Causal Inference Approaches for Understanding the Social Determinants of Substance Abuse and Depression in the 21st Century: The Opioid Epidemic ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Please do not remove this page Causal Inference Approaches for Understanding the Social Determinants of Substance Abuse and Depression in the 21st Century: The Opioid Epidemic and the Great Recession Swift, Samuel L. https://scholarship.miami.edu/discovery/delivery/01UOML_INST:ResearchRepository/12355360940002976?l#13355512550002976 Swift, S. L. (2019). Causal Inference Approaches for Understanding the Social Determinants of Substance Abuse and Depression in the 21st Century: The Opioid Epidemic and the Great Recession [University of Miami]. https://scholarship.miami.edu/discovery/fulldisplay/alma991031447520902976/01UOML_INST:ResearchR epository Embargo Downloaded On 2021/10/22 14:56:27 -0400 Please do not remove this page
UNIVERSITY OF MIAMI CAUSAL INFERENCE APPROACHES FOR UNDERSTANDING THE SOCIAL DETERMINANTS OF SUBSTANCE ABUSE AND DEPRESSION IN THE 21ST CENTURY: THE OPIOID EPIDEMIC AND THE GREAT RECESSION By Samuel L. Swift A DISSERTATION Submitted to the Faculty of the University of Miami in partial fulfillment of the requirements for the degree of Doctor of Philosophy Coral Gables, Florida May 2019
©2019 Samuel L. Swift All Rights Reserved
UNIVERSITY OF MIAMI A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy CAUSAL INFERENCE APPROACHES FOR UNDERSTANDING THE SOCIAL DETERMINANTS OF SUBSTANCE ABUSE AND DEPRESSION IN THE 21ST CENTURY: THE OPIOID EPIDEMIC AND THE GREAT RECESSION Samuel L. Swift Approved: ________________ _________________ Adina Zeki Al Hazzouri, Ph.D., M.Sc. Tali Elfassy, Ph.D., M.P.H. Assistant Professor Assistant Professor Department of Epidemiology Division of Epidemiology Mailman School of Public Health Department of Public Health Columbia University Sciences ________________ _________________ Hermes Florez, M.D., Ph.D., M.P.H. Zinzi Bailey, Sc.D., M.S.P.H. Professor Assistant Scientist Division of Epidemiology Jay Weiss Institute for Health Department of Public Health Sciences Equity, Sylvester Comprehensive Cancer Center ________________ ________________ Daniel J. Feaster, Ph.D. Guillermo Prado, Ph.D. Professor Dean of the Graduate School Division of Biostatistics Department of Public Health Sciences
SWIFT, SAMUEL L. (Ph.D., Epidemiology) (May 2019) Causal Inference Approaches for Understanding the Social Determinants of Substance Abuse and Depression in the 21ST Century: The Opioid Epidemic and the Great Recession Abstract of a dissertation at the University of Miami. Dissertation supervised by Assistant Professor Adina Zeki Al Hazzouri. No. of pages in text (83) The great recession and the opioid epidemic are two defining public health events of the 21st century. Within the context of these two events, the 21st century has been marked by increases in mortality due to suicide, alcohol misuse, and drug overdose among Americans, and especially among white Americans, warranting further epidemiological investigation. For example, in recent years a black-white disparity in opioid pain reliever (OPR) misuse has emerged such that white Americans are more likely to suffer opioid overdoses or opioid related hospitalizations than black Americans. There is evidence to support that much of the opioid epidemic is related to overprescribing of OPR medications, and that whites are more likely to be prescribed these medications than blacks. In aim 1 of this dissertation I build on prior work which suggests that discrimination in medical settings may actually be protective against iatrogenic outcomes in medicine. I postulate that discrimination could result in less prescribing of OPR medications for blacks and thus a lower risk of OPR misuse. While most epidemiologic studies rely on a self-reported measure of OPR misuse, these measures are often an underreport of true OPR misuse when
compared with gold standard measures. Aim 2 of this dissertation examines the possible bias introduced to the observed associations of aim 1 which uses self- reported OPR misuse. Finally, in aim 3 of this dissertation, I examined the great recession of 2008, another defining public health event of the 21st century which resulted in shocks to financial wellbeing that were felt by persons worldwide, and its effect on drug misuse, alcohol misuse, and depression. During the great recession in the United States shocks to financial wellbeing such as unemployment drastically increased, while median income and household assets decreased. While shocks to financial wellbeing have been shown to be associated with increased depressive symptoms, the associations between these shocks and alcohol and drug use behaviors are less understood. As a whole, this dissertation aims to better understand how the opioid epidemic and the great recession have played out with regards to the social axes of class and race, using causal inference methods. All three of my aims were evaluated using the Coronary Artery Risk Development In young Adults study (CARDIA) which is an ongoing prospective longitudinal cohort study of black and white adults who were ages 18 to 30 when they were enrolled in the study in 1985. This sample is ideal for these dissertation aims because the participants were adults during the opioid epidemic and at the peak of their working years during great recession of 2008 (mean ages 45-50). Additionally, this study collects rich data on discrimination, as well as socioeconomic data related to employment, income, debts and assets.

In aim 1 of the dissertation, I first assess the black vs white disparity in OPR misuse, and then I evaluate whether racial discrimination in medical care settings mediates this disparity. In my framework, race is the exposure, racial discrimination in a medical care setting is the mediator, and OPR misuse is the outcome. I used causal mediation analysis to compute the total effects and controlled direct effects, which are as follows: the total effect (TE) is the effect of race on OPR misuse, adjusted for measured confounders; and the controlled direct effect (CDE) is the effect of race on OPR misuse when discrimination is set at the same level for all participants, adjusted for measured confounders. I calculated inverse probability treatment weights (IPTW) for discrimination to address confounders that also act as mediators. I found that black participants were more likely to report discrimination in a medical setting (20.3% vs 0.9%) and less likely to report OPR misuse (OR=0.71, 95% CI= 0.55, 0.93), in the total effect model. In my final model adjusting for the IPTW of the confounding/mediating variables, my controlled direct effect suggests that when everyone is set to being not discriminated against, the disparity is wider such that black persons are further less likely to report OPR misuse (OR=0.63, 95% CI=0.45, 0.89) compared to their white counterparts. These findings suggest racial discrimination in medical settings is a risk factor for OPR misuse rather than protective. In aim 2 of the dissertation, I evaluate how potential measurement error in discrimination could have influenced the findings of aim 1. Validation studies that compare self-reported misuse with urine or hair analysis show that self-reporting
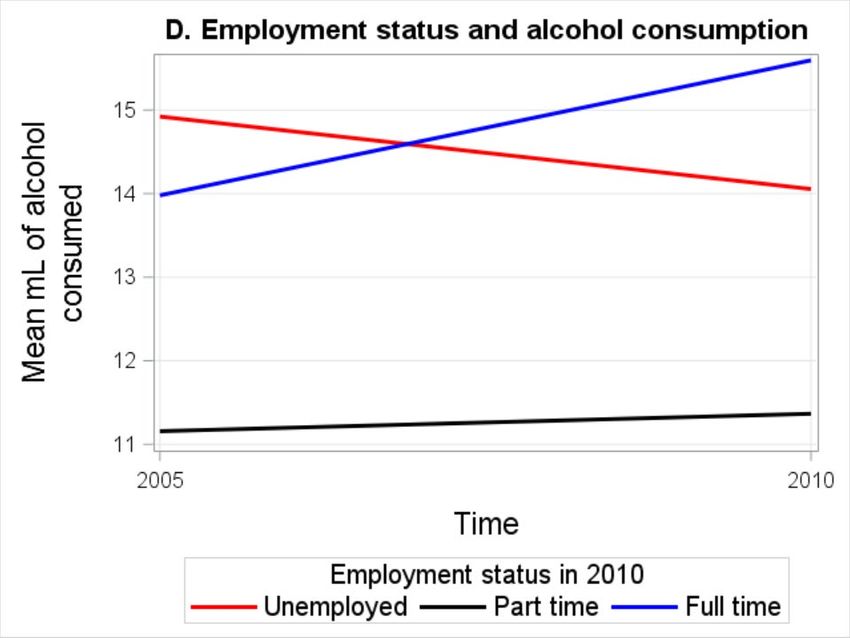
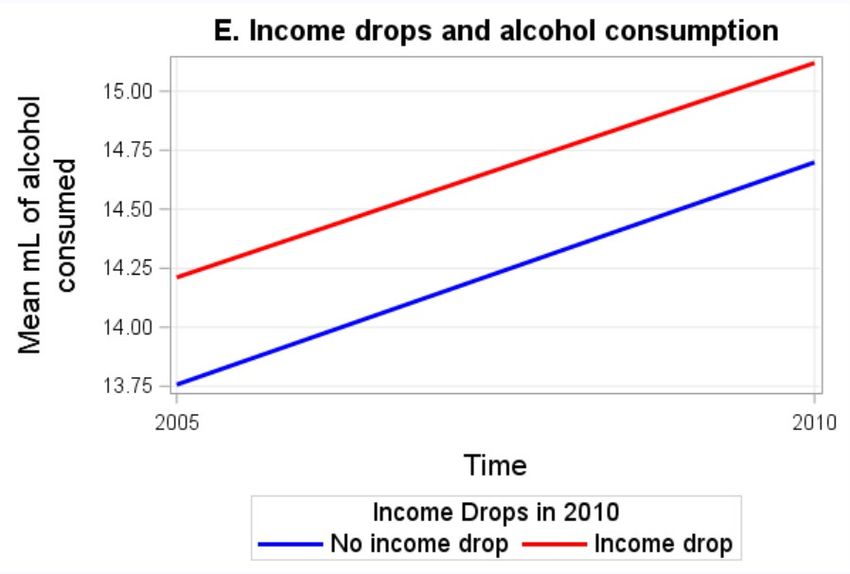
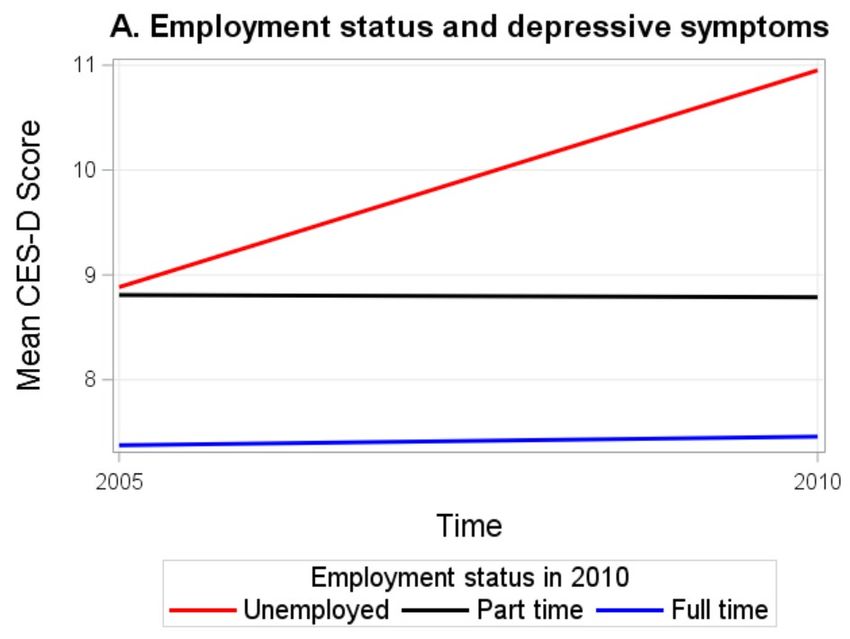
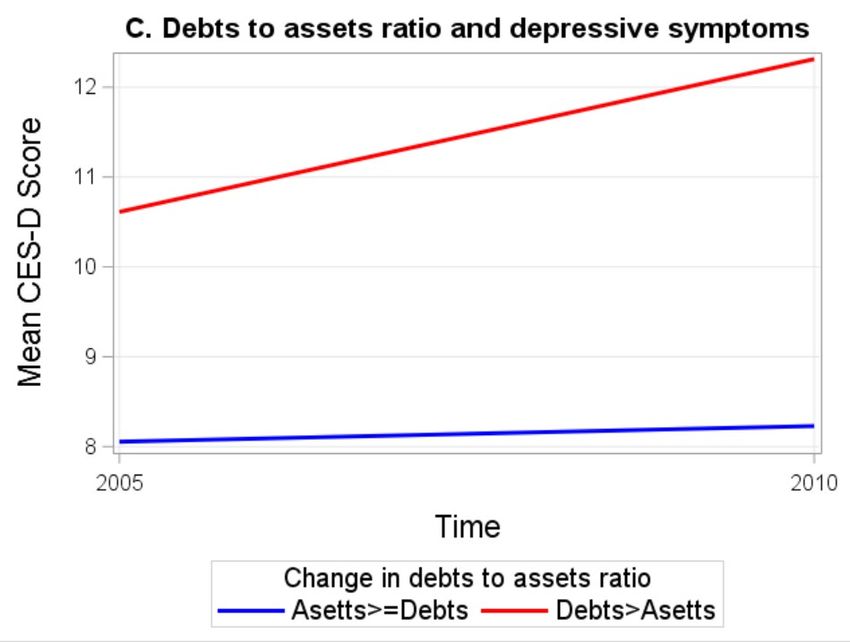
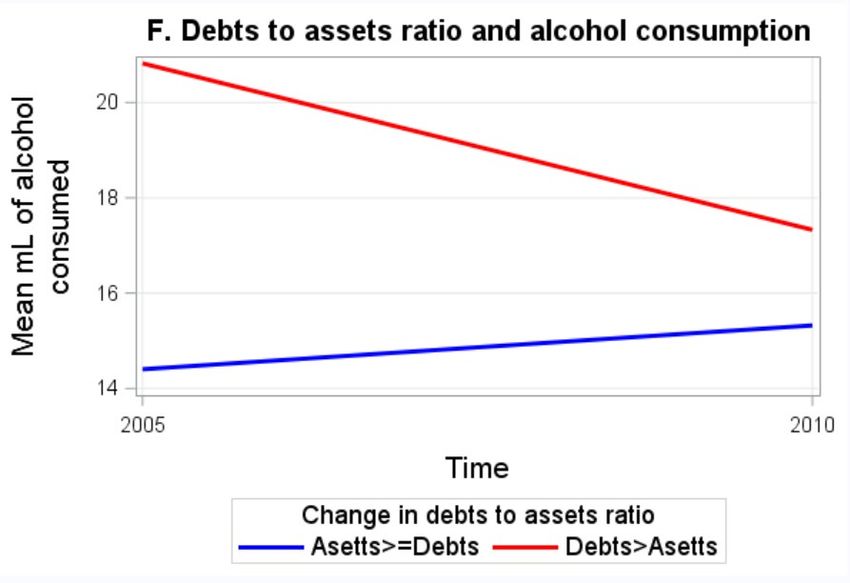
of OPR misuse is usually underreported, often at very low levels of sensitivity. In this aim I use probabilistic bias analysis applying different values of the sensitivity of self-reported OPR misuse to the observed bivariate relationships between race and OPR (from aim 1). Assuming a non-differential misclassification and a sensitivity of 75% among blacks and 90% among whites, which is higher than that found in validation studies among high risk OPR users, our aim 1 black-white disparity (i.e. race – OPR association) reflects an overestimate of the true disparity (bias corrected OR =0.94, 95% CI =0.91, 0.97) vs. observed OR=0.73, 95% CI= 0.57, 0.93). When we change the sensitivity among blacks to a very low level (50%) with the white sensitivity at 75%, the observed black-white disparity would actually flip (bias corrected OR= 2.13, 95% CI=1.51, 3.30 vs. observed OR= 0.73, 95% CI= 0.57, 0.93). In aim 3 of the dissertation, I use a fixed effects design to examine how within person change in financial well-being at time of the great recession influenced depressive symptoms, alcohol and drug misuse. I consider three types of shocks to financial wellbeing: unemployment, drops in income, and a shift in the ratio of household debts to assets. In my final models, I found that unemployment was associated with an increase in depressive symptoms (β=2.0, 95% CI=0.6, 3.3). A shift in debts to assets ratio was also associated with an increase in depressive symptoms (β=1.3 95% CI= 0.1, 2.5) but a decrease in daily mL of alcohol consumed (β=-4.1, 95% CI= -6.7, -1.5). While the associations between shocks to financial wellbeing and drug misuse were not
statistically significant, the odds ratios suggest that these shocks were a possible risk for drug misuse. Taken together, these three aims illustrate methodological approaches to evaluating research questions pertaining to some of the most currently pressing public health issues. The results of aim 1 suggest that racial discrimination in a medical setting is a risk factor for OPR misuse rather than being protective, and thus could not explain the seen black-white disparity in OPR misuse. This finding is consistent with previous literature on discrimination and substance misuse among other health outcomes. Further research is needed to investigate the mechanisms behind the black–white disparity in OPR misuse, including the source of OPR medications. In aim 2 I found that differential misclassification of OPR misuse at levels similar to those found in validation studies has the potential to significantly bias observed associations. In aim 3 I found that unemployment and shifts in debts to assets ratio during the great recession increased depressive symptoms. A shift in debts to assets ratio also decreased the total mL of alcohol consumed. These results highlight the complex relationship between recessions and health and the importance of examining different types recession related shocks.
Dedication For Neal Stewart and for all the people in Albuquerque. iii
Acknowledgments In chronological order of influence on my life: I would like to acknowledge my parents and their spouses for inspiring me to seek knowledge and believe in justice. I am grateful to my sister for being an inspiration to my life constantly and often editing my writing. Academically and professionally I have also had several mentors who changed my life forever, and it is likely that I would not be here without them. My high school photography teacher Annie Bromberg taught me that the world is full of art and beauty if you look at it right. My paramedic field trainers Randy Anderson (rest in peace) and Sean Robertson took a big chance on me and gave me my start at Albuquerque Ambulance, which is where I came of age. Dr. Celia Iriart, my MPH mentor taught me the importance of using public health as a lens to make larger critiques about society. At the New Mexico Department of Health Dr. Michael Landen and Dr. Lois Haggard taught me how to put that worldview into real life public health practice. Especially for this dissertation I would like to acknowledge the people on my committee who are helping me cross this major milestone in my life. Dr. Feaster and Dr. Florez have supported me through their courses and also as knowledgeable experts who I look up to in this field. Dr. Bailey is the type of epidemiologist I would like to be someday, and I am lucky to have had her as a collaborator and as committee member. Dr. Elfassy went above and beyond guiding me through multiple analyses and challenges in the program and I am very grateful to her for going the extra mile to help me learn so much. Finally, my dissertation chair Dr. Adina Zeki Al Hazzouri has definitely changed the course of iv
my life through her mentorship in this program. Under her mentorship I have not only learned an incredible amount of epidemiology, but more importantly I believe in myself much more than I did before, which is the best lesson a mentor can teach. I sincerely hope to take what everyone has taught me and continue to grow moving forward in my career. v
Table of Contents LIST OF FIGURES……………………………………………...……………………..vii LIST OF TABLES…………………………………………………………………...…viii Chapter 1: Introduction…………………………………………………………………1 Chapter 2: Methodological Overview………………………………………………….7 Chapter 3: The Opioid Epidemic and Racial Discrimination in a Medical Care Setting…………………………………………………………………………………..11 Chapter 4: Probabilistic Bias Analysis for Misclassification……………………….31 Chapter 5: The Great Recession, Depressive Symptoms, Alcohol Misuse and Drug Misuse…..………………………………………………………………………..46 Chapter 6: Conclusions……………………………………………………………….70 References……………………………………………………………………………..74 Appendix A: Aim 1 Supplemental: SAS Code………………………………………81 Appendix B: Aim 2 Supplemental: STATA Code…………………………………..82 vi
LIST OF FIGURES Figure 3.1…..…………………………………………………………………………..12 Figure 3.2 ………………………………………………………………………………13 Figure 3.3..……………………………………………………..………………………18 Figure 4.1..……………………………………………………..………………………35 Figure 4.2..……………………………………………………..………………………35 Figure 5.1..……………………………………………………..………………………53 Figure 5.2..……………………………………………………..………………………54 Figure 5.3..……………………………………………………..………………………62 vii
LIST OF TABLES Table 3.1. ……………………………………………………………………………....20 Table 3.2……………………………………………………………………………..…22 Supplementary Table 3.1………………………………………..……………………24 Supplementary Table 3.2………………………………………..……………………25 Supplementary Table 3.3………………………………………..……………………26 Supplementary Table 3.4………………………………………..……………………27 Table 4.1………………………………………..………………………………………37 Table 4.2………………………………………..………………………………………39 Table 4.3………………………………………..………………………………………41 Table 4.4………………………………………..………………………………………41 Table 5.1………………………………………..………………………………………58 Table 5.2………………………………………..………………………………………59 Table 5.3………………………………………..………………………………………60 Table 5.4………………………………………..………………………………………61 viii
Chapter 1: Introduction I. Overview In the United States the 21st century has been marked by two notable public health challenges, the opioid epidemic and the great recession. As is shown by Case and Deaton, after decades of improving all-cause mortality rates in the United States, in the 21st century all-cause mortality actually increased among whites, which is a trend not seen in other developed nations. Case and Deaton attribute this phenomena to increases in drug overdoses, suicides, and alcohol related mortality, which offset decreases in cancer and heart disease mortality1. Case and Deaton paint a bleak portrait of this current trend in mortality in the United States, naming these deaths “deaths of despair”. The broad objective of this dissertation is to better understand the social determinants of this modern despair, disentangling how the current social conditions of the United States may be influencing these unprecedented trends in substance misuse and depression related outcomes. Substance misuse and depressive symptoms are particularly sensitive to social stressors such as discrimination and shocks to financial wellbeing. Class and race are two (of many) important axes to consider when examining the ways that social subordination, inequity, and other unjust conditions existing in modern life influence health outcomes. In this dissertation I examine two specific aspects of social determinants related to racial discrimination and financial wellbeing, understanding that the broader influence of these large constructs falls outside of the scope of a single dissertation. First, I examine the role of racial discrimination 1
2 in a medical care setting in the black-white disparity in Opioid Pain Reliever (OPR) misuse. Second, I examine how measurement error may influence observed disparities in OPR misuse, which is an important consideration for epidemiologists wanting to make stronger inferences. Finally, I examine the relationship between shocks to financial wellbeing during the great recession and depressive symptoms, alcohol misuse, and drug misuse. As these are difficult and important questions to ask using observational epidemiological data, I explore methodological approaches for improving the inferences I can make about my results. Taken together, the three aims of this dissertation use emerging causal inference methodologies in epidemiology to provide a critique of some of the defining public health issues of the current generation. II. The Need for Causal Inference Methods Our three research aims are not only poised to ask difficult questions about the public health challenges of the United States in the 21st century, they are designed to explore methodological approaches to exploring these questions. When evaluating the influence of social factors like discrimination and shocks to financial wellbeing, traditional methods in observational epidemiology may not be sufficient. As exposures these constructs are often hard to define, difficult to measure, unethical to randomize, and subject to confounding, both observed and unobserved. Meeting causal assumptions is often a challenging task when investigating the relationships between measures of social or economic factors and health. When evaluating the role of racial discrimination in a medical setting in the relationship between race and OPR misuse, careful consideration of the
3 mediation analysis approach and causal structure of this relationship is required. When assessing relationships using self-reported variables, careful consideration of the influence of measurement error is also required in assessing this relationship. Finally, a true controlled experiment in which participants are randomly assigned different levels of financial status would be difficult and likely unethical to conduct. In lieu of a truly randomized experiment, the great recession provides researchers with a natural experiment in which I can exploit a fixed effects design to examine the associations between shocks to financial wellbeing and depressive symptoms, substance misuse, and drug misuse, making stronger inferences about the results. Causal inference methods, including causal mediation analysis (chapter 3), probabilistic simulation studies to assess measurement error (chapter 4), and fixed effect models (chapter 5) are all tools that can fill the gap of better understanding contemporary issues in social epidemiology. III. Dissertation Aims As explained above, one goal of this dissertation is to provide an example of how emerging epidemiological methods can be better applied to observational data to understand the context of social issues in public health today. More specifically, this dissertation will use causal mediation to examine the mediating role of racial discrimination in the opioid epidemic, simulation methods to assess measurement bias in measurement of OPR misuse, and finally fixed effects methods to examine the ways that the great recession may have influenced
4 mental health, alcohol misuse, and drug misuse. My specific research aims are as follows: Aim 1 (chapter 3): Evaluate whether a black–white disparity in OPR misuse exists, and if so whether racial discrimination in a medical setting mediates such disparity in OPR misuse, using causal mediation methods. H1.1. Black or African Americans will be at a lower risk of OPR misuse than whites in my sample. H1.2 Discrimination will act as a mediator in this relationship and will explain the black–white disparity in OPR misuse. This will be evaluated by looking at the controlled direct effect of race on OPR misuse. Aim 2 (chapter 4): Assess measurement error in self-reported OPR Misuse across categories of race and racial discrimination in a medical setting, using probabilistic bias analysis. H2.1: When assessing the role of differential misclassification of OPR misuse across categories of race, the introduction of significant bias will change the effect estimate observed in the black-white disparity in OPR misuse and its interpretation. . H2.1: When assessing the role of differential misclassification of OPR misuse across categories of racial discrimination in a medical setting, the introduction of significant bias will change the effect estimate in the bivariate relationship between racial discrimination in a medical setting and OPR misuse and its interpretation.
5 Aim 3 (chapter 5): Evaluate the influence of three shocks to financial wellbeing during great recession (employment status, income and debt to assets ratio) on outcomes related to depressive symptoms, alcohol misuse and drug misuse using a fixed effects design. H3.1. Persons who experienced unemployment, an income drop, or a shift in debt to assets ratio during the great recession will have increased depressive symptoms following the great recession. H3.2. Persons who experienced unemployment, an income drop, or a shift in debt to assets ratio during the great recession will have decreased total alcohol consumption and lower odds of binge drinking behavior following the great recession. H3.3. Persons who experienced unemployment, an income drop, or a shift in debt to assets ratio during the great recession will have higher odds of drug misuse following the great recession. IV. Summary The opioid epidemic and the great recession are two defining American public health issues in early 21st century. Taken together, research on the health consequences of these two issues helps us make a deeper critique of issues of disparity, racial discrimination, and economic inequity in American life, diving deeper into the conditions influencing Case and Deaton’s “deaths of despair”. Through the dual lenses of the opioid epidemic and great recession, this dissertation will explore racial disparities in opioid misuse and the role of racial
6 discrimination in such disparities, and the effect of the great recession on depressive symptoms, alcohol misuse, and drug misuse outcomes. These research questions pose serious methodological challenges. Epidemiology has shifted from the infectious disease focused perspectives of the 19th and 20th centuries to a focus on chronic disease, substance abuse, and social epidemiology. Just as threats to public health have evolved, so must my methodological approaches to understanding the causes and consequences of social maladies. Causal inference methods, including causal mediation analysis, probabilistic simulation studies to assess measurement error, and fixed effect models are all tools that can fill the gap of better understanding contemporary issues in social epidemiology.
Chapter 2: Methodological Overview I. Overview In this chapter I review the cohort study I employ in this dissertation, I broadly review the methodological approaches that I use to evaluate each aim. The measures, methods and statistical approaches for each aim are discussed in greater detail in each study’s respective chapter 3, 4 and 5. II. Study Sample We evaluated all three aims using the Coronary Artery Risk Development in young Adults (CARDIA) sample. The CARDIA study is an ongoing multisite prospective cohort study of the determinants of clinical and subclinical cardiovascular disease. In 1985 and 1986 a total of 5,114 black and white adults were recruited into this study from four field centers which include: The University of Alabama at Birmingham, The University of Minnesota, Northwestern University, and Kaiser Permanente in Oakland California. Participants were followed from 1985-86 to the present with follow up visits in 1987-88, 1990-91, 1992-93, 1995-96, 2000-01, 2005-06, 2010-11, and 2015-16. Details of the study design are described elsewhere2. The study was IRB approved at each field center. The CARDIA Study is especially well suited to answer the questions posed in this dissertation because it includes a sample of black and white adults who were going into their 30s, 40s and early 50s during the opioid epidemic and the great recession. As is noted by Case and Deaton, the largest increases in “deaths of despair” were among white males in their 40s3, making this sample 7
8 well suited for assessing these research questions. Furthermore, the CARDIA study includes a wealth of information on the social determinants of health, such as discrimination and financial wellbeing. These determinants are described in greater detail in the methods sections of chapters 3, 4 and 5. III. Aim 1 (Chapter 3) Methodological Overview In Aim 1 I employ mediation models using causal mediation structures for binary outcomes as outlined by VanderWeele and Vansteelandt4. Causal mediation approaches build on traditional mediation approaches outlined by Baron and Kinney5 by allowing for exposure mediator interactions and using counterfactual logic to assess more causal effects. For this Aim, I will first examine the black-white disparity in OPR misuse. Second, I will employ a causal mediation framework to examine whether racial discrimination in a medical setting may be mediating such disparity. I use marginal structural models and construct inverse probability treatment weights to account for time variant confounding variables that may also act as mediating variables. IV. Aim 2 (Chapter 4) Methodological Overview. When compared to gold standard instruments like hair or urinalyses6-11, previous research shows that underreporting is common when OPR misuse (outcome of interest in Aim1) is self-reported. The objective of this aim is then to examine different situations related to misclassification of OPR misuse, and how
9 different levels of sensitivity of self-reported OPR misuse could be biasing the observed effect sizes of the relationships in Aim 1. A full discussion of the methodological approach for Aim 2 is provided in more detail in chapter 4. I examined OPR misclassification scenarios across categories of race and racial discrimination in a medical setting. I employ the episensi package in STATA12, which is a tool made for these types of probabilistic bias analyses. The episensi package allows me to quantify the size of the bias, inputting various levels of sensitivity and specificity (bias parameters) on the classification of my outcome (OPR misuse) and examining the influence that these levels of bias parameters has on my observed effect. The episensi package does this by allowing users to specify a probability density function for each bias parameter, and then uses Monte Carlo simulations to generate simulated datasets based on summary data from the measured data. The episensi package then averages effect sizes across a user specified number of simulated datasets, producing “bias adjusted estimates”. V. Aim 3 (Chapter 5) Methodological Overview Recessions provide researchers with an opportunity to take advantage of a “natural experiment” using observational data. The structure of the fixed effects design is described in detail in some texts13, but the overall idea of this design is rather simple. By examining within person variation rather than between person variation during an exogenous event such as a recession, the fixed effects design compares individuals to themselves at different time points. Said differently, in a fixed effects design individuals act as their own controls, which
10 offers several advantages from a causal inference perspective. By having individuals act as their own controls, this design removes the threat of time invariant confounding, both measured and unmeasured. Additionally, if an exposure is truly exogenous, the fixed effects design allows for epidemiologists to say a study is quasi-experimental rather than observational, also allowing for stronger causal inferences.
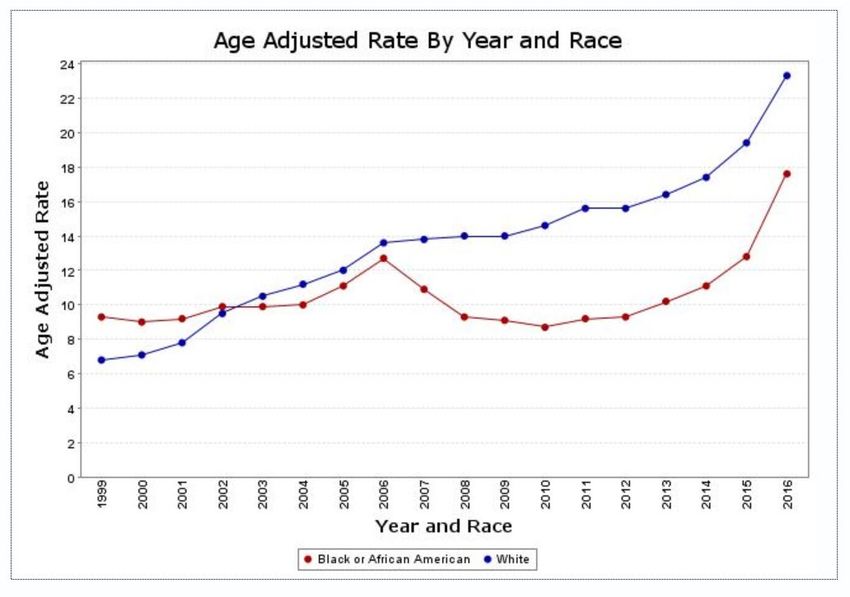
Chapter 3: The Opioid Epidemic and Racial Discrimination in a Medical Care Setting I. Chapter 3 Introduction Drug overdose death rates within the United States nearly tripled between 1999 and 201514. Vital records data, opioid sales data, and other sources suggests that a large portion of this increase in deaths is attributable to Opioid Pain Relievers (OPRs) such as oxycodone, hydromorphone and oxymorphone15,16. The National Institute on Drug Abuse (NIDA) defines misuse of prescription drugs as “taking a medication in a manner or dose other than prescribed; taking someone else’s prescription, even if for a legitimate medical complaint such as pain; or taking a medication to feel euphoria (i.e., to get high)”17. During the prescription opioid epidemic, death rates attributed to OPR overdose among whites have been more than twice that of the rates seen among blacks16, and whites have had significantly higher rates of hospitalization due to OPRs than blacks18. This interesting pattern black vs white substance misuse is reflected in all cause drug overdose death can be seen in figure 1.1, which was produced using vital records data. From the 1990s to early 2010s OPR misuse was attributable mostly or in part to patterns of OPR overprescribing in the United States15. The sales of OPRs within the United States increased by almost 500% between 1999 and 2011 and the same time the rates of OPR related deaths were tripling15, as can be seen in figure 1.2. Given this knowledge, it would follow that any racial/ethnic disparities in OPR misuse could be related to disparities in 11
12 OPR prescribing, based on the premise that less prescribing for minorities might result in fewer opportunities for misuse. Figure 3.1 Drug overdose death by year and race within the United States, 1999- 2016 Source: Centers for Disease Control14 A recent review paper found that across 70 studies of prescribing patterns, racial and ethnic minorities received less treatment for acute and chronic pain than their white counterparts19. A study of disparities in opioid prescribing in pain- related emergency room visits also showed blacks to have a lower odds of receiving OPRs than whites20. These disparities pose several interesting questions related to discrimination in medical care and drug misuse in the United States. Perceived interpersonal discrimination (henceforth called discrimination)
13 Figure 3.2 Opioid sales, deaths and treatment admissions within the United States, 1999 to 2010. Source: Kolodny et al, 201515 due to race within the medical care setting has been associated with negative healthcare service outcomes and underutilization of preventive services21,22. Using an experimental design and actors playing cardiac patients, one study found that given identical clinical presentations for white and black patients, physicians were more likely to recommend white patients for cardiac catheterization than black patients23. In another study, Krieger et al. hypothesized that the lack of prescription of hormone therapy to black women, due to discrimination, was likely the reason why black women had lower rates of breast
14 cancer in the 1990s before the results of the Women’s Health Initiative Study showed an association between these hormones and breast cancer24. In this chapter I will examine the relationship between race and OPR misuse (i.e. the black-white disparity), and whether discrimination in a medical setting acts as a mediator in this relationship. Following the evidence from the studies noted above23,24, I hypothesized that racial discrimination in a medical setting would result in under prescribing of OPR to blacks, which would then result in lower OPR misuse among blacks and thus explain the black-white disparity. II. Chapter 3 Methods a. Mediator: Perceived discrimination in a medical setting prior to year 2000 Discrimination is measured using the Experiences of Discrimination (EOD) instrument, which has been previously validated25. The discrimination questions were asked in years 1992, 2000, 2005, 2010 and 2015. Study participants were asked “have you ever experienced discrimination, been prevented from doing something, or been hassled, or made to feel inferior in any if the following situations because of your race?”. They were then presented with situations/domains, which included, “at school,” “getting a job,” “getting housing,” “at work,” “at home,” “getting medical care,” or “on the street in a public setting”. In this study, I used discrimination because of race in “getting care in a medical setting” (and not in any other setting). Since the question reflects lifetime experience, I used discrimination from exam years 1992 and 2000 for my
15 exposure of interest, thus reflecting lifetime discrimination prior to year 2000. These two exam years were combined to increase the sample size of persons who experienced discrimination in a medical setting, while I used other approaches/definitions in sensitivity analyses (described later). b. Outcome: Nonmedical Opioid Pain Reliever (OPR) Misuse from 2005 to 2015 CARDIA participants were asked about lifetime illicit drug misuse in all examination years. For this analysis, I combined lifetime OPR misuse in exam years 2005, 2010 and 2015 as my outcome, excluding people who reported OPR or opiate misuse in years 2000 and prior. This allowed us to capture new users and that OPR misuse took place after my exposure period (defined above). In exam year 2005, the question combined heroin and prescription opioids, with a follow-up question that specifically asked if a participant used “Heroin,” “Dilaudid,” Morphine,” “Demerol,” “Oxycodone,” “Hydromorphone,” or “other prescription opioids” for non-medical reasons. For exam year 2005, participants that used only heroin and no other opioids were not included as being OPR misusers. In all subsequent exam years OPR misuse (non-medical use or prescription opioids) was asked about in a question separate from non- pharmaceutical opiate misuse (heroin and other non-prescription opiates), so these exclusions were not necessary.
16 c. Covariates Participants reported their race (white vs. black), sex, age, years of educational attainment, total household income (collected in 8 brackets and treated continuously using the midpoint dollar amount of bracket), and health insurance status (insured vs. not). Parental SES was operationalized measured as the highest level of education in years achieved by any parent or guardian. Depressive symptoms were measured using the Center for Epidemiological Studies depression scale (CES-D) instrument, which includes 20 items and ranges from 0-6026. All covariates were measured in year 1992 (study baseline, and when discrimination was first measured), except for depressive symptoms which was measured in year 1990. d. Statistical Analysis Of the 4617 participants who were present at any exam between 1992 and 2015, I excluded 264 participants without a measure of lifetime discrimination in 1992/2000. Since the OPR question is also a lifetime measure, I further excluded 318 participants who by exam year 2000 had misused OPR at least once in their lifetime, and further excluded 507 participants with missing OPR measures in 2005, 2010 and 2015. This left a final analytical sample of 3528 persons. As such, for this analysis, I established temporality between exposure and outcome by defining the exposure period as lifetime medical discrimination prior to year 2000, and the outcome period as any OPR misuse in years 2005 through 2015.
17 I first compared black and white participants across my covariate characteristics using chi-squared tests and t-tests. Next, I used a causal mediation framework to assess whether there is a racial disparity in OPR misuse, and if so, whether this disparity could be explained by discrimination. The directed acyclic graph (DAG) for this research question is presented in Figure 1. Race as the exposure/ treatment (white =0 (reference), black=1), discrimination in a medical care setting as the mediator (M=1 discrimination, M=0 no discrimination), and OPR misuse as the outcome (Y=1 OPR misuse, Y=0 no OPR misuse). I performed causal mediation analysis as described by Valeri and VanderWheele27, a method that uses counterfactual contrasts to compute a total effect (TE) and a controlled direct effect (CDE) for the relationship of interest. The total effect (TE) is the effect of race on OPR misuse, adjusted for measured confounders; and the controlled direct effect (CDE) is the effect of race on OPR misuse when discrimination is set at the same level for all participants (either M=0 or M=1), adjusted for measured confounders. I focus on the CDE, setting M to 0 (i.e. no discrimination), because it makes little sense to imagine the racial inequality if both whites and blacks all encountered racial discrimination in medical care. I consider the following variables as confounders of the discrimination–OPR path: parental SES, sex, age, and study site. Variables such as education, income, depressive symptoms, and insurance status are confounders of the discrimination–OPR path but are also descendants of race and thus mediators of the race–OPR path (see Figure 3.3).
18 Figure 3.3. Directed Acyclic Graph for Proposed Relationship Between Race, Discrimination in a Medical Care Setting, and OPR Misuse. Since my outcome was rare (
19 race as describing the racial inequality in OPR misuse, and the controlled direct effect (CDE, setting the mediator to zero) as the magnitude of the racial inequality I would expect if discrimination were absent for both blacks and whites. Due to the nature of mediation models, I conducted the following sensitivity analyses. First, I performed an analysis excluding participants who reported lifetime discrimination in 1992 but not in 2000, as this pattern is indicative of inconsistent responses to the question. Second, I conducted an analysis examining “recent” discrimination rather than lifetime discrimination, by including only persons who reported discrimination in a medical setting in 2000 and not in 1992 or prior. Third, since the opioid epidemic has been characterized by increases in prescribing of OPRs for various conditions related to both chronic and acute pain15, I conducted an analysis adjusting for self-reported pain in year 2000 as a proxy variable for pain related conditions that may influence OPR misuse. Participants were asked the following question: “During the past 4 weeks, how much did pain interfere with your normal work (including work outside the home and housework)?”; and responses were coded as “no pain, a little bit of pain to moderate pain, or quite a bit of pain to extreme pain”. In a final sensitivity analysis, I analyzed the effect of discrimination on the racial disparity in OPR misuse outside of a causal mediation framework. The latter was done by assessing the association between discrimination and OPR misuse, stratified by race. All analyses were conducted using SAS version 9.4 and SAS University Edition Software29.
20 III. Chapter 3 Results As shown in table 3.1, black participants were much more likely to report experiencing discrimination in a medical setting (20.3% vs 0.9%) and less likely to report OPR misuse (5.8% vs 8.0%). Black participants were more likely to be female, have lower incomes, lower educational attainment, and lower parental SES, and were more likely to have elevated depressive symptoms (CES-D≥16). Table 3.1. Baseline Characteristics of Study Participants by Race, CARDIA Study, 1992-2015 Black White P n= 1717 n= 1811 value Age (years), mean, (SD) 31 (3.8) 32 (3.4)
21 CI=0.55, 0.93) compared to their white counterparts. Adjusting for all measured confounders, the controlled direct effect in model 2 suggests that when everyone is set to being not discriminated against (M=0), black persons would have 0.63 times the odds of reporting OPR misuse (OR=0.63, 95% CI=0.45, 0.89) compared to their white counterparts. Adjusting for all measured confounders as well as confounders/mediators, the controlled direct effect in model 3 suggests that when everyone is set to being not discriminated against (M=0), black persons would have 0.55 times the odds of reporting OPR misuse (OR=0.55, 95% CI=0.38, 0.80) compared to their white counterparts. Finally, the controlled direct effect in model 4 which uses stabilized weights to account for measured confounding, suggests that when everyone is set to being not discriminated against (M=0), black persons would have 0.65 times the odds of reporting OPR misuse (OR=0.65, 95% CI=0.46, 0.91) compared to their white counterparts. The results of my four sensitivity analyses can be seen in Supplementary Tables 3.1, 3.2, 3.3, and 3.4. In my first sensitivity analysis (Supplemental Table 3.1), I assessed measurement error in the lifetime discrimination measure by excluding 127 participants who inconsistently responded to the discrimination measure across years 1992 and 2000, and my results were largely similar to those seen in my main analysis (Table 3.2). In my second sensitivity analysis (Supplemental Table 3.2) including only “recent” experience of discrimination in a medical setting, my sample size of persons who experienced discrimination was drastically reduced (n=116) and thus I were unable to draw conclusions from these models, however the point estimates were in the same direction as my
Table 3.2. Relationship of Race, Discrimination in a Medical Setting, and OPR Misuse Using Causal Mediation Methods, CARDIA Study (N=3528) Total effect CDE: Adjusted for CDE: Adjusted for Marginal (model 1) discrimination and discrimination, structural model confounders confounders, and (model 4) (model 2) confounders/mediators (model 3) OR 95% CI OR 95% CI OR 95% CI OR 95% CI Black vs. white 0.71 (0.55, 0.93) 0.63 (0.45, 0.89) 0.55 (0.38, 0.80) 0.65 (0.46, 0.91) No discrimination vs. discrimination 0.54 (0.34, 0.86) 0.50 (0.31, 0.83) 0.51 (0.31, 0.83) Model 1 is adjusted for race; Model 2 is adjusted for race, medical discrimination and confounders (parental SES, age, sex, and study site); Model 3 is adjusted for race, medical discrimination, confounders (parental SES, age, sex, and study site), and confounders/mediators (education, income, depressive symptoms, and insurance status); Model 4 is adjusted for race and medical discrimination, and uses stabilized inverse probability weights to account for the confounders and confounders/mediators (see supplemental SAS code). 22
23 main analysis. In my sensitivity analysis adjusting for self-reported pain as a confounder (Supplemental Table 3.3), the results were also similar to those seen in table 3.2. In my final sensitivity analysis (Supplemental Table 3.4), when the sample is stratified by race, I see that discrimination in a medical setting is associated with significantly greater odds of OPR misuse among blacks (OR= 1.74, 95% CI= 1.06, 2.86), and similarly a greater odds among whites, though not statistically significant (OR= 3.15, 95% CI=0.87, 11.45). IV. Chapter 3 Discussion Our findings are counter to my original hypothesis that discrimination in a medical setting would be protective against iatrogenic effects of healthcare-related opioid misuse and thus a mediator of the black-white disparity. While my total effect of 0.71 suggests that blacks have lower odds of OPR misuse compared to whites – which is in line with the established rates of racial disparity in OPR misuse16,18 – in my final model my controlled direct effect of 0.65 became more protective (i.e. further away from the null), thus widening the disparity and suggesting that discrimination in a medical setting is a risk factor, rather than a protective factor, for OPR misuse. We hypothesized that racial discrimination in a medical setting would result in less treatment and thus under prescribing of OPR to blacks, which would then result in lower OPR misuse among blacks, and thus explain the observed black- white disparity. As my findings were counter to my hypothesis, I must consider the possibility that misused OPR medications originated from potential sources
Supplementary Table 3.1: Relationship of Race, Discrimination in Medical Settings, and OPR Misuse Using Causal Mediation Methods, Restricted to Participants Whose Answer to Lifetime Discrimination was Consistent Across Years 1992 and 2000, CARDIA Study (N=3,401) Total effect CDE: Adjusted for CDE: Adjusted for Marginal structural model (model 1) discrimination and discrimination, (model 4) confounders confounders, and (model 2) confounders/mediators (model 3) OR 95% CI OR 95% CI OR 95% CI OR 95% CI Black vs. white 0.71 (0.55, 0.93) 0.64 (0.45, 0.9) 0.54 (0.37, 0.79) 0.65 (0.46, 0.91) No discrimination vs. discrimination 0.61 (0.34, 1.01) 0.52 (0.28, 0.95) 0.52 (0.29, 0.95) Model 1 is adjusted for race; Model 2 is adjusted for race, medical discrimination and confounders (parental SES, age, sex, and study site); Model 3 is adjusted for race, medical discrimination, confounders (parental SES, age, sex, and study site), and confounders/mediators (education, income, depressive symptoms, and insurance status); Model 4 is adjusted for race and medical discrimination, and uses stabilized inverse probability weights to account for the confounders and confounders/mediators (see supplemental SAS code). 24
Supplementary Table 3.2: Relationship of Race, Recent Discrimination in Medical Settings, and OPR Misuse Using Causal Mediation Methods, CARDIA Study (N=3,528) Total effect (model CDE: Adjusted for CDE: Adjusted for Marginal structural model 1) discrimination and discrimination, (model 4) confounders confounders, and (model 2) confounders/mediators (model 3) OR 95% CI OR 95% CI OR 95% CI OR 95% CI Black vs. white 0.71 (0.55, 0.93) 0.70 (0.51, 0.98) 0.61 (0.43, 0.88) 0.72 (0.52, 0.98) No discrimination vs. discrimination 0.77 (0.35, 1.72) 0.66 (0.29, 1.51) 0.66 (0.29, 1.49) Recent discrimination was constructed by restricting to participants answering “Yes” to Lifetime Discrimination in 2000 but “No” in 1992. Model 1 is adjusted for race; Model 2 is adjusted for race, medical discrimination and confounders (parental SES, age, sex, and study site); Model 3 is adjusted for race, medical discrimination, confounders (parental SES, age, sex, and study site), and confounders/mediators (education, income, depressive symptoms, and insurance status); Model 4 is adjusted for race and medical discrimination, and uses stabilized inverse probability weights to account for the confounders and confounders/mediators (see supplemental SAS code). 25
Supplementary Table 3.3: Relationship of Race, Discrimination in Medical Settings, and OPR Misuse Using Causal Mediation Methods, additionally adjusted for Self-Reported Pain in Models 3 and 4 (N= 3,528) Total effect (model CDE: Adjusted for CDE: Adjusted for Marginal structural model 1) discrimination and discrimination, (model 4) confounders confounders, and (model 2) confounders/mediators (model 3) OR 95% CI OR 95% CI OR 95% CI OR 95% CI Black vs. white 0.71 (0.55, 0.93) 0.63 (0.45, 0.9) 0.56 (0.38, 0.84) 0.63 (0.44, 0.90) No discrimination vs. discrimination 0.54 (0.34, 0.86) 0.53 (0.31, 0.90) 0.52 (0.31, 0.88) Model 1 is adjusted for race; Model 2 is adjusted for race, medical discrimination and confounders (parental SES, age, sex, and study site); Model 3 is adjusted for race, medical discrimination, confounders (parental SES, age, sex, and study site), and confounders/mediators (education, income, depressive symptoms, insurance status and self-reported pain); Model 4 is adjusted for race and medical discrimination, and uses stabilized inverse probability weights to account for the confounders and confounders/mediators including self-reported pain. 26
Supplementary table 3.4. Association of Discrimination with OPR Misuse, Overall and by Race, CARDIA Study Overall Black White (n=3528) (n=1717) (n=1811) OR 95% CI OR 95% CI OR 95% CI Unadjusted No discrimination - - - (ref) Discrimination 1.27 (0.86, 1.88) 1.56 (0.99, 2.46) 2.49 (0.71, 8.78) Adjusted No discrimination - - - (ref) Discrimination 1.48 (0.97, 2.28) 1.74 (1.06, 2.86) 3.15 (0.86-11.45) *Models adjusted for sex, age, study site, and parental SES 27
28 other than the medical setting, such as the diversion of OPR medications and black market sale of these medications. A recent paper estimated that 42% of OPRs prescribed in the emergency department may be ultimately misused, either by the patient or persons close to them30. Given these diversion rates, prescribing practices may have little impact on the actual availability of OPR medications for persons who would misuse them. This could be a larger problem in the future, as recent research points to a new shift in the opioid epidemic since 2010, wherein the large disparity in black versus white OPR misuse from the 1990s to 2010 (largely driven by prescription OPRs) has narrowed in recent years due to the return to synthetic and illicit OPRs31. Our findings suggest that discrimination in a medical setting is a risk factor for OPR misuse. This is further illustrated in my stratified sensitivity analysis, where discrimination in a medical setting increased the odds of OPR misuse among blacks as well as whites. The relationship between discrimination in a medical care setting and OPR misuse I found is likely similar to the relationship observed between discrimination in any other setting and negative outcomes. In this cohort, experiences of discrimination in any setting have been associated with several negative health outcomes, including lower birthweight among mothers who reported such experiences32, greater waist circumference33, and increased sedentary behaviors34. There is also a large body of evidence supporting the relationship between perceived discrimination across all settings and increased substance misuse and risky behaviors among both whites, blacks and other groups35-42, suggesting that substance misuse could be a coping
You can also read