Bible Class: HBV Infection - Nasser Semmo
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Bible Class:
HBV Infection
Nasser Semmo UVCM, Hepatology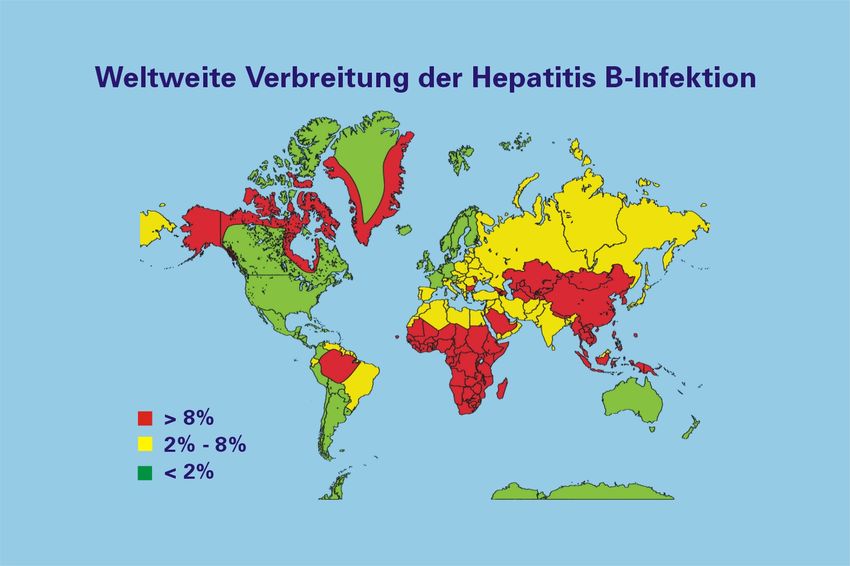
What is the HBV prevalence?
2Hepatitis B
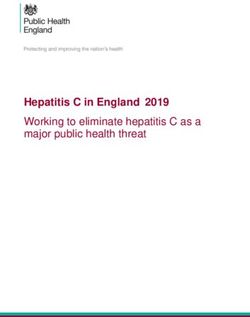
• Worldwide approx. 350 Mio. chronically infected with HBV
• Approx. 40% of the world population: anti-HBc-Antibodies
positive
• Approx. 15 Mio. chronically HBV infected in Europe
• Switzerland 0,3% (24000)
• Worldwide annually, 0,6 -1 Mio. people die from
complications of chronic HBV-Infection (WHO, 2002)
• HBV responsible for 60% of all HCC cases worldwide
3Worldwide distribution of HBV infection
4What are Hepatitis B Risk Factors?
5Hepatitis B Risk Factors
• Blood contamination
– IV-Drug Abuse
– Injured mucus membranes
• Sexual Transmission
• Perinatal Transmission
6Natural course of HBV Infection?
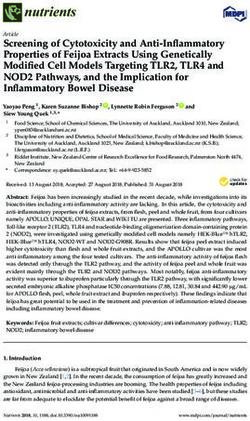
7Natural Course of Hepatitis B Infection
Acute Hepatitis B
90%
Resolution 10% Fulminant Hepatitis (0.5-1%)
Chronic Hepatitis B
70%
Asymptomatic 30% ?
carriers
Liver cirrhosis
3-5%/year
Liver failure HCC
8Who to screen for HBV ?
9Hepatitis B
Whom to screen?
• Elevated Liver enzymes and/or signs of hepatitis or chronic
liver disease of unknown origin
• Liver cirrhosis/-fibrosis
• New diagnosis of HCC
• Pat. with migration background and from regions with high
HBsAg prevalence (East Europe, Mediterranean)
• Family member or sexual partner from HBV infected
patients
DGVS-Leitlinie Hepatitis B 2007/ EASL 2012
10Hepatitis B
Whom to screen?
• Medical staff
• Homosexuals a/o persons with frequent changing sexual
partners
• Active o. previous i.v.-drug abuse
• Dialysis patients
DGVS-Leitlinie Hepatitis B 2007/ EASL 2012
11Hepatitis B
Whom to screen?
• HIV- a/o HCV-infected Pat.
• Recipients of organs before transplantation
• Blood- and Organ donors
• Patients before or during immunsuppressive therapy or
Chemotherapy
• Pregnant women (HBsAg)
DGVS-Leitlinie Hepatitis B 2007/ EASL 2012
12Prevention of HBV Reactivation
Algorithm??
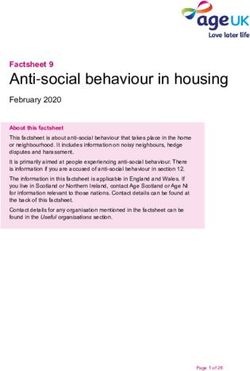
13Prevention of HBV Reactivation
HBsAg + HBsAg - HBsAg -
Anti-HBc + Anti-HBc -
Anti-HBs +/- Anti-HBs -
HBV-DNA +/- HBV-DNA & Impfung
ALT alle 1-3 m Vor Start immun-
suppressiver Tx
HBV DNA – HBV DNA –
HBV DNA +
ALT < ULN ALT > ULN
Preemptive antivirale Tx Suche nach anderen
(NAs) bis zu 12 M nach Ursachen einer Erhöhung
Ende immunsuppr. Tx der Leberenzyme
14When to treat pregnant HBV pos. women?
15Vertical transmission despite active and
passive vaccination
• N=1068 Kinder von HBeAg positiven Müttern
• 3% vertikale Transmission bei HBV DNA >106 cop/ml
• 5,5 % vertikale Transmission bei HBV DNA >107 cop/ml
• 9,6% vertikale Transmission bei HBV DNA >108 cop/ml
à Antivirale Therapie im 2./3. Trimester ab 200.000 IU/ml
Han et al., J Hepatology 2011, Petersen Hepatology 2011
16Prävention einer HBV Reaktivierung
• Screening aller Patienten auf HBsAg und anti-HBc
vor Einleitung einer immunsuppressiven Therapie
und/oder einer Chemotherapie!
• HBV Impfung, wenn HBV Serologie komplett negativ
• HBsAg + Pat.: Preemptive Therapie mit NA bis zu 12
Monate nach Ende einer immunsuppressiven Tx/
Chemotherapie, unabhängig von HBV Viruslast
• Behandlung mit Lamivudine, wenn HBV Viruslast <
2000 IU/mL
• Behandlung mit Entecavir oder Tenofovir wenn HBV
Viruslast > 2000 IU/mL
EASL CPG, J Hepatol 2012
17Prävention einer HBV Reaktivierung
• HBsAg -/ Anti-HBc + pat.: HBV Viruslast-Bestimmung,
wenn pos. = „Okkulte“ HBV Infektion
• „Okkulte“ HBV Infektion: Preemptive Therapie mit NA
• HBsAg -/ Anti-HBc + / HBV DNA - pat.: Regelmässige
Kontrollen von ALT und HBV DNA, und Tx mit NA
sobald HBV-Reaktivierung, vor Erhöhung der ALT
• Kontrollintervalle zwischen 1-3 Monate, abhänging von
der Art der immunosuppressiven Therapie und
Komorbiditäten
EASL CPG, J Hepatol 2012
18Prävention einer HBV Reaktivierung
• Empfehlung einiger Experten: Prophylaxe mit Lamivudin
bei allen HBsAg-negativen, anti-HBc positiven
Patienten, die Rituximab und/oder kombinierte
Therapien für hämatologische Tumorerkrankungen
erhalten, wenn sie anti-HBs negative und/oder eine
engmaschiges Monitoring der HBV DNA nicht garantiert
ist
• Die optimale Prophylaxedauer für diese Indikation ist
nicht klar
• HBsAg-negative Empfänger von Lebertransplantaten
von anti-HBc positiven Spendern sollten eine
dauerhafte Prophylaxe mit Lamivudin erhalten
EASL CPG, J Hepatol 2012
19When to treat HBV ?
20HBV Treatment Indication
21How to treat HBV ?
22HBV- Treatment: HOW?
High TA (>3-5 x)
Low viral titer
Short duration of infection
GT A or B
PEG-IFN 2a 180ug 48 weeks
23Is there a stopping rule for PegIFN?
24Practical application of response-guided
therapy using HBsAg levels (pegIFN-treated)
Identify responders (PPV) Identify non-responders (NPV)
Week 12: Week 12:
- HBeAg-positive e+ - HBeAg-positive e+
HBsAg 20,000 IU/mL
- HBeAg-negative e-
- HBeAg-negative e-
No decline in HBsAg +
≥10% decline HBsAgHBV Treatment: HOW?
26Response-guided therapy (RGT) using HBsAg
levels in Peg-IFN-treated patients: to identify
good responders
HBeAg positive HBeAg negative
Week 12 - 24: Week 12 - 24 (geno D):
- HBsAgResponse-guided therapy (RGT) using HBsAg levels in
Peg-IFN-treated patients: to identify non responders
HBeAg-positive HBeAg-negative (geno D)
Week 12: Week 12:
- No decline of HBsAg (A,D) - No decline in HBsAg +
- HBsAg >20,000 IU/mL (B,C) 20,000 IU/ml (A,B,C,D)
97-100% Negative Predictive Values
Sonneveld et al. Hepatology 2010
Piratvisuth et al. APASL 2010
Liaw et al. Hepatology 2011 Rijckborst et al. Hepatology 2010
Sonneveld et al., Hepatology 2013 Rijckborst / Lampertico et al. J Hepatol 2012
28What are the NUC options?
29HBV is suppressable
…in most cases with indefinite treatment duration...
Lamivudin (Zeffix, 36-72%
Epivir)
Adefovir (Hepsera) 21-51
%
Entecavir (Baraclude) 67-90%
Telbivudin (Sebivo) 60-88%
Tenofovir (Viread) 76-94%
25.03.15
Lai CL, et al. Hepatology 2005; 42:748A (AASLD Abstract LB01); Lau G, et al. NEJM 2005; 352:2882–2695; Chang T-T, et al.
NEJM 2006; 354:1000–1010; Marcellin P, et al. NEJM 2003;348:808–816; Marcellin et al., AASLD 2007, Heathcote et al., 30Can NUCs be stopped?
31When to stop NUC therapy ?
Treatment End points
HBeAg+
HBeAg-‐
Seroconversion
No
HBeAg-‐/anA-‐HBe+
seroconversion
End
of
therapy:
At
least
a6er
12
months
Long-‐term
therapy
Long-‐term
therapy
A6er
seroconversion
And
HBV-‐DNA
negaAve
End
of
therapy:
AnA-‐HBs-‐Seroconversion
EASL HBV Guidelines 2012
32When to stop NUC therapy ?
CHB Treatment
Guidelines
EASL 2012 guidelines
A) confirmed anti-HBe seroconversion (and undectable
HBV DNA) after at least 12 months of consolidation*
HBeAg positive
B) confirmed HBsAg loss and anti-HBs seroconversion
HBeAg negative confirmed HBsAg loss and anti-HBs seroconversion
Cirrhotics confirmed HBsAg loss and anti-HBs seroconversion
*A proportion of patients who discontinue NUC therapy after anti-HBe seroconversion may
require retreatment, since they fail to sustain their serological and/or virological response
adapted from EASL HBV Guidelines, J Hepatol 2012
33Management of adverse events
When to reduce IFN, and when to stop it?
34Pegylated Interferon
- Reduce Peg IFN if
- Absolute neutrophil count falls below 750/mm3
- Platelet count falls below 50,000/mm3
- Stop Peg IFN if
- Absolute neutrophil count falls below 500/mm3
- Platelet count falls below 25,000/mm3
- or if severe unmanageable depression develops
35Leukopenia/Neutropenia • In general, infection rate during HBV treatment is elevated • However, neutropenia alone in patients with compensated HBV infection is not associated with elevated infection risk • Patients with neutropenia do not have higher infection rate in comparison to those without neutropenia • Dose reduction of IFN does not lead to reduction of susceptibility to infections • Therefore dose reduction not necessary if no signs of infection present Thus: IFN-reduction in pat. with co-morbidities, older pat, liver cirrhosis a/o Diabetes if neutrophiles < 750, Filgrastim (Neupogen) if neutrophiles
Thrombopenia • IFN Dose reduction if Tc
THANK YOU
38You can also read