He was treated w/ prophylactic anticoagulant on
admission. CTA showed no evidence of DVT or PE. Now that he has worsened,
what was your decision regarding anticoagulant dose intensity of the patient?
a. Re-assess VTE risk score, perform serial D-dimer to determine anticoagulant
dose
b. Switch to intermediate dose anticoagulation during hospitalization
c. Consider therapeutic dose anticoagulant IV
d. Combine with antiplatelet
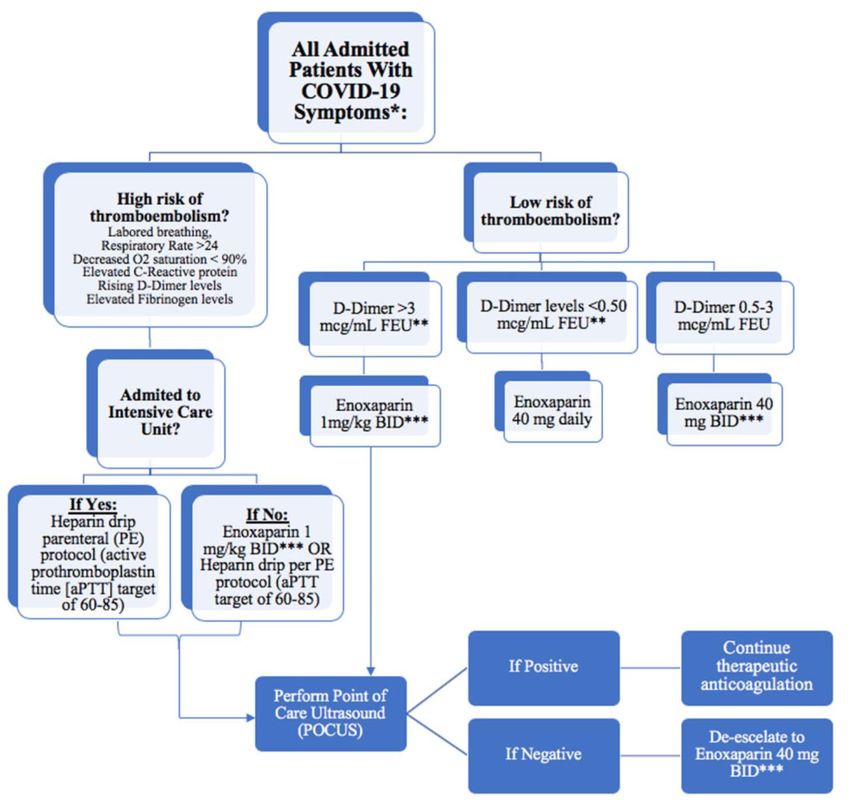
4What intensity of VTE prophylaxis should
patients with COVID - 19 receive?
Data PaucityCONSIDERATIONS • Status : Hospitalized / Outpatients • Clinical Severity : Mild/Moderate/Severe • Observation : Ward/Intermediate/Intensive Care • Predisposing VTE : Mild/Moderate/High risk • Laboratories : IL-6/D-Dimer/PCT • Risk of Bleeding : Improve, hasbled score • Possible of Invasive Procedures : CVC, IABP
RECENT STUDIES
01 02
Netherlands, COVID critically ill France, 150 COVID ARDS pts,
w/ std prophylaxis >> 25 of 184 receiving thromboprophylactic
developed VTE (Klok et al, 2020) 80%, therapeutic 20% (>> LMWH).
16.7% pts still suffered PE (Helms
et al, 2020)
Thrombosis Research 191 (2020) 145–147 Intensive Care Med 2020; 46:1089Prophylaxis Regiment SCC ISTH
Prophylaxis Regiment
J Am Coll Cardiol 2020;75:2950–73To be Kept in Mind
• VTE may still develop with prophylaxis or treatment dose
• Dose might be adjusted thru clinical course :
• Prophylaxis
• Intensified
• Treatment
• Always consider Risk : Benefit ( Embolism : Bleeding ) !
• It is important for providers and clinicians to stay apprised of
emerging evidence and adjust practices accordingly
Journal of Thrombosis and Thrombolysis (2020) 50:72–81blood® 4 JUNE 2020 | VOLUME 135, NUMBER 23
Mr. Dumbledore, 59 yo with confirmed COVID-19 was admitted to Intensive
care unit for a couple days. He was intubated, and known to have unilateral leg
swelling which then confirmed as VTE on femoral vein. D Dimer level 2300 ng/ml.
No data on fibrinogen. CRP was elevated. CrCl 28 ml/min. He had history of heart
failure and was planned to be undergoing CVC placement.
What type of anticoagulant did you preferred on this patient?
a. Enoxaparin
b. Unfractionated Heparin
c. Fondaparinux
d. DOAC
5What drugs are recommended?
Availability and FamiliarityDalteparin Nadropari n Tinzaparin
COMPARISONS
Heparin Enoxaparin Fondaparinux
(+) (+)
(+)
Cheap Usually no monitoring Usually no monitoring
Antidot + 1-2x SC 1 SC
Onset Immediate Bleeding + Bleeding +/-
Minimal Drugs Interactions 2 Mechanisms
1 Mechanisms
Can be stopped anytime
(-)
(-) : Partial Antidot (-)
Serial Checks & Adjustments Porcine Antidot not available
Bleeding ++ HIT < 1 %
Renal Impairment 1 Mechanisms
HIT 3-5%
Renal ImpairmaentCOMPARISONS
Heparin Enoxaparin
Fondaparinux
Prophylaxis Prophylaxis Prophylaxis
2x5000 IU SC, or 1x40 mg SC, or 1x2.5 mg SC
80 IU/kg/24hr; APTT 1.2-1.5x 2x30 mg
Intensified/Intermediate Treatments
Intensified/Intermediate
Loading2-3 x 7500 IU SC, or
2x 40 mg SC , or < 50 Kg : 1x5mg SC
5-8 IU/Kg/Hour 2x0.5mg/kg 50-100 : 1x7.5 mg SC
> 100 : 1x10 mg SC
Treatments Treatments
80 IU/Kg IV 2x60 mg SC, or
(or Bolus 5000 IU ) 2x1mg/kg SC
Maint : 18 IU/kg/hour
APTT 1.5-2xTherapeutic Regiment
Therapeutic Regiment
J Am Coll Cardiol 2020;75:2950–73Suggested Dose Adjustments of LMWH w/ Renal Insufficiency
Coronavirus disease 2019 (COVID-19): Hypercoagulability -UPTODATEPlausible Superiority
• Heparin has been implicated in binding to COVID-19 spike proteins as
well as downregulating interleukin-6 (IL-6), which has been shown to
be elevated in COVID-19 patients
• Thus unfractioned heparin or LMWH remains as the best choice of
anticoagulant for admitted patients
• What about UFH vs LMWH?
European Heart Journal - Cardiovascular PharmacotherapyEfficacy of Subcutaneous Unfractionated
Heparin
Meta AnalysisSubcutaneous UFH vs Intravenous UFH
Cochrane Database of Systematic Reviews 2017, Issue 2. Art. No.: CD006771.Subcutaneous UFH
vs
LMWH
Cochrane Database of Systematic Reviews 2017,
Issue 2. Art. No.: CD006771.Should we do ultrasound screening for the
detection of asymptomatic DVT?J Am Coll Cardiol 2020;75:2950–73
Mrs. Ginny, 28 yo, pregnant, 32-33 weeks, confirmed COVID-19 was being
hospitalized and admitted to general wards. The patient was having mild
symptoms. D-dimer level was 2500 ng/ml. No signs of VTE what so ever.
Regarding anticoagulant in this patient, what could be the best option?
a. No anticoagulant is needed
b. Intensified dose of LMWH
c. Prophylaxis dose of enoxaparin
d. Less than 36 weeks, VKA could be the best option
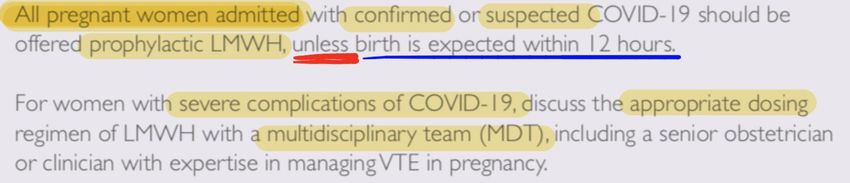
6Special Population
PregnancyJournal of Thrombosis and Thrombolysis (2020) 50:72–81 Royal College of Obstetricians and Gynaecologists. Coronavirus (COVID-19) Infection in Pregnancy.
Mrs. Lovegood, 28 yo, pregnant, 33-34 weeks, confirmed COVID-19. She was
hospitalized for several days, and being discharge 2 days before. Recent SWAB PCR showed
that SARS COV-2 not detected. She present to the outpatient clinics, asymptomatic,
mobility is good. The latest D Dimer level was 400 ng/ml. She was treated with LMWH
before, and now asking whether she needs anticoagulant any longer. What is your answer?
a. No anticoagulant is needed
b. Offer thromboprophylaxis for 10 days
c. DOAC
d. Less than 36 weeks, we may consider VKA
7Royal College of Obstetricians and Gynaecologists. Coronavirus (COVID-19) Infection in Pregnancy.
Coronavirus disease 2019 (COVID-19): Hypercoagulability -UPTODATE
Mrs. Lily Evans, 25 yo, pregnant, 36-37 weeks, confirmed COVID-19, and was
being admitted to general wards. She was treated with therapeutic dose
anticoagulant LMWH and planned to be undergoing cesarean delivery. The
Gynecologist ask you, a Cardiologist, regarding the time they should stop
anticoagulant prior to SC. What is your answer?
a. 24 hours prior to SC
b. 12 hours prior to SC
c. Switch to UFH first
d. 36 hourst before SC
8Use of anticoagulant during pregnancy and postpartum-UPTODATE
Use of anticoagulant during pregnancy and postpartum-UPTODATE
Mr. Draco, 59 yo, with atrial fibrillation was hospitalized for COVID-19. Currently he
had moderate symptoms. Admitted to a general ward. No signs of heart failure. He had
consumed Rivaroxaban 15 mg once a day for 6 months now.
You’ve been consulted regarding the best choice of anticoagulant regiment in this
patient. What is the best possible answer?
a. Patient not admitted to ICU ward, continue rivaroxaban
b. Switch to LMWH
c. Re-adjust rivaroxaban dose
d. Settle with rivaroxaban, add mechanical thromboprophylaxis
9Why Shouldn’t we consider oral anticoagulant in hospitalized patients?
SCC-ISTH ISTH-IG
LMWH or UFH
Journal of Thrombosis and Thrombolysis (2020) 50:72–81Short half-lives 01
The Versatility in administration
02
Rationale Less drug-drug interaction
compared to anticoagulants 03
Anti-inflammatory properties
04
Ebio Medicine 59 (2020) 102969
Journal of Thrombosis and Thrombolysis (2020) 50:72–81Properties of
LMWH/UFH
Heparin inhibits HPSE activity
Anti-inflammatory properties
Reduces viral entry to host cells
Neutralizes circulating histones
Anticoagulation
Ebio Medicine 59 (2020) 102969Mr. Longbottom, 39 yo, are planned to discharge after being horspitalized for
COVID-19. He was previously admitted to ICU ward which was then transferred into
general ward since was improving. Latest D dimer 1500 ng/ml. RFT and LFT were within
normal limits. Ultrasound showed no sign of thrombus. His pulmonologist asked you
regarding the anticoagulant post discharge. What would be the best answer possible?
a. No signs of VTE, no need anticoagulant at discharge
b. Perform VTE Risk assessment and bleeding risk score, consider continuation of
anticoagulant if low bleeding score
c. Continue anticoagulant
d. Monitoring D-Dimer at outpatient setting, may treat w/anticoagulant if D-dimer is
escalated
10Mr. Tom Riddle, 78 yo with HTN and Hyperlipidemia, was brought to ER 48 hrs
ago, with 2 day history of SOB and fever (T 38.5). D dimer level was 980 ng/ml.
Swab PCR (+). Over the past 48 hrs, he has worsened, he remained febrile, CRP
and D-dimer increased to 1656 ng/ml. He was treated w/ prophylactic
anticoagulant on admission. CTA showed no evidence of DVT or PE. His clinical
status was improved and now was planning to discharge. You’ve been consulted
regarding anticoagulant prophylaxis at discharge. What could be your best choice?
a. No need anticoagulant at discharge
b. Re-assess VTE risk score, perform serial D-dimer to determine anticoagulant
dose
c. If the patient have high bleeding risk, consider antiplatelet instead
d. Perform Duplex ultrasound at discharge,
11Mr. Dudley, 78 yo with HTN and Hyperlipidemia, was brought to ER 48 hrs ago,
with 2 day history of SOB and fever (T 38.5). D dimer level was 980 ng/ml. Swab
PCR (+). Over the past 48 hrs, he has worsened, he remained febrile, CRP and D-
dimer increased to 1656 ng/ml. He was treated w/ prophylactic anticoagulant on
admission. CTA showed no evidence of DVT or PE. His clinical status was
improved and now was planning to discharge. You’ve been consulted regarding
anticoagulant prophylaxis at discharge. What could be your best choice?
a. Re-assess VTE risk score, perform serial D-dimer to determine anticoagulant
dose
b. Continue anticoagulant after hospital discharge
c. Use Caprini RAM score to determine thromboembolism risk
d. High D-Dimer, combine anticoagulant with aspirin
12Should patients with confirmed COVID-
19 receive VTE prophylaxis following
hospital discharge?
Data PaucityCOVID-19 Pandemic Situation
• No direct evidence for extended VTE prophylaxis in COVID-19 pts to
date.
• ASH 2018 & Chest 2012 >> against anticoagulant at discharge
• Severely ill patients w/ COVID-19 may experience:
• Prolonged hospital stay
• Significant deconditioning
• Post-ICU syndrome >> limits or delays full recovery to baseline
mobility or health status by time of discharge
• Pts with COVID-19 may be discharged early in their recovery while they
remain quite ill in order to free up hospital beds for sicker patients
Journal of Thrombosis and Thrombolysis (2020) 50:72–81SCC-ISTH
If no VTE, perform VTE RAM score and
analyze bleeding risk
J Am Coll Cardiol 2020;75:2950–73Novel Oral Anti Coagulants
• The benefit of oral anticoagulation with DOACs includes the lack of need for
monitoring
• Facilitation of discharge planning, and outpatient management.
• The potential risk (especially in the setting or organ dysfunction) may include
clinical deterioration and lack of timely availability of effective reversal agents
• Rivaroxaban (31-39 days), Enoxaparin (6-14 days), Betrixaban (35-42 days)
Journal of Thrombosis and Thrombolysis (2020) 50:72–81 J Am Coll Cardiol 2020;75:2950–73VTE RAM assesment IMPROVE vs PADUA, which one is superior?
PADUA Score IMPROVE VTE RAM
Empirically Derived Database-Derived
J Thromb Haemost 2010 Nov;8(11):2450-7 Chest. 2011 Sep;140(3):706-714.IMPROVE
bleeding RAM
Bali Medical Journal (Bali Med J) 2020, Volume 9, Number 2: 482-488
Chest. 2011 Jan;139(1):69-79Mr. Ollivander, 53 yo, was previously hospitalized for COVID-19. He turned
out having deep vein thrombosis (DVT) in leg ankle. He was already discharged
and came to outpatient clinics. He asked you, cardiologist, on how long he should
consume anticoagulant medication (Rivaroxaban) since he apparently didn’t feel
any symptoms. What could be your best possible answer?
a. Pursue anticoagulant for at least 3 months
b. No prolonged anticoagulant is needed
c. Perform Ultrasound right at the day, terminate anticoagulant if no thrombus
d. Continue Rivaroxaban up until 31-39 days
13Duration of Therapeutic Anticoagulant
European Heart Journal (2017) 0, 1–13 Minimum of 3 months
Mr. Remus Lupin, 48 yo, with longstanding atrial fibrillation, present to your
clinics. He has consumed warfarin for 4 years now. He asked you whether any
regimen besides warfarin that he could use, since it’s pandemic now and he was
afraid if he has to go back and forth every once in a month. He even considered to
stop taking warfarin. His latest RFT was normal. His echo showed biatrial
enlargement, with no valves abnormalities. What is your best solution ?
a. Continue warfarin
b. Prolong the duration of INR Monitoring
c. Switch to LMWH
d. Switch to DOAC if feasible
14Switching Oral Anticoagulant
Strategies to minimize Covid-19 exposure
for patients on Warfarin
• Transition to DOAC if possible
• Referral for patient self testing
• Use of face masks, social distancing, good hand hygiene before, after and during
clinic visit
• Avoiding busy laboratory times, such as Mondays or weekdays morning
Journal of Thrombosis and Thrombolysis (2020) 50:72–81Journal of Thrombosis and Thrombolysis (2020) 50:72–81
J Am Coll Cardiol 2020;75:2950–73
Mr. Rubeus Hagrid, 41 yo, was hospitalized with COVID-19 and respiratory
failure, he was intubated for several days now. Serial D-Dimer was performed. His
admission D-Dimer was 6000 ng/ml. He had no proven VTE and being
anticoagulated with UFH intermediate dose (escalated dose). His anesthesiologist
consulted with cardiologist fellow whether it’s needed to increase anticoagulant
dose since D Dimer value the day afterwas 11.000 ng/ml. What could be the best
choice below?
a. Switch to therapeutic dose right at that moment
b. Stick to the intensified dose of LMWH
c. Prepare thrombolytics therapy
d. Less than 36 weeks, VKA could be the best option
15Role of D-Dimer in CAC
Fundamental IssueD-Dimer
• D-dimer is a degradation product of cross-linked fibrin
indicating augmented thrombin generation and fibrin dissolution by
plasmin
• High D-dimer levels are common in acutely ill individuals with a
number of infectious and inflammatory diseases
• Some of the markers of deranged coagulation (eg, D-dimer) appear to
correlate with illness severity.
• It is unknown if intensification of anticoagulant therapy based on
biomarker thresholds alone improves patient outcome
Coronavirus disease 2019 (COVID-19): Hypercoagulability -UPTODATED-Dimer
• An increase in D-dimer is not specific for VTE and is not sufficient to
make the diagnosis
• We suggest against daily monitoring of d-dimer for the purpose
of guiding anticoagulant therapy
• Acutely worsening clinical status in conjunction with laboratory value
changes, such as rising D-dimer, may necessitate further
thromboembolic workup
• >1,500 ng/ml has a sensitivity of 85.0% and specificity of 88.5% for
detecting VTE events
Journal of Thrombosis and Thrombolysis (2020) 50:72–81
Coronavirus disease 2019 (COVID-19): Hypercoagulability - UpToDateSCC-ISTH
Laboratory testing for risk stratification and triage
ISTH-IG
J Thromb Haemost. 2020;18(5): 1023–6.DIC and CAC Differences in similarities
Distinguishing Features between CAC and DIC
American Journal of Cardiovascular Drugs, 2020: 20(5), pp.393–403.Mr. Sirius Black, 39 yo, was hospitalized with COVID-19 and respiratory
failure, he was intubated for several days now. Serial D-Dimer was performed. His
admission D-Dimer was 6000 ng/ml. Few days later, ulmonary embolism was
shown from CTA. Patient was hemodynamically stable. Should you give
thrombolytics therapy for this patient?
a. Perform thrombolytics
b. Stick to the therapeutic dose of LMWH
c. Add aspirin
d. Check the latest D-Dimer first
16Thrombolytics therapy
Should we consider?Pulmonary Embolism
• The use of catheter-directed therapies during the current
outbreak should be limited to the most critical situations.
• Indiscriminate use of inferior vena cava filters should be avoided
• Recurrent PE despite optimal anticoagulation, or clinically significant
VTE in the setting of absolute contraindications to anticoagulation,
would be among the few scenarios in which placement of an inferior
vena cava filter may be considered
(J Am Coll Cardiol 2020;75:2950–73)ACF
J Am Coll Cardiol 2020;75:2950–73Antiplatelets When benefits outweigh the risk
What Should we do • No proven interactions, continue whenever possible • In the absence of evidence, decisions for antiplatelet therapy need to be individualized • In general, it is reasonable to continue dual antiplatelet therapy if platelet count is >50,000, reduce to single antiplatelet therapy if platelet count is >25,000 and
Heparin-induced Thrombocytopenia
Management of Heparin Induced Thrombocytopenia-Uptodate
Management of Heparin Induced Thrombocytopenia-Uptodate
Overt Bleeding
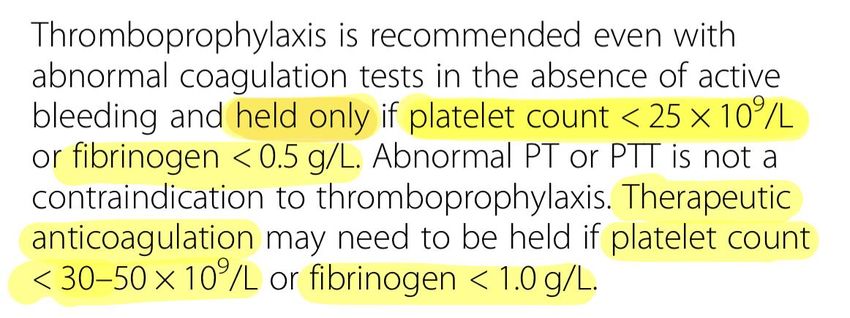
The Recommendations • Stop bleeding related antithrombotics • Administer antidote whenever possible • blood products support should be considered as per septic coagulopathy • TC to maintain platelet count >50 x 109/l in DIC patients with active bleeding or >20 x 109/l in those with a high risk of bleeding or requiring invasive procedures
The Recommendations • Fresh frozen plasma (15 to 25 ml/kg) in patients with active bleeding with either prolonged PT or aPTT ratios (>1.5x normal) or decreased fibrinogen (
CONCLUSIONS
• While evidence of COVID-19 associated coagulopathy and thrombosis risk is
rapidly emerging, there is no high quality evidence to guide antithrombotic
treatments.
• It is critical for providers and clinicians to stay apprised of emerging
evidence and adjust practices accordingly.THANKS!
You can also read