Archives of Clinical Case Studies and Case Reports - ScieniQ ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Archives of Clinical Case Studies and Case Reports
Research Article
Medical Treatment in Uterine Adenomyosis Manage *Corresponding author
*
Kulvinder Kochar Kaur, Scientific Director, Centre for Hu-
ment – A Systematic Review man Reproduction, 721, G.T.B. Nagar Jalandhar-144001,
Punjab, India, Tel: 91-181-9501358180, 91-181-4613422;
Kulvinder Kochar Kaur1*, Gautam Allahbadia2 and Mandeep Singh3 FAX: 91-181-4613422
1Scientific Director, Centre For Human Reproduction, 721,G.T.B. Nagar Jaland-
har-144001, Punjab, India
Received: 16 Mar 2021
Accepted: 24 Mar 2021
2Scientific Director, Department of Obstetrics & Gynecology, Ex-Rotunda-A Cen-
Published: 31 Mar 2021
tre for Human Reproduction, 672, Kalpak Garden, Perry Cross Road, Near Otter’s
Club, Bandra(W)-400040, Mumbai, India Copyright
3Consultant Neurologist, Swami Satyanand Hospital, Near Nawi Kachehri, Bar- © 2021 Kulvinder Kochar Kaur
adri, Ladowali road, Jalandhar, Punjab OPEN ACCESS
Abstract
*
Adenomyosis represents a benign uterine problem that involves women at different ages presenting with a variety of symptomatology. The management
continues to be controversial till date. Very little studies that have concentrated on only medical or surgical treatment for adenomyosis have been carried
out. Till now no drug gets the label for treatment of adenomyosis, with no existing particular guidelines for getting the best method to manage a case
of adenomyosis. But still medical therapies are efficacious in aiding in improvement of symptoms like pain, abnormal uterinebleeding (AUB) as well as
infertility. The basis of using medical treatment for adenomyosis is the common etiopathogenesis with endometriosis like steroid hormone irregulari-
ties, as well as a escalated inflammation, disturbed apoptosis as well as neurogenesis. Variety of non hormonal (Nonsteroidal anti-inflammatory drugs
(NSAIDS) as well as hormonal therapies like (progestins, oral contraceptives (OC’s), gonadotropin releasing hormonal (GnRH) analogues) are used
currently off label for getting pain controlled as well as regulation of, abnormal uterine bleeding (AUB) in Adenomyosis. Prior to infertility therapies
gonadotropin releasing hormone agonist are indicated for getting pregnancy chances escalated. The anti-inflammatory as well as antiproliferative actions
of progestins like Dienogest, danazol, as well as Norethindrone acetate (NETA), point that they can be efficacious for medical therapy of adenomyosis
basically for regulating pain symptoms. Conversely the Levonorgestrel –releasing IU System (LNG-IUS) helped in marked efficacy in resolving AUB
as well as decreasing uterine volume as well as decreasing urinary symptoms for a longterm plan of management. On the basis of new findings on etio-
pathogenesis of adenomyosis and our observations innovative therapies like Selective Progesterone receptor modulators (SPRM), aromatase inhibitors,
valproic acid as well as antiplatelet therapy are under consideration.
Keywords: Adenomyosis, Dienogest, Danazol, GnRH analogues, LNG-IUS, Medical therapy, Progestins
Introduction treatment have been done these days with medical treatment demonstrate
Adenomyosis represents a uterine problem which presents with pelvic increased effectiveness in patients needing symptom control as well as in-
pain symptoms, abnormal uterine bleeding (AUB) as well as infertility [1]. fertility treatment. Basic outcome wanted for symptomatic adenomyosis is
There is a mixed type of clinical way in which a patient might present, and relief of symptoms, mainly as well as improve fertility, while minimizing
now higher pick up in lieu of good imaging diagnostic ability, adenomyo- side effects.
sis might get picked up in aymptomatic cases also [2-6]. Based on the age
of a woman, her reproductive status, clinical features, adenomyosis might Rationale for using medical therapy is based on the pathogenic mode of
need lifelong plan, where medical, surgical as well as infertility therapy adenomyosis, most of which are shared with endometriosis. Adenomyosis
might have a part alone or in combination [7]. actually is a sex hormone dependent problem, with property of escalated
inflammation, disturbed apoptosis as well as neurogenesis [11,12] (Fig-
Now adenomyosis is no longer thought to be a disease typical of >40yrs ure 1). Various nonhormonal(nonsteroidal anti-inflammatory drugs[N-
women as considered earlier and about 30% of young women might be SAIDS] as well as hormonal therapies (i.e progestins, oral contracep-
afflicted with adenomyosis [8]. Further adenomyosis gets diagnosed in tives(OC’s), gonadotropin releasing horomone(GnRH) analogues) are the
22% of infertile women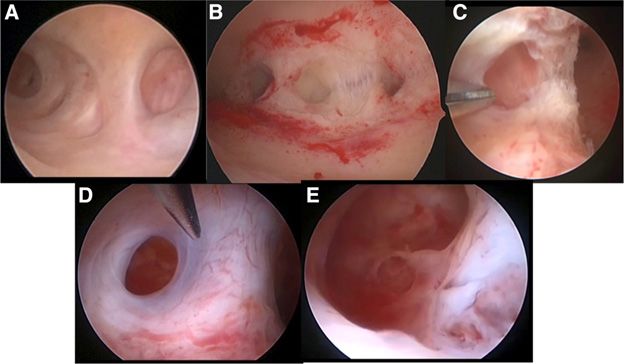
Figure 1: Courtesy ref no-11-Invagination of the endometrial basalis: hyperestrogenism, hyperperistalsis, and TIAR mechanism activation. (A) A hyper-
estrogenic condition in the eutopic uterus may lead to increased proliferation in the endometrial basalis and tissue microtrauma in the vicinity of the JZ,
thus allowing endometrial intramyometrial invagination. (B) As a consequence of tissue microtrauma, the TIAR mechanism is activated (blue arrows),
generating a mechanism of positive feedback whereby estrogen production promotes uterine peristalsis and further autotraumatization, progressively
worsening the microtrauma and endometrial invagination and eventually leading to adenomyosis establishment.
Methods
We conducted a systematic review using the pubmed search engine using TVS (Transvaginal Sonography and MRI (Magnetic
the MeSH terms like GnRH agonists; GnRH antagonists; danazol; proges- Resonance Imaging) and Hysteroscopy
tins; dienogest; NETA; antiplatelet therapy; histone deacetylate inhibitors, Bazot M, Darai E. recently suggested a classification of adenomyosis ac-
therapy in infertile women from 1975 till date. cording to MRI features which allows us to distinguish between internal
adenomyosis, external adenomyosis andstructural-related adenomyoma
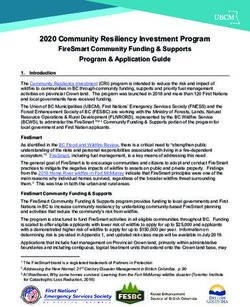
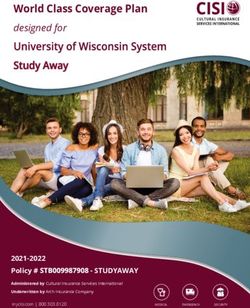
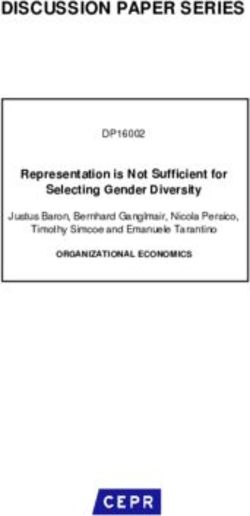
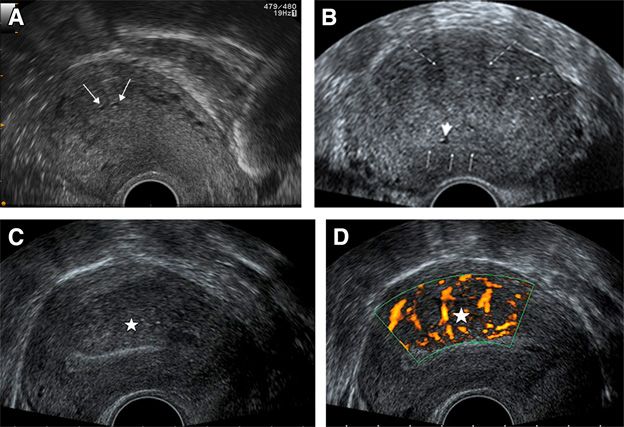
Results and Discussion subtypes with a potential relation for therapeutic strategy (Figure 2-4 for
We found a total of 1731 articles out of which we selected 93 articles for classification, TVS and MRI images) Internal, external adenomyosis, and
this review. No meta-analysis was done. adenomyomas can be present alone or in association in this model [16].
Current classification proposals and future perspectives are discussed
Diagnosis more extensively by Gordts et al. Further they discuss role of hystereosco-
Initially we give a little information regarding how to confirm diagnosis py [17] (Figure 5 for hysteroscopic images).
using TVS as well as magnetic resonance imaging (MRI) and hysteroscopy
if required only.
Archives of Clinical Case Studies and Case Reports, 2021
Volume 2 | Issue 3 | 190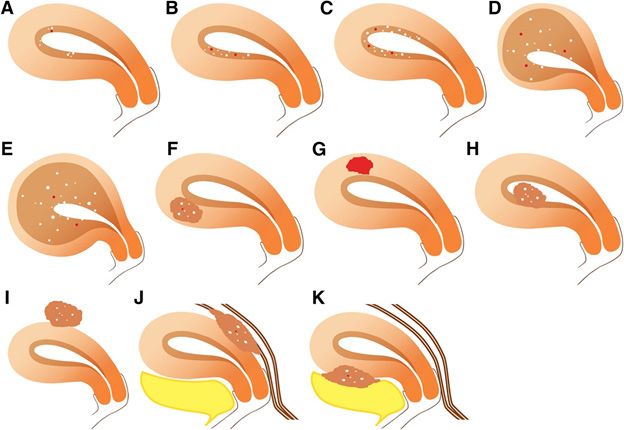
Figure 2: Coiurtesy ref no 16 -Magnetic resonance imaging classification of adenomyosis: different morphologic and locations of adenomyosis subtypes including internal adenomyosis, adenomyomas, and external adenomyosis. (A) Internal adenomyosis comprised focal or multifocal adenomyosis, (B) superficial asymmetric or (C) symmetric adenomyosis, and (D) diffuse asymmetric or (E) symmetric adenomyosis. Adenomyomas are related to intra- mural adenomyoma, (F) solid or (G) cystic and (H) submucosal or (I) subserosal adenomyomas. External adenomyosis are represented by (J) posterior adenomyosis and (K) anteriorassociated respectively with posterior and anterior deep endometriosis. Figure 3: Cortesy ref no-16-Transvaginal sonographic examinations in different patients showing (A) tiny subendometrial cysts (arrows) related to focal internal adenomyosis; (B) regular enlarged asymmetric heterogeneous myometrium containing multiple hypoechoic striations (dotted arrows), tiny myometrial cystic (short arrow) adjacent to poor definition of the endometrial-myometrial interface (thin arrows) related to diffuse adenomyosis; and (C, D) large posterior hypoechoic myometrial area (star) containing vessels following their course perpendicular to the endometrial interface due to diffuse adenomyosis. Archives of Clinical Case Studies and Case Reports, 2021 Volume 2 | Issue 3 | 191
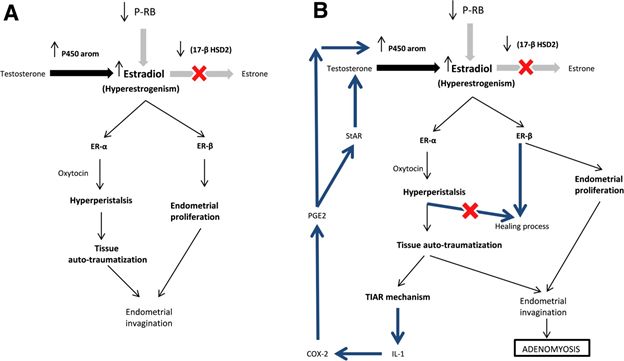
Figure 4: Courtesy ref no-162DT2-weighted magnetic resonance imaging examinations of two different women. (A) A normal uterus with localized high intense tiny cystic component (arrows) surrounded by ill-defined low intense myometrial mass related to focal internal adenomyosis; (B) a huge uterus containing multiple cystic myometrial cysts with anterior diffuse thickening of junctional zone (double arrow) on sagittal view; and (C) coronal view related to diffuse internal adenomyosis with associated leiomyomas (star). Figure 5: Courtesy ref no-16-T2-weighted magnetic resonance imaging examinations in two different women. (A) A large low intense ill-defined mass invading bladder wall, vesicouterine pouch, and adjacent anterior myometrium related to bladder endometriosis (star) with anterior external adeno- myosis (arrows); (B) retroflexed uterus presenting with normal junctional zone on sagittal view (double arrow); and (C) large posterior ill-defined low signal intense mass (star) containing tiny cystic component (thin arrow) on axial oblique view associated with uterosacral ligament thickening (dotted arrow) related to posterior deep endometriosis and posterior external adenomyosis. Figure 6: Courtesy ref n0-17Adenomyotic hysteroscopic images become pathognomic after sub-endometrial exploration: (A) visible endometrial defects on uterine septum; (B) after incision different cystic structures become visible; (C) incision of lateral wall of T-uterus reveals the presence of adenomyotic cyst; (D) formation of cyst, still small opening is present; and (E) opening of this defect shows the inner sight of the cyst. Archives of Clinical Case Studies and Case Reports, 2021 Volume 2 | Issue 3 | 192
Medical Treatments LH surge as well as raised serum free T [27,28]. The androgenic as well as
hypoestrogenic milieu have a direct action on adenomyotic lesions as well
GnRH Analogue as indirect one on symptoms [29]. In vitro studies demonstrated Danazol
Point of using GnRH analogues for medical treatment of adenomyosis is
has a direct effect on cell proliferation, via inhibition of DNA synthesis as
the direct antiproliferative action within the myometrium via action on
well as induction of apoptosis evaluated following systemic treatment with
GnRH receptors expressed on adenomyotic lesions, together with a sys-
Danazol show a decrease in E2 receptors as well as bcl protein amounts,
temic as well as local hypoestrogenic action via central downregulation
with an escalating apoptotic cell necrosis [30]. Danazol further inhibits
as well as deep suppression of gonadotropin liberation [18]. Actually ad-
lymphocytic proliferation via decrease in monocyte –increased endo-
enomyosis has property of hyperestrogenism (E2) in view of escalation of
metrial proliferation, in peripheral blood as well as escalates peritoneal
E2 receptors, activation of sulphatase as well as aromatase as well as de-
macrophage cytotoxicity Study via Ota et al. is the only randomized con-
creased catabolism of E2. This, in turn causes down regulation of proges-
trolled trial (RCT) on Danazol, compared hysterectomy vs 4mth therapy
terone(P) receptors, loss of their action, and ultimate P resistance [12]. But
with 400mg of daily danazol; post treatment antibody amounts as well as
GnRH analogues also act on other pathogenesis modes, ii) by induction
antiphospho antibody lipids(APL) amounts were reduced, in lieu of inhib-
of apoptosis in adenomyosis tissues, iii) decreased inflammation as well as
itory action of danazol on autoimmunological response correlated with
iv) angiogenesis [19]. v) Additionally GnRH analogues can cause marked
adenomyosis [31,32].
decrease in nitric oxide synthase(NOS) as well as peroxy nitrite, repressing
serum amount of nitrite /nitrate, stable metabolites of NO, that are mostly
Limited proof is there on systemic therapy of adenomyosis with danazol,
escalated in adenomyosis [20].
in view of high androgenic side effects. Igarachi was the 1st individual to
use danazol for therapy adenomyosis therapy in a separate was achieved
1st case of adenomyosis treated using GnRH analogues demonstrated sig-
in 66.6% cases Cervical injections of danazol at 12 wk interval for 12wks
nificant decrease of uterine volume, with severe symptoms getting relieved
have also got utilized success, with 60% relief in symptoms of bleeding,
[21]. Goserelin, leuprolide as well as nafarelin are commonly utilized in
pain as well as dyspareunia, as well as a decrease in uterine size [33,34].
clinical practice, causing decrease in uterine size as well as pelvic pain get-
Further an intra uterine device (IUD) loaded with 300-400 mg of danazol
ting beter as well as bleeding [13,21,22]. But the use of GnRH analogues
=>reduction of pain symptoms. At the time of treatment blood danazol
is correlated with hypoestrogenic side effects like vasomotor syndrome
were undetectable ,ovulation did not get inhibited and no side effects were
(VMS) decrease mineral density, genital atrophy as well as a mood insta-
documented [35]. The same device that was loaded with danazol was used
bility. Hence an add back therapy needs to be used for minimizing side
in a murine model, and it was visualized that as the danazol dose got esca-
effects, even if long term treatment with GnRH analogues needs to be re-
lated, the adenomyotic nodule numbers got reduced with a low as well as
stricted in women not responsive to other medicine or in surgically high
stable plasma danazol levels [36].
risk patients. But there is no specific indication on when, which type of
add back therapy needs to be used in severe VMS, or to prevent bone loss
In a prospective study it was shown that long term vaginal delivery of
on prescription of GnRH analogue is given for adenomyosis [23]. Option
200mg danazol tablet /day was efficacious in decreasing heavy menstru-
of use of long term low dose GnRH analogue, so called draw back therapy,
al bleeding as well as pain in adenomyotic women [37]. Recently it was
was checked in a small sample of women with adenomyosis. Buserelin ac-
seen that a long term treatment with a vaginal danazol can control pain as
etate /nasal administration for 2 yrs allowed maintaining E2 levels within
well as AUB in women with adenomyosis. Improvement in visual analog
therapeutic window, suppressing adverse events while maintaining thera-
score (VAS) for pain symptoms, pictorial blood loss evaluation chart for
peutic efficacy in adenomyosis [24].
uterine bleeding as well as quality of life (QOL) measures with a decrease
in uterine volume examined by USG. 6mth treatment followed by cyclical
Progestins 3mth therapy for a further18mths had the best compliance of symptomatic
A. Norethindrone Acetate (NETA) patients with adenomyosis [38].
Basis of use of NETA is on the basis of watching that Progestins.
Can inhibit e2 induced vascular endothelial growth factor (VEGF) as well The positive changes caused via danazol were marked as compared to that
as stromal cell differentiation factor1 (SDF1) in human endometrial stro- with leuprolide acetate although, even following 6 mth of therapy, men-
mal cells, decrease bleeding as well as pain [25]. Additionally progestins orrhagia as well as dysmenorrhea recurred with a few cycles of treatment
might act on the Progesterone resistance seen in ectopic as well as eutopic suspension of danazol [30].
endometrium, but also in the inner as well as outer layers of myometrium
adenomyosis [12]. C. Dienogest (DNG)
Dienogest,represents, a 19 nor testosterone derivative that is a Progestin
Efficacy of NETA in the adenomyosis management has been shown in having great selectivity for P receptors[39]. It=>mild inhibition ofovarian
women having moderate to severe pelvic pain as well as bleeding following function, with minimal hypoestrogenic actions, as well as gives an anti
5mg/d dose [26]. In this treatment group, the 3 wks on, one week off reg- proliferation effect on endometrium [40]. Cellular proliferation of adeno-
imen was used to prevent side effects of Break through Bleeding, causing myotic cells get inhibited via induction of apoptosis pathways [41]. Addi-
an incomplete suppression of the hypothalamo-pituitary-ovarian (H-P-O) tionally ,uterine samples collected following hysterectomy from women
axis as well as less hypoestrogenic action. As per these results NETA might receiving DNG therapy displayed significant alterations in histological
be thought to be efficacious, well tolerated as well as cheap medical therapy features like decrease in Cellular proliferation, nerve growth factor expres-
for adenomyosis, with few to minimal side effects. But no future studies sion as well as nerve fibre density [21]. These observations corroborate
have been carried on comparing NETA to other Progestins or other drug the clinical proof that DNG is efficacious in improving pain symptoms
and no proof available on long time actions on symptoms as well as ultra- correlated with adenomyosis. With marked alterations in immune system,
sonography(USG) as well as magnetic resonance imaging (MRI) image of with an escalating number of uterine infiltrating natural killer (NK) cells
adenomyosis following treatment. in glandular structures of eutopic endometrium, a potential advantage on
embryo implantation has also been posited [42].
B. Danazol
Danazol represents an isoxazole derivative of 12 alpha –ethinyl testoster- 1st pilot study on (DNG got carried out in 17 premenopausal women
one(T) possesses strong antigonadotropic properties, lower the mid cycle having symptomatic adenomyosis as well as drug caused efficacy in im-
Archives of Clinical Case Studies and Case Reports, 2021 Volume 2 | Issue 3 | 193proving pain symptoms, though some had >frequent menorrhagia with following 12mth of combined therapy, women had significant decrease in
anaemias getting worse [43]. A randomised, double blind, multicentre as menstrual bleeding as well as dysmenorrhea with a decrease uterine size,
well as placebo controlled trial on DNG, daily given for 16wks in women with a low incidence of LNG-IUS expulsion rate.
with adenomyosis displayed a significant decrease of pain score as well
as VAS among DNG as well as placebo [44]. A higher uterine decrease in A RCT that compared LNG-IUS system with combined oral contracep-
uterine volume in DNG group was seen, without reaching significance. It tives (COC) low dose demonstrated both decrease in pain as well as men-
was a well tolerated drug, though a great portion of women documented strual blood loss, but, the IUD had >effectiveness in these outcomes [59].
irregular uterine bleeding at the time of treatment. Till date the cutoff value of uterine volume >than 150ml was significant
correlated with failure of LNG-IUS, hence the insertion in a large volume
The same group examined safety as well as effectiveness of long term ad- uterus has a significant >failure rate as compared to small volume of uterus
ministration of DNG for 52 wks [45]. DNG had efficacy in improving pain [60].
score scale for dysmenorrhea as well as pelvic pain as well as in decrease in
need for analgesics. pain score decreased significance following 24 as well E. Combined Oral Contraceptives (COC)
as 52 wks of treatment improving patients QOL. Additionally the bodi- Basis of using Combined Oral contraceptives (COC) in adenomyosis is
ly pain subscale score in SF-36 was almost same for general population. associated with induced decidualization as well as ultimate atrophy of
The commonest side effect was metorrhagia (96, 9%, as well as hot flushes the endometrium, decrease pain as well as AUB. Patients presenting with
(7,7%), but in most patients the bleeding secondary to P action of DNG on dysmenorrhea as well as menorrhagia might benefit from the amenorrhea
endometrium, was tolerable. But in a retrospective study (on 51 patients) that results that might favour symptomatic improvements [61]. Addition-
demonstrated that young women as well as anaemia before treatment were ally, COCs repress aromatase expression in the case of eutopic endometri-
risk factors for omitting treatment with DNG [46]. um as well as in adenomyotic foci [62]. Inspite of commonly used off label
COCs for adenomyosis is associated symptoms with satisfactory longterm
Comparing DNG with GnRH analogues demonstrated no alterations as pain control, no well controlled trials are there supporting the pharmaco-
far as pelvic pain decrease was concerned. But 4 mths of treatment with logical use of COCs for treatment of adenomyosis.
GnRH analogues caused a >decrease of AUB symptoms as checked by
USG [47].
F. Nonsteroidal Anti-inflammatory Drugs (NSAIDS)
NSAIDS are non-hormonal compounds usually used in a symptomatic
D. Levonorgestrel –Releasing IU System (LNG-IUS) treatment of dysmenorrhea as well as heavy bleeding related with ade-
LNG-IUS has been utilized for therapy of adenomyosis with the basic idea nomyosis. A systematic review showed that NSAIDS might be utilized in
of decrease bleeding during menstruation as well as pain by decrease in treatment of pain with menstruation, without pointing which drug is most
thickness of the myometrial junctional zone as well as total uterine vol- proper as well as safest for this [63]. Another systematic review showed
ume [48]. LNG-IUS manages to decrease menstrual bleeding even women that NSAIDS might be utilized in decrease heavy bleeding even though
not having adenomyosis and gets inserted for contraceptive requirements their efficiency is < than hormonal therapy as well as tranexamic acid [64].
[49]. Decrease of menstrual blood is thought to be secondary to direct
effects of. Levonorgestrel on adenomyosis foci with decidualization as well
as escalation in apoptosis in endometrial glands as well as stroma [50]. G. Novel Drugs (Investigational)
Actually Levonorgestrel liberation =>atrophy as well as shrinkage of ad- i) Aromatase Inhibitor
enomyosis lesions via a downregulation of estrogen receptors, avoiding Aromatase cytochrome P450 (CYP19A1), i.e a crucial enzyme in the
future stimulation by estrogens [51]. This LNG-IUS system sees to it that synthesis of estrogens via androgens is found typically in endometrium
side effects secondary to oral treatment provided further stimulation in of women with endometriosis, adenomyosis, leiomyoma, but not that in
contrast to relatively low serum amounts, locally high amounts in the en- healthy women [65]. This enzyme has a role in the androstenedione→T
dometrium as well as other tissues present adjacently. →Estrone to estradiolrespectively. 1ST documented use of Aromatase In-
hibitor (AIs) in adenomyosis was documented in a woman with severe
Thus LNG-IUS system becomes an efficacious, simple alternative approach adenomyosis refractory to GnRH analogues as well as danazol, who
of medical treatment of chronic pelvic pain. It represents a cost efficacious wanted preservation of fertility. Anastrazole was given orally for 16wks in
,reversible as well as long term therapy for women presenting with pelvic combination with GnRH analogues for suppressing the synthesis of estro-
pain correlated with adenomyosis especially in mild as well as moderately gens.Dec rease in uterine volume was 60%,8wks following treatment and
severe, decrease the requirement for surgery [52]. the patient had no AUB for 6mths following cessating Ais [66]. From a
RCT outcome that compared a treatment for 3mths with an AIs(letrozole
Those treated with LNG-IUS system for 3 yrs there was a total satisfaction 2.5mg/d as well as goserelin 3.6mg mthly demonstrated that AIs had same
rate of 72% with continuous significant reduction in dysmenorrhea as well efficacy as GnRH analogues in decrease of Adenomyoma volume as well
as uterine volume as compared to baseline [53]. Despite partial decrease as improvement of symptoms .Actually both treatments a significant de-
improved very fast, uterine volume decrease might not occur till 2 yrs post crease in uterine volume following 3mths was seen, without any relevant
insertion [54]. LNG-IUS action on bleeding gets modulated via VEGF, alteration in Adenomyotic areas (41% vs 49%) at study completion [67].
endometrial levels [55]. A randomized controlled trial(RCT)) on 75wom- AIs appear to be promising for Adenomyosis when resistant to other treat-
en who had either LNG-IUS system or hysterectomy demonstrated that 6 ments although other studies are required [6].
mths following treatment haemoglobin amounts were comparable as well
as QOL with LNG-IUS vs hysterectomy [56]. ii) Selective Progesterone Receptor Modulators (SPRMs)
Progesterone receptor has a necessary part in uterine physiology in repro-
Further LNG-IUS system had efficacy in decreasing urinary symptoms duction. Selective Progesterone receptor modulators (SPRMs)have come
at 6mths post treatment as well as incontinence in 65 women who had out to be valuable option [68 case report by us [for hormone dependent
USG adenomyosis prospectively enrolled [57]. A prospective study was situations like uterine fibroids [69]. Both Progesterone agonist as well as
conducted via Zhang et al. on 21 women having a uterine size of < 12 antagonist actions in the endometriosis are exerted by (SPRMs decreas-
wks gestation treatment with GnRH analogues till uterine size wasmyosis [70-72]. Earlier proof with mifepristone demonstrated the effect of that adenomyosis lesions are wounds that are undergoing repetitive tis-
caspase 3 expression in adenomyosis tissue, that included cell apoptosis, sue injury as well as repair [82]. Platelets induce epithelial-mesenchymal
inhibiting the initiation as well as formation of adenomyosis [73]. But only transition, fibroblast–to myo fibroblast trans differentiation that ultimately
a few small clinical studies on endometriosis demonstrated the potential cause fibrosis [83] (Figure 1). A recent study in a mouse model of ade-
use of SPRMs in adenomyosis although we have found good results al- nomyosis showed that Anti Platelet Therapy(thromboxane A2 synthase
though no RCT done. Giving mifepristone 50mg daily improved pain as inhibitor) is effective in suppression of myometrial infiltration, improv-
well as =>regression of endometriosis lesions (we get success with 50 mg ing generalized hyperalgesia decrease both uterine hyperactivity as well
alternate day although recurrence of endometriosis occurs on discontin- as systemic corticosterone levels .Further a decreased expression of some
uation of SPRMs [74]. Similarly although asoprisnil and teapristone ace- proteins implicated in adenomyosis fibrogenesis was shown, corroborat-
tate were reported to give relief in endometriosis related pain, asoprisnil ing the promising roles of Anti platelet Therapy in adenomyosis [84]. But
development was given up [75]. But SPRMs require evaluation as well as till now, no studies have been published or registered on the use of agents
well-designed randomized controlled trials (RCT’s) for evaluation of long targeting platelets.
term actions as well as their clinical use in adenomyosis. a Phase II ran-
domized double blind, controlled trial with ulipristal acetate 10mg/day
for 3 mths in patients with adenomyosis who want to preserve fertility Medical Treatment of Adenomyosis -In Infertile
has been just reviewed. Although drawback might be the liver function Women
abnormalities recently reported with ulipristal acetate might prove to be In cases with infertility adenomyosis diagnosis is done with >frequen-
a hurdle. The primary outcome is to examine the efficiency of ulipristal cy with prevalence rate between 20-25% of women undergo ART [10].
acetate on bleeding control as well as pain in adenomyosis. Dysregulation of myometrial structure as well as changed endometrial
function causing negative influence on fertility [85]. But no agreement is
iii) Oral GnRH Antagonist (elagolix) there on the best approach for management of adenomyosis in women
GnRH antagonists (GnRH-ant) represent compounds having same struc- attempting to conceive. A lot of studies have demonstrated that GnRH
ture like natural GnRH which inhibit the reproductive system via an treatment might prove reproductive outcomes probably helping in uterine
immediate antagonist action on GnRH receptors in the pituitary, hence as well as endometrial receptivity [86]. Initial case reports on utilization
blocking the secretion of gonadotropins. They are mostly used for antag- of GnRH analogues following 6mth therapy with nafarelin acetate or a
onists protocols for ovarian hyperstimulation (OHS) in assisted repro- 5mth therapy with leuprolide acetate respectively 2 women with severe
ductive technology (ART). Currently 2 double blind, randomized phase adenomyosis conceived spontaneously [87]. Use of GnRH analogues was
III controlled trials on women having endometriosis treated with various examined both prior to and following surgical treatment of adenomyo-
doses of elagolix were efficacious, which is an oral non peptide GnRH-ant sis, with relatively good results for fertility, even though only small series
got documented [76]. Both schedules of elagolix had efficacy for improve- or case reports corroborated this management [86,88,89].Certain studies
ment of dysmenorrhea as well as nonmenstrual pelvic pain during a 6mth have demonstrated that administration of GnRH analogues prior to in vi-
period in women with mod to severe endometriosis-related pain [76]. tro fertilization (IVF) cycles treatment significantly escalated chances of
Mechanistically GnRH-ant are separate from that of GnRH analogues that pregnancy in infertile women with adenomyosis [90]. Niu et al. showed
following an initial stimulatory phase desensitize GnRH receptors in the that longterm GnRH agonist pre-treatment escalated pregnancy rates in
pituitary and then =>depletion of pituitary gonadotropins as well as to- adenomyosis patients undergoing frozen embryo transfer (FET ) follow-
tal suppression of estradiol. GnRH-ant do not induce either downregula- ing preparation of endometrium with hormone response therapy (HRT)
tion or desensitization of the receptors, since they work competitively by [91,92]. Another retrospective study was carried out on 241 infertile wom-
avoiding endogenous GnRH from binding as well as activating its pituitary en with adenomyosis diagnosed by USG in those undergoing IVF as well
receptors. Hence based on the dose of antagonists given, the estradiol sup- as fresh embryo transfer (ET) cycles or FET cycles. No difference among
pression can be manipulated. The treatment might partially suppress es- cases with or without GnRH analogues pretreatment with goserelin for
tradiol without needing add back therapy, or fully suppress estradiol when 2-3mths in a large number of fresh embryo transfer (ET) cycles pointing
combined with add back therapy [78]. In view of promising outcomes of that GnRH analogues pre-treatment has no advantage in enhancing IVF
GnRH-ant in endometriosis, a future utilization for treatment of Adeno- results in such cases. Conversely, a >clinical pregnancy rates was seen in
myosis-associated symptoms might be posited. women undergoing FET cycles following GnRH analogues pre-treatment
(39.5%) or without(25.2%) GnRH analogues pre-treatment [92].
iv) Valproic Acid (VPA) A Very current systematic review as well as meta-analysis gave a summary
Escalating proof shows that adenomyosis is an epigenetic disease. Class 1 of the existing proof in relation to the influence of adenomyosis on fertility
histone deacetylases appear to be implicated in the etiopathogenesis, since as well as a IVF results demonstrating that GnRH analogues pre-treatment
their expression has been observed to be escalated in eutopic as well as or long protocol might be advantageous in escalating pregnancy rates
ectopic endometrium in Adenomyosis, that has an association with se- .both in symptomatic as well as asymptomatic patients [93]. Adenomyosis
vere dysmenorrhea [79]. Valproic Acid (VPA)Is a specific treatment potent has negative influence on IVF clinical results, decease pregnancy as well
histone deacetylases inhibitor, that has been utilized for epilepsy therapy as live birth rates (LBR) as well as enhances miscarriage rates. Although
for decades ,has shown efficacy in treating a small series of women with GnRH analogues pre-treatment might help more studies are needed [93].
adenomyosis, reducing dysmenorrhea treatment uterine bleeding as well
as decrease uterine size [80]. Murine model of Adenomyosis studies im-
plicated that the mode of action of VPA, which suppressed myometrial Conclusions
infiltration, enhanced generalized hyperalgesia as well as decrease the am- Medical Treatment of Adenomyosis has a significant role particularly in
plitude as well as irregularity of uterine contractions [81]. Inspite of these the management of diffuse forms as well as those women needing preser-
promising outcomes favouring histone deacetylases inhibitor, till now no vation or restoration of fertility. Medical Treatment is a good method for
clinical trials have been carried on for analyzing the efficiency of VPA in the therapy of symptoms of pain as well as bleeding occurring very fre-
adenomyosis. quently that is more acceptable rather than than the surgical one. Till date
no labelled drugs are available, but those used frequently are efficacious in
the management of symptoms as well as improvement of pregnancy rates
v) Anti Platelet Therapy in ART. Randomized clinical studies are required for systemically check-
Escalating role of Platelets in adenomyosis pathogenesis as per the posit
Archives of Clinical Case Studies and Case Reports, 2021 Volume 2 | Issue 3 | 195ing the usefulness of drugs usually used and find the more efficacious ones. osis, Adenomyosis and uterine myoma after GnRH agonists therapy.
Additionally on the basis of the newer discoveries of pathogenic insights of Hum Reprod 25: 642-653.
adenomyosis, introducing newer molecules will be required. 20. Kamada Y, Nakatsuka M, Asagiri K, Naguchi S, Habara T, et al.
(2000) GnRH agonist suppressed expression of nitric oxide synthase
References and generation of peroxy nitrite in Adenomyosis. Hum Reprod 15:
1. Abbott AG (2017) Adenomyosis and, abnormal uterine bleeding 2512-2519.
(AUB-A)-Pathogenesis, diagnosis and management. Best Pract Res 21. Takakuchi A, Koga K, Miyashita M, Makabe T, Sue F, et al. ( 2016)
Clin Obstet Gynaecol 40: 68-81. Dienogest reduces proliferation,NGF expression and nerve fibre den-
2. Exacoutos C, Luciano D, Corbert B, De Felice G, Di Felicianto M, sity in human Adenomyosis. Eur J Obstet Gynaecol Reprod Biol 207:
et al. (2013) The junctional zone .A 3 dimensional ultrasound study 157-161.
of patients with endometriosis. Am J Obstet Gynaecol 200: 248e1-7. 22. Nelson JR, Corson SL (1993) Long term management of Adenomy-
3. Exacoutos C, Menganaro L, Zupi E (2014) Imaging for the evaluation osis with a gonadotropin releasing hormone agonist:a case report.
of endometriosis and Adenomyosis. Best Pract Res Clin Obstet Gy- Fertil Steril 59: 441-443.
naecol 28: 655-681. 23. Streuli I, Dulbulsson J, Santulli F, DeZiegler D, Batteux F, et al. (2014)
4. Van den Bogh T, Dueholm M, Leone EPG, Valentin L, Rasmussen An update on the pharmacological management of Adenomyosis.
CK, et al. (2015) Terms ,definitions and measurements to describe so- Expert Opin Pharmacother 15: 2437-2460.
nographic features of myometrium and uterine masses :A consensus 24. Akira S, Mine K, Kuwahara Y, Takeshita T (2009) Efficacy of low dose
opinion from the Morphological Uterine Sonographic Assessment gonadotropin releasing hormone agonist (drawback therapy) for Ad-
(MUSA)group. Ultrasound Obstet Gynaecol 46: 284-298. enomyosis. Mol Sci Monit 15: CR1-4.
5. Kulvinder Kochar Kaur, Allahbadia GN, Singh M (2018) Advances in 25. Okada H, Okamoto R, Tsuzuki T, Tsuji S, Yasuda Y, et al. (2011) Pro-
Adenomyosis Diagnosis Utilizing Transvaginal Ultrasonography-A gestins inhibit estradiol induced vascular endothelial growth factor
Short Summary. Open Acc J Repro & Sexaual Dusord 2: 154-155. and stromal cell differentiation factor1 in human endometrial stro-
6. Peric H, Fraser JS (2006) The symptomatology of Adenomyosis. Best mal cells. Fertil Steril 96: 786-791.
Pract Res Clin Obstet Gynaecol 20: 547-555. 26. Muneyyirci –Delate O, Chandrareddy A, Mankame S, Osei-Tutu N,
7. Tosti C, Troia I, Vannuccini S, Lazzen L, Tosti S, et al. (2016) Current Von Gizycri H (2012) Norethindrone acetate in the management of
and future medical treatment of adenomyosis. J Endometr 8: 127- Adenomyosis. Pharmaceuticals 5: 1120-1127.
135. 27. Laursen NH, Wilson KH, Birmbaum S (1975) Danazol an antigonad-
8. Chapron C, Tosti C, Marcellini L, Bourdon M, Lafay-Pillet MC, et otropic agent in the treatment of pelvic endometriosis. Am J Obstet
al. (2017) Relationship between the magnetic resonance imaging ap- Gynaecol 123: 742-747.
pearance of Adenomyosis and endometriosis phenotypes. Hum Re- 28. Berberi RL (1990) Danazol:molecular,endocrine and clinical Phar-
prod 32: 1393-1401. macology. Prog Clin Biol Res 323: 241-252.
9. Puente JM, Fabris A, Patel J, Patel A, Cerrillo M, et al. (2016) Ade- 29. Beaumont H, Augood C, Duckitt K, Lethaby A (2002) Danazol for
nomyosis in infertile women :prevalence of the 3D Ultrasound as a heavy menstrual bleeding. Cochrane Database Syst Rev CD001017.
marker of severity of the disease. Reprod Biol Endocrinol 14: 60. 30. Ueki K, Kumagai K, Yamashita H, Li ZL, Ueki M, et al. (2004) Ex-
10. Lazzeri L, Govvani A, Exacoutos C, Tosti C, Prizauti S, et al. (2014) pression of apoptosis-related proteins in adenomyotic uteri treated
Preoperative and post operative clinical and transvaginal Ultrasound with Danazol and GnRH agonists .Int J Gynecol Pathol 23: 248-258.
findings of Adenomyosis in patients with deep infiltrating endome- 31. Brauri DP, Gebel H, Dmowski WP (1994) Effect of Danazol in vitro
triosis. Reprod Sci 21: 1027-1033. and in vivo on monocyte mediated enhancement of endometrial Cell
11. Garcia-Solares J, DonnezJ, Donnez O (2018) Pathogenesis of uterine proliferation in women with endometriosis. Fertil Steril 62: 89-95.
Adenomyosis:invagination or metaplasia. Fertil Steril 109: 371-379. 32. Ota H, Mal TM, Shidara Y, Kodama H, Takahashi H, et al. (1992)
12. Vannuccini S, Tosti C, Carmona F, Huang SJ, Chapron C, et al. (2017) Effect of Danazol at immunologic patients in patients with Adeno-
Pathogenesis of adenomyosis:an update on molecular mechanisms. myosis with special reference to autoantibodies :a multicentric study.
Reprod Bimed Endocrinol 35: 592-604. Am J Obstet Gynaecol 167: 418-426.
13. Feciele L, Bianchi S, Frontino G (2008) Hormonal treatment for ade- 33. Igarashi M (1990) A new therapy for pelvic pelvic endometriosis and
nomyosis. Best Pract Res Clin Obstet Gynaecol 22: 333-339. uterine denomyosis:Local effect of vaginal and intra uterine Danazol
14. Pontis A, D’Alieno MN, Pirarba S, De Angelis C, Tineli R, et al. (2016) application.Asia Oceana J Obstet Gynecol 116: 1-12.
Adenomyosis:A systematic review of medical treatment Gynaecol 34. Takebayashi T, Fujino Y, Umesaki N, Ogita S (1995) Danazol suspen-
Endocrinol 3590: 1-5. sion injected into the uterine cervix of patients with Adenomyosis
15. Kulvinder Kochar Kaur, Allahbadia GN, Singh M (2020) Dilemna and myoma. Preliminary Study. Gynecol Obstet Invest 39: 207-211.
regarding preference of surgery or medical treatment in case of tubal 35. Igarashi M, Abe Y, Fukuda M, Ando A, Miyasal AM, et al. (2000)
blockade, endometriosis or adenomyosis and pelvic adhesion pre- Novel conservative medial therapy for uterine Adenomyosis with a
vention once surgery is contemplated –a systematic review. in press. Danazol loaded intra uterine device. Fertil Steril 74: 412-413.
16. Bazot M, Darai E (2018) Role of trans vaginal sonography and mag- 36. Zhang X, Yuan H, Deng I, Hu F, Ma J, et al. (2008) Efficacy of a Da-
netic resonance imaging in the diagnosis of adenomyosis. Fertil Steril nazol loaded intra uterine contraceptive device on Adenomyosis in
109: 389-397. an ICR mouse model . Hum Reprod 23: 2024-2030.
17. Gordts S, Grimbizis G, Campo R (2018) Symptoms and classification 37. Luisi S, Razza S, Lazzeri L, Bocchi C, Severi FM, et al. (2009) Efficacy
of uterine Adenomyosis including the place of hysteroscopy in the of vagina Danazol treatment in women with menorrhagia during fer-
diagnosis. Fertil Steril 109: 380-388. tile age. Fertil Steril 92: 1351-1354.
18. Khan FN, Kitajima M, Hiraki K, Fujishita A, Nakashima H, etal 38. Tosti C, Vannuccini S, Trola L, Luisi S, Centrini G, etal. (2017) Long
(2010) Cell proliferation effects of GnRH agonists on pathological term vaginal Danazol treatment in fertile age women with endome-
lesions of women with endometriosis, Adenomyosis and uterine my- triosis.J Endometr Pelvic Pain Disord 9: 39-43.
oma. Hum Reprod 25: 2878-2890. 39. Sasagawa S, Shimizu Y, Kami H, Takeuchi t, Mita S, et al. (2008) Di-
19. Khan FN, Kitajima M, Hiraki K, Fujishita A, Sekine I, (2010) Chang- enogest is a selective Progesterone receptor agonist in transactivation
es in tissue inflammation, angiogenesis and apoptosis in endometri- analysis with potent Endometrial activity due to its efficient pharma-
Archives of Clinical Case Studies and Case Reports, 2021 Volume 2 | Issue 3 | 196cokinetic profile. Steroids 73: 222-231. Biol 170: 517-520.
40. Moore C, Carol W, Graser T, Mellinger U, Walter T (1999) Influence 58. Zhang P, Song K, Li L, Yukuwa K, Kong R (2013) Efficacy of com-
of Dienogest in young fertile women.Clin Drug Investig 18: 271-278. bined levonorgestrel releasing intra uterine system with gonadotro-
41. Yamanaka A, Kimura F, Kishi Y, Takahashi K, Suginami H, et al. pin releasing hormone analogue for the treatment of adenomyosis
(2014) Progesterone and synthetic Progestins, Dienogest induce .Med Princ Pract 22: 480-483.
apoptosis of human primary cultures of adenomyotic stromal cells . 59. Shaabian OM, Ali MK, Sabra AM, Abd ElAll DE (2015) Levonorge-
Eur J Obstet Gynaecol Reprod Biol 179: 170-174. strel releasing intra uterine system versus a low dose combined oral
42. Prathoomthong S, Tingtha natikul Y, Lertvikool S, Rodratri N, Waiya contraceptives for treatment of adenomyotic uteri: a randomised
put W, et al. (2018) The effects of Dienogest on macrophage and nat- clinical trial . Contraception 92: 301-307.
ural killer cells in adenomyosis:a randomized controlled study. Int J 60. Lee KH, Kim JK, LeeMA, Ko YB, Yang IB, et al (2016) Relationship
Fertil Steril 11: 279-286. between uterine volume and discontinuation of treatment with Levo-
43. Hirata T, Izum G, Takamura M, Harada M, et al. (2014) Efficacy norgestrel releasing intra uterinedevice in patients with adenomyosis.
of Dienogest in the treatment of symptomatic adenomyosis :a pilot Arch Gynaecol Obstet 204: 564-566.
study. Gynaecol Endocrinol 30: 725-729. 61. Schindler AE (2008) Non contraceptives use of hormonal contracep-
44. Osuga Y, Fujimoto –Okabe H, Hagino A (2017) Evaluation of the Ef- tives. Gynaecol Endocrinol 24: 235-236.
ficacy and safety of Dienogest in the treatment of painful symptoms 62. Mala H, Casay J, Correla T, Freitas L, Pimentel K, et al. (2006) Effect
in patients with adenomyosis :a randomized double blind ,multi- of the menstrual cycle and oral contraceptives on aromatase and cy-
centre, placebo controlled trial. Fertil Steril 108: 673-678. clooxygenase-2 expression in adenomyosis. Gynaecol Endocrinol 22:
45. Osuga Y, WatanabeM, Hagino M (2017) Longterm use of Dienogest 547-551.
in the treatment of painful symptoms in adenomyosis.J Obstet Gy- 63. Manjoribanks I, Ayelele R, Farquhar C, Proctor M (2015) Nonsteroi-
naecol Res 43: 1441-1448. dal anti-inflammatory drugs for dysmenorrhoea. Cochrane Database
46. Nagata C, Yanagida S, Okamata A, Morikawa A, Sujimoto K, et al. Syst Rev : CD001751.
(2012) Risk factors for treatment discontinuation due to uterine 64. Lethaby A, Duckitt K, Farquhar C (2013) Nonsteroidal anti-inflam-
bleeding in adenomyosis patients treated with Dienogest. J Obstet matory drugs for heavy menstrual bleeding. Cochrane Database Syst
Gynaecol Res 38: 639-644. Rev :CD000400.
47. Fawzy M, Meshaw Y (2015) Comparison of Dienogest versus trip- 65. Yamamoti T, Noguchi T, Tamura T, Kitawaki J, Okada H (1993) Ev-
torelin acetate in premenopausal women with adenomyosis :a pro- idence for estrogen synthesis in adenomyotic tissues. Am J Obstet
spective clinical trial. Arch Gynaecol Obstet 292: 1267-1271. Gynaecol 169: 734-738.
48. Sabboloni I, Petraglia F (2017) Non contraceptive benefits of intra- 66. Kimura T, Takahushi K, Takabayashi Y, Fujiwara M, Kita N, et
uterine levonorgestrel administration:why not? Gynaecol Endocrinol al.(2007) Concomitant treatment of severe uterine Adenomyosis in a
33: 822-829. premenopausal women with an aromatase inhibitor and a a gonado-
49. Kelekri S, Kelekri KH, Yalmaz B (2012) Effects of levonorgestrel re- tropin releasing hormone agonist. Fertil Steril 87: 1468e9-12.
leasing intra uterine system and T380 intra uterine copper device on 67. Badawy AM, ElNashar AM, Mosbah AA (2012).Aromatase inhibi-
dysmenorrhea and days of bleeding in women with and without ade- tion or gonadotropin releasing hormone agonist for the management
nomyosis.Contraception 86: 458-463. of uterine Adenomyosis: a randomized controlled trial.Acta Obstet
50. Maruo T, Laong-Fernandez IB, Pakarinen P, Murakoshi H ,Spitz IM, Gynaecol(Scand) 91: 489-495.
et al. (2001) Effects of levonorgestrel releasing intra uterine system 68. Kulvinder Kochar Kaur, Allahbadia GN, Singh M (2018) Sponta-
on proliferation and apoptosis of the endometrium. Hum Reprod 16: neous Conception in a Case of Adenomyosis with Submucus Fibroid
2103-2108. Following Treatment with Mifepristone in a 38 year Old Lady with
51. Critchley HOD, Wang H, Kelly RW, Gebbe AE, Glasier AF (1998) 10year Secondary Infertility J. Hum Bio & Health Edu 2: 014.
Progestin receptor isoforms and prostaglandin dehydrogenase in the 69. Whitaker LHR, Willaims ARW, Critchley HOD (2014) Selective Pro-
Endometrium of women using a levonorgestrel releasing intra uter- gesterone receptor modulators.Curr Obstet Gynaecol 26: 237-242.
ine system . Hum Reprod 13: 1210-1217. 70. Kulvinder Kochar Kaur, Allahbadia GN, Singh M (2015) Medical
52. Radzinsky VE, Khamoshina MB, Nosenrika EN, Dukhin AO, Soju- Management of Leiomyomas-Emphasis for Different Geographical-
nov MA, et al. (2016) Treatment strategies for pelvic pain associated Regions J Gynecol Neonatal Biol 1: 1-8.
with adenomyosis. Gynaecol Endocrinol 32(suppl 2): 19-22. 71. Kulvinder Kochar Kaur, Allahbadia GN, Singh M (2017) Meeting the
53. Sheng Z, Zhang WY, ZhangI P, Lu D (2009) The LNG-IUS study on Challenges of Endometriosis Associated Pain-Newer Options for Fu-
adenomyosis: a 3 year follow up study on the efficacy and side effects ture and Research Directions. BAOJ Bioinfo 1: 09.
of the use of levonorgestrel releasing intra uterine device in patients 72. Kulvinder Kochar Kaur, Allahbadia GN, Singh M (2019) “An Update
with adenomyosis . Contraception 79: 189-193. on Diagnosis and Management of Adolescent Endometriosis - A
54. Cho S, Nam A, Kim H, Chay D, Park I, et al. (2008) Clinical effects Short Communication”. Acta Scientific Paediatrics 22: 48-50.
of the levonorgestrel releasing intra uterine device in patients with 73. Wigenfeld A, Satinder PTI, Whitaker LHR, Critchley HOD (2016)
adenomyosis. Am J Obstet Gynaecol 198: 373.e1-7. Selective Progesterone receptor modulators(SPRM). Progesterone
55. Laong-Fernandez IB, Maruo T, Pakarinen P, Spitz IM, Johansson E receptor action:mode of action on the Endometrium and treatment
(2003) Effects of levonorgestrel releasing intra uterine system on the outcome options in gynaecological therapies. Expert Opin Ther Tar-
expression of vascular endothelial growth factor and adrenomedullin gets 20: 1045-1054.
in the Endometrium in adenomyosis. Hum Reprod 18: 694-699. 74. Wang Y, Kang X, Wang S (2014) The influence of mifepristone to
56. Ozdegarmeno O, Kayiikcioglu F, Akgul MA, Kaplan M, Karcattin- caspase 3 expression in Adenomyosis.Clin Exp Obstet Gynaecol 41:
caba M, et al. (2011) Comparison of levonorgestrel releasing intra 145-147.
uterine system versus hysterectomy on efficacy of and quality of life 75. Kettel LM, Murphy AA, Morales MI, Ulmann A, Baulieu EE, et al.
in patients with adenomyosis. Fertil Steril 95: 497-502. (1996) Treatment of endometriosis with the anti Progesterone mife-
57. Ekin M, Cengiz H, Ayag MI, Kaya C, Yasar I, et al. (2013) Effects of pristone(RU486). Fertil Steril 65: 23-28.
the levonorgestrel releasing intra uterine system on urinary symp- 76. Chwaliz K, Perez MC, De Marino D, Winkel C, Schubert G, et al.
toms in patients with adenomyosis. Eur J Obstet Gynaecol Reprod (2005) Selective Progesterone receptor modulators Development and
Archives of Clinical Case Studies and Case Reports, 2021 Volume 2 | Issue 3 | 197use in Treatment of leiomyomas and endometriosis.Endocr Rev 26: 86. Wang PH, Yang TS, LeeWL, Chao HT, Chang SP, et al. (2000) Treat-
423-438. ment of infertile women with adenomyosis with a conservative mi-
77. Taylor HS, Guidice C, Lessey BA, Abrao MS, Kotanki Z, et al. (2012) crosurgical technique and a a gonadotropin releasing hormone ago-
Treatment of endometriosis associated pain with elagolix or oral nist. Fertil Steril 73: 1061-1062.
GnRH antagonist. N Engl J Med 322: 28-40. 87. Silva PD, Perkins HE, Schauberger CW (1994) Live birth after treat-
78. Donnez J, Taylor RN, Taylor HS (2012) Partial suppression of estra- ment of severe adenomyosis with a gonadotropin releasing hormone
diol: a new strategy in treatment of endometriosis. Fertil Steril 74: agonist. Fertil Steril 61: 171-172.
50-55. 88. Huang BS, Seow KM, Tsui KH, Huang CY, Lu YF, et al. (2012) Fertil-
79. Liu X, Nit J, Glue MN (2012) Elevated immunoreactivity against class ity outcome of infertile women with adenomyosis withthe combina-
1 histone deacetylation in Adenomyosis. Gynaecol Obstet Invest 34: tion of a conservative microsurgical technique and a GnRH agonist
50-55. :longterm follow up in a series of nine patients. Taiwan J Obstet Gy-
80. Liu X, Yuan L, Kim SW (2010) Valproic acid as a therapy for adeno- naecol 51: 212-216.
myosis:a comparative case series.Repr Sci 17: 904-912. 89. Ozaki T, Takahashi K, Okarta M, Kurioka H, Miyazaki K (1994) Live
81. Mao X, Wang Y, Carter AV, Zhen X, Guo SW (2011) The retardation birth after conservative surgery of severe adenomyosis following
of myometrial inflammation :.Reduction of uterine contractility and magnetic resonance imaging and gonadotropin releasing hormone
alleviation of general and hyperalgeasia in mice with induced Ade- agonist.Int J Fertile Women Med 44: 260-264.
nomyosis by levo tetrahydropalmitate g-THP and Androgre pbolide 90. Mijatovic V, Flonin E, Halim N, Schats R, Hompes P (2010) Adeno-
. Repr Sci 18: 1025-1037. myosis has no adverse effects on IVF/ICSI outcomes in women with
82. Ding D, Liu X,D uan J, Guo SW (2015) Platelets are an unindicated endometriosis and treated with long term pituitary downregulation
culprit in the development of endometriosis: Clinical and experi- before IVF/ICSI. Eur J Obstet Gynaecol Reprod Biol 151: 62-65.
mental evidence. Hum Reprod 30: 812-832. 91. Nu Z, Chen O, Sun Y, Feng Y (2013) Long term pituitary downregu-
83. Shen M, Liu X, Zhang H, Guo SW (2016) Transforming growth fac- lation before frozen embryo transfer could improve pregnancy out-
tor β1 signaling coincides with epithelial-mesenchymal transition come in with women with Adenomyosis. Gynaecol Endocrinol 29:
and fibroblast –to myo fibroblast transdifferentiation in the develop- 1026-1030.
ment of Adenomyosis in mice. Hum Reprod 31: 355-369. 92. Park CW, Choi MH, Yang KM, Song IO (2016) Pregnancy rates in
84. Zhu B, Chen Y, Shen X, Liu X, Guo SW (2016) AntiPlatelet therapy women with adenomyosis undergoing fresh or frozen embryo trans-
holds promise in treating Adenomyosis: experimental evidence[in- fer cycles following gonadotropin releasing hormone agonist treat-
ternet]. Reprod Biol Endocrinol 14: 66. ment. Clin Exp Reprod Med 43: 163-173.
85. Benagiani G, Brosens I, Habiba M (2014) Structural and molecular 93. Younes G, Tulandi T (2017) Effects of adenomyosis on in vitro fer-
features of the endomyometrium in endometriosis and Adenomyo- tilization treatment outcomes:a meta-analysis. Fertil Steril 108: 483-
sis. Hum Reprod Update 20: 386-402. 490e3.
Cite
* this article: Kulvinder Kochar Kaur, Gautam Allahbadia and Mandeep Singh (2021) Medical Treatment in Uterine Adenomyosis Management
– A Systematic Review. Archives of Clinical Case Studies and Case Reports 2: 189-198.
*Copyright: ©2021 Kulvinder Kochar Kaur. This is an open-access article
distributed under the terms of the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any
medium, provided the original author and source are credited.
Archives of Clinical Case Studies and Case Reports, 2021 Volume 2 | Issue 3 | 198You can also read