Hepatitis B management during immunosuppression for haematological and solid-organ malignancies: An Australian consensus statement 2019
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Hepatitis B management during
immunosuppression for haematological
and solid-organ malignancies:
An Australian consensus statement 2019
page 1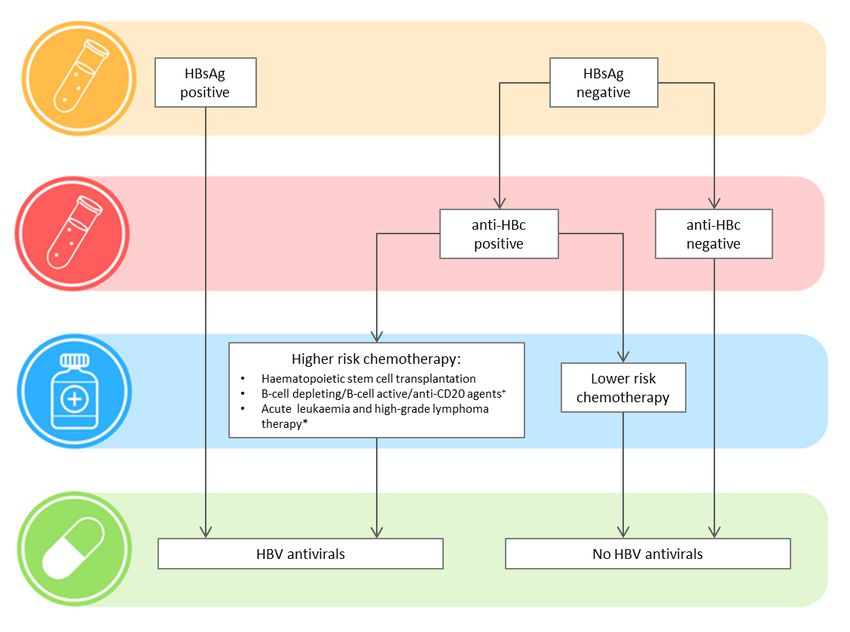
HBV management during cancer therapy 2019: Australian Consensus Statement
© Hepatitis B Management During Cancer Therapy Consensus Statement Group 2019
This work is copyright. You may download, display, print and reproduce the whole or part
of this work in unaltered form for your own personal use or, if you are part of an organisation,
for internal use within your organisation, but only if you or your organisation do not use the
reproduction for any commercial purpose and retain this copyright notice as part of that
reproduction. Apart from any use as permitted under the Copyright Act 1968 or allowed by
this copyright notice, all other rights are reserved and no part of this work may be reproduced
by any process (electronic or otherwise) without prior written permission from the Hepatitis
B Management During Cancer Therapy Consensus Statement Group. Requests and enquiries
concerning reproduction and rights for purposes other than those indicated above should be
directed to the Hepatitis B Management During Cancer Therapy Consensus Statement Group,
care of the Department of Gastroenterology, St Vincent's Hospital Melbourne, PO Box 2900,
Fitzroy VIC 3065, Australia or by email to svhm.gastro@svha.org.au
Published April 2019.
Disclaimer
The recommendations in this consensus statement represent the best available evidence at the
time of compilation and are intended to be used as a guide only. The compilers of these
recommendations shall not be liable for any loss, direct, indirect or consequential, on
whatsoever account for any omission or negligent mis-statement contained herein, or by
reason of, arising from or in relation to any such user, by any other person, company or body
relying or acting upon or purporting to rely or act upon any matter contained therein or
arising thereout.
Suggested Citation
Hepatitis B Management During Cancer Therapy Consensus Statement Group 2019. Hepatitis
B management during immunosuppression for haematological and solid-organ malignancies: an
Australian consensus statement 2019. Melbourne: Hepatitis B Management During Cancer
Therapy Consensus Statement Group.
page i
HBV management during cancer therapy 2019: Australian Consensus Statement
Contribution and Endorsement
This consensus statement was prepared by an expert panel of medical specialists in infectious
diseases, hepatology, haematology, oncology and paediatrics, and representatives from the
Australasian Society for Infectious Diseases, the Gastroenterological Society of Australia
(Australian Liver Association), the Haematology Society of Australia and New Zealand, the
Medical Oncology Group of Australia, and the Australasian Society for HIV, Viral Hepatitis
and Sexual Health Medicine. The Australasian Society for Infectious Diseases,
Gastroenterological Society of Australia, Haematology Society of Australia and New Zealand,
Medical Oncology Group of Australia, and Australasian Society for HIV, Viral Hepatitis and
Sexual Health Medicine have endorsed this consensus statement.
Steering committee members: Joseph Doyle (chair), Alex Thompson, Monica Slavin, Sue-
Anne McLachlan, Harshal Nandurkar, Simone Strasser (working group chair), Anna
Johnston, Narin Bak, Joe Sasadeusz (working group chair), Jess Howell (working group
chair), Krispin Hajkowicz (working group chair), Michelle Raggatt (project officer).
Working group members: Venessa Pattullo (deceased), Benjamin Cowie, Gabrielle Haeusler,
Winita Hardikar, Jane Beith, Peter Bardy, William Sievert, Katherine Stuart, Ashish Bajel, Orla
Morrissey, Nick Murphy, Mark Douglas, John Lubel, Kumar Visvanathan, Wendy Cheng,
Joshua Davis, Anouk Dev, Lynette Chee, Michael Gilbertson, Sam Miliken, Hang Quach,
Bogda Koczwara, Ben Teh, Miriam Levy, David Iser.
Acknowledgements
The Consensus Statement Group particularly acknowledge the work of Dr Venessa Pattullo,
a dedicated hepatologist who contributed enormously to the practice of hepatology in
Australia and was passionate about preventing hepatitis B reactivation in cancer patients.
Vanessa passed away during the development of these guidelines and wrote much of the
commentary on HBV testing.
Disclosures of conflicts of interest
This document was produced independently from industry funding, with support from a
competitive funding grant from the Western & Central Melbourne Integrated Cancer Service
(WCMICS, Melbourne, Australia).
page iiHBV management during cancer therapy 2019: Australian Consensus Statement
Executive summary
Approximately 239,000 Australians are living with chronic hepatitis B virus (HBV) infection;
individuals born overseas are more likely to be affected. Individuals with chronic HBV or past
exposure to HBV infection are at risk of reactivation during immunosuppressive cancer
chemotherapy. The risk of reactivation varies with the degree and duration of
immunosuppression, mechanism of action of chemotherapy, underlying HBV disease activity
and degree of liver disease. HBV reactivation can lead to liver failure, death or cancer
treatment interruption that reduces cancer survival. Oral antiviral therapy for HBV is highly
effective and known to prevent reactivation when used appropriately.
Clinical concordance with screening and treatment guidelines is inconsistent in practice.
Individualised therapeutic decisions lead to both overuse and underuse of HBV antivirals and
potentially increase medication side effects or HBV reactivation risks and increase potential
for errors.
International guidelines were developed recently following appraisal of evidence-based
practice in this area. There is a need to apply this evidence to the local epidemiology, testing
rules under Medicare, and prescribing rules under the Pharmaceutical Benefits Scheme.
This document presents the Australian consensus statement on hepatitis B management
during immunosuppression for haematological and solid-organ malignancies. When funded
access to testing and treatment are not available under current programs, we suggest that
access criteria should be re-evaluated in line with the consensus statement’s
recommendations.
This is a living document that will be updated as new data emerge. Grading of the levels of
evidence for the recommendations is described in the Methodology section.
page iiiHBV management during cancer therapy 2019: Australian Consensus Statement
Recommendations summary
Consensus recommendations GRADE
1. Who to test for hepatitis B infection
1.1. We recommend that all patients undergoing therapy for A1
haematological malignancy are tested for hepatitis B infection.
1.2. We recommend that all patients undergoing therapy for solid B1
tumours are tested for hepatitis B infection.
1.3. We suggest that the treating haematologist or medical C2
oncologist prescribing cancer therapy is responsible for
hepatitis B testing.
1.4. We recommend that HBsAg, anti-HBc and anti-HBs are A1
performed when testing for hepatitis B infection.
1.5. We recommend hepatitis B testing in children should follow the C1
same approach as for adults.
2. When to start antiviral agents
2.1. We recommend that all HBsAg positive patients with A1
haematological or solid tumour malignancy undergoing
therapy should receive antiviral prophylaxis.
2.2. We recommend that risk for HBV reactivation in patients who B1
are HBsAg negative and anti-HBc positive is determined by the
cancer therapy regimen (higher risk vs lower risk).
We make the following recommendations for patients who are
HBsAg-negative and anti-HBc positive:
2.3. Patients undergoing higher risk cancer therapy B1
(haematopoietic stem cell transplantation, B-cell depleting/B-
cell active/anti-CD20 agents, acute leukaemia and high-
grade lymphoma therapy) should receive antiviral prophylaxis.
2.4. Patients undergoing lower risk cancer therapy do not require C1
antiviral prophylaxis.
2.5. We recommend that patients without evidence of prior HBV C1
exposure (HBsAg negative/anti-HBc negative) do not require
antiviral prophylaxis.
We suggest that these patients should be assessed for HBV C2
immunity (using anti-HBs) and offered vaccination if anti-
HBsHBV management during cancer therapy 2019: Australian Consensus Statement
2.7. We recommend the use of potent, high barrier to resistance A1
nucleoside/nucleotide analogues (ie, entecavir or tenofovir)
for antiviral prophylaxis.
2.8. We recommend that all HBsAg positive patients should be C1
referred to a viral hepatitis specialist for routine assessment.
2.9. We recommend antiviral prophylaxis for children should follow C1
the same approach as for adults.
3. When to stop antiviral agents
3.1. We recommend that HBsAg positive patients should be C1
assessed at the start of cancer therapy to determine their
phase of disease and ongoing need for hepatitis B treatment
after immunosuppression.
3.2. We recommend that patients who fulfil treatment criteria for A1
chronic hepatitis B regardless of their malignancy should
remain on therapy and follow standard management
guidelines.
3.3. We recommend that patients continue prophylaxis with a B1
nucleoside/nucleotide analogue for 18-24 months after B-cell
depleting/B-cell active/anti-CD20 agent or haematopoietic
stem cell transplantation therapy provided they DO NOT fulfil
criteria for hepatitis B treatment independent of
immunosuppression status.
3.4. We recommend that patients continue prophylaxis with a B1
nucleoside/nucleotide analogue for 6–12 months post
cessation of cancer therapy (that is not B cell-depleting/B cell-
active/anti-CD20 agent or haematopoietic stem cell
transplantation therapy; see recommendation 3.3 above)
provided they DO NOT fulfil criteria for hepatitis B treatment
independent of immunosuppression status.
3.5. We recommend that ALT, HBsAg and HBV DNA level should be B1
tested every 3 months following nucleoside/nucleotide
analogue withdrawal for at least 12 months.
3.6. We recommend when to stop antiviral agents in children C1
should follow the same approach as for adults.
4. How to monitor individuals
4.1. We suggest that patients receiving antiviral prophylaxis during C2
cancer therapy should be seen 3 months after initiating
antiviral therapy, and then every 3–6 months.
4.2. We suggest that ALT and HBV DNA should be used to monitor C2
patients receiving antiviral prophylaxis during cancer therapy.
4.3. We suggest that patients’ adherence to antiviral prophylaxis C2
should be evaluated throughout therapy.
4.4. We suggest that clinicians should consider hepatitis B infection C2
for any unexplained ALT elevation among patients receiving
cancer therapy.
page vHBV management during cancer therapy 2019: Australian Consensus Statement
4.5. We recommend that all cases of HBV reactivation should be A1
urgently referred to a viral hepatitis specialist for treatment.
4.6. We recommend all children commenced on antiviral C1
prophylaxis should be monitored using the same approach as
for adults, in consultation with a viral hepatitis specialist (ideally
with paediatric expertise).
Flowchart for HBV antiviral prophylaxis in patients undergoing cancer therapy
Notes: “Lower risk” agents are all others not included in “higher risk”; implications for
monitoring and duration of antivirals are discussed in the text. +Including rituximab,
obinutuzumab, ocrelizumab, ofatumumab and ibrutinib; this is not an exhaustive list as new
agents will be introduced and more evidence about the risk of HBV reactivation comes to
light. *Lower level of evidence for risk of HBV reactivation in acute leukaemia and high-grade
lymphoma therapy.
page viHBV management during cancer therapy 2019: Australian Consensus Statement
Abbreviations
ALT Alanine aminotransferase
CI Confidence interval
EASL European Association for the Study of the Liver
eGFR estimated glomerular filtration rate
anti-EGFR epidermal growth factor receptor antibodies
GRADE Grading of Recommendations Assessment, Development and Evaluation
anti-HBc hepatitis B core antibody
anti-HBe hepatitis B envelope antibody
anti-HBs hepatitis B surface antibody
HBeAg hepatitis B envelope antigen
HBsAg hepatitis B surface antigen
HBV hepatitis B virus
HSCT haematopoietic stem cell transplantation
INR international normalised ratio
IU international units
MBS Medicare Benefits Schedule
mL millilitre
NHMRC National Health and Medical Research Council
OR odds ratio
PBS Pharmaceutical Benefits Scheme
VEGF Vascular endothelial growth factor
page viiHBV management during cancer therapy 2019: Australian Consensus Statement
Table of Contents
Executive summary ....................................................................................................................... iii
Recommendations summary ........................................................................................................ iv
Abbreviations................................................................................................................................ vii
Introduction .................................................................................................................................... 1
Methodology ................................................................................................................................... 4
1. Who to test for hepatitis B infection .......................................................................................... 5
2. When to start antiviral agents .................................................................................................. 14
3. When to stop antiviral agents .................................................................................................. 24
4. How to monitor ........................................................................................................................ 28
References ..................................................................................................................................... 31
page viiiHBV management during cancer therapy 2019: Australian Consensus Statement
Introduction
Epidemiology of hepatitis B in Australia Strait Islander peoples, who constitute 2.8% of the
total population, are estimated to represent 9% of
It is estimated that 239,000 Australians were living
people living with chronic hepatitis B. Other
with chronic hepatitis B in 2015 (1.0% population
priority populations include people with a history
prevalence), with the number of people affected
of injecting drugs, men who have sex with men,
steadily increasing (MacLachlan et al., 2018). Of
and people born in Australia whose parents
these, only 62% have been diagnosed and 15% are
migrated from endemic areas.
receiving guideline-based care (MacLachlan et al.,
2018). In addition, over 10% of all Australians – These risk factors lead to substantial heterogeneity
approximately 2.3 million individuals – are in the prevalence of chronic hepatitis B across
estimated to be hepatitis B core antibody (anti- Australia, with more than 2% of the population
HBc) positive through previous resolved infection estimated to be living with chronic hepatitis B in
(Cowie et al., 2010). some areas of Sydney, Melbourne and the
Northern Territory, and less than 0.5% of the
Most Australians living with chronic hepatitis B
population affected in other areas (MacLachlan
were born overseas in endemic areas, particularly
and Cowie, 2016).
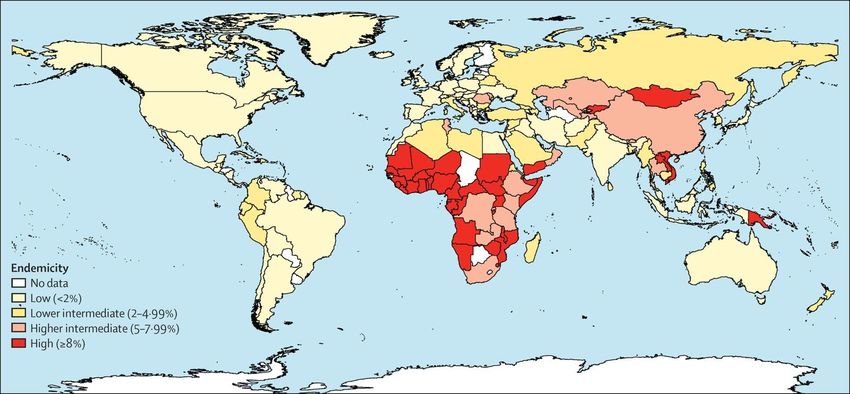
Asia and the Pacific, southern Europe and Africa
(see Figure 1). In addition, Aboriginal and Torres
Figure 1. Global HBsAg endemicity (1957–2013)
Source: Schweitzer et al. (2015). Copyright The Lancet, Elsevier 2015; reprinted with permission.
page 1HBV management during cancer therapy 2019: Australian Consensus Statement
Hepatitis B virus reactivation during haematological malignancies (Lok et al., 1991, Lau
cancer therapy et al., 2003) as well as HBsAg-positive patients
Haematological and solid tumour malignancies with solid tumours such as breast (Yeo et al., 2003,
are a major cause of illness in Australia (Australian Liu et al., 2017), lung (Lin et al., 2014, Wu et al.,
Institute of Health and Welfare, 2018). 2017), gastrointestinal (Yang et al., 2015), liver
Chemotherapy is a common treatment for (Jang et al., 2006), and head and neck (Yeo et al.,
haematological malignancies and solid tumours. 2005, Paul et al., 2016). Patients with resolved or
In 2014–15 there were 440,561 hospitalisations for past HBV infection (HBsAg negative/anti-HBc
chemotherapy, with many more patients receiving positive) also remain at risk for HBV reactivation
chemotherapy outside hospital (for example, in an (Perrillo et al., 2015), particularly patients with
outpatient or day centre) (Australian Institute of haematological malignancies undergoing therapy
Health and Welfare, 2018). Individuals with rituximab or other B cell-depleting therapies
undergoing immunosuppressive cancer therapy and novel biological agents (Mozessohn et al.,
and with serologic markers for HBV infection are 2015, Yeo et al., 2009).
at risk of HBV reactivation. Given the number of
Existing international guidelines
people undergoing cancer therapy and the
prevalence of HBV in Australia, several thousand Major international organisations, including the
people are likely to be at risk of HBV reactivation. American Gastroenterological Association (Reddy
Many of these individuals are also likely to be et al., 2015), the American Association for the
unaware of their HBV status. Study of Liver Diseases (Lok and McMahon, 2009,
Terrault et al., 2016), the Asian Pacific Association
HBV reactivation is defined as a tenfold increase in for the Study of the Liver (Sarin et al., 2016), the
HBV DNA levels from baseline in HBsAg-positive (European Association for the Study of the Liver,
individuals and as seroreversion to HBsAg 2017), the European Conference on Infections in
positivity in HBsAg-negative and anti-HBc- Leukaemia (Mallet et al., 2016), and the American
positive individuals (Reddy et al., 2015, European Society of Clinical Oncology (Hwang et al., 2015),
Association for the Study of the Liver, 2017, Lubel have produced recommendations for the testing
and Angus, 2010), although reappearance of HBV and management of HBV in patients undergoing
DNA often occurs before HBsAg (Mallet et al., cancer therapy. These guidelines were developed
2016). by expert panels based on reviews of scientific
literature and expert opinion and experience. Most
HBV reactivation has potentially serious
guidelines panels evaluated the strength of the
consequences including hepatitis flares associated
recommendation and quality of evidence available
with elevated alanine amino-transferase (ALT),
using the Grading of Recommendations
increased mortality due to liver failure, and
Assessment, Development and Evaluation
interruptions to cancer therapy that contribute to
(GRADE) system, while the European Conference
poorer curative rates and lower overall survival
on Infections in Leukaemia used the Infectious
(Paul et al., 2016, Perrillo et al., 2015).
Diseases Society of America grading system and
HBV reactivation during cancer therapy has been the American Society of Clinical Oncology did not
reported in many HBsAg-positive patients with use a formal grading system.
page 2HBV management during cancer therapy 2019: Australian Consensus Statement
Objectives of this consensus statement Advocacy statement
The purpose of this consensus statement is to make The recommendations presented in this consensus
recommendations for the testing and management statement reflect best practice at the time of
of HBV in Australian patients undergoing therapy writing. We advocate for these recommendations
for haematological and solid tumour to be reflected in the Australian funding structure.
malignancies. The Pharmaceutical Benefits Scheme (PBS) should
cover the prescription of new-generation
This consensus statement is limited to cancer
prophylactic HBV antiviral agents for patients
therapy for haematological and solid tumour
identified as at-risk of HBV reactivation during
malignancies. ‘Cancer therapy’ refers to anti-
immunosuppressive cancer therapy. The Medicare
cancer systemic treatments for haematological and
Benefits Schedule (MBS) should cover regular
solid tumour malignancies. Such systemic
HBV testing during and after cancer therapy. We
treatments usually fall into the categories of (a)
acknowledge that the recommendations may not
conventional cytotoxic chemotherapy, (b)
reflect current practice in all cancer and hepatitis
hormonal agents or (c) targeted therapy or
services across Australia. We urge health care
immunotherapy, in contrast to local therapies such
service administrators and specialists to think
as surgery or radiotherapy. Other indications for
about systems and procedures that can enable
immunosuppressive therapy such as
implementation of the best practice
rheumatologic conditions and solid organ
recommendations described in this document.
transplantation are beyond the scope of this
consensus statement.
This document is intended to be practical and
approachable for a broad audience with an interest
in the care of patients undergoing cancer therapy
and patients with chronic HBV. This includes
medical specialists, nurses and pharmacists in
cancer or hepatitis services, and general
practitioners with a special interest.
The goals of this consensus statement are:
• to prevent HBV reactivation in all patients
during and after cancer therapy, and
• for there to be no preventable mortality and no
interruptions to cancer therapy due to HBV
reactivation.
page 3HBV management during cancer therapy 2019: Australian Consensus Statement
Methodology
This consensus statement was developed by as high (A), moderate (B) or low (C). The strength
medical specialists with expertise in infectious of recommendations was classified as strong (1) or
diseases, gastroenterology, haematology, weak (2). Consensus was reached through
oncology and paediatrics, and representatives discussion within each working group. If
from the Australasian Society for Infectious disagreements arose, further discussion and
Diseases, the Gastroenterological Society of justification of opinions occurred until a consensus
Australia (Australian Liver Association), the was achieved or the steering committee made a
Haematology Society of Australia and New final decision. This final consensus statement was
Zealand, the Medical Oncology Group of reviewed and endorsed by the following medical
Australia, and the Australasian Society for HIV, societies:
Viral Hepatitis and Sexual Health Medicine.
• the Australasian Society for Infectious Diseases
This consensus statement was prepared using a (ASID);
consultative process involving the steering • the Gastroenterological Society of
committee and working parties. The Australia/Australian Liver Association
recommendations presented in this consensus (GESA/ALA);
statement were developed through a review of • the Haematology Society of Australia and New
existing guidelines and published literature, and Zealand (HSANZ);
tailored to the Australian context by referring to • the Medical Oncology Group of Australia
local epidemiology and MBS and PBS rules. (MOGA); and
• the Australasian Society for HIV, Viral
Levels of evidence for the recommendations were
Hepatitis and Sexual Health Medicine
graded according to the GRADE system (Guyatt et
(ASHM).
al., 2008). The quality of evidence was classified
page 4HBV management during cancer therapy 2019: Australian Consensus Statement
1. Who to test for hepatitis B infection
Consensus recommendations GRADE
1.1. We recommend that all patients undergoing therapy for A1
haematological malignancy are tested for hepatitis B infection.
1.2. We recommend that all patients undergoing therapy for solid tumours B1
are tested for hepatitis B infection.
1.3. We suggest that the treating haematologist or medical oncologist C2
prescribing cancer therapy is responsible for hepatitis B testing.
1.4. We recommend that HBsAg, anti-HBc and anti-HBs are performed when A1
testing for hepatitis B infection.
1.5. We recommend hepatitis B testing in children should follow the same C1
approach as for adults.
Recommendation 1.1. We recommend Hepatitis B Virus (HBV) Testing Policy Expert
that all patients undergoing therapy for Reference Committee, 2015), the Australasian
haematological malignancy are tested Society for HIV, Viral Hepatitis and Sexual Health
for hepatitis B infection.
Medicine “B Positive” monograph (Australasian
Quality of Evidence: High Society for HIV Medicine, 2014) and local clinical
Strength of Recommendation: Strong practice guidelines (e.g., Lubel et al. (2007)), and by
Background the Asian Pacific Association for the Study of the
Liver (Sarin et al., 2016), the (Gastroenterological
Several international and national guidelines Society of Australia, 2010), the European
provide recommendations as to which patients Association for the Study of the Liver (European
should be tested for serological markers of HBV Association for the Study of the Liver, 2017), and
infection prior to cancer therapy to identify and the European Conference on Infections in
manage patients at risk of HBV reactivation. Leukaemia-5 (Mallet et al., 2016).
Inconsistencies in these guidelines likely reflect
global and regional differences in HBV prevalence, A “test high-risk” approach is recommended by
the chemotherapeutic or immunosuppressive the American Gastroenterological Association
therapies used, differences in health systems, and (Reddy et al., 2015), American Association for the
cost effectiveness considerations. In particular, Study of Liver Disease (Terrault et al., 2016, Lok
recommendations for testing patients undergoing and McMahon, 2009) and American Society of
haematopoietic stem cell transplantation (HSCT) Clinical Oncology (Hwang et al., 2015) to stratify
are inconsistent. As much of the literature the risk of HBV reactivation according to the
concerning HBV reactivation in haematology individual’s risk of HBV infection (Weinbaum et
patients is retrospective or in case series, al., 2008), chemotherapeutic/immunosuppressive
knowledge gaps and limitations to the current drug class to be prescribed or planned HSCT.
evidence base contribute to the inconsistencies. Approximately 239,000 Australians are living with
A “test all” approach is recommended in the chronic hepatitis B, 38% of whom have not yet
Australian National Testing Policy (National been diagnosed (MacLachlan et al., 2018). As the
page 5HBV management during cancer therapy 2019: Australian Consensus Statement
prevalence of HBV is higher in migrants from Evidence and rationale
high-prevalence countries, it is expected that
When considering who to test for HBV prior to
adherence to the “test all” approach will identify a
cancer therapy, three approaches were considered.
significant burden of HBV within Australian
haematology patients requiring HBV prophylaxis Testing all patients before cancer therapy can
during cancer therapy, as well as after therapy has identify patients who may benefit from antiviral
been completed (for those with chronic HBV prophylaxis, allow for assessment of chronic HBV
meeting criteria for long-term therapy). complications and permit contact tracing of family
members for chronic HBV infection and link them
The cost of serological testing for HBV is covered
to care.
by the MBS; the Medicare rebate for a full panel of
tests (HBsAg, anti-HBs, anti-HBc) is A Canadian analysis of pre-treatment HBV
approximately $35 (item 69481). The cost- serological testing in patients with lymphoma
effectiveness of universal screening among receiving R-CHOP found that a “test all” approach
patients with haematological malignancies has not was associated with a tenfold lower rate of HBV
yet been determined in the Australian context. reactivation than “test only high risk” or “test
However, even outside the context of impending none” approaches. The “test all” approach is
immunosuppression, international evidence associated with the highest one-year survival rate
suggests that screening for hepatitis B may be cost and is the most cost effective (Zurawska et al.,
effective down to a population prevalence of 0.3% 2012).
(Eckman et al., 2011); the estimated prevalence in
The second approach is to screen only patients at
the Australian population is 1.0% (MacLachlan et
risk of HBV according to Centers for Disease
al., 2018).
Control “high risk” groups (Weinbaum et al.,
Technical remarks 2008). This would reduce the number of HBV tests
performed, but may miss cases of HBV if risk
1. HBV testing should include patients planned
factors are not identified or considered.
for both curative and non-curative treatment
Suboptimal testing rates have been observed in
regimens.
2. We suggest that a “test all” approach be pre-treatment oncology patients based on the “test
incorporated into institutional protocols to only high-risk” approach (Hwang et al., 2015).
ensure that HBV testing is not missed in
The third approach is to screen only patients who,
patients due to receive therapy for
if serological testing were positive, would be
haematological malignancy.
prescribed antiviral prophylaxis. In evaluating this
3. Testing for HBV should not delay cancer
approach, the prevalence of serological markers of
therapy, but ideally should occur prior to the
HBV amongst patients with haematological
initiation of chemotherapy and be up to date
malignancy, the reported risk of HBV reactivation,
(i.e., within the 12 months prior to cancer
and particular risk factors (patient factors, drug
therapy) so that HBV prophylaxis may be
class) could identify haematology patients at
prescribed concomitant with cancer therapy.
higher risk of HBV reactivation; this pathway
would then test only these patients at risk of HBV
page 6HBV management during cancer therapy 2019: Australian Consensus Statement
reactivation. Like the “test high-risk” approach, prevalence rates, reactivation risks associated with
this has the potential to miss patients, including specific therapy regimens and varying conclusions
those who, if not tested for HBV prior to low from cost-effectiveness modelling. The Australian
intensity immunosuppression (i.e., not requiring National Hepatitis B Testing policy recommends
HBV reactivation prophylaxis), might be missed if testing all patients prior to undergoing
cancer therapy was subsequently intensified. chemotherapy or immunosuppressive therapy
(National Hepatitis B Virus (HBV) Testing Policy
In view of these considerations, a “test all”
Expert Reference Committee, 2015). This
approach is strongly recommended.
recommendation is in line with recommendations
from the Centers for Disease Control and
Prevention, the American Association for the
Recommendation 1.2. We recommend Study of Liver Diseases, the American
that all patients undergoing therapy for
Gastroenterological Association, the Asian Pacific
solid tumours are tested for hepatitis B
infection. Association for the Study of the Liver, and the
European Association for the Study of the Liver.
Quality of Evidence: Moderate
Strength of Recommendation: Strong The NSW Cancer Institute Cancer Treatment
Guidelines recommend screening for all patients
Background
with solid tumours receiving curative treatment
While less frequent than in haematological and those receiving immunosuppressive
malignancy, HBV reactivation has been reported chemotherapy or high-dose glucocorticoids, but
in patients with a variety of solid tumours. not for patients with incurable solid tumours. It
Systematic reviews of patients receiving should be noted that even if a tumour is incurable,
immunosuppressive treatment for common chemotherapy may prolong life but HBV
malignancies such as breast cancer (Liu et al., 2017) reactivation may reduce the duration and quality
and lung cancer (Wu et al., 2017) report of life significantly.
reactivation rates up to 38%, with significant
The American Society of Clinical Oncology
variation among studies according to population
recommends screening of patients at high risk for
prevalence of HBV. HBV reactivation has also been
HBV infection. These include people born in a
reported in individuals with a range of underlying
country with a ≥2% HBV prevalence, household or
malignancies including nasopharyngeal
sexual contact with persons with HBV infection,
carcinoma, colorectal cancer, gastric cancer,
people with a history of injecting drug use, and
pancreatic cancer and renal cell carcinoma (Voican
men who have sex with men. The National
et al., 2016). As for patients with haematological
Comprehensive Cancer Network also
malignancy, the impact of HBV reactivation
recommends screening high-risk patients but if
includes hepatitis, chemotherapy disruption and
risk based screening cannot be implemented, then
mortality from liver failure.
universal screening should be considered.
A recommendation for screening all patients for
HBV prior to therapy for solid tumours has been
controversial based on varying population
page 7HBV management during cancer therapy 2019: Australian Consensus Statement
Technical remarks diagnosed (MacLachlan et al., 2018). The
Australian National Testing Policy recommends
1. Patients scheduled to undergo both curative
that all people from priority populations be tested
and non-curative treatment regimens should
at least once for HBV exposure using HBsAg, anti-
have HBV testing.
HBc and anti-HBs (National Hepatitis B Virus
2. In patients with very poor prognosis an
(HBV) Testing Policy Expert Reference Committee,
individualised decision not to undertake
2015). It cannot be assumed that people at
screening may be made.
particularly high risk have previously been
3. A “test all” approach should be incorporated
into institutional protocols to ensure that HBV screened, and for many patients from these
testing is not missed in patients due to receive populations, the first opportunity for HBV testing
therapy for solid tumours. may be in the context of screening prior to cancer
4. Testing for HBV should not delay cancer therapy.
therapy, but should occur prior to the initiation
Unless the HBV status of an individual from a
of cancer therapy (or be up to date within the
priority population is already recorded, it is
last 12 months) so that HBV prophylaxis may
recommended that all such people be tested for
be prescribed concomitant with cancer
HBV regardless of the underlying malignancy or
therapy.
proposed cancer therapy regimen. Priority
Evidence and rationale populations include people born in an
intermediate or high-prevalence country
Multiple cancer therapy regimens have been
(including countries in the Asia Pacific region,
associated with HBV reactivation. Alkylating
Europe, Africa/Middle East, and South America),
agents, anthracyclines, antimetabolites,
Aboriginal or Torres Strait Islander people, and
topoisomerase inhibitors and high-dose
family, sexual or household contacts of a person
glucocorticoids are regarded as being high or
with HBV infection. The identification of
moderate-risk therapies for HBV reactivation
additional risk factors for HBV infection such as
(Loomba and Liang, 2017). Multikinase inhibitors
injecting drug use, high-risk sexual activity, or
and mTOR inhibitors have also been associated
previous incarceration should also prompt testing
with HBV reactivation and death. Anti-VEGF
in unvaccinated adults. Furthermore, all people
(vascular endothelial growth factor), anti-EGFR
with primary liver cancer and all people with
(epidermal growth factor receptor) and checkpoint
evidence of chronic liver disease should undergo
inhibitors have not been associated with HBV
HBV testing.
reactivations to date (Voican et al., 2016).
Limiting HBV testing only to patients with
Clearly some individuals are at higher risk of
identified risk factors increases the risk of failing
chronic hepatitis B infection than others. However,
to identify HBV-infected patients. A study from
it is not possible to identify all those living with
France, a country of low HBV endemicity,
chronic hepatitis B based solely on country of
evaluated the ability of a screening questionnaire
birth, racial background, age, perceived risk
to identify patients with solid tumours at risk for
factors or any other specific variables. As noted
HBV (Brasseur et al., 2015). The sensitivity of their
earlier, only an estimated 62% of people living
risk-based screening questionnaire for identifying
with chronic hepatitis B in Australia have been
page 8HBV management during cancer therapy 2019: Australian Consensus Statement
HBV was only 45.5%, leading the authors to In contrast to these negative findings, a modelling
conclude that serologic testing should be study from the United States concluded that
undertaken in all patients requiring population screening for hepatitis B may be cost
chemotherapy. effective down to a prevalence of 0.3% (Eckman et
al., 2011). As noted earlier, the estimated
The cost-effectiveness of screening all patients
prevalence in the Australian population is 1.0%
undergoing chemotherapy for solid tumours has
(MacLachlan et al., 2018).
been modelled for Australia using adjuvant
therapy for early breast cancer and palliative The disparity in these findings may in part be
therapy for advanced lung cancer. In the explained by the fact that studies addressing
Australian health care system, based on 2009 patients undergoing cancer therapy may limit
costings, a “test all” (universal) approach was not cost-effectiveness analysis only to the period of
considered cost effective using an incremental cancer treatment, and not consider the long-term
cost-effectiveness ratio threshold of AUD $50,000 benefits for patients diagnosed with chronic
(Day et al., 2011a). Modelling in the adjuvant hepatitis B who undergo treatment for their
setting was associated with a 13% probability of condition. Appropriate care for people living with
being cost-effective, which increased significantly hepatitis B (including monitoring and antiviral
in populations with high rates of undiagnosed treatment where necessary) has been found to be
HBV and high HBV prevalence. However, this highly cost effective in the Australian setting
cost-effectiveness study was performed in a higher (Robotin et al., 2009). With only 15% of people
treatment cost environment (prior to generic HBV living with hepatitis B in Australia estimated to be
antiviral availability) and with a different receiving guideline-based care (MacLachlan et al.,
monitoring approach to that proposed in this 2018), there is significant scope for improvement in
document. A study from Singapore evaluated the identification and linkage to care.
cost-effectiveness of HBV screening in patients
with sarcomas and gastrointestinal stromal
tumours (Tan et al., 2016). Modelling was based on
a clinical cohort of 485 patients; 5.5% of screened
patients were HBsAg positive and 11.8% were
HBsAg negative/anti-HBc positive. None of the
patients experienced HBV reactivation. The
authors determined that a “test all” strategy was
not cost effective, except where the risk of death
from HBV reactivation was substantial. The
success of this strategy, however, relied on close
monitoring and prompt treatment of HBV
reactivation. If such close monitoring is not
undertaken, HBV reactivation may not be
promptly diagnosed and treated and a favourable
outcome not assured.
page 9HBV management during cancer therapy 2019: Australian Consensus Statement
Recommendation 1.3. We suggest that the treating clinician or person responsible so
the treating haematologist or medical that testing can be performed.
oncologist prescribing cancer therapy is 4. Testing for HBV should not delay
responsible for hepatitis B testing.
chemotherapy.
Quality of Evidence: Low
Evidence and rationale
Strength of Recommendation: Weak
Background Multiple studies have indicated that rates of
screening prior to cancer therapy in both
In clinical practice, pre-cancer therapy HBV testing haematological and solid tumour settings are low
has occurred inconsistently (Leung et al., 2011). around the world. In a recent study of HBV
This may be due to lack of consensus among screening undertaken in the USA, only 8.3% of
treating clinicians (general practitioners, nearly 10,000 patients underwent testing; patients
haematologists, medical oncologists, from Asia and those older than 50 years of age
hepatologists) as to who should perform and act were less likely to be screened, despite being at
on HBV test results, as well as a lack of higher risk than younger, non-Asian patients
institutional protocols. (Kwak et al., 2018). The authors observed that
screening rates were higher in university hospital
Despite the publication of international guidelines
clinics (20%) than in community clinic settings
and an Australian National Hepatitis B Testing
(13%) (pHBV management during cancer therapy 2019: Australian Consensus Statement
HBsAg-negative/anti-HBc-positive patients. As a avoid confusion of who will request and act on the
result, all international guidelines, as well as HBV results, and also avoid testing being missed.
approved product information, recommend HBV The need for HBV testing should be incorporated
screening prior to use of rituximab. An Australian into patient management protocols.
single-centre study reported low rates of pre-
treatment HBV screening even in this high-risk
group (Leung et al., 2011). Of 355 patients Recommendation 1.4. We recommend
undergoing treatment with rituximab, only 31% that HBsAg, anti-HBc and anti-HBs are
underwent HBV screening, and only half were performed when testing for hepatitis B
infection.
tested prior to introduction of treatment.
Quality of Evidence: High
An Australian nationwide electronic survey of
Strength of Recommendation: Strong
medical oncologists, conducted in 2009, indicated
that only a minority had adopted universal Background
screening for patients undergoing cancer
The risk of HBV reactivation in the setting of
chemotherapy (Day et al., 2011b). When asked
cancer therapy depends on HBV serological status.
why they did not screen, most cited inadequate
All current international guidelines recommend
evidence for a benefit of screening. When they did
hepatitis B surface antigen (HBsAg) testing and the
screen, patient ethnicity was reported as the reason
majority recommend hepatitis B core antibody
for screening in 82%. However, over one fifth of
(anti-HBc) testing prior to chemotherapy. Most
respondents had observed at least one case of HBV
international guidelines do not specify a
reactivation in their practice, and 30% of those
recommendation on hepatitis B surface antibody
reactivations occurred in Caucasians. Since that
(anti-HBs) testing, or do not recommend it based
time the evidence for universal screening in
on a lack of evidence. However evidence is
patients with solid tumours has firmed, and
mounting that the presence of anti-HBs in patients
international guidelines have increasingly
who are HBsAg negative/anti-HBc positive is
recommended universal screening. From this
associated with a reduced rate of HBV reactivation
survey, it would appear that medical oncologists
in the setting of treatment for haematological
accepted that it was their responsibility to decide
malignancy (Paul et al., 2017).
which patients should and should not be screened.
The MBS covers the cost of all three serological
None of the existing guidelines specifies who
tests for hepatitis B (HBsAg, anti-HBc and anti-
should be responsible for HBV testing. Our
HBs) performed at the same time. The additional
recommendation is based largely on the rationale
rebate paid for adding a third serologic marker is
that someone must be responsible for the overall
approximately $10.
care of the patient, and that the treating clinician
(or their delegate) should also be the one Technical remarks
responsible for HBV testing. Testing should be
1. HBsAg and anti-HBc tests should occur prior
undertaken if the management plan includes
to initiation of cancer therapy to guide the
prescription of cytotoxic or immunosuppressive
introduction and duration of antiviral
chemotherapy, including ‘biologics’. This will
prophylaxis for HBV reactivation.
page 11HBV management during cancer therapy 2019: Australian Consensus Statement
2. Individual tests should be ordered separately negative) provides an opportunity for HBV
to ensure the laboratory performs the correct vaccination in susceptible individuals (see
test (a request for HBV serology may not recommendation 2.5.).
provide all required results).
Evidence and rationale
3. When found in the context of HBV screening,
a positive HBsAg test indicates a diagnosis of HBsAg
chronic hepatitis B infection. Further testing
for HBeAg, anti-HBe HBV DNA and LFTs In a prospective study of 626 consecutive cancer
should be performed and the patient should be patients who received chemotherapy, the
referred to a viral hepatitis specialist for prevalence of HBsAg positivity was 12% (78/568
complete assessment and evaluation for long- tested for HbsAg) (Yeo et al., 2000). Patients with
term treatment and monitoring beyond the lymphoma had the highest prevalence of HBsAg
period of prophylaxis. positivity (15/70; 21%) in comparison to
4. Serological patterns can change over time, leukaemia/myeloma patients (1/17; 6%) and 5-13%
particularly following periods of with solid tumours. ALT elevation occurred
immunosuppression. Retesting of HBsAg and during chemotherapy in 34 of 626 patients; of
anti-HBc should be performed in patients who these, 15 cases (44%) were attributed to HBV
present with long intervals between cancer reactivation. Six of these HBV reactivations (40%)
therapy treatments (e.g., patients with relapse occurred in lymphoma cases. Overall, this
of underlying haematological malignancy).
translates to a HBV reactivation rate of 8.6% (6/70)
5. The presence of an isolated anti-HBc antibody
of all lymphoma patients included in the study.
(HBsAg negative/anti-HBc positive/anti-HBs
negative) may reflect occult hepatitis B with anti-HBc
intermittent or persistent viraemia.
Patients with chronic hepatitis B (HBsAg positive)
6. The presence of anti-HBs reduces but does not
eliminate the risk of HBV reactivation in may spontaneously lose HBsAg at an annual rate
patients who are HBsAg negative/anti-HBc of 0.5%; this is defined as “spontaneous clearance”
positive. Patients should therefore still be (Liaw et al., 2012). Alternatively, patients may
considered for HBV prophylaxis according to have serological evidence of past HBV exposure,
the recommendations of this consensus both scenarios leading to an HBsAg-negative/anti-
statement. HBc-positive state. Globally, these patients by far
7. Even when present prior to cancer therapy, outnumber those with chronic HBV. The HBV may
anti-HBs may become undetectable in the persist in hepatocytes and other tissues in the form
context of intensive or myeloablative cancer of covalently closed circular DNA. Although the
therapy (e.g., in stem cell transplant HBV DNA may not be detectable in serum,
recipients). Such patients may be at increased patients remain at risk of HBV reactivation during
risk of HBV reactivation as anti-HBs titres fall. some cancer therapy regimens (Bréchot et al., 1985,
Re-vaccination against HBV should be Chemin et al., 2001).
considered after immune reconstitution (see
recommendation 2.5).
8. The absence of any HBV serological markers
(HBsAg negative/anti-HBc negative/anti-HBs
page 12HBV management during cancer therapy 2019: Australian Consensus Statement
anti-HBs Recommendation 1.5. Hepatitis B testing
in children should follow the same
The presence of anti-HBs is not completely approach as for adults.
protective against HBV reactivation in patients
Quality of Evidence: Low
who are HBsAg negative/anti-HBc positive. There
Strength of Recommendation: Strong
is some low-level evidence that an anti-HBs titre ofHBV management during cancer therapy 2019: Australian Consensus Statement
2. When to start antiviral agents
Consensus recommendations GRADE
2.1. We recommend that all HBsAg positive patients with haematological or A1
solid tumour malignancy undergoing therapy should receive antiviral
prophylaxis.
2.2. We recommend that risk for HBV reactivation in patients who are HBsAg B1
negative and anti-HBc positive is determined by the cancer therapy
regimen (higher risk vs lower risk).
We make the following recommendations for patients who are HBsAg-
negative and anti-HBc positive:
2.3. Patients undergoing higher risk cancer therapy (haematopoietic stem cell B1
transplantation, B-cell depleting/B-cell active/anti-CD20 agents, acute
leukaemia and high-grade lymphoma therapy) should receive antiviral
prophylaxis.
2.4. Patients undergoing lower risk cancer therapy do not require antiviral C1
prophylaxis.
2.5. We recommend that patients without evidence of prior HBV exposure C1
(HBsAg negative/anti-HBc negative) do not require antiviral prophylaxis.
We suggest that these patients should be assessed for HBV immunity
(using anti-HBs) and offered vaccination if anti-HBsHBV management during cancer therapy 2019: Australian Consensus Statement
for HBsAg-positive patients at high and moderate The risk of HBV reactivation is also substantial in
risk of HBV reactivation (Reddy et al., 2015). patients with solid tumours. A recent review of
HBV reactivation in solid tumours (Paul et al.,
Evidence and rationale
2016) included 19 studies with 1751 HBsAg
Reactivation of HBV replication with increase in positive patients of whom 774 received
serum HBV DNA and ALT levels has been prophylaxis (14 studies with lamivudine, two
reported in 16–80% of hepatitis B carriers studies with lamivudine or entecavir, one study
undergoing chemotherapy (Lok et al., 1991, Levy with entecavir, and one study with lamivudine or
et al., 1990). The hepatitis flares are often adefovir). HBV reactivation in HBsAg-positive
asymptomatic; however, icteric hepatitis, clinical patients without antiviral prophylaxis ranged
hepatic decompensation and death have been from 4% to 68% (median 25%) (Paul et al., 2016).
reported. HBV reactivation is well documented in Most included studies – sub-grouped by
patients with haematological malignancies, in chemotherapy class or tumour type – reported a
particular those treated with rituximab-based greater than 10% risk of HBV reactivation. In
chemotherapy (Evens et al., 2011, Dong et al., HBsAg-positive patients, antiviral prophylaxis
2013). substantially reduced the odds of HBV
reactivation by 88% (OR 0.12, 95% CI 0.06–0.22),
Several prospective, randomised controlled trials HBV-related hepatitis by 82% (OR 0.18, 95% CI
(Hwang et al., 2012, Huang et al., 2013, Lau et al.,
0.10–0.32), and chemotherapy interruption by 90%
2003, Hsu et al., 2008, Jang et al., 2006) and
(OR 0.10, 95% CI 0.04–0.27) (Paul et al., 2016).
multiple published case series have demonstrated
the effectiveness of antiviral prophylaxis (therapy
started prior to or at the same time as starting
Recommendation 2.2. We recommend
cancer therapy), predominantly using lamivudine that risk for HBV reactivation in patients
in preventing HBV reactivation in HBsAg-positive who are HBsAg negative and anti-HBc
patients receiving cancer therapy. positive is determined by the cancer
therapy regimen (higher risk vs lower risk).
A systematic review (Loomba et al., 2008) of the
Quality of Evidence: Moderate
effect of prophylactic lamivudine on HBV
Strength of Recommendation: Strong
reactivation during chemotherapy of HBsAg-
positive patients included 14 studies with 275 Background
patients receiving lamivudine prophylaxis and 485
Recommendations for prophylaxis in HBsAg-
control patients who were not given lamivudine.
negative/ anti-HBc-positive patients undergoing
Prophylactic lamivudine therapy decreased HBV
cancer therapy vary across international
reactivation and HBV-related hepatitis by 80–
guidelines. Various factors are used to recommend
100% and eliminated HBV-related hepatic failure.
antiviral prophylaxis, including chemotherapy
Cancer-related mortality was decreased in the
regimen, presence of HBV DNA, presence of anti-
lamivudine treated patients, probably by reducing
HBs, and underlying disease. The European
the need for delay or interruption of cancer
Association for the Study of the Liver and the
therapy.
Asian Pacific Association for the Study of the Liver
page 15HBV management during cancer therapy 2019: Australian Consensus Statement
guidelines recommend that HBsAg-negative/anti- Evidence and rationale
HBc-positive patients with detectable HBV DNA
Higher vs lower-risk cancer therapy
should be treated similarly to HBsAg-positive
patients (i.e., should receive HBV antiviral In this consensus statement, higher-risk cancer
prophylaxis) (European Association for the Study therapy for HBsAg-negative/anti-HBc-positive
of the Liver, 2017, Sarin et al., 2016). European patients refers to HSCT, B cell-depleting/B cell-
Association for the Study of the Liver and Asian active/anti-CD20 agents (including rituximab,
Pacific Association for the Study of the Liver obinutuzumab, ocrelizumab, ofatumumab and
guidelines also suggest prophylaxis in all HBsAg- ibrutinib) and acute leukaemia and high-grade
negative/anti-HBc-positive patients with lymphoma therapy (see Figure 2). Some
undetectable HBV DNA who receive rituximab combinations of cancer therapies may also elevate
(anti-CD20) and/or combined regimens for reactivation risk and should be considered on an
haematological malignancy, if they are anti-HBs individual basis.
negative and/or if close monitoring of HBV DNA
HBsAg-negative/anti-HBc-positive patients
is not guaranteed (European Association for the
Study of the Liver, 2017, Sarin et al., 2016). The receiving rituximab-containing chemotherapy
American Association for the Study of Liver remain at risk of HBV reactivation (Hsu et al., 2014,
Diseases does not make a specific Mozessohn et al., 2015, Yeo et al., 2009). Studies of
HBsAg-negative/anti-HBc-positive patients with
recommendation for prophylaxis in HBsAg-
haematological malignancy who underwent
negative/anti-HBc-positive patients due to
treatment with rituximab have found that even
insufficient evidence. The American
Gastroenterological Association’s risk-based patients with undetectable HBV DNA at baseline
are at risk for HBV reactivation (Huang et al., 2013,
approach includes prophylaxis for HBsAg-
Hsu et al., 2014).
negative/anti-HBc-positive patients treated with
B-cell-depleting agents such as rituximab and Due to the profound immune suppression
suggests prophylaxis for HBsAg-negative/anti- associated with chemotherapy conditioning before
HBc-positive patients undergoing treatment that HSCT, HBsAg-negative/anti-HBc-positive patients
places them at moderate risk (e.g., tumour necrosis undergoing HSCT are at high risk of HBV
factor alpha inhibitors, tyrosine kinase inhibitors, reactivation (Hammond et al., 2009, Mallet et al.,
prolonged or high-dose corticosteroids) (Reddy et 2016). The risk of reactivation may be higher in
al., 2015). The American Society of Clinical allogenic HSCT than in autologous HSCT (Yoo et
Oncology and European Conference on Infections al., 2015).
in Leukaemia recommend prophylaxis for HBsAg-
negative/anti-HBc-positive patients with high risk Evidence for HBV reactivation in HBsAg-
of reactivation (e.g., rituximab or HSCT) (Hwang negative/anti-HBc-positive acute leukaemia and
et al., 2015, Mallet et al., 2016). high-grade lymphoma receiving therapy that does
not contain B cell-depleting/B cell-active/anti-
CD20 agents is limited. Studies with HBsAg-
negative/anti-HBc-positive patients receiving
chemotherapy without rituximab for acute
page 16HBV management during cancer therapy 2019: Australian Consensus Statement
leukaemia and high-grade lymphoma reported prophylaxis in HBsAg-negative, anti-HBc positive
rates of HBV reactivation of 2.0–12.5% (Paul et al., individuals. All anti-HBc-positive individuals
2017, Totani et al., 2015, Chen et al., 2015a, Lok et receiving novel immunotherapies and targeted
al., 1991). therapies should be monitored closely,
particularly when used in combination with other
There is limited evidence on the risk of HBV
immune suppressing agents
reactivation in HBsAg-negative/anti-HBc-positive
patients not receiving higher-risk cancer therapy. HBV DNA
A prospective study of 32 HBsAg-negative/anti-
Most international guidelines recommend HBV
HBc-positive patients with solid tumours
DNA testing when HBsAg and/or anti-HBc are
undergoing non-B cell-depleting chemotherapy
positive (Sarin et al., 2016, European Association
(for example, cyclophosphamide, methotrexate,
for the Study of the Liver, 2017, Mallet et al., 2016,
docetaxel) reported no HBV reactivation in the
Reddy et al., 2015, Terrault et al., 2016, Lok and
follow-up period (up to 36 months) (Federico et al.,
McMahon, 2009, Hwang et al., 2015). The presence
2017). This study suggests that the risk of
of HBV DNA in HBsAg-negative/anti-HBc-
reactivation is low in this patient group, but
positive patients indicates occult HBV infection.
further research is required.
Patients with isolated anti-HBc (HBsAg
Emerging classes of immunotherapy or targets negative/anti-HBs negative) may have occult HBV
agents, for example checkpoint inhibitors and with detectable viraemia and be at increased risk
tyrosine kinase inhibitors have been reported to of HBV reactivation. An Australian study with
cause HBV reactivation with uncertain 1,451 patients found that prevalence of occult HBV
mechanisms (Voican et al., 2016, Chang et al., 2017, infection was 0.69% (Martinez et al., 2015),
Bui and Wong-Sefidan, 2015). In studies of novel suggesting that it is rare in Australia. Given this
immunotherapies, patients with HBV exposure rare occurrence of HBV DNA, universal HBV
(anti-HBc positive) have been required to be on DNA testing for all HBsAg-negative/anti-HBc-
suppressive HBV antivirals making it difficult to positive patients is not cost effective and would
determine reactivation risks currently. Immune detect HBV DNA in very few individuals.
stimulating drugs can also cause immune- However, if patients are already known to have
mediated hepatitis (independent of HBV) or other occult infection, it is reasonable to treat them as
organ inflammation, sometimes requiring the use similar to HBsAg-positive patients and prescribe
of other immune supressing medications like antiviral prophylaxis.
steroids. While contributing to HBV reactivation in
anti-HBs
some circumstance, tyrosine kinase inhibitors have
not been classified as high risk in previous There is insufficient evidence about the role of
systematic reviews (Perrillo et al., 2015). anti-HBs in protecting against HBV reactivation in
HBsAg-negative/anti-HBc-positive patients (see
At this stage, novel immunotherapies and targeted
recommendation 1.4.). Meta-analyses have
therapies are not consider high-risk drugs when
explored the protective role of anti-HBs, finding
used alone. HBsAg-positive individuals should be
79% lower odds of reactivation among people with
given prophylaxis (as with all other cancer
anti-HBs compared to without anti-HBs (both anti-
therapies), but their use should not prompt
page 17You can also read