COVID Oximetry @home COVID virtual wards - Remote monitoring of people at risk from COVID-19 using pulse oximeters February 2020 - Academic ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
COVID Oximetry @home COVID virtual wards Remote monitoring of people at risk from COVID-19 using pulse oximeters February 2020

Matt Inada-Kim National Clinical Director Infection & Deterioration NHS England and NHS Improvement @mattinadakim

WHY? Late Early presentations Silent hypoxia
56 year old, usually well man with a PMH of hypertension/asthma
14.4 first symptoms -> isolation, partner worked in care home “a characteristic of this virus that causes oxygen
21.4 1st NHS call saturation levels of some sufferers to fall to
23.4 2nd NHS call Terrible cough, joint pains
24.4 3rd NHS call asked if he was breathless & if he could walk upstairs dangerously low levels without them suffering
24.4 partner was admitted with hypoxia via ambulance conspicuous difficulties when breathing.”
28.4 He died
The battle for lives will be won in the community
It is GPs, paramedics & ED staff who will shift the
balance & save most lives.
It will be clear, sound triage systems & clear clinical
guidelines that will determine mortality more than
the total number of ventilators available”
@home to self-monitor & self-escalate
in early deterioration
Matt Inada-Kim, Consultant Acute physician, HHFT, Clinical Director Patient Safety/Digital, Wessex AHSN
National Clinical Director Infection & Deterioration, Chair COVID pathways, NHS England & Improvement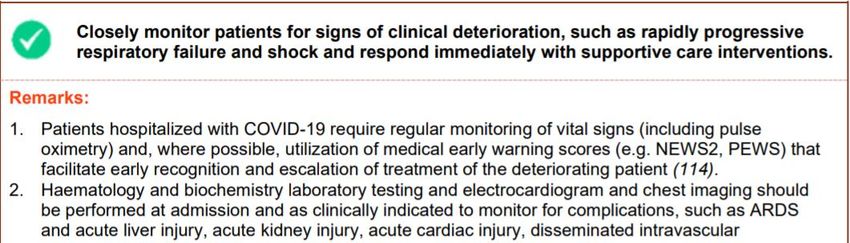
COVID Oximetry@home WHAT? COVID Virtual Ward
Primary care, Care homes, community health services ED/ Inpatient supported Discharge
INCLUSION CRITERIA
CLINICAL CONCERN / JUDGEMENT
1. Diagnosis of COVID-19: either clinically or positive test result
AND
2. Symptomatic AND
3. Aged 65 years or older OR for patients under 65 years at risk of a
poor outcome (CEV, LeD, BAME, obesity, SMI)
COVID OXIMETRY@HOME / VIRTUAL WARD
Care Home/GP/ED/SDEC issues COVID oximetry Diary (incl. admission/CPR status)
Patient Self-Monitoring – TDS diarising of Symptoms & Trend of O2 saturations
Patients Self-escalate if worsening of symptoms/saturations
Follow up call At Day 14 (when recovery is expected)
• Check up symptoms/saturations
• Reminder to return oximeter/diary
HOW ? COVID Diary
210k +/- 150k
Safety netting Pt instruction
Multilingual translations
COVID virtual ward apps https://www.youtube.com/watch?v=ifnYjD4IKus&feature=youtu.b
e
Interoperable
digital
systems
COVID virtual ward resources
https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2020/06/C0445-remote-monitoring-in-primary-care-annex-2-diary.pdf
Aligned national pathways across all settings Low Acuity/Community pt- COVID Oximetry@home, High Acuity non-admitted patients are ‘placed’ on the COVID virtual ward
Dr Caroline O’Keeffe Clinical Lead for Urgent and Emergency Care North Hampshire CCG @carolineokeeffe
COVID Oximetry at Home (CO@h)
• 6 PCNs / 230,000 patients • Referral Pathway
• Email
• Phone Line in hours / 111 OOH
• Co-located
• Winter Assessment Centre
• Opened 2.11.2020 • IT Solution
• Entered into ward on EMIS or by phone/email
• AccuRx – COVID Monitoring Florey
• Single integrated platform 24/7
• Automated texts daily for 14d asking about
symptoms and observations
• Staffing • Single CO@h spreadsheet – shared on Teams
• Lead ANPs • InHealthcare – 12th January 2021 (10w)
• Care Coordinator
• Monitoring
• Pulse Oximeter pack • CO@h Lead ANP oversees
• Instructions • Checks data, identifies deterioration and acts
• Link to YouTube video • Digital exclusion – paper diary and phone
• Paper diary – TDS readings
• Return envelope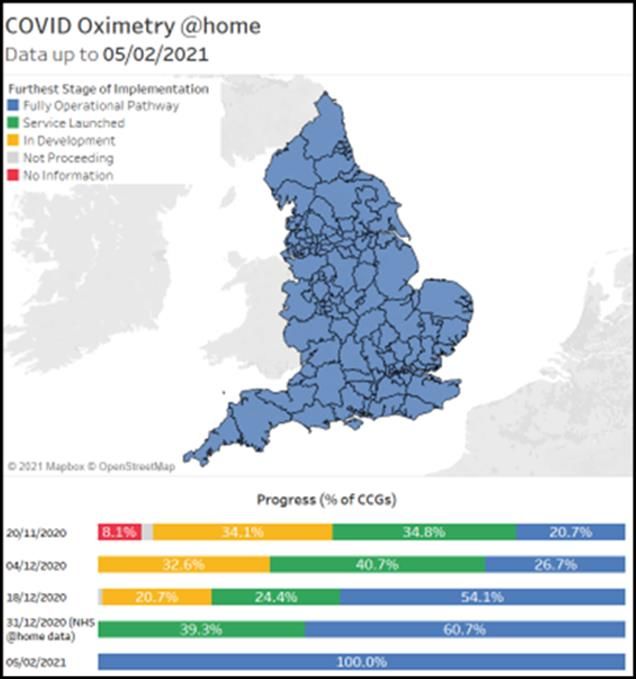
COVID in North Hampshire – current situation
• Started 2nd November - operating 15 weeks
• Total seen at Winter Assessment Hub – 2710
• RED admissions to hospital - 134
• AMBER assessments in hospital - 92
• GREEN – managed at home - 2483
• COVID Oximetry at Home
• Onboarded – 695
• Active – 101 (91 remain active at home, 10 in care homes)
• Discharged – 594
• Early detection – admissions 101 (19 deaths)
• Testing
• Total of 1157 rapid tests
• 124 new positive cases (case positivity 10.7%)
Lessons learned and next steps
• InHealthcare Platform
• Care Home Outbreaks
• ReSPECT forms for all Care Homes
• Cohort becoming younger – impact of vaccine
• Discharges – first 100 – 18% >80
• Discharges – last 100 – 4% >80
• MDT – PCN/OneTeam
• Strengthen links with practices
• Palliative Care/H@H input
• Increased capacity from PCN ARRS
• Care Coordinators / Health and Wellbeing coaches
• Social Prescribers
• Active Case Finding
• Review to identify all positives, safety net low risk
• Refer high risk positive cases to CO@h
• Secondary Care Virtual Wards
• SDEC/Telemedicine
• Communication and clear responsibilitiesPatient feedback – 130 respondents
https://vimeo.com/486820611t BBC South Today, 3 December 2020
Tara Sood Emergency Medicine Consultant Royal Free London NHS Foundation Trust @TaraSood5
The Virtual Ward Supporting
SDEC During
The Pandemic and Beyond
Dr Tara Sood
Consultant Emergency Medicine
National Clinical Lead Same Day Emergency Care NHSEI
NHS England and NHS ImprovementKey differences between COVID
Oximetry@home and COVID Virtual Wards
COVID Oximetry @home COVID virtual ward
(led by Primary Care) (led by Secondary Care)
WHERE Primary care supervised Hospital supervised
WHO Lower acuity / complexity Higher acuity / complexity
WHEN community diagnosed patients emergency hospital patients
AIMS Safe Admission Alternative Safe Admission Alternative
Early supported hospital discharge
HOW Patient self-monitoring/escalation More intensive monitoring
Earlier deterioration presentation Reliable deterioration recognition
WHAT Supportive treatments +/- Dexamethasone, LMWH, O2Investigation Treatment Management Patient presents in an Emergency SAME DAY Without requirement for admission to a hospital bed Virtual Ward /Oximetry@Home
Virtual Wards Supporting SDEC Delivery
Access to rapid diagnostics
and investigation
Hospital based services
without admission
Ongoing monitoring for
deterioration
Innovative Technology
Locally designed services
locally deliveredCOVID-19 / Non COVID-19 SDEC Pathways
NHS 111
RED SDEC* / COVID
Primary Virtual Ward
Care
Clinical
Conversation Yes
Community *SDEC Red
COVID – 19 highly patients/ individuals who
Services /
suspected have or likely to have
Care homes
COVID-19.
N
o **SDEC Amber
Outpatients patients/individuals who
have no symptoms of
COVID-19 but do not have
Self a COVID-19 SARS- CoV-
Referral Emergency
Department 2 PCR test result.
Ambulance
Services AMBER SDEC**Emergency Department guidance for referral in to COVID Oximetry @ home
or Virtual Ward
Clinical assessment with pulse oximetry on air and exertion testing*
Sats ≥ 95% Sats 93-94% with < 3% desaturation on exertion* Sats < 93%
and < 3% desaturation on
OR ≥ 95% with ≥ 3% desaturation on exertion* OR 93-94% with ≥ 3% desaturation on
exertion* exertion*
NEWS2, CXR, bloods and senior review
YES
Additional risk factors,
clinical concern or NEWS2 ≥ 3
NO
CONSIDER DISCHARGE
consider GP led COVID consider referral to hospital led Consider admission
oximetry@home COVID virtual ward
Lower acuity Higher acuity
Lower clinical concern Higher clinical concernSupported Discharge
22 | With thanks to Dr Simon
BrillKey enablers for implementation
Ready supply of probes – each acute trust has 300 assigned from NHSE
Protocols and SOPs - these are easily and readily shared between sites that are
already up and running
Empowered staff – great for training, fast learning curve and can use shielding /
pregnant staff
Senior Executive and operational support
Money ….not as much as you think, can be done with paper and a pen, fancy
apps not required
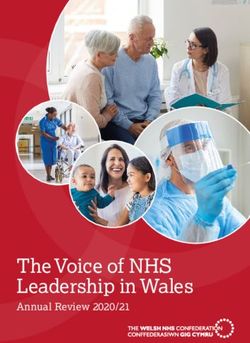
23 |Medical Admissions 24 |
Impact of Virtual Ward
COVID POSITIVE ADMISSIONS
60
medicaMedical Admission
50
Virtual Ward
40
Number admitted
30
20
10
0
02-Mar 02-Apr 02-May 02-Jun 02-Jul 02-Aug 02-Sep 02-Oct 02-Nov 02-Dec 02-Jan
25 |Future State Same Day Emergency Care
NHS 111
Primary
Care
Clinical
Conversation
Community
Services /
Care
Homes
SDEC Virtual Ward
Outpatients
Self
Referral Emergency
Department
Ambulance
ServicesDr Alison Tavaré GP and Clinical Lead West of England AHSN Regional Clinical Lead COVID Oximetry @home @Alison.Tavare
Care homes: building on good practice https://www.bgs.org.uk/resources/covid-19-managing-the-covid-19-pandemic-in-care-homes https://www.youtube.com/playlist?list=PLrVQaAxyJE3cJ1fB9K2poc9pXn7b9WcQg RESTORE2 and videos to improve communication What matters conversations: https://www.whatmattersconversations.org/videos End of life and treatment escalation planning: https://www.resus.org.uk/respect
https://portal.e-lfh.org.uk/LearningContent/LaunchForGuestAccess/684697
https://portal.e-lfh.org.uk/LearningContent/LaunchForGuestAccess/684697
Learning disabilities
Estimated more than six times more likely
to die from COVID (PHE Nov 2020)
• Younger age group than general population
• People with Downs at particular risk
• Co-morbidities
Why?
• Could this be linked to underlying conditions e.g. respiratory
problems?
• Diagnostic overshadowing
• communication e.g. accessing NHS111
https://assets.publishing.service.gov.uk/government/uploads
/system/uploads/attachment_data/file/933612/COVID-19__
learning_disabilities_mortality_report.pdfLearning disabilities
Sharing Easy Read information on COVID-19
Recommendations CO@H should be 'offered' from
to people with Downs and considered for others
with a learning disability
Reasonable adjustments: consider making more
frequent calls and not using apps. May need to
speak to clinician
Training for families and carers NHSE
https://www.events.england.nhs.uk/identifying-
early-signs-of-worsening-health-in-a-person-with-a-
learning-disability
https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2020/06/Pulse-Oximeter-Easy-Read-final-online-v4.pdfPatient Safety Collaboratives
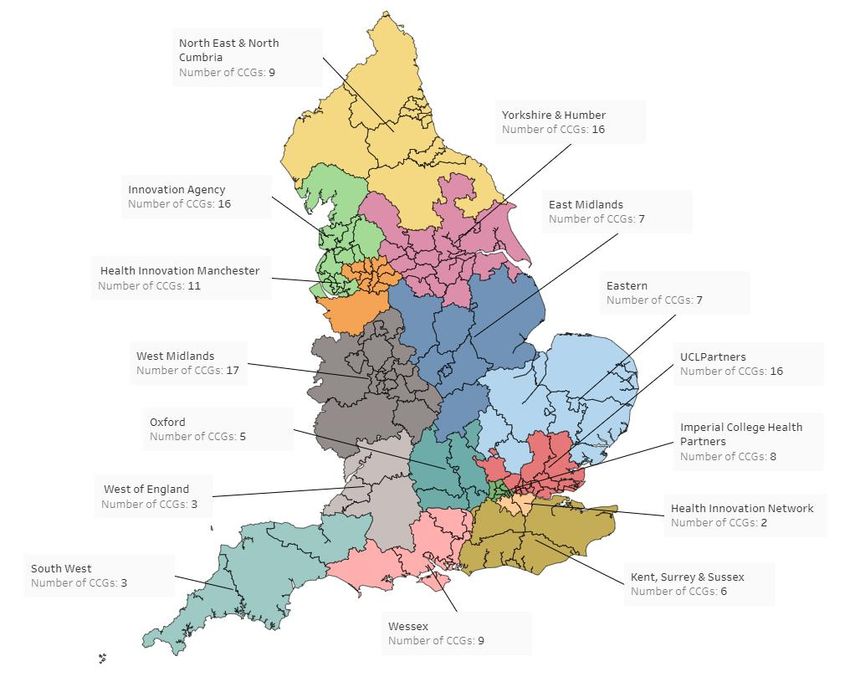
AHSN Lead Email
East Midlands Eddie Alder eddie.alder@nottingham.ac.uk
Eastern Caroline Angel caroline.angel@eahsn.org
Greater Manchester Jay Hamilton jay.hamilton@healthinnovation
manchester.com
Health Innovation Network Catherine Dale catherine.dale3@nhs.net
Imperial College Kenny Ajayi Kenny.Ajayi@imperialcollege
healthpartners.com
Kent Surrey & Sussex Ursula Clarke ursula.clarke@nhs.net
North East and North Tony Roberts T.roberts@nhs.net
Cumbria
Innovation Agency (NWC) Andrew Cooper andrew.cooper@innovation
agencynwc.nhs.uk
Oxford Katherine Edwards katherine.edwards@
oxfordahsn.org
South West Rebecca Whitting rebecca.whitting@swahsn.com
UCL Partners Valentina Karas valentina.karas@uclpartners.com
Wessex Kathy Wallis Kathy.Wallis@wessexahsn.net
West Midlands Jodie Mazur jodie.mazur@wmahsn.org
West of England Kevin Hunter kevin.hunter@weahsn.net
www.ahsnnetwork.com/about-academic-health-science-networks/patient-safety Yorkshire and Humber Mel Johnson melanie.johnson@yhia.nhs.ukResources AHSN Patient Safety Collaboratives National network of 15 PSCs working in NHSE/I regions: www.ahsnnetwork.com/covid-oximetry-home FutureNHS collaboration platform NHS@home: National guidance and information Specific care homes patient diary National Deterioration Forum: Collated resources specifically for care homes CO@h toolkit Monthly national learning network meetings Discussion forum
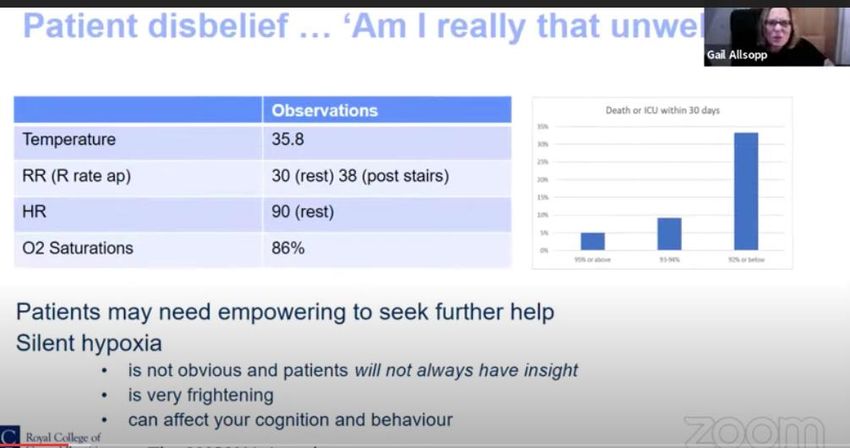
Silent hypoxia
Physiological Value
parameter
Resp rate 30 at rest 3
Oxygen sats on air 86% 3
(scale1)
Blood pressure Not noted 0
Pulse rate 90 (usual 58) 0
Level of Subtle reduction 3
consciousness cognition
Temperature 35.8 1
Incomplete NEWS2 of 9Sharing information on pulse oximetry https://www.youtube.com/watch?v=tWlv2V-MJU8
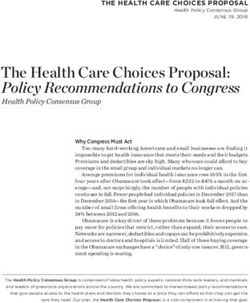
NHS COVID Oximetry@home & virtual ward
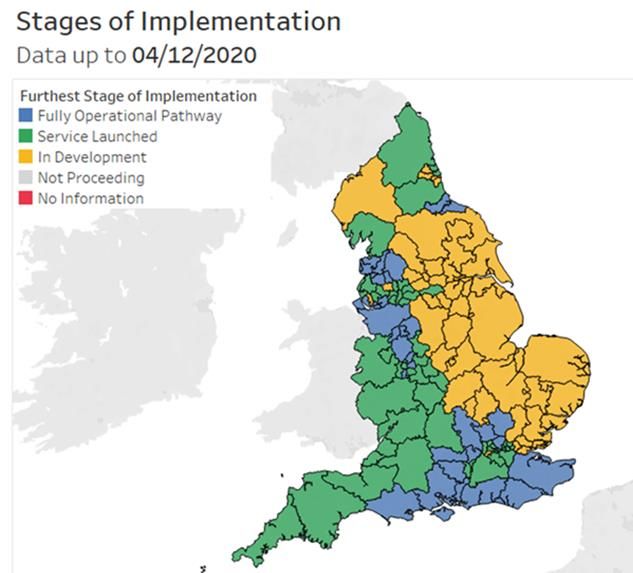
Principles National implementation
Empowering patients to Self-monitor & Escalate Aligned Pathways
Safely avoid unnecessary hospital admissions Hospital
Community Ambulance
Earlier escalation in deterioration
Safe Discharge Inclusion criteria
Home oxygen sats 30 day Clinical Judgement
Outcome data (2000 patients/5 sites) mortality/ICU And other High-Risk patients
14.4% case fatality rate →1% > 94% 93-94% e.g. Age>64, Male, BAME, obesity, Immunosuppression (cancer, transplant)
20% reduction in admissions
33 IHD, Diabetes ,deprived, Resp.illness, Cancer, liver disease
< 93% %
30d…
Shared decision making
9.8
0% COVID VIRTUAL WARD
5% Daily check in calls (or at clinical discretion)
Patient education & Empowerment
Patient Self-Monitoring – diarising of Symptoms & Trends of O2
saturations
Patients Self-escalate if worsening of symptoms/saturations *70 DAYS
Royal Berks NHS Foundation Trust Patient may be suitable for home dexamethasone, LMWH, oxygen
Weekly referrals to CVW Oct-Jan
Patient/Carers Community of
700k oximeters* practice/forum/webinars
Safety netting* National policy
Videos/animations Implementation in all 15 regions
Data/measurement/evaluation
Healthcare professionals
Apps/tech
Aligned national pathways*
Webinars, learning events*
Data/measurement
Follow-up by AHPs/HCPs under
supervision of clinicians
RECOVERY LONG COVIDhttps://www.who.int/publications/i/i tem/WHO-2019-nCoV-clinical-2021-1
Thank you @ universal national rollout of COVID oximetry
Past, present & future
Pursuit of integrated care opportunitiesA Massive Thanks to the COVID Oximetry at home team
More information • Visit: https://www.ahsnnetwork.com/covid-oximetry • Download Patient safety in partnership: Our plan for a safer future 2019-2025: one year on at www.ahsnnetwork.com/psplan • Read our report: Safer care during COVID-19 at www.ahsnnetwork.com/patient-safety-covid19-report • Follow us: @AHSNNetwork
You can also read