Burn Care in the Austere Environment - Special Operations Medical ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

6/29/2018
Burn Care in the Austere
Environment
Julie A. Rizzo, MAJ, MC, U.S. Army
U.S. Army Institute of Surgical Research
Fort Sam Houston, TX
• Because of the hazards of military operations (for
both combatants and non-combatants), burns are a
common injury pattern
• Objectives:
1) Review burn casualty assessment
2) Review initial stabilization
3) Review wound care options
1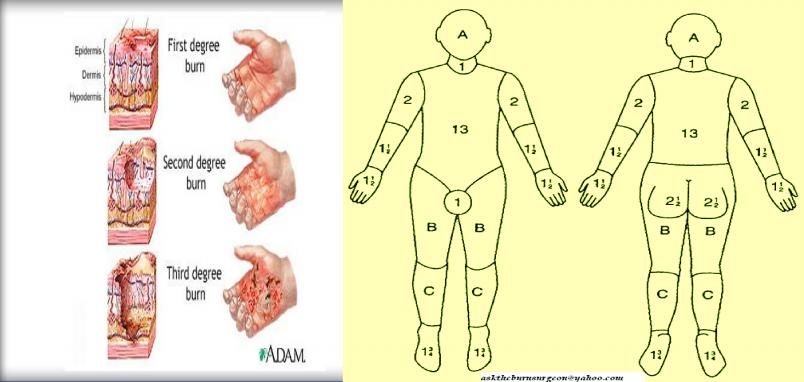
6/29/2018
Burn Care – Operational Considerations
Austere Environment Burn Care Requirements
• Limited resources • Extensive resources
• Limited personnel • Multi-disciplinary team
• Limited expertise • Subject matter experts
• Limited time • Longitudinal care
Phases in burn care
• EMERGENCY assessment and care (TC3)
• RESUSCITATION (usually hours 0-48)
• Definitive care (from initial excision until wounds
are closed)
• Rehabilitation (begins during resuscitation and
lasts the remainder of the casualty’s life)
*Definitive care and rehabilitation are difficult if not
impossible to provide in the deployed setting
2
6/29/2018
Emergency Assessment
• Interrupt the burning process
• Stop life-threatening bleeding
• Secure the airway if needed
• Decompress tension pneumothorax
• Brush off dry chemicals
• Rinse off dirt and contaminants
• Prevent hypothermia
THE BURN IS NOT THE FOCUS
INITIALLY !!
- ASSESS FOR LIFE-THREATENING
PROBLEMS IN THE ABC’S!!
- Reassess the ABC’s/Repeat M-A-R-
C-H constantly while caring for the
burned trauma patient
3
6/29/2018
Airway Injury
• Intubate all patients with:
• Large burns (>40% TBSA)
• Deep facial burns
• Symptomatic smoke
inhalation injury (voice change,
difficulty breathing, accessory
muscles, anxious)
• Use a size 8 endotracheal tube or larger
(less likely to get obstructed with debris and clot)
• Secure the tube in place with umbilical ties; adhesives do not stick
• Place an NG tube in all intubated patients
• SECURE THE AIRWAY EARLY!
Burn Wound Edema +
Resuscitation
• Just After Arrival • One Hour Later
4
6/29/2018
Initial Stabilization
• Obtain IV access anywhere possible
• Sew or staple all IV lines and vascular catheters in
place!!!
• Warm the patient (sheets, blankets) and the environment
(room temp >85 degrees)
• Tetanus prophylaxis
• IV antibiotics are not indicated (unless associated injury or
an identified source of infection)
Define the Burn
DEPTH and SURFACE AREA
5
6/29/2018
Superficial Burns
• First-degree burns
– Only the epidermis is damaged.
– Think “sunburn” - skin is dry, red, painful.
– Heal without intervention and without scarring.
• Superficial Second-degree burns
(Superficial Partial-thickness)
– Damage extends part-way into the dermis; hair
follicles, glands, etc, are preserved.
– Skin is moist, red, blanches, blisters, and is
extremely painful.
– Healing can be slow but scarring is infrequent.
Deep Burns
• Deep Second-degree burns
(Deep Partial-thickness)
– Damage extends deep into the
dermis and hair follicles, glands,
etc, are often destroyed.
– Skin is less moist, slow to blanch,
but may still be painful.
– Heal mostly with scarring and
contracture over several weeks.
Skin grafting may be necessary to
avoid these problems.
6
6/29/2018
Deep Burns
• Third-degree burns (Full-
thickness)
– All layers of the skin are destroyed.
– Can be any color (white, black, red,
brown), dry and leathery to the
touch, usually not painful (dermal
plexus of nerves destroyed).
– Heal by scarring and contracture of
the wound over a long time. Skin
grafting is almost always necessary.
– Circumferential full-thickness burns
of the extremities and trunk may
require decompression
(escharotomy) to avoid ischemic
complications.
Burn Surface Area
Percent total body surface area:
% TBSA = 2nd degree + 3rd degree
burns
• Burns >20% TBSA usually
need resuscitation.
In adults, use the "Rule of Nines" or
the Lund-Browder chart to
approximate % TBSA
The patient’s HAND = approximately
1% TBSA
7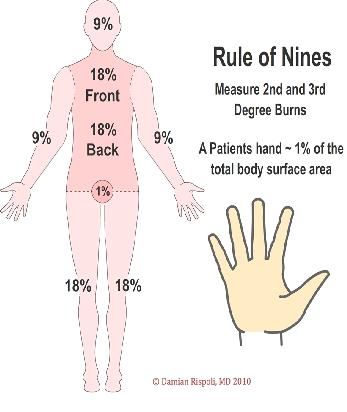
6/29/2018
Adult Resuscitation Strategy
1. Estimate % TBSA
2. Apply the RULE OF TENS…
for casualties between 40-80kg with burns >15% TBSA
10 x % TBSA = initial fluid rate in mL/hour
for casualties > 80kg
add 100mL/hr for each extra 10kg
Use Lactated Ringer’s (LR) or other isotonic fluid
(Plasmalyte)
Sample Calculation
• 40y M AD soldier injured in fire at a fuel point,
approx 70kg, approx 50% TBSA
• RULE OF TENS:
Weight is between 40-80kg? yes
10 x 50 = 500
500mL/hour LR infusion
1 bag of LR needed every 2 hrs
8
6/29/2018
Adult Resuscitation Strategy
• The Rule of Tens (and all formulas) only gives the initial estimated hourly rate.
• Monitoring the resuscitation:
– Place foley catheter
– Check UOP hourly
– Goal UOP is 30-50mL/hr
– Increase/decrease the LR rate each hour
by 20-25% to maintain UOP at 30-50mL/hr
Example:
Starting LR rate of 500mL/hr
UOP decreases to 10mL/hr
Increase the LR rate by 20%
500 x 0.20 = 100
500 + 100 = 600mL/hr new LR rate
3 bags of LR needed every 5 hrs
Oral Rehydration Therapy
• IV solutions may not be available
• Water alone (and most common sports drinks) can lead to
dangerous hyponatremia in the volumes required for burns
• Commercial options:
– World Health Organization (WHO) Oral Rehydration Salts (ORS)
solution (preferred)
– Pedialyte®
• Homemade options:
– Per 1L water – 8tsp sugar, 0.5tsp salt, 0.5tsp baking soda
– Per quart Gatorade® - 0.25tsp salt, 0.25tsp baking soda
• Weight-based dosing (start with 10mL/kg per hour and advance up
to 1500mL/hr in adults if well-tolerated)
9
6/29/2018
Resuscitation Morbidity
• Over-resuscitation can be deadly!
– Acute respiratory distress syndrome (ARDS)
– Abdominal compartment syndrome (ACS)
– Extremity compartment syndrome
– Orbital compartment syndrome
• Hourly fluid management is critical - use the JTTS Burn
Resuscitation Flow Sheet to record both fluid intake and
UOP.
APPENDIX A
JTTS Burn Resuscitation Flow Sheet, Page 1 of 3
#2 Use “Rule of Tens” to
Date Initial Treatment Facility
calculate adult starting LR
Calculate Rule of
%TBSA
Name SSN
Pre-burn
(Do not
include
Tens
>4055)
CVP
0.02-0.04 u/min)
Bladder Pressure (Q4)
DSN 312-429-2876 or
1st burntrauma.consult.army@mail.mil
nd
2
3rd
4th
5th
6th
7th
8th
9th
#3 Titrate LR hourly to
10th
11th achieve UOP 30-50
12th
13th
ml/hr and tissue
14th perfusion
15th
16th
17th
18th
19th
20th
21st
22nd
23rd
#4 If 24 hour projected fluid total
24th
Total Fluids: (Use adjuncts if >24hr max) *Titrate LR hourly to maintain adequate UOP (30-50ml/hr) and perfusion >250mL/kg, use adjuncts and
monitor for fluid overload
106/29/2018
Abdominal
compartment
syndrome
• Large fluid resuscitations
• Increased intraabdominal
pressure
• Decreased preload, CO
• Renal failure
• Mesenteric ischemia
• Decreased lung
compliance, increased
ETCO2, pCO2
• Measure bladder pressure
250 ml/kg during first 24 h: DANGER
Indicators of Adequate Resuscitation
• Urine output 30-50mL/hr (adults)
• Clear mentation (follows commands)
• Appropriate tachycardia (100-120’s) and blood
pressure (MAP >55)
• Peripheral pulses should be palpable (or
dopplerable if edema is present)
116/29/2018
Escharotomy
• Full thickness circumferential extremity burns
can have a tourniquet effect
• Full thickness circumferential torso burns can
restrict ventilation
• Treatment (or prophylaxis) is escharotomy – the
full thickness of burned skin is incised
longitudinally to release the underlying tissues.
• Escharotomy may be required prior to transport
Basic Burn Wound Care
• Burns do not need to be formally dressed in the first 24-48
hours, especially if the patient is unstable or if multiple
transport stops are being made
• A CLEAN SHEET to cover the patient or CLEAN GAUZE
WRAPS will suffice in most cases prior to transport
• Leave blisters in place and transfer to a surgical facility
• Avoid wet dressings or hydrogels initially in burns >20%
TBSA – these can lead to hypothermia
126/29/2018
Basic Burn Wound Care
• Facial burns: thin layer of bacitracin or similar antibiotic
ointment
• Ear burns: thick layer of mafenide acetate (sulfamylon)
cream
• Eye burns: IRRIGATE, use fluorescein test if available
– Apply ophthalmic bacitracin if no globe injury
– Cover with fox shield (do not use gauze)
– Send to ophthalmologist
Basic Burn Wound Care
• Superficial partial thickness burns: thin layer of bacitracin
covered by gauze
• Deep partial thickness burns:
– Silver nylon bandages covered with water-moistened gauze
– Moistened gauze with 5% sulfamylon solution
– Thin layer of silvadene cream covered by gauze
• Full thickness burns: Thin layer of sulfamylon cream (daily)
alternating with silvadene cream (nightly)
136/29/2018
Considerations for Casualties Who
Cannot Be Evacuated
• Care provided in theater is not envisioned to be definitive.
• Things that worsen outcomes:
- Age
- Inhalation injury
- Associated traumatic injuries
- Delay in treatment
• At >50% TBSA full thickness burns, local national patients in the
CENTCOM AOR are generally triaged as expectant.
• If full thickness burns compriseYou can also read