Creatine & Rugby : Effect on Body Composition - FAT MASS LEAN TISSUE MASS - SINSEB
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Creatine & Rugby : Effect on Body
Composition
FAT MASS LEAN TISSUE MASS
CREATINE: 0,1 g/kg CRE + 0,7 g/kg CHO x 8 wks
PLACEBO: 0,8 g/kg CHO x 8 wks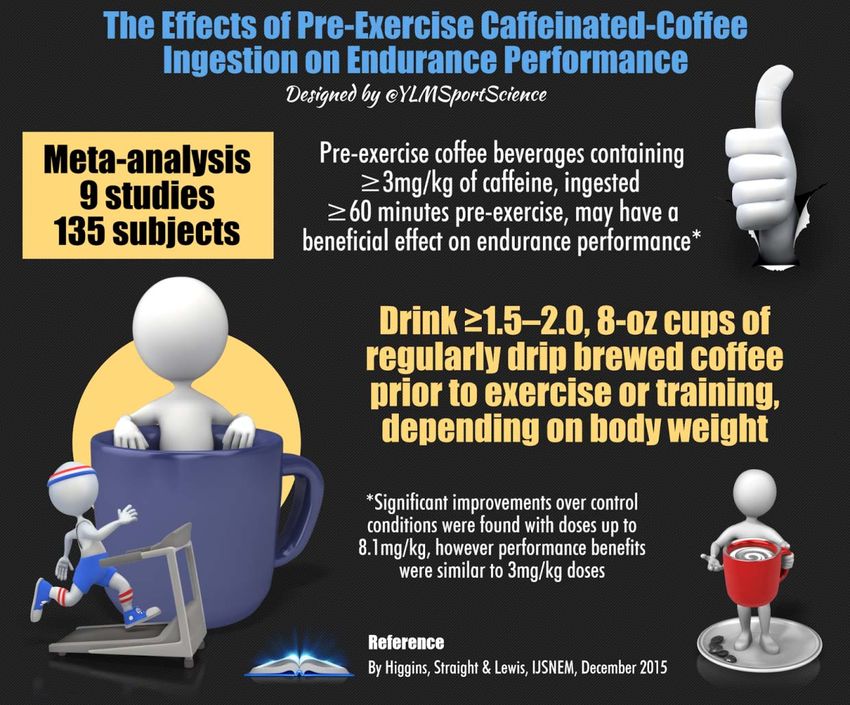
Winter Break ‐ Intervention
Team A Team B
Different Trends
Dic vs Nov
Dic vs Nov
Creatine No Intervention
β‐Alanina
Beta alanina è un efficace tampone di
idrogenioni aumentanto il contenuto di
carnosina muscolare
4-6 g/d di beta-alanine possono influenzare :
Esercizio Acuto
Riduce Fatica
Aumenta la potenza
Aumenta capacità di resistenza
Allenamento
Incrementa Forza
Incrementa Massa Magra
Incrementa il Volume d’ Allenamento
Hill et al., Stout et al., Hoffman et al., Van Thienen et al.
75
OMEGA-3
(APPLICAZIONE NELLO SPORT)
Controllo della
risposta
infiammatoria Effetto anabolico
‐ Dolore ‐ Mantenimento PKB‐
‐ rimodellamento mTOR
tissutale
‐ riparo e Anticatabolico
recupero EPA/DHA ‐ Modulazione
(OLIO DI PESCE) proteolitica
Sistema di supporto
multiorgano
‐ cardio/vasoportettivo Metabolismo/Wellness
‐ cervello/umore ‐ Sensibilità
‐ neuroprotezione insulinemica
‐ muscolo scheletrico/ ‐ Composizione
ortopedia corporea
Ω‐3 & INTERACTIONS WITH THE ADIPOSE ORGAN

CAFFEINE
«We Can Conclude that 3 Mounths of Gannoderma
and Cordyceps Supplementation may protect
endurance athletes from nonfunctional effects of
overreaching/overtraining ….»
Placebo
Ganoderma and
Cordyceps
Supplementation
DHPPSUCCO DI BARBABIETOLA
MECCANISMO DI AZIONE
82
Jones AM. Sports Med. 2014 May;44 Suppl 1:S35-45Tempo di esaurimento esercizio massimale
83BETAINE
84
Cholewa JM et al. . Amino Acids. 2014 Aug;46(8):1785-93.Figure 1. [A] Oxy and dROMs test data in plasma; [B] T/C ratio in plasma; [C] T/C ratio in saliva
Subjects
● Soccer top team of the Italian Soccer Serie A
Methods A B C
● Seasonal observations
● D‐ROMs Test (plasma)
● OXY Adsorbent Test (plasma)
● T/C Ratio (plasma and saliva)
Results
● No correlation between TAC and d‐ROMs
● Correlation between T/C data both in plasma and saliva Figure 2: in saliva [A] T/C Jul vs Oct; [B] T/C Jul vs Jan; [C] T/C Jul vs Apr
● Correlation between T/C data both in plasma and saliva
A B C
with d‐ROMs A B C
Conclusion
● d‐ROMs is the best marker for oxidative stress
● Saliva can be used as an alternative non invasive method
to evaluate hormonal levels.
Accepted for a poster presentation at the
upcoming international conference for the
International Society of Sports Nutrition (ISSN)
to be held on June 23th – 25th 2010 in Las
Vegas, NV (USA).TESTOSTERONE
Salivary test Analysis
348,0
176,0
132,0
81,0
16/7 24/10 29/1 22/4
13,1 11,5
7,9
CORTISOLO
6,9
16/7 24/10 29/1 22/4
26,6
19,1
15,3
10,3
T/C
16/7 24/10 29/1 22/4
117,8
47,1 55
IgA
33,5
16/7 24/10 29/1 22/4Hindawi Publishing Corporation
Relationship between International Journal of
Endocrinology. Volume 2014,
Article ID 525249, 9 pages
Testosterone and Magnesium
antioxidant capacity and the control of
oxidative stress
Inadequate intracellular magnesium may
reduce the mitochondrial efficiency and
The change in magnesium levels inside the biological serum increase the production of ROS
concentration range could lead to an enhancement of the Bio‐T.
The activity of anabolic hormones, where T plays a central role, is influenced by
mineral status (magnesium), along with caloric and protein intake
The systemic inflammation, which negatively influences magnesium and T and is in turn down
regulated by these 2 factors.Relationship between Testosterone and Zinc Zinc enhances human chorionic gonadotropin‐induced production of cAMP and consequently testosterone in rat testes. Nishi Y, Hatano S, Aihara K et al (1984) Effect of zinc ion on human chorionic gonadotropin stimulated in vitro production of cAMP and testosterone by rat testis. Pediatr Res 18:232 Zinc may increase the conversion of androstenedione to testosterone in the periphery tissue. Bermudez JA, Perex‐Pasten E, Villalpando S et al (1986) Low plasma zinc and androgen in insulin dependent diabetes mellitus. Arch Androl 16(2):151 Zinc interferes with the metabolism of testosterone by decreasing its hepatic clearance and reducing hepatic 5 alpha‐reductase activities. Grumbach MM, Coute FA (1992) Disorders of sex in differentiation. In: Wilson JD, Foster WD (eds) Williams textbook of endocrinology, 8th edn. WB Saunders Co, Philadelphia, p 853
Probiotici Martarelli, D., Verdenelli, M. C., Scuri, et al. 2011 Investigazione dell’efficienza di L. rhamnosus in combinazione con L. paracase • dosaggio 2x109CFU/die x 4 weeks • Variazioni immunitarie e forte aumento livelli plasmatici antiossidanti, • Limite: il gruppo di controllo non ha consumato nessun integratore ( no effetto placebo) Athletes and all those exposed to oxidative stress may benefit from the ability of these probiotics to increase antioxidant levels and neutralize the effects of reactive oxygen species
VITAMINA D E BENEFICI NELLO SPORT
Multiple musculoskeletal benefits with
increases of:
- Muscle protein syntesis,
- ATP concentration,
- strength,
- jump height,
- jump velocity,
- Jump power,
- exercise capacity,
- physical performance
Additionally increased levels of
vitamin D decrease muscle protein
degeneration and reverse myalgias
Shuler, Franklin D., et al. "Sports Health Benefits of Vitamin D." Sports
Health: A Multidisciplinary Approach - (2012)Objective and Subjects
● To examine the vitamin D shortage and BMC
variations in Italian Serie A elite male soccer playe
Results
● 25(OH)D3 significantly decreased from autumn to
winter (P0.05).
● Significance reduction (p• A repeated‐measures design was implemented in which 46 elite
professional European athletes were block randomized based on
their basal 25[OH]D concentration into two treatment groups.
• Athletes received either 35,000 or 70,000 IUIwkj1 vitamin D3 for
12 wk, and 42 athletes completed the trial.
• Blood samples were collected for 18 wk to monitor the response
to supplementation and withdrawal from supplementation.SPORT INJURIES
Ossa, Tendini e Legamenti
Vitamina D: Predisposizione Infortunio
Soggetti E Metodi
• 89 giocatori (58 di colore)
• Età 25,0 ± 2,6 anni (21‐32)
• Valutazione pre‐stagionale
100%
White Black ○ Not Injured ● Injured
19,1% Normal (>32 ng/ml) 40 50
25(OH) D (ng/mL)
25(OH)D (ng/mL)
30 40
50,6% Insufficiency (20‐31,9 30
50%
ng/mL) 20 24,7
20 19,9
Deficient (VItD3 4000 – 5000 UI/die
Nutrients 2013, 5, 1856‐1868;
• Vitamin D is established as a major factor in preventing
stress factors and optimizing bone health, both of which
are of great importance to the athlete
• Rates of Vitamin D insufficiency in athletes vary among
studies, but most researchers agree that athletes should
be evaluated regarding vitamin D status and given intake
recommendations to maintain optimal 25(OH)D levels >40
ng/mL.
• Not only does Vitamin D assist in growth and maintenance
of the bone, but it also aids in regulation of electrolyte
metabolism, protein synthesis, gene expression, and
immune function
“Without vitamin D, the ability of the cell to respond adequately to pathologic and physiologic signals is impaired”
Heaney, R.P. Vitamin D in health and disease. Clin. J. Am. Soc. Nephrol. 2008, 3, 1535–1541.TAKE HOME MESSAGE
• La Nutrizione dello Sport ha avuto nel Tempo varie «Tendenze / Evoluzioni» passando da
Diete Iperglucidiche e povere in Proteine e Grassi a Diete Iperlipidiche e/o Iperproteiche
• Grande attenzione andrà posta all’Idratazione seguendo anche in criteri di
personalizzazione e giusto equilibrio tra zuccheri e Sali minerali durante l’attività
escludendo totalmente bevande contenti alcol prima ma anche dopo l’esercizio
• Non esiste la Dieta che fa vincere una Gara ma si deve «tendere» sempre di più ad una
«Personalizzazione» dello Schema Nutrizionale basandosi su vari aspetti dal Gusto , alla
Stagionalità dell’alimento ma soprattutto adattando lo Schema al Trainig / Competizione in
atto
• L’utilizzo dei Supplementi e dei Nutraceutici è utile ma deve essere basato su una attenta
valutazione dell’obiettivo da raggiungere (Valutazione antropometrica ematochimica e/o
ormonale dell’atleta) e basato su evidenze scientifiche
102Dr. Mario Angelini – Clinica Chirurgica Università di Pisa ‐ 1936
You can also read