Review of High Dose Opioids in Chronic Non-Malignant Pain 2017/18
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Review of High Dose Opioids in Chronic Non-Malignant Pain 2017/18
Review of High Dose Opioids in Chronic Non-Malignant Pain 2017/18 Kathryn Steele Senior Medicines Optimisation Pharmacist Brighton & Hove CCG (Pain & Substance Misuse) Clinical Pharmacist (Independent Prescriber) Wellsbourne Healthcare CIC (GP Surgery) (Chronic Pain Clinic)
Project Referenced
• SPS: Review of high dose opioids in chronic non-malignant pain
• University of East Anglea: Toolkit for tackling chronic opioid use
in non-cancer pain
• BMJ: Opioids: new toolkit aims to help GPs manage long term use
• PJ: A call for action on high-dose opioid prescribingWhy focus on this in 2017/18?
• Faculty of Pain Medicine (Royal College of Anaethetists):
Good for acute pain & pain at end of life, but little evidence for long term pain
If pain remains severe they are not working & should be stopped, even if no other
treatment available
Harms outweigh benefits > 120mg oral morphine or equivalent (OME) / 24hours
Above this the risk of harm and mortality increases substantially with no increased
benefit
May help a small proportion if the dose can be kept low and used intermittently
• Rxs for opioids rose dramatically in England
1991 = 3 million, 2001 = 7.5 million, 2016 = 24 million (NHS Digital)
costing over £340 million
• Opioids prescribed to 5% of patients in 2015 (Clinical Practice Research Datalink - NCSR)
• Patients with chronic non-cancer pain have historically been prescribed
opioids in good faith based on evidence that we now know to be misleading
Dangerous - Ineffective - Prescribing IncreasingHarms of high dose opioids
Serious bodily harm, overdose or death (respiratory depression)
Increased pain sensitivity
Hormone changes (e.g. loss of libido, infertility, impotence in men, amenorrhoea)
Depression
Anxiety
Drowsiness or a change in thinking (e.g. a “bubble”)
Decreased immune function (increased risk of e.g. pneumonia)
Increased risk of falls and fractures (increased risk of osteoporosis)
Decreased function & reduced muscle tone
Physical dependence
Dry mouth (increased risk of dental caries and tooth loss)
Faye’s StoryBenefits of reducing opioids
• More energy
• Improved mood & less anxiety
• Be able to think more clearly
• Will feel less drowsy or ‘spaced out’
• Improved libido
• Less risk of falls
• Less risk of infections
• May even experience less pain (majority: pain is unchanged)
• May be able to gradually increase activity and exercise, which, in turn, can help to reduce pain levels
• Reduces the risk of serious harm & death
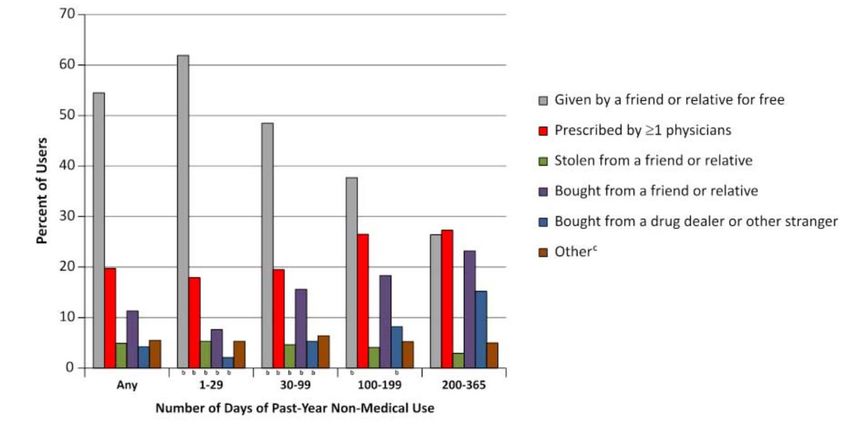
Reduced Risks & Improved Quality of Life (& Ineffective!)Diversion?
Sources of
Prescription Opioids
Amongst Non-
Medical Users
(US National Survey on Drug
Use and Health 2008 – 2011)
Prescription Patterns of Family Members After Discontinued Opioid or BZD
Therapy JAMA Internal Medicine, July 2019
• Increase in first-time opioid or BZD Rx requests by family members around
therapy discontinuation date of the high volume opioid or BZD userThe Domain • Prescribing Incentive Scheme, PIS (now: Prescribing Quality Improvement Scheme, PQIS) • Aim: To identify patients in primary care in B&H with non-malignant chronic pain on >120mg OME/24 hrs Subsequently for GP surgeries to review with an aim to reduce these doses in order to reduce the potential and real harm experienced from these medications • MMT technicians conducted baseline search and calculation of total OME/24hrs N.B. Technician added all prescribed opioids, not just the ones in the search • Submit ‘Summary & Data Collection Form’ • Points awarded based on % of identified patients reviewed (not reduced) (
Search Limitations
• The search was limited in order to control workload for the domain (for the
MMT technician and general practice)
• Search identified patients on the following opioids:
Morphine (IR tabs/caps/soln – all strengths. MR tabs/caps/sachets ≥ 60mg)
Oxycodone (IR caps/soln – all strengths. MR tabs/caps ≥ 30mg)
Fentanyl patches (50mcg/hr, 75mcg/hr, 100mcg/hr)
Buprenorphine patches (52.5 mcg/hr, 70mcg/hr)
Any patients receiving multiple low strengths that add up to ≥120mg
OME/24 hrs will have been missed
• Search excluded patients with a read code for cancer or
palliative care
Some of these patients may not be on the opioids for cancer related pain
• Hoped that once domain completed clinicians would have the knowledge and
confidence to carry onCalculating the Total Oral Morphine Equivalence
(OME) Estimated total daily morphine dose equivalent
Taken from The Royal College of Anaethetists, Faculty of Pain Medicine
(this currently differs to the conversion in the BNF)
Work out the total daily dose of each opiate and enter it in column E.
OME= Oral Morphine Equivalent
PRN doses: In order to estimate dose it is suggested to look at past 3 months actual patient
usage (drug history) and work out average daily dose taken
Analgesia Equivalent to Daily dose Estimated Daily
10mg oral (column E) OME
morphine
sulphate
Codeine 100 0.0
Dihydrocodeine 100 0.0
Morphine 10 0.0
Morphine 10 0.0
Oxycodone 5 0.0
Oxycodone 5 0.0
Tramadol 67 0.0
Fentanyl lozenge
enter
66.67
Also: Oxford
mcgs 0.0
Buprenorphine SL
enter
mcgs
133.33
0.0
University
Hydromorphone
Tarpenadol
1.3
25
0.0
0.0
Hospitals Opioid
Equivalent to Number of patches Estimated daily
Calculator
10mg oral applied daily OME
Patch (mcg/hr)
morphine (column E)
sulphate
5 12 0.0
Buprenorphine
10 24 0.0
(changed weekly)
20 48 0.0
Buprenorphine 35 84 0.0
(changed every 3 - 4 52.5 126 0.0
days) 70 168 0.0
12 45 0.0
25 90 0.0
Fentanyl
50 180 0.0
(changed every 72 hours)
75 270 0.0
100 360 0.0
Total estimated
daily OME: 0.0Results
• 27 out of 36 practices participated (more surgeries now undertaking the work)
• £14,983 (53/72 points) awarded
• 227 patients identified on high dose opioids (>120mg OME/24 hrs)
• 210 patients (93%) reviewed
• Origin of dose escalation above 120mg OME/24 hrs
123 patients (54%) by primary care
44 patients (19%) by a specialist
60 patients (26%) unknown origin
• 119 patients (52%) were undergoing a dose reduction
• 70 patients (31%) had their dose decreased to0
1
2
3
0.5
1.5
2.5
01/08/2014
01/10/2014
01/12/2014
01/02/2015
01/04/2015
01/06/2015
01/08/2015
Open Prescribing
01/10/2015
01/12/2015
01/02/2016
01/04/2016
01/06/2016
01/08/2016
01/10/2016
01/12/2016
01/02/2017
01/04/2017
01/06/2017
01/08/2017
01/10/2017
High Dose Opioids / 1000 Patients
01/12/2017
01/02/2018
01/04/2018
01/06/2018
01/08/2018
01/10/2018
High Dose Opioids / 1000 Patients
01/12/2018
01/02/2019
01/04/2019
01/06/20190
5000
10000
15000
20000
25000
30000
35000
40000
01/08/2014
01/10/2014
01/12/2014
01/02/2015
01/04/2015
01/06/2015
Open Prescribing
01/08/2015
01/10/2015
01/12/2015
01/02/2016
01/04/2016
01/06/2016
01/08/2016
01/10/2016
01/12/2016
01/02/2017
01/04/2017
01/06/2017
01/08/2017
01/10/2017
01/12/2017
01/02/2018
Total opioid prescribing (OME) / 1000 patients
01/04/2018
01/06/2018
01/08/2018
01/10/2018
01/12/2018
01/02/2019
01/04/2019
Total Opioid Prescribing OME / 1000 Patients
01/06/2019Patient Quotes Post-Reduction
• “I’m absolutely delighted, I’ve got my life back”
• “So so pleased that I am off those horrible things. They were controlling my life”
• “Very happy with decrease! My sex drive back which has saved my relationship ”
• “I used to fall or nearly fall on a weekly basis and that’s stopped now”
• “It has completely changed my life. I’m back to work, lost 2 stone, exercising – it’s
amazing!”
• “I feel so much better on the lower dose and I want to keep going” – “I have more
energy, a better memory and it has improved my mood”
• “I’m so proud of myself. I was on tramadol & diazepam & now I feel so much
better. I’m so grateful!”
• “I’m so happy. I’ve now stopped taking all morphine [zomorph, mst, oramorph].” “I
used to feel like I was in a bubble, my thoughts weren’t clear. I worry what I used
to say to people as a result.” “I can now engage in life & my pain is the same as it
was when I was on high dose”Patient Experience Video
Surgery Feedback
• ‘Opioid reduction is a time consuming yet highly rewarding intervention’
• ‘The results are rewarding and well worth the efforts’
• ‘I have observed a very apparent improvement in quality of life of patients who have achieved reduction. Feedback
from these patients is that they feel more energised, engaged and happier’
• ‘Pharmacist and GPs worked together as a team and discussed patients at the weekly clinical meetings to ensure that
patients were given consistent advice’
• ‘We [GPs] now barely see these patients & they used to come in for appointments with us all the time’
• ‘Patients were introduced to the practice pharmacist as the expert in opiates’
• ‘This has encouraged us to look further into alternative ways to manage chronic pain such as acupuncture, craniosacral
therapy, massage and health coaching’
• ‘Community navigators can be very helpful to address the complex social and emotional factors which influences the
perception of pain experience’
• ‘Early intervention post-discharge to manage patient expectations and reduce long-term opioid exposure’
• ‘Defining “when required” doses to prevent dose creeping up (e.g. with morphine sulphate 10mg/5ml oral solution).
Stating max dose per day & providing the correct amount improves adherence & allows us to monitor use & facilitate
slow reduction’
• ‘Questionnaires designed to ask about % pain relief obtained were not helpful ‘
• ‘Make yourself available & stay in regular contact with every patient undergoing reduction’
• ‘Use the (long list of) adverse effects – see what resonates with your patient – what could they gain?’
• ‘Use patient experience quotes – there are so many!’Advice for Hospital Pharmacists
• Survey of 264 patients – JAMA:
Prescribing fewer opioid tablets was associated with lower postoperative opioid use
Pre-operative education was associated with lower duration & quantity of
postoperative opioid use
• Discharge Summaries:
• Define the recommended duration of opioid use
• e.g. ‘acute use’ or ‘short term use’ - not ‘To Continue’
Facilitate early reduction & cessation of treatment
Help manage patient expectations from the initial decision to prescribe - only intended
as a short-term measure
Reduce the risk in this patient group
• Marsdon use a post-surgical agreement & follow up everyone d/c on opioids post-op
• All opportunities should be taken to review opioid prescribing for chronic pain and reduce
risk
It is everyone’s responsibility to question opioid prescribingRecent Publications
• Effectiveness of opioids for chronic non-cancer pain (The Journal of Pain, 2018)
• A two-year multicenter, prospective cohort study with propensity score matching
Opioid users reported no improvement in:
Pain symptoms
Functional outcomes
Quality of life
• 2018 Briefing Statement to Health Professionals
Faculty Of Pain Medicine (Royal College of Anaethetists)
• There is an urgent need to:
Screen and assess people on opioids
Make clinical decisions about opioid reduction and optimal pain management
Identify the best clinical approach and place for this to occur
Ensure that there are resources to deal with those patients captured
The required services need to be fully commissioned to support patientsHow?
• Initial consultation:
F2F
Education, explanation, lack of efficacy, risks, benefits of reducing, patient
quotes, advice around self-help options
Build rapport
A team, joint decision making (stress that you are here for them)
Involve & educate close family, carers, patient's health care team as appropriate
Reduce the total opioid dose by 10% every 1 - 2 weeks (to prevent unpleasant
withdrawal effects)
Individualise - Can be slower or with smaller reductions and can be paused
• Subsequent consultations:
Weekly / bi-weekly telephone calls
Discuss how the patient is doing. Focus on support, coaching & encouragement
Agree on the next reductionAlternative Treatment Options
• Mindfulness (e.g. ‘Headspace’ phone app)
• Acupuncture
• Tai Chi
• Slow Movement
• Yoga / Stretch & Relax Sessions (e.g. You Tube)
• Pilates Pain
• Walking (e.g. Health Walks)
Mood Sleep
• Gardening / Art / MusicSome Good Resources for Patients / Clinicians • My Live Well with Pain (patients) and Live Well with Pain (clinicians) • The Pain Toolkit • Opioids Aware the Faculty of Pain Medicine (Royal College of Anaesthetists) • RCGP top 10 tips: dependence forming medicines • Oxford University Hospitals Resources for GPs regarding opioids and chronic pain • Book - Explain Pain • PrescQIPP elearning: Reducing opioid prescribing in chronic pain • SPS Opioids, the Story so far… • NHS Choices: 10 ways to reduce pain • NHS Active walking • The Good Relaxation Guide and The Good Sleep Guide • Northumberland, Tyne & Wear NHS Foundation Trust - Excellent Self-Help leaflets & Audio Relaxation Techniques • Mind: Tips for everyday living • Mindfulness phone apps e.g. Headspace • Videos: Understanding Pain in Less than 5 Minutes “Brainman stops his opioids” It's time to rethink persistent pain: Tame the Beast Chartered society of physiotherapy: 10 Things You Need To Know About Your Back & Advice on Managing Back Pain
Take Home Messages • Chronic pain = a long term condition • Set Patient Expectation: 30-50% reduction in pain – AT BEST from medication • Patients were escalated to this dose historically due to the belief that chronic pain should follow the WHO analgesic ladder. We now know that opioids do not help chronic pain and have substantial long term risks, as well as reducing patients quality of life • Opioids = Ineffective, Dangerous & Reduce Quality of Life • The strongest evidence is for emotional support, wellbeing, physical therapies and lifestyle modification / adaptation – Holistic approach • Knowledge, confidence & skills = patient activation (NHS Long Term Plan) • Health Coaching (PLS event?) • Get them moving – Pacing - Increase muscle mass, strength & function • ‘The results are rewarding and well worth the efforts’ • It is everyone’s responsibility to question opioid prescribing
Thank you • Senior Medicines Optimisation Pharmacist Brighton & Hove CCG (Pain & Substance Misuse) • Clinical Pharmacist (Independent Prescriber) Wellsbourne Healthcare CIC (GP Surgery) (Chronic Pain Clinic) • BH CCG Prescribing Incentive Scheme 2017-18 • kathryn.steele2@nhs.net
You can also read