Gastroesophageal Reflux Disease - Sutep Gonlachanvit GI Motility Research Unit Department of Internal Medicine Chulalongkorn University
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Gastroesophageal Reflux Disease
Sutep Gonlachanvit
GI Motility Research Unit
Department of Internal Medicine
Chulalongkorn University
GERD - New Definition
GERD is a condition which develops when the reflux
of stomach content causes troublesome symptoms
and / or complications
Esophageal Extra-esophageal
Syndromes Syndromes
Symptomatic Syndromes with Established Proposed
Syndromes Esophageal Injury Association Association
Typical reflux Reflux esophagitis Reflux cough Sinusitis
syndrome Reflux stricture Reflux laryngitis Pulmonary
Reflux chest Barrett's fibrosis
Reflux asthma
pain syndrome esophagus Pharyngitis
Reflux dental
Adenocarcinoma erosions Recurrent otitis
media
Vakil et al. Can J Gastroenterol 2005
Causes of increased exposure of
the esophagus to gastric refluxate
Defective
esophageal
clearance
LES
‘dysfunction
Hiatal hernia
’
Delayed gastric
emptying Increased intra-abdominal
pressure
Katzka & DiMarino 1995
4 Gonlachanvit-GERD
Time Trends of GERD symptoms: Review of
Cross-sectional population-based studies
Prevalence of at least weekly heartburn and / or acid regurgitation
35
Europe
30 USA
ASIA
South America
Prevalence
25
(%)
20
15
10
5
0
1980 1985 1990 1995 2000 2005 2010
Date of publication
EL-Serag HB. Clin Gastroenterol Hepatol. 2007;5:17-26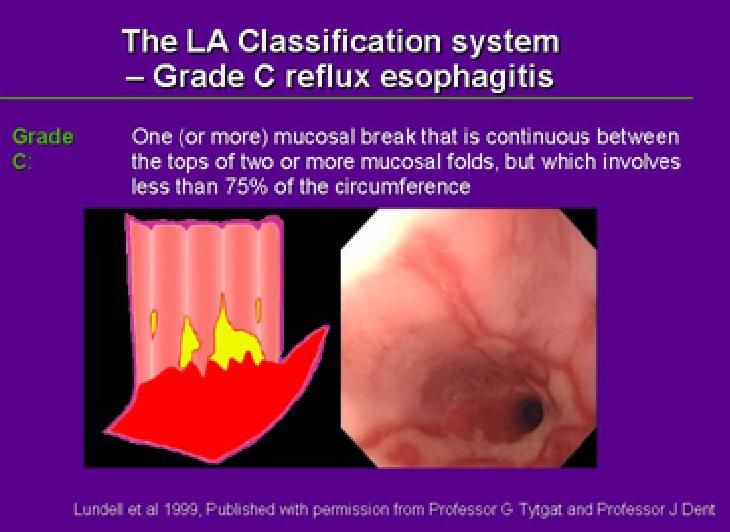
5 Gonlachanvit-GERD
The Changing Epidemiology
of GERD Complications
Esophageal Adenocarcinoma
Melanoma
Prostate Cancer
Breast Cancer
A 6-fold increased incidence Lung Cancer
of adenocarcinoma was Colorectal Cancer
found from 1975-2001 7
Rate Ratio (Relative to 1975)
The rate of increase of 6
adenocarcinoma is greater 5
than
Melanoma 4
Prostate cancer 3
Breast cancer
2
Lung cancer
Colorectal cancer 1
0
1975 1980 1985 1990 1995 2000
Pohl, Welch. J Natl Cancer Inst. 2005;97:142-146.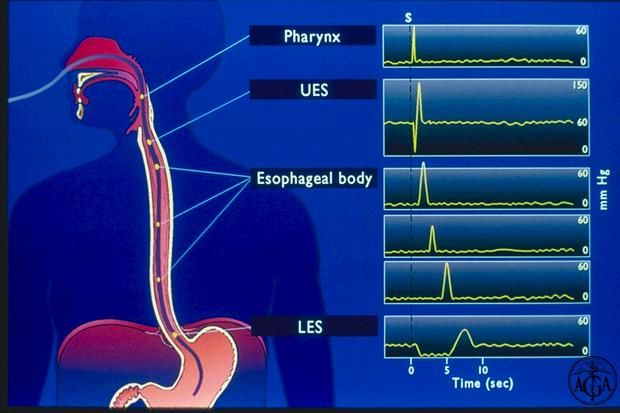
6 Gonlachanvit-GERD
Factors Responsible for the
Changing Epidemiology of GERD
Increased longevity1
Obesity epidemic2
Comorbid conditions affecting the
esophagus3
Use of drugs that affect LES pressure and
gastric emptying3
Self-treatment / access to OTC Medications?
1. Lee et al. Clin Gastroenterol Hepatol. 2007;5:1392-1398.
2. Watanabe et al. J Gastroenterol. 2007;42:267-274.
3. Bonatti et al. J Gastrointest Surg. 2007; Epub ahead of print.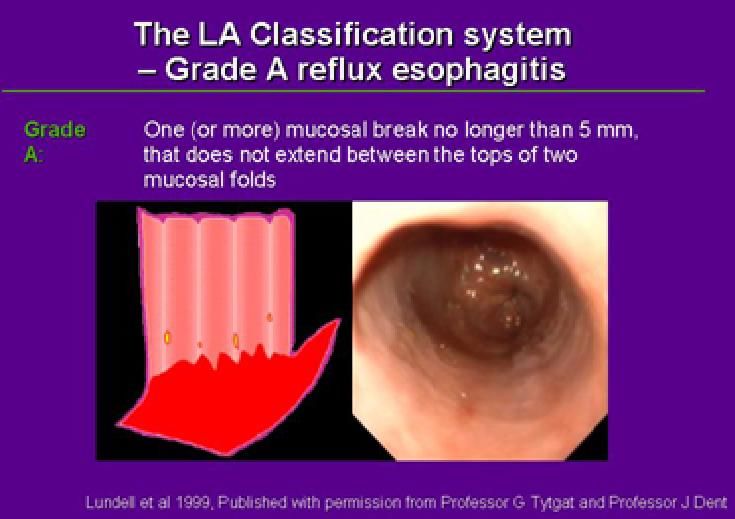
7 Gonlachanvit-GERD
Higher Body Mass Index Increases
Risk of GERD Symptoms
• Even moderate weight gain among persons of normal weight
can cause or worsen reflux symptoms
• Weight loss is associated with a decreased risk of symptoms
Multivariate odds ratio
for reflux symptoms
4
3.5 P < .001 for trend
3
2.5
2
1.5
1
0.5
0
< 20 20 - 22.4 22.5 - 24.9 25 - 27.4 27.5 - 29.9 30 - 34.9 ≥ 35
Body mass index (kg/m2)
N = 2306 women with at least weekly GERD
symptoms and 3904 with no symptoms Jacobson BC, et al. N Engl J Med. 2006;354:2340-2348.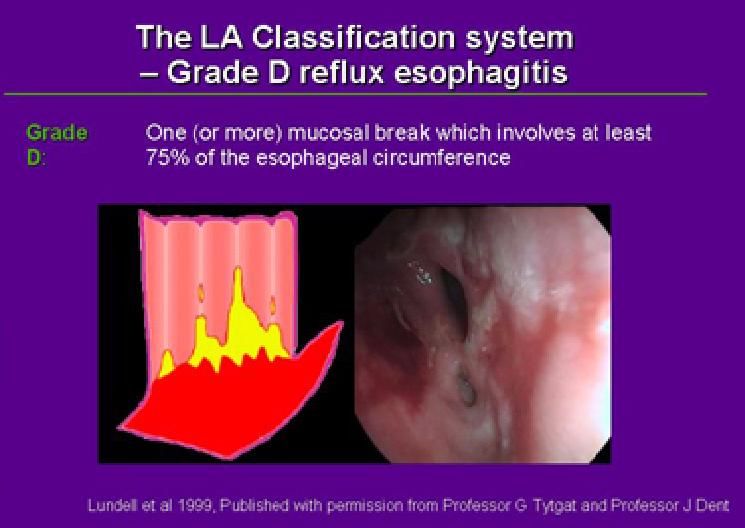
8 Gonlachanvit-GERD
Obesity in Thailand (2004)
50%
37%
26%
Women
25%
18% 16% 16% Men
9%
0%
BMI 25-30 >30 Abd Obesity
• Rate of obesity significantly increased from 1997 to 2004
• Persons living in urban areas more likely to be obese than those in rural areas
Aekplakorn et al. Obesity 2007; 15: 3113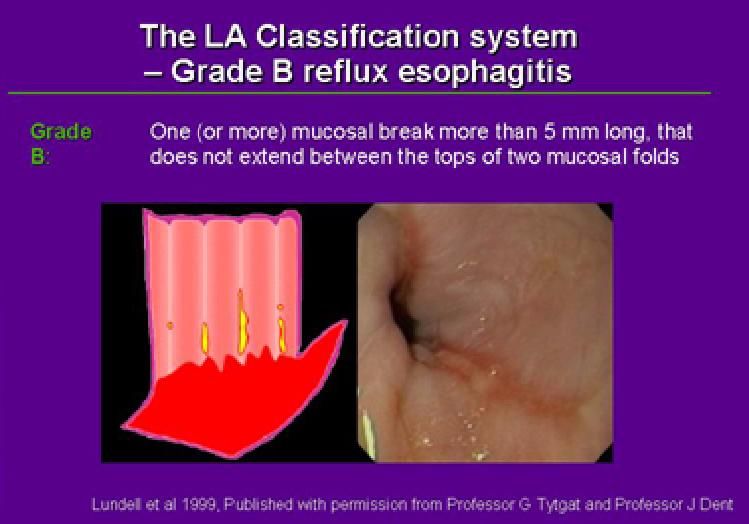
Diagnosis : Reflux symptoms
When patients present predominantly with
heartburn and acid regurgitation, there are
59-78 % of sensitivity and 60-66 % of
specificity for diagnosis of GERD.
Heartburn and acid regurgitation without
dyspeptic symptoms are more specific for
GERD than heartburn and acid
regurgitation with other GI symptoms*.
* Klauser AG et al. Lancet 335:205, 1990.
Heartburn and Acid Regurgitation in GERD: Thai vs
Germany
PGERD symptom score
Placebo Capsicum
**
**
**
[mean + SE(* p value ≤ 0.05, ** p value ≤ 0.01)]
Digestive Disease Week 2009Diagnosis : Endoscopy Endoscopy is the most useful available tests for assessing reflux esophagitis as well as its complications such as stricture and Barrett’s esophagus. Sensitivity = 20-68 %, specificity = 96 % Sensitivity is depended on the prevalence of NERD in the population. Indications for endoscopy are: A brief history of symptoms in older patients (>50 yr) Weight loss Dysphagia or bleeding Failure to respond to antireflux medications. Long history of reflux symptoms (>5 years)
Endoscopy : Reflux esophagitis
Causes of Dyspepsia in CU Hospital During 2000-2002
(Endoscopic data, N=1,708)
100
90
80.7
80
70
60
50
40
30
20
10.71
10 4.5 2.5
0.9 1.05
0
GU DU GU+DU GERD Ca NUD
stomach15 Gonlachanvit-GERD
Do symptoms predict the presence of EE?
1011 consecutive pts at the Mayo Clinic
undergoing EGD for GERD symptoms
Completed validated GERQ survey
20% had erosive esophagitis
Erosive esophagitis associated:
With age, gender, heartburn frequency and any
regurgitation or dysphagia (P16 Gonlachanvit-GERD
Esophageal Manometry
Water
Perfused
Manometry
System
High
Resolution
Manometry
System17 Gonlachanvit-GERD
Diagnosis
24 hour esophageal pH monitoring
The gold standard for measuring esophageal acid
exposure
Indications for 24 hr esophageal pH monitoring
When patients present with atypical symptoms, such as NCCP
and ENT symptoms
When symptoms do not respond to conventional medications
In preparation for antireflux surgery
In difficult cases, for evaluation the adequacy of antireflux
medications
pH monitoring parameters:
Quantitation of the actual time the esophageal mucosa is exposed
to gastric juice
Measurement of the esophageal ability to clear refluxed acid
Correlation of reflux episodes with symptoms18 Gonlachanvit-GERD
24 hour esophageal pH monitoring19 Gonlachanvit-GERD
20 Gonlachanvit-GERD
Multichannel Intraesophageal
Impedance – pH (MII-pH) Monitoring21 Gonlachanvit-GERD
Esophageal impedance testing
Swallow Reflux
Bolus Movement
Bolus Entry Bolus Entry
Bolus Entry Bolus Entry
Bolus Entry Bolus Entry
Bolus Entry Bolus Entry
Bolus Entry Bolus Entry
Bolus Entry Bolus Entry
Bolus Movement22 Gonlachanvit-GERD
Multichannel Intraesophageal Impedance – pH
(MII-pH) Monitoring
An Acid Reflux23 Gonlachanvit-GERD
Multichannel Intraesophageal Impedance – pH
(MII-pH) Monitoring
Non Acid Reflux24 Gonlachanvit-GERD
37 patients with non-diagnostic EGD
and previous normal 24 hr. pH study
24 hr. MII pH testing
6 patients (16%) 7 patient (18%)
Positive standard Negative symptom index
24 hr pH test
10 patients (27%) 14 patients (38%)
Positive symptom index Positive symptom index
for acid reflux for non-acid reflux
Kline et al. Clinical Gastroenterol and Hepatol 2008; 6: 880–88525 Gonlachanvit-GERD
168 Patients with Persistent Symptoms
on Medication
Impedance-pH Monitoring on Medication
144 Patients Symptomatic During Study
Acid Reflux Reflux Not
Associated with Symptom Associated with Symptom
11 % (16 patients) 52 % (75 patients)
Nonacid Reflux
Associated with Symptom
37 % (53 patients)
Mainie et al. Gut 2006;55;1398-140226 Gonlachanvit-GERD
Multichannel Intraesophageal
Impedance – pH (MII-pH) Monitoring
MII-pH is superior to standard pH monitoring for
evaluation of non-acid refluxes.
More sensitive than standard pH monitoring for
detecting of GER during on PPI therapy.
Demonstrate extent of GER.
Demonstrate liquid, gas, mix liquid-gas refluxes.PPI Test in Thai GERD Patients
Effect of PPI test on GERD and the other symptoms in all
patients
1.8
1.6
Symptom scores
1.4
Baseline
1.2 *
1 * * End of
0.8 * treatment
*
0.6
*
0.4
0.2
*
0
* P ≤ 0.05PPI tests for diagnosis of GERD Sensitivity 34.3% Specificity 46.4% Positive predictive value 44.0% Negative predictive value 36.0% Accuracy 60.3%
Non-Cardiac Chest
PainEsophageal manometry & Total % time pH < 4 in NCCP
N=45
Total % time pH < 4
< 4.5 % > 4.5 % Total
EM Normal
7 10 17
NSEMD
5 8 13
Hypertensive LES
2 0 2
Scleroderma like
0 2 2
DES 3 2 5
Nutcracker
1 2 3
Missing data
3 0 3
Total 21 24 45
P > 0.05Extraesophageal GERD (LPR)
Nov 05% of ENT Symptoms in Patients Referred for pH Monitoring (N=59)
70
60
% of Patients
50
40
30
20
10
0
Globus Hoarseness Sore throat Clearing throat Chr coughDual Channel 24 hour esophageal pH monitoring
Diagnosis of GERD in ENT Patients (Gold Standard = 24 hr pH
Monotoring)
Abnormal upper esophageal pH Abnormal lower esophageal pH
(pH 1%) (pH 4%)
GERD GERD
48% 47%
52% 53%
Non Non
GERD GERDPrevalence Prevalence of GERD in Thai Asthma patients using 24 hr pH monitoring (n=56) Prevalence 37.50% 15 pts (71.43%) had GERD symptoms Jaimchariyatam N, Wongtim S, Udompanich V, Sittipunt C, Kawkitinarong K, Chaiyakul S et al. J Med Assoc Thai 2011; 94(6):671-678.
Uncontrolled Asthma and GERD
The association between GERD and level of
asthma control by ACT score at KCMH
GERD in partly controlled asthma
prevalence = 25.72%
GERD in uncontrolled asthma
prevalence = 51.17%
GERD in poorly controlled asthma
prevalence = 80.89%
Wongtim S., et al 2009GERD is common in Thailand. Around 50% of patients with typical or atypical GERD symptoms have positive pH tests. Heartburn is less prevalence in Thai GERD patients. GERD patients with atypical symptoms are more common than typical GERD at KCMH. PPI tests in Thai patients at tertiary care center provide low sensitivity and specificity for diagnosis of GERD.
Treatment of GERD Benefit of GERD Treatment Decrease mortality = No evidence support Decrease morbidity = Yes, prevent stricture and bleeding esophageal ulcer Relieve GERD symptoms = Yes Improve quality of life = Yes
Impact of Lifestyle
Modification on GERD
16 trials examined effectiveness of lifestyle changes
Lifestyle Change Effect
Tobacco cessation No significant effect
Alcohol cessation No significant effect
Weight loss Improved pH metry results and symptoms
Elevation of head of bed Improved pH metry results and symptoms
Left lateral decubitus position Raised LES pressure, improved pH metry results
Lifestyle changes are logical and may work if used on an individual basis
LES = lower esophageal sphincter
Kaltenbach T, et al. Arch Intern Med. 2006;166(9):965-971.GERD Management
Uninvestigated GERD
Non-erosive reflux disease (NERD)
Reflux esophagitis (RE)Non-erosive reflux disease (NERD)
NERD
Abnormal increase acid exposure (Typical NERD)
Normal acid exposure but positive symptom index
(esophageal hypersensitivity to acid)
F:M = 1:1
Unlikely to progress to erosive reflux disease
Heartburn severity and effect on QOL is similar to
erosive reflux disease.
May have symptoms of dyspepsia
Aim of treatment = control symptomsErosive reflux disease ERD = reflux symptoms + esophagitis (Gr C or D on endoscopy M>F (2-3:1) May progress to more severe esophagitis and stricture. In severe esophagitis, after stop antireflux medications, 80 % of patients have symptom recurrence within 6 months. Aims of treatment Mild esophagitis = controls symptoms Severe esophagitis = controls symptoms, heals esophagitis, and maintains remission of symptoms and esophagitis.
GERD Management
Uninvestigated GERD
Non-erosive reflux disease
(NERD) Healing and
Maintenance of
Esophagitis
Reflux esophagitis (RE) Induce symptom
remission and
prevent symptom
recurrenceSpeed of Healing of Reflux Esophagitis
Esophagitis cases healed
%
100 Room for
improvement ! 83.6 PPIs
80
60 51.9 H2-receptor pSpeed of Symptom Resolution in
Patients with Reflux Esophagitis
Patients free from heartburn %
80 Room for PPIs
improvement !
pGERD tends to be a chronic condition
100
No mucosal breaks
LA grade A
symptomatic remission
80
LA grade B
% patients in
60 LA grade C
40
20
0
0 1 2 3 4 5 6
Time after cessation of therapy (months)
Lundell et al. Gut 1999Maintenance Therapies for Healed Erosive
Esophagitis
Cochrane systematic review
of 36 controlled trials
100
80
80
60 55
45
40 32
19
20
0
Placebo H2RA Prokinetics Half-dose Full-dose
PPI PPI
Donnellan C, et al. Gastroenterology. 2003;124:A108.GERD Management
Uninvestigated GERD
Induce symptom
Non-erosive reflux disease remission and
(NERD) prevent symptom
recurrence
Reflux esophagitis (RE)On demand therapy
Symptom Response with On-demand vs.
Continuous PPI Therapy for GERD
100% 86%
75%
Response to PPI (%)
75%
176 pts with END or
50% Grade I/II esophagitis
and >moderate H-burn
who improved with
25%
rabeprazole 10mg/d
0%
Continuous On-demand
Bour et al. Aliment Pharm Ther 2005;21:805Treatment of Uninvestigated GERD
Uninvestigated GERD with Empiric
no Alarm Symptoms Therapy
Alarm Symptoms
Non-erosive reflux disease
Weight loss
(NERD) Dysphagia
Odynophagia
Bleeding, anemia
Reflux esophagitis (RE) Frequent vomiting
Recent onset in old
age
Long duration of
symptomsGERD: Initial Management
The fastest, most
economical path to:
Step-in
Empirical Symptom relief
with a PPI
therapy
for 4 weeks Diagnostic
confirmation
After O'Connor et al. Am J Gastroenterol 2000
Dent, Talley. Aliment Pharmacol Ther 2003 (Suppl 1)
Dent et al. Gut 2004 (Suppl 4)GERD: Long-term management
Continuous daily
Step down therapy
Empirical to the lowest
therapy dose that Intermittent
controls courses of therapy
successful
symptoms
On-demand therapy
Dent & Talley. Aliment Pharmacol Ther 2003 ( Suppl 1)
Dent et al. Gut 2004 (Suppl 4)Treatment of Uninvestigated GERD
On demand PPI vs Maintenance Therapy PPI and H2
Receptor Antagonist
Hansen AN, et al. Int J Clin Pract 2006, 1, 15-22Algorithm for the management of Typical GERD in
primary care
Typical GERD Symptoms
Alarm features present Alarm features absent
PPI test
Symptom persist Symptom respond
NERD: On demand Rx
Refer for EGD Maintain therapy
Erosive: Maintenance for 4 weeks
Frequent relapses,
alarm features On-demand
therapySafety of Long-Term PPI Therapy in GERD
Enteric Infection
- Increased risk of Clostridium difficile infection in PPI users
- Risk Increased from 0.02% to 0.06%
Pneumonia
- Flawed study as they did not control for important
confounders
- Adjusted relative risk 1.89 (1.3-2.6)
Osteoporosis
- Increased risk of hip fractures
- Adjusted OR 2.65 (1.8-3.9)
Rebound Symptoms
Drug Interaction
OR = odds ratio.
Dial S, et al. JAMA. 2005;294(23):2989-2995. Laheij RJ, et al. JAMA. 2004;292(16):1955-1960. Yang YX, et al.
JAMA. 2006;296(24):2947-2953. Giten D, et al. Gastroenterology. 1999;116:239-247.Effect of Omeprazole on The Antiplatelet Activity
of Clopidogrel
The variability in the response
to clopidogrel has been linked,
at least in part, to its
cytochrome P450–dependent
metabolism steps including
CYP2C19 and CYP3A4.
Gilard M, et al. J Am Coll
Cardiol 2008; 51(3):256-260.Effect of PPI on Recurrent MI
(13,636 cases vs 2,057 controls)
Juurlink DN, Gomes T, Ko DT, et al. CMAJ. 2009; DOI: 10.1503/cmaj.082001.61 Gonlachanvit-GERD
Methods
Multicenter, international, randomized, double-blind, double-
dummy, placebo-controlled, parallel group, phase 3 efficacy and
safety study of CGT-2168, a fixed-dose combination of
clopidogrel (75 mg) and omeprazole (20 mg), compared with
clopidogrel.
Patients were stratified based on two baseline factors: H. pylori
serology (positive or negative) and concomitant use of any
NSAID.
All patients were to receive enteric coated aspirin at a dose of
75 to 325 mg.
COGENT — Presented at TCT 2009
http://www.cardiosource.com/clinicaltrials/trial.asp?trialID=187262 Gonlachanvit-GERD
Results
3627 patients (above the initial target of 3200)
393 sites
Median follow-up 133 days (maximum 362 days)
136 adjudicated cardiovascular events (preliminary)
105 adjudicated GI events (preliminary)
143 had been planned
COGENT — Presented at TCT 2009
http://www.cardiosource.com/clinicaltrials/trial.asp?trialID=1872Baseline Characteristics
Variable Treated Placebo p-value for
n (%) n (%) difference
H. Pylori Positive 923 (49.2) 926 (49.0) 0.938
Used NSAIDs 116 (6.2) 105 (5.6) 0.456
Sex – Male 1251 (66.7) 1313 (69.6) 0.061
White/Black/Other 1756/68/51 1769/63/56 0.808
History of ACS 669 (36.1) 699 (37.5) 0.382
History of MI 484 (26.1) 466 (25.0) 0.468
History of PAD 172 (9.3) 158 (8.5) 0.426
History of Stroke 208 (5.8) 114 (6.1) 0.757
Mean (SD) Mean (SD)
Median Median
Age 67.2 years (10.8) 67.2 years (11.1) 0.984
68.7 years 68.6 years
BMI 29.2 kg/m2 (5.6) 29.2 kg/m2 (5.3) 0.655
28.4 28.3
COGENT — Presented at TCT 2009
http://www.cardiosource.com/clinicaltrials/trial.asp?trialID=1872Survival Curves for PPI Treated vs Placebo
Composite Cardiovascular Events
1.00
0.98
Survival Probability
0.96
Placebo: 67 events, 1821 at risk
HR = 1.02
0.94
Treated: 69 events, 1806 at risk
95% CI = 0.70; 1.51
Placebo
0.92
Treated
Adjustment through Cox Proportional Hazards Model
Adjusted to Positive NSAID Use and Positive H. Pylori Status
0.90
0 30 60 90 120 150 180 210 240 270 300 330 360 390
Days
COGENT — Presented at TCT 2009 http://www.cardiosource.com/clinicaltrials/trial.asp?trialID=1872Survival Curves for PPI Treated vs Placebo
Revascularization
1.00
0.98
Treated
Placebo
Survival Probability
0.96
0.94
HR = 0.95
95% CI = 0.59; 1.55 Placebo: 67 events, 1821 at risk
Treated: 69 events, 1806 at risk
0.92
0.90
Adjustment through Cox Proportional Hazards Model
Adjusted to Positive NSAID Use and Positive H. Pylori Status
0 30 60 90 120 150 180 210 240 270 300 330 360 390
Days
COGENT — Presented at TCT 2009
http://www.cardiosource.com/clinicaltrials/trial.asp?trialID=1872Survival Curves for PPI Treated vs Placebo
1.00 MI Events
Treated
0.98
Placebo
Survival Probability
0.96
0.94
HR = 0.96
95% CI = 0.59; 1.56 Placebo: 37 events, 1851 at risk
Treated: 36 events, 1839 at risk
0.92
Adjustment through Cox Proportional Hazards Model
0.90
Adjusted to Positive NSAID Use and Positive H. Pylori Status
0 30 60 90 120 150 180 210 240 270 300 330 360 390
Days
COGENT — Presented at TCT 2009
http://www.cardiosource.com/clinicaltrials/trial.asp?trialID=1872Survival Curves for PPI Treated vs Placebo
Composite GI Events
1.00
0.98
Treated
Survival Probability
0.96
0.94
Placebo
HR = 0.55
95% CI = 0.36; 0.85
0.92
p=0.007 Placebo:
Treated:
67 events, 1895 at risk
38 events, 1878 at risk
(preliminary)
0.90
0 30 60 90 120 150 180 210 240 270 300 330 360 390
Days
COGENT — Presented at TCT 2009
http://www.cardiosource.com/clinicaltrials/trial.asp?trialID=187268 Gonlachanvit-GERD
Summary
-PPIs’ side effects have been
identified reported.
- PPI should be used only in
patients who really need it.Gonlachanvit-GERD 69
Thank youYou can also read