Critical Observations on the Neurotoxicity of Silver
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Critical Reviews in Toxicology, 37:237–250, 2007
Copyright c Informa Healthcare
ISSN: 1040-8444 print / 1547-6898 online
DOI: 10.1080/10408440601177665
Critical Observations on the Neurotoxicity of Silver
A. B. G. Lansdown
Investigative Sciences, Imperial College, Faculty of Medicine, London, United Kingdom
Silver is a xenobiotic element with no recognized trace metal value in the human body. It
is absorbed into the body through the lungs, gastrointestinal tract, mucus membranes of the
urinogenital tract, and through the skin, mainly in the form of silver protein complexes. Although
silver is metabolized throughout the soft tissues, available evidence from experimental animal
studies and human clinical reports has failed to unequivocally establish that it enters tissues
of the central nervous system or is a cause of neurotoxic damage. Argyria characterized by
deposition of particles of silver sulfide or silver selenide is the principle contraindication for
using silver in medical devices or occupationally. This presents discoloration of the skin but is
not regarded as a health risk or manifestation of toxicity. No evidence is available to demonstrate
the toxic risk of silver to the peripheral nervous system, although silver sulfide deposits have
been identified in the region of cutaneous nerves. Transitory silver sulfide deposits seen in the
tissues of the blood–brain and blood–CSF barriers are mostly lysosomally bound or deposited
on basement membranes or collagen without toxic effect. Silver is mostly excreted from the
body in the urine and feces. Further research is indicated to evaluate the role of metal binding
proteins including metallothioneins as cytoprotectants for neurological tissue.
Keywords Argyria, Blood Brain Barrier, Brain, Central Nervous System, Medical Devices, Silver
Silver is widely distributed in the earth’s crust and is found in sulfadiazine, and other silver compounds incorporated in the
soil, fresh and sea water, and the air. It is readily absorbed into various devices, and its lethal effect on pathogenic organisms.
the human body with food and drink and through inhalation, but Experience has shown that a large proportion of the silver ion
the low levels of silver commonly present in the bloodstream released from medical devices not required for antimicrobial
(238 A. B. G. LANSDOWN
sulfide or silver selenide. The resulting slate grey discoloration TABLE 1
of the skin occasionally associated with melanogenic changes, is General characteristics of neurotoxic materials
semipermanent and cosmetically undesirable but is not known
to be life-threatening.13 Fung and Bowen reported that up to 1. Penetrate the blood brain barriers and the blood
10% of silver salts ingested may be deposited in soft tissues, cerebrospinal fluid barrier to enter tissues of the central
with highest concentrations in skin, liver, spleen, and adrenal nervous system.
glands, with lesser levels in muscle and brain.9 The clinical im- 2. Exhibit a predilection for specific cell or tissue types
plications of argyria are discussed extensively in the literature (neurons, glial cells).
and there is evidence that in severe cases, silver deposited in 3. Impair essential metabolic pathways in target cells leading
the central nervous system “may be a cause” of neuromuscular to functional disturbances and/or progressive degenerative
dysfunction and behavioral abnormality.15−19 This has not been and changes resulting in cell death.
unequivocally substantiated clinically or experimentally. 4. The severity of responses seen show a direct correlation
William Roper in 1990 comprehensively reviewed the toxi- with the amount of toxin present and the duration of its
cology of silver for the U.S .Public Health Service and discussed action.
clinical and experimental studies associating silver deposition
in the brain and neurological tissue and its propensity to cause
injury.20 He indicated that published reports available then were serve as enzyme cofactors, transcriptional factors, or modulators
not only inconclusive but failed to demonstrate clear causal rela- of gene expression. This last group of metals may exert patho-
tionships between silver deposition and tissue damage. He rec- physiological changes if present in supra-optimal quantities.2
ommended that specific behavioral tests might be beneficial in The position of silver as a neurotoxic metal is equivocal and un-
defining the neurotoxic hazards of silver exposure and the vul- clear at the moment.29 An early experimental study in tadpoles
nerability of the central nervous system to injury. Surprisingly, implicated silver nitrate as a cause of “white matter edema,” with
although analytical procedures for silver have become increas- water-filled vacuoles developing between extracellular mem-
ingly more sensitive in recent years and accurate methods of x- brane surfaces of myelin lamelli,30−32 but this has not been ob-
ray microanalysis, histochemistry, and autometallography have served in mammals.
been developed for visualising silver deposits in tissues,21,22 no
such reports have been published as far as I am aware.13,23 Such BLOOD–BRAIN BARRIERS
an appraisal is highly relevant now in view of the greatly in- The blood–brain barriers (BBB) perform a central role
creased use of silver in medical devices, major technological in maintaining chemical homeostasis within the central ner-
advances in materials science, and the widespread applications vous system.33,34 By modulating the uptake of nutrients and
of nanotechnology in medicine.24,25 The minute silver particles electrolytes from the circulation and regulating the egression
produced by nanotechnology in wound dressings (Acticoat) and of metabolites, they control brain chemistry and limit minor
in in-dwelling catheters permit considerably greater levels of changes, which may be expressed in terms of learning difficul-
ionization and biological reactivity than previously shown with ties, memory loss, and behavioral dysfunction.
silver metal foil or many soluble silver salts, and are expected to This research illustrates how chemically induced defects in
achieve higher levels of antimicrobial activity and bioreactivity the BBB may be a cause of edema, aberrant brain development
within the human body.26 The present critical review was con- and neurodegeneration.27,28,31 Zheng demonstrated that BBB
ducted to analyze experimental and clinical reports purporting have special significance in regulating the uptake and neuro-
to show neurotoxic effects attributable to silver absorption, and toxic action of metals and exhibit a limited capacity to metabo-
to identify circumstances under which they might occur in pa- lize certain lipophilic materials that influence carrier-mediated
tients fitted with a medical device with silver antibiotic content processes.33 The neurotoxicity of metals and other xenobiotic
or coating. materials is largely determined by the protective efficiency of
the BBB in different regions of the central nervous system.27,34
NEUROTOXICITY OF METALS An understanding of the critical role of the BBB is essential
Metals differ greatly in their transport mechanisms in the hu- in appreciating the putative neurotoxic action of silver and the
man body and their accumulation in the central nervous system. increased vulnerability of certain areas of the brain to injury.
Acknowledged neurotoxic metals differ greatly in their ability The BBB is a complex system comprising the interface be-
to penetrate into soft tissues and their mechanisms of action and tween the blood and the brain, and that separating the blood and
pathogenicity, but share the characteristics listed in Table 1.27,28 cerebrospinal fluid (CSF).28,34,35 Endothelial cells lining the ex-
At least nine metals are known to penetrate into neurological tensive vascular network of the brain and subarachnoid space
tissues,29 including the toxic metals lead, cadmium, and mer- provide a major component of the BBB, whereas the blood–CSF
cury, with no known trace metal value. Sodium, potassium, cal- barrier resides largely in the choroid plexus and in the ependy-
cium, iron, copper, zinc, manganese, cobalt, and molybdenum mal cells lining the cavity of the CSF. Peripheral nerves have
perform essential physiological functions in the human body or analogous barrier systems comprising the vascular network andNEUROTOXICITY OF SILVER 239
TABLE 2
Classification of metal ions according to their toxic action on the choroid plexus
1. General toxicants Metals that accumulate within the tissues of the plexus and Mercury, arsenic, and cadmium
cause substantial structural and functional damage
2. Selective toxicants Metals that do not alter the permeability of the choroid plexus Lead, manganese, copper, and
or evoke significant pathophysiological changes, but tellurium
influence critical regulatory functions as a prelude to
neurological damage.
3. Sequestered toxicants Metals that are sequestered by the choroid plexus as an integral Silver, gold, zinc, and iron
part of its neuroprotective role
connective tissues of the endoneurium and the perineurium sur- the neurotoxic action of silver.29 The blood flow in the choroid
rounding nerves and nerve bundles, respectively. In humans, the plexus is high and exposes it to a greater influx of toxic materials
BBB is established at birth but in the choroid plexus and circum- and efflux of metabolites than elsewhere in the brain.34
ventricular organs (median eminence, subfornical organ, area Ependymal cells lining the CSF surface are densely packed
postrema and neurohypophysis) it becomes less well developed. with tight junctions providing a modest barrier to the transfer of
The endothelial cells lining vascular channels are of a fenestrated metal ions. In contrast, the fenestrated endothelial cells lining
type even though they maintain tight gap junctions.27 Variations choroidal capillaries are more porous or “leaky,” thereby per-
in the permeability of the BBB according to age and the region mitting greater exchange of solutes and metal ions between the
of the brain implies that that certain areas of the brain are more blood and connective-tissue matrix.34.39 The ependymal cells
vulnerable to metal-induced injury than others.34,35 In the rat, regulate the production and composition of the CSF including
the structure of the BBB and its relationship to surrounding as- the interchange of metal ions, but their mechanisms of action,
trocytes has been investigated using a silver–protein complex possibly involving sodium and potassium ATP-ase pump mech-
as a marker.36 This has demonstrated that the subfornical organ anisms, are imperfectly understood. Transport through the BBB
is largely devoid of BBB and that micro-vessels are separated is limited to nonpolar substances and several nutrients for which
from surrounding astrocytes only by a basement membrane. special carrier-mediated pathways exist.27 Experimental stud-
Early evidence of the protective role of the BBB in con- ies have demonstrated the ability of the connective tissue of the
trolling the penetration of xenobiotc materials was provided by choroid plexus to concentrate metal ions, including organic mer-
experiments in which the intravital dye trypan blue was injected cury, cadmium, arsenic, and lead, and regulate their penentration
intravenously into rabbits.37,38 The dye bound to plasma protein into the neural tissues to evoke pathological damage.42−44 Metal
was not absorbed into the tissues of the brain but sequestered ions may be conveniently classified according to their specific
and bound lysosomally in endothelial cells. It stained other soft action on the choroid plexus33 (Table 2).
tissues but was excluded from the brain unless injected intracere-
brally. These observations promoted the concept that the BBB
was unique to the central nervous system and acted in the form SILVER AND THE BLOOD–BRAIN BARRIER
of an “exclusionary interface” separating brain from blood. Ac- Silver-induced neurotoxicity is believed to be rare,33 even
cording to Rapoport, cerebral capillaries facilitate diffusion and though some experimental studies in the rat claim that sil-
regulate exchange of metabolites between blood and brain.34 ver ions do penetrate the BBB and the blood–placental bar-
The ependymal surfaces of the cerebral ventricles and the pia- rier to locate heterogeneously throughout the central nervous
glial surfaces of the brain do not impede transfer of substances system.21,22,42,43 Predictive experimental studies conducted in
between the cerebrospinal fluid and the brain and do not consti- animal models are expected to provide more accurate and re-
tute a subbarrier. producible information on the neurotropic action of silver than
Zheng studied the morphology of the blood–CSF barrier, with is possible with postmortem material obtained from patients dy-
particular reference to the role of the choroid plexus in modu- ing with argyria or supposed silver intoxication. Neurological
lating metal-induced neurotoxicities.29,33 The choroid plexus is tissues autolyse readily after death and visualization of sites
a highly vascular villous structure extending from the ventric- of silver deposition may be obscured. Electron microscopy has
ular surfaces of the brain into cerebral spinal fluid like coral been widely used in examining the deposition of silver in the
fronds.39,40 Although it represents less than 5% of total brain region of the brain and other tissues, but x-ray microanaly-
weight,41 it has a proportionately high surface area permitting sis and autometallography have been developed as a means
greater exposure to the circulating CSF. Compelling evidence of visualizing fine silver deposits in the choroid plexus, neu-
illustrates the critical role of the choroid plexus in sequester- rons, glial cells, and extraneural tissues of the BBBs.22,45−48
ing toxic heavy metals like lead and mercury, and may regulate Analysis of silver in “the brain” using 111 Ag tracer studies,240 A. B. G. LANSDOWN
atomic absorption spectrometry, and neutron-activation analysis argyria and chronic silver exposure are difficult to explain if
is insufficient to discriminate between silver deposited within silver had not penetrated the BBB.46 They administered silver
tissues of the brain and that contained within tissues of the nitrate or silver lactate to rats and mice orally or by intraperi-
BBB.49 toneal injection and employed autometallographic methods to
demonstrate silver penetration of the blood–brain barrier and its
Experimental Studies deposition in all parts of the central nervous system.46,59−63 An-
Early studies conducted in rats exposed chronically to silver imals given silver nitrate or silver lactate chronically in drinking
nitrate in drinking water failed to provide evidence that silver water (0.01%), or injected intraperitoneally with silver lactate
passes the BBB to accumulate in neural tissues of any part of (3–55 mg for up to 13 months) or a colloidal silver preparation
the central nervous system. Where silver nitrate was employed (Protagol (0.1–0.5 ml, 2–5 days) exhibited intracellular and ex-
as an intravital dye to demonstrate the integrity of the BBB in tracellular silver sulfide deposition throughout the brain, dorsal
the rat, silver was deposited preferentially in basal laminae and root ganglia, enteric ganglia, peripheral nervous system, anterior
perivascular spaces of the choroid plexus, hypophysis, pineal pituitary gland, and neural retina of the eye.64 These distribu-
body, area postrema, and subfornical organ.51−54 . It could not tion patterns were heterogeneous but particularly heavy in large
be identified outside circumventricular areas or around cerebral motor neurons and protoplasmic astrocytes. The silver granules
capillaries in severely argyric rats. Although silver is readily were bound specifically in secondary lysosomes.47 In keeping
metabolized from tissues like liver and kidney in humans,1 it with earlier observations,55 tissues of the BBBs were heavily
exhibited a longer half-life in endothelial cells of the BBB site stained with silver sulfide deposits but much silver was located
than in other soft tissues in the rat. Later more elaborate studies as extracellular deposits on basement membranes of cerebral
by Scott and Norman confirmed the inability of silver to cross blood vessels and on elastic fibers.43,47,48 The intensity of silver
the BBB and demonstrated fine electron-dense silver granules deposition in each case was proportional to the amount of silver
(10–15 nm diameter) in the basal laminae of arterioles of the administered and the duration of exposure, although subtle dif-
parietal cortex and subcortical white matter.55 Accumulation ferences were evident between administration of silver nitrate
in these sites “maximized” by 241 days and did not change in and silver lactate. Importantly, silver deposits were transitory
concentration or distribution up to 455 days after exposure. In in these locations and declined when silver treatment was with-
an attempt to increase the vulnerability of the brain to silver, drawn. Macrophages engorged with silver deposits have been
Scott and Norman induced surgical intracerebral stab wound consistently reported in the BBB. Interestingly, when silver was
injury.55 This had the effect of increasing silver accumulation injected into the lateral ventricles of the brain, it was absorbed
in the laminae of small blood vessels, tissue fragments of the into ependymal cells of the BBB, rather than locating in neurons
BBB, and associated macrophages, but deposits were not iden- or glial cells. Rungby and Danscher46 conceded that the paral-
tified within the brain parenchyma. They confirm earlier studies ysis reported in earlier studies in rats dosed with silver nitrate
demonstrating that silver protein complexes do not penetrate might be attributable to the toxic effects of silver accumulating
the gap junctions of cerebral endothelia, even though some sil- in capillaries associated with the central nervous system,46,65
ver might dissociate at cell membranes and penetrate cells by but gave no details.No specific neurobehavioral tests of the type
an undefined mechanism other than pinocytosis.36 Alternatively, promulgated by Roper20 were conducted.
silver ion bound strongly to collagen and glycoproteins of the Although Rungby and Danscher provided substantial evi-
BBB.56 dence based upon electron microscopy, photochemical and auto-
Two Russian studies (unseen) cited by the Joint FAO/WHO metallographic techniques that silver does cross the BBB to ac-
Expert Committee on Food Additives (1977) may provide evi- cumulate in specific locations in the central nervous system, they
dence of a direct toxic effect on silver in the brain.57,58 The first failed to associate this with frank neurological damage or behav-
claimed to show decreased brain RNA and DNA and dystrophic ioral changes.46,60,61 Thus, irrespective of route of administra-
changes in rats given 0.2% silver nitrate in drinking water for tion (oral or intravenous), silver accumulation in lysosomal vac-
12 months or 2.0% for 6 months, while in the second study uoles occurs in a dose-related fashion in neurons and glial cells
histopathological changes were reported in neuronal, glial, and of the olfactory lobes, cerebral cortex, hippocampus, substan-
vascular tissues of the encephalon and medulla of rabbits dosed tia innominata, and hypothalamus, but the thalamus, substantia
with 0.025 or 0.25 mg/kg silver (possibly by intravenous injec- nigra, and nuclei pontis seemed to be resistant. Neurons of the
tion), but further details are not available. globus pallidus, brainstem, spinal cord and basal root ganglia,
Evidence that silver penetrates the BBB and blood–placental cerebellum (deep nuclei), and the trigeminal nerve also showed
barrier relies heavily on a comprehensive series of anatomical, a strong tendency to concentrate silver. Silver deposits in the
histochemical, and electron-microscopical studies conducted rat hippocampus and in the peripheral nervous system remained
in rats at the University of Aarhus in Denmark. Rungby and stable for at least 45 days.60 The brains of young postnatal an-
Danscher considered that the symptomatic effects of paralysis, imals may be more vulnerable to the toxic effects of silver, as
loss of coordination, cerebella ataxia, convulsions, and elec- suggested by a significant reduction the pyramidal cell layer of
troencephalograph (EEG) changes seen in patients with severe the hippocampus.61 This may be an indication of a cytostaticNEUROTOXICITY OF SILVER 241
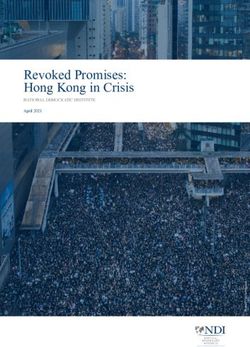
TABLE 3 in 8–12 weeks. It is unclear from this study to what extent the
Mean tissue silver concentration (ng/g wet wight) in mice silver released accumulated in the central nervous system or
given 0.03 mg/L silver nitrate to drink for 1 or 2 weeks67 whether it evoked behavioral or other pathological changes.
Tissue 1 week 2 weeks
CLINICAL OBSERVATIONS
Cerebellum 9.39 ± 1.90 7.45 ± 4.4.9 Evaluation and clinical definition of neurotoxic risks asso-
Cerebrum 2.46 ± 0.57 1.72 ± 0.48 ciated with occupational or environmental exposure to silver
M. soleus 23.63 ± 9.79 28.57 ± 15.35 are complicated by wide variations in patterns of exposure,
M. gastrocnemius 1.28 ± 0.41 1.55 ± 0.22 quantitative analysis of silver in blood and tissues, and scien-
Blood 0.97 ± 0.30 0.95 ± 0.27 tific detail presented. Clinical studies on silver nitrate and sil-
ver sulfadiazine in treating patients with severe burns injury
provide fundamental information on silver absorption and tis-
sue distribution, but accurate information on the accumulation
effect or other toxic effect of silver on developing hippocampal
or distribution in the central nervous system is still urgently
cells, but its implications on further development in the brain
required.1,12,70 Wan et al. critically examined methods available
and behavior patterns are unclear.
for quantifying silver in body tissues and fluids, and provided
Rungby and Danscher failed to identify frank toxic changes
useful “baseline” or control silver levels in key tissues of patients
in neurological tissues in rats exposed by various routes to silver
with no known exposure to silver occupationally or therapeuti-
nitrate, silver lactate, or Protargol, but they did report that mice
cally (Table 4).1 In their experience, flameless thermal atomic
exposed chronically to very low levels (0.015%) of silver nitrate
absorption spectrometry was far more accurate than older and
or silver lactate in drinking water became argyric and hypoac-
more commonly reported techniques including spectrophotom-
tive in open-field behavioral studies.66 If this species-specific
etry and flame atomic absorption.71−73 The levels of silver found
neurobehavioral change attributable to silver accumulation has
in the cerebral gray matter of patients not knowingly exposed to
a pathophysiological basis, the mechanism is unclear at present.
silver and analyzed by high-resolution spectroscopy have been
More recent work by Pelkonen et al. reports silver accumula-
given as 0.029 µg/g.17 More recent analyses of patients dying in
tion in the cerebellum and the soleus muscles of young adult
North America has shown the average silver content of tissues
mice given 0.03 ml/L silver nitrate to drink for 1–2 weeks, but
to be: skin 1.3 µg/g (range 0.8–2.5µg/g), liver 0.7–1.0 µg/g,
failed to show changes in behavioral activity or disturbed health
adrenal242 A. B. G. LANSDOWN
Light and electron-microscopic examination has demonstrated Silver Nitrate in Oral Hygiene
electron-dense granules of 30–100 nm in the skin and other tis- Silver nitrate and colloidal silver preparations have been used
sues; these granules are composed largely of silver sulfide with in the treatment of mucus membrane infections and infective
traces of selenium, mercury, titanium, and iron. The electron rhinitis for many years.83 Although not legally available now
microscope x-ray analyzer is capable of detecting silver sulfide in the United States and some other countries, colloidal silver
deposits in tissue at concentrations as low as 1 × 10−14 g/µm2 .76 is widely available in various forms for treating miscellaneous
In each case, the granules have been observed mostly within ailments. It is a common cause of argyria and has been impli-
secondary lysosomes of the basal lamina of the epidermis, small cated as a cause of neurological problems.84−87 In his Manual
dermal blood vessels, Schwann cells, basement membranes of of Pharmacology, Sollemann83 listed recommendations for the
eccrine glands, and dermal elastic and collagen fibers and not use of silver nitrate and colloidal silver for nose and throat in-
associated with pathological changes.14 Other clinical studies fections as 2–10% silver nitrate, 0.5–10% strong silver proteins
examining the chemical constitution of so-called “silver de- (Protargol), 10–30% sprays of mild silver proteins (Argyrol). In
posits” in brain, liver, and other tissues have confirmed these practice, it is almost impossible to calculate the amount of silver
observations.15,19,77,78 consumed in long-term therapies, and blood silver levels are a
The famous “blue man” of Barnum and Bailey’s Circus poor guide to silver absorption in the chronic consumption or in-
in 1927 is possibly the earliest recorded evidence of silver halation of over-the-counter silver products. Silver accumulates
in the brain, where an estimated total body silver content of in the blood initially but rapidly declines as some is excreted
90–100 g was associated with 0.011% in “the brain.”79 Silver in urine and feces and the balance is distributed to soft tissues
deposits were mainly associated with connective tissues and throughout the body.
macrophages. The reliability of these estimates might be ques- A recent case reported as the “silver man” concerned a
tioned on account of the accuracy of the analytical procedures 42-year-old patient with severe argyria resulting from chronic
available at the time. use of a silver protein-containing vasoconstrictor preparation
(Coldargan, SigmaPharm, Vienna) for treating allergic rhinitis.88
He consumed 10–20 ml weekly of Coldargen (drops containing
Environmental and Occupational Exposures 0.85 mg silver protein) and punch biopsies showed perivascular
Occupational exposure to silver in refining, metal work, pho- deposits characteristic of argyria in muscle, skin, and nerves but
tography, and preparation of silver compounds for industry is no other undesirable effects.
commonly associated with argyria and argyrosis.11,14,76 Blood In contrast, argyria reported in a fatal case of a 72-year-old
silver concentrations in these workers may be more than twice woman with carcinoma of stomach and uterus was associated
that seen in unexposed individuals (11 µg/L) and associated with with a deposition of silver sulfide in the basal lamina of her
high urinary (5 µg/g) and fecal silver excretion (15 µg/g).71 choroidal epithelium.89 This patient had consumed an unknown
Invariably, reported studies have focused on the deposition of concentration of Argyrol in nose drops over 2–5 years. Although
silver sulfide granules in the skin and eye, with rare reference her tissues were badly autolysed, the authors claimed that silver
to other tissues or report of neurological abnormalities. Occu- sulfide granules (70–220 nm) were not membrane bound (lyso-
pational health studies have shown that the cornea is a sensitive somal) and mostly associated with collagen fibrils and stroma
indicator of silver exposure. of blood vessel walls. Silver granules were not contained within
Moss et al. examined 30 employees in an industrial plant in- leptomeninges, ependymal cells, or subependymal regions or in
volved in the manufacture of silver nitrate and silver oxide and the cells of the choroid plexus and minimal amounts present
identified corneal and conjunctival pigmentation in 20, with the within the area postrema. Elsewhere, florid agyria reported in
severity of the discoloration being directly related to duration a 78-year-old woman following chronic administration of over-
of employment.80 Ten workers with impaired night vision at- the-counter nasal drops was associated with widespread silver
tributable to the silver deposits failed to show electrophysiologic sulfide deposits in skin, liver, kidney, arteries, pituitary, and
or psychophysiologic evidence of functional deficits. Although choroid plexus.16,90 The authors employed specialized scanning
direct evidence of neurobehavioral changes has not been seen in electron microscopy with energy-dispersive spectroscopy (x-ray
workers exposed to silver occupationally, Rosenman et al. did microanalysis) (EDAX) to characterize the chemical composi-
observe that most of the 20 New York factory workers show- tion of the deposits. A later analysis of this case suggested that
ing occupational argyrosis complained of headaches, tiredness, silver deposits were predominantly in those parts of the brain
and nervousness.81 They emphasized the importance of moni- having higher regional blood flow and possibly greater perme-
toring silver in the work environment and regularly examining ability to environmental chemicals.8,34,35
staff with slit lamp to assess health status. In a more recent A case of myoclonic status eplepticus following repeated
case of occupational argyrosis, multifocal degenerative epithe- oral ingestion of colloidal silver in the form of a homemade
lial changes in the cornea were associated with a diffuse depo- “silver drink” was a cause for irreversible neurologic toxicity
sition of silver in the corneal stroma and Descemet’s membrane with poor prognosis.17 Myoclonic status epilepticus has not
and tissue debris.82 previously been associated with silver toxicity and this caseNEUROTOXICITY OF SILVER 243
deserves close attention. The 71-year-old male had used this and metallothionein induction may underlie changes in smell
homeopathic remedy containing a colloidal silver preparation and taste perception.93 ]
for 4 months, along with an antiandrogen for treating prostatic
cancer and various nutritional supplements. He developed paral- SILVER IN WOUND CARE
ysis with high levels of silver in blood and CSF, and markedly
elevated silver excretion in urine. Plasmaphoresis resulted in a Silver Nitrate
significant reduction in blood and CSF silver concentrations but Silver nitrate (0.5 or 1.0%) was probably the first antibacterial
no improvement in his neurological condition. He lapsed into a agent adopted in human and veterinary medicine. In Sollemann’s
coma and his EEG revealed 14-to 18-Hz electropositive central- Manual of Pharmacology,83 inorganic salts of silver, notably the
frontal polyspikes during myoclonic jerks. He died 5.5 months nitrate, were recorded as being astringent, caustic, and antiseptic
after the onset of his seizures. Autopsy revealed that his brain was but with their local action easily controlled by their precipitation
overtly normal, but showed evidence of diffuse Alzheimer type with proteins at the site of application. The cutaneous irritancy
2 astrocytosis and microglial activation. His nervous system was seen is directly proportional to concentration, duration of ex-
sampled extensively but showed no evidence of neuronal loss or posure, and the sensitivity of the skin at sites of exposure. The
focal pathology. High-resolution spectroscopy revealed elevated literature is replete with case studies of the use of silver ni-
silver deposition in the grey matter of his cerebrum (0.068 µg/g trate in treating neonatal eye disease, abrasion of warts, ulcers,
wet weight), estimated to be at least twice control levels. Silver and excessive granulations, and in the cauterization of chronic
deposits were not specifically associated with Alzheimer-related catarrhal infections.8,9 Additionally, silver nitrate has been used
changes and their distribution in aspects of the choroid plexus as an abortifacient and urethral sterilant. The literature shows
and BBB is unclear. The spectrometry confirmed silver in the considerable inconsistency in the exposure of skin and mucus
region of the cerebrum but did not exclude the possibility that membranes to silver nitrate, and the extent to which the silver ion
the vast proportion of this silver was contained within the BBB absorbed into the circulation is metabolized to internal organs.
and not neurological tissues. The toxicology of silver nitrate has been reviewed and limited
More tangible evidence of neurotoxicity resulting from sil- evidence provided to show that when used under clinical con-
ver nitrate administration was reported in a 59-year-old woman ditions for burn wound antisepsis or wound abridement, it is a
using self-adminstered drops for ulcers of her tongue.15 She potential cause of neurological damage.8 Silver nitrate ionizes
developed cutaneous argyria and a manic-depressive psychosis readily in the presence of moisture and light energy; the nitrate
but died 6 years later from a ruptured aortic aneurism. At au- anion is acidic and largely responsible for the corrosive and
topsy silver deposits were identified in skin, mucus membranes, toxic effects ascribed to the parent compound.94 Strong silver
and in many aspects of her central nervous system, notably lep- nitrate solutions are still used to cauterize or remove calluses,
tomeninges, choroid plexus, basal ganglia, hypothalamus, sub- warts, and excessive granulations, but application is normally
stantia nigra, and cerebellum. The silver deposits were lysoso- acute and levels of silver ion penetrating to the circulation are
mally bound and located specifically within intraparenchymal exceedingly low. In a fatal case of a 60-year-old man exposed
regions and not in neurons or glial cells. Progressive glial cells to silver nitrate dressings 8 h daily for 30 days, argyria devel-
changes and cellular gliosis were evident in many areas of the oped and skin silver levels of 2800 mg/kg and plasma silver of
brain. In a similar way, generalized argyrosis, was reported in 0.12 mg/L were recorded, but no silver was seen in his brain.95
a 52-year-old man treated with 35 mg of an unidentified sil- A similar situation was seen in an 18-year-old man receiving sil-
ver preparation for 18 years (estimated total intake of 35 g ver nitrate for only 6 days; his plasma silver was 0.12 mg/L and
silver).91 This patient died of cardiac failure, but dense silver skin silver 1250 mg/L. Neither patient was reported as showing
sulfide deposits were observed in blood vessels, kidney, liver, neurological or behavioral change.
and choroid plexus at postmortem. Westhofen and Schafer con- Greater risk of argyria and deposition of silver in the cen-
sidered that silver exhibits a strong predilection for membrane tral nervous system are anticipated where silver nitrate is used
and neuronal structures in severe cases of argyria with neurolog- to cauterize the cervix following surgical biopsy or as a means
ical involvement, but that silver sulfide deposition advanced the of inducing abortion. The extent to which this practice is per-
“progression of clinical disease.”92 They used light and elec- formed today is not known, but at concentrations of greater than
tron microscopy to demonstrate silver sulfide granules in the 5% silver nitrate is highly astringent and irritant to mucosal
perineurium of peripheral nerves of a severely argyric patient membranes.96 Silver ion released in the presence of urethra flu-
following chronic self-administration of an unidentified silver ids actively binds to cell surfaces and proteins in tissue exudates,
product. Symptoms of progressive taste and smell disorders, ver- but some will be available for diffusion to the peripheral circula-
tigo, and hypesthesia were confirmed by chemosensitivity tests tion. This diffusion will be promoted through local inflammation
and electrophysiological investigations. Blood and brain silver and cellular damage through the acidity of the nitrate ion. Free
levels in this patient were not given and it is unclear whether the silver ion can be expected to precipitate locally in the form of
symptoms (other than argyria) receded following withdrawal of an innocuous argyria. A forensic case is recorded of a German
silver therapy. [Silver-induced alterations in zinc metabolism woman given a highly corrosive 7% solution of silver nitrate to244 A. B. G. LANSDOWN
induce abortion.65 The woman died with extreme trauma and cir- ity has invariably been attributed to the painful condition of the
culatory failure within 3 hours and at autopsy, silver was found wound rather than to any neurotoxic action of the silver released.
widely distributed throughout her body, including her brain, but
her tissues were heavily congested. SILVER IN MEDICAL DEVICES
Medical devices including catheters, bone cements, ortho-
pedic fixation pins, and cardiac prostheses and valves are no-
Silver Sulfadiazine
toriously prone to bacterial adhesion, colonization, and biofilm
Silver sulfadiazine is a white microcrystalline powder with
formation. Recent advances in silver nanotechnology, materials
low solubility in water. As a 1% formulation in amphiphilic
science, and ion beam silver coating techniques have been in-
cream it readily ionized in burn wounds to release Ag+ for an-
creasingly employed in an attempt to engineer out these risks
timicrobial purposes.97,98, It is appreciably less corrosive to the
of infection and improve patient comfort and survival.106,107
skin than silver nitrate although local irritancy is reported.99,100
Intraurethral catheters are of particular interest; in the United
The reservoir of silver ions accumulating in the wound allows
States alone physicians implant more than 5 million catheters
a prolonged release of silver for protein binding and absorption
annually.
into the circulation. Up to 10% of topically applied silver sulfa-
Adverse effects attributable to silver including argyria are
diazinde is absorbed from deep partial-thickness burn wounds,
exceedingly rare. Absorption of silver from catheters im-
particularly in the region of high vascularity. Blood concentra-
planted following prostatectomy and surgery is not well doc-
tions in patients with greater than 60% total body area burns may
umented despite recent advances in biotechnology and catheter
rise to 300 µg/L, with urinary excretion in the range 100–400
design.107−110 The hydrophilic coatings impregnated with silver
µg/L.70 Although early reports emphasise the low risks of silver
metal (including nanocrystalline forms), silver oxide, and sil-
sulfadiazine toxicity in routine wound care,13 its more extensive
ver sulfadiazine on inner and outer surfaces of catheters release
use and incorporation in medical devices for long-term implan-
free silver ion in the presence of urethral fluids and exudates
tation have indicated greater caution than at one time considered,
for antimicrobial purposes. The concentration of silver required
including the risk of neurological damage.
for antimicrobial action in intraurethrine catheters has been esti-
Argyria is occasionally observed in patients treated with sil-
mated to be about 10−9 .111 This exceedingly low concentration
ver sulfadiazine for severe burns of 60% or greater total body
is achieved by novel technology in which nanocrystalline silver
area. In a patient with end-stage renal disease, argyria was as-
is distributed in polyurethane at 0.8% in a hygroscopic matrix of
sociated with a marked elevation of blood silver and deterio-
450 cm2 /polyurethane. An Erlanger polyurethane catheter de-
ration in his mental state.101 Blood silver levels of 291 µg/L
veloped to reduce the risks of infection with a mass ratio of
were associated with greatly raised brain silver (617.3 ng/g,
0.6% silver released a total of 7 µg/L silver into physiological
cerebrum; 823.7 ng/g cerebellum wet weight). Hemodialysis,
saline within 26 hours (0.1 µg/L for 30-cm catheter).112 Other
hemofiltration, and plasma exchange were effective in reduc-
estimates suggest that concentrations of silver released from
ing blood silver, but the patient died. Although this case might
acute care catheters coated with a polymer containing 1012−13
implicate silver per se as a neurotoxin, the information pre-
silver nanoparticles ranged from 250 to 350 ng/cm2 /day over
sented fails to demonstrate silver within neurological tissues or
10 days. These levels are deemed suitable for antimicrobial
its association with neurodegenerative changes. The study does
action but unlikely to significantly influence blood silver lev-
not preclude infection or immunosupression as a possible cause
els or neurophysiological activity. The Cochrane Incontinence
of fatality. Flammacerium (Solvay Pharmaceuticals) (contain-
Group and the Cochrane Renal Group evaluated the manage-
ing 1% silver sulfadiazine and 2.2% cerium nitrate) was intro-
ment of silver coated catheters for short-term use.113 They em-
duced to alleviate problems of immunosuppression attributable
phasized the cost-benefit ratio of the new silver technology
to products forming in burn wounds as a result of thermal
in controlling bacterial adhesions and biofilm formation as a
energy.102
cause of fatality but have failed to recognize the potential toxic
implications of the silver released. Cymet questioned whether
Sustained Silver-Release Wound Dressings silver “alloy” catheters might increase the inherent risks of
Numerous sustained silver-release wound dressings have systemic argyria and risks of silver toxicity,114 but no satisfac-
been developed in recent years. The silver content of these dress- tory responses have been received. An unseen Russian study
ings ranges fromNEUROTOXICITY OF SILVER 245
but acknowledged that the risk did exist in long term urethral argyric implications.78 In a particularly severe case of a woman
drainage with the consequence of silver deposition in internal using up to 2500 needles over 13 years, macular argyria with ir-
organs. regularly shaped silver sulfide granules of 40–500 nm diameter
Clinical studies with hemodialysis and intravascular catheters distributed mainly in extracellular dermal sites and around nerve
have similarly failed to produce evidence of silver toxicity or fibers and elastic tissues but overt nerological changes were not
brain involvement even though silver ion released directly into recorded.
the circulation would be expected to lead to increased plasma- Suggestions that argyria developing through implantation of
bound silver and greater tissue deposits. Tobin and Bambauer acupuncture needles might interfere with tissue function have
reviewed clinical studies designed to assess the efficacy and bio- not been substantiated.8 Although discolorations of the face and
compatibility of silver-coated dialysis catheters.117 They noted body have been associated with acupuncture needles containing
that blood silver levels increase from a mean of 1.3 to 6.9 µg/L up to 69% silver, brain involvement has not been reported.78,121
for acute catheters and from 3.4 to 19.6 µg/L for long-term Blood silver levels are not known in these cases but are expected
catheters, in each case with plasma levels returning to normal to be well below toxic range of 50–500 mg/kg body weight that
on removal of the catheters. No data was provided for tissue has been associated with abnormal encephalographic changes
silver deposition or evidence of toxic side effects. Maki et al. and brain scan findings.122
evaluated triple-lumen catheters (ARROWgard) designed for in- Antismoking remedies containing silver are included in med-
travenous insertion.118 They contained 0.70 mg silver sulfadi- ical devices, although there is no evidence that they present a
azine and evoked a mild local erythema at insertion points and neurotoxic hazard. An example documented is of a healthy 47-
plasma silver levels of 45–73 ng/mL in the 12 patients tested. year-old female patient who showed profound argyria following
These incredibly low concentrations are of minimal toxicologi- excessive oral dosage of silver acetate as an antismoking remedy
cal significance. for 6 months.123 Silver–protein complexes are readily absorbed
Mechanical heart valves containing silver have been associ- through the buccal mucosa, and in this patient analyses using
ated with greater hazard than in-dwelling catheters. Thus, St. neutron activation showed her total body silver burden to be
Jude Medical applied a silver coating to the sewing cuff of its 6.4 g, of which only 1.8% was retained within the blood. Silver
Silzone range of heart valves with the objective of reducing absorption and retention analyzed by radioactive trace admin-
risks of infective endocarditis. Over 30,000 of these valves were istration showed that after an initial decrease, 18% silver tracer
distributed after 1997, but the valve was withdrawn through remained in the body for up to 30 weeks, but the amount de-
thrombo-embolytic complications.119 In one such case, a St. posited in her brain is not known. She remained in overt good
Jude Medical Silzone valve was implanted into a 72-year-old health throughout the observation.
woman suffering from mitral valve disease. Her fatality was at- Strong evidence implicating silver as a cause of neurologi-
tributed to chronic inflammatory disease but the implication of cal toxicity and behavioral changes derives from use of a silver
silver in this case is unclear. Experimental studies in sheep im- as an antimicrobial agent in arthroplasty cement. Bone cement
planted with the Silzone valve showed plasma silver of 40 ppb containing an unknown quantity of silver was used to anchor a
within 10 days and mean brain silver of 4.32 ± 0.28 µg/g dry Christiansen prosthesis in a 78-year-old woman.18,19 Five years
tissue weight after up to 20 days.117 Liver concentrations were a after insertion of the prosthesis, the patient became unstable
lot higher at 16.75 ± 5.18 µg/g, but changes were not reported and exhibited muscle weakness in her left leg. Electromyogra-
in other tissues. phy revealed no activity in those muscles innervated by her left
Acupuncture needles should be included among the med- tibial and femoral nerves and a total paralysis of her quadri-
ical devices containing silver. Their use has been associated ceps muscle. This was related to exceptionally high levels of
with macular or widespread argyric changes with occasional silver in her hip joint fluid (956 nmol/L), blood (58 nmol/L),
neurological involvement.121 This “Hari” therapy conducted in and biopsies of acetabulum. Biopsies of soft tissue revealed
Japan for many centuries for relief of fatigue and headache in- granules characteristic of argyria in the region of elastic fibers
volves long-term intracutaneous insertion of silver–gold nee- and in numerous macrophages, but not in peripheral nerves.
dles. A 21-year-old Japanese woman given this Hari therapy The right leg was entirely normal. The prosthesis was removed
over 2 years to relieve asthma developed a profound macular and blood silver levels declined to 15 nmol/L within 12 months
argyria and chrysiasis on her neck, face, and chest.77 Minute and conducting activity was restored fully to her tibial muscle
silver–gold particles (20–60 nm) were deposited along the outer and partially to her femoral nerve. Motor activity was also im-
edge of basement membranes of blood vessel and sweat glands, proved in her quadriceps muscle. The patient was closely mon-
and in lines around but not in nerve fibers. Small amounts of itored over 10 yearss by which time the paralysis had receded
silver–gold were evident also in basement membrane collagen and the patient was able to walk unaided. Although transitory
associated with myelinated and nonmyelinated nerves but nerve electrophysiological changes were observed several months af-
damage was not reported. Silver acupuncture needles are used ter removal of the prosthesis, neurotoxic action of silver was not
in treating for sterility and general fatigue conditions, but have substantiated.246 A. B. G. LANSDOWN
DISCUSSION only in the suitability of a silver-containing reagent to demon-
All medical devices, wound dressings, and medicaments con- strate silver deposits in a tissue, but in the resistance of the two
taining silver or coated with a silver complex to achieve antimi- principal silver precipitates seen in argyria, that is, silver sulfide
crobial action release silver ion in the presence of moisture, and silver selenide, to reduction with potassium cyanide. The
body fluids, and exudates.103 A proportion of this biologically observations are entirely contradictory to the results of several
active silver will be absorbed into the body in a carrier-mediated earlier studies using a similar experimental model, and in which
process; it enters the bloodstream and is deposited in soft silver was contained within the BBB and acted in the form of an
tissues.1,12,71 Clinical studies in patients with severe argyria or intravital dye like trypan blue.50−55
with purported silver “poisoning” have consistently failed fully Lack of frank evidence for the neurotoxic action of silver
establish the ability of silver to pass the blood–brain barrier or may in part be explained by the deposition of inert precipitates
evoke irreversible damage at any site in the central nervous sys- of silver sulfide or silver selenide in lysosomal vesicles. Electron
tem. Silver does not satisfy the criteria for neurotoxins set out microscopy has demonstrated the membrane-bound deposits in
in Table 1, although several equivocal issues remain. Not least endothelial cells of the BBB, especially the choroid plexus in
of these is whether and to what extent silver is able to penetrate cases of generalized argyria.15,59,92 Previous studies have com-
the blood–brain barriers in any part of the central nervous sys- prehensively established that lysosomally bound silver in liver
tem to precipitate in the form of argyria within neurons or glial and kidney (14 µg Ag/g wet tissue weight) is not associated with
cell populations to evoke pathological or behavioral changes. functional abnormalities and that there is no correlation between
Evidence reviewed shows that silver is absorbed into the circu- silver levels in the tissues and circulation.12 Wang et al. used 20–
lation following inhalation, ingestion, and through use of various 50% silver sulfadiazine to treat patients with severe burns and
medicated devices, but levels or argyremia tend to fall rapidly reported argyremia of >300 µg/L, yet reported normal tissue
as the silver is disseminated throughout the body. Prolonged function.1,12 Early alterations in liver metabolizing enzymes re-
exposure to silver occupationally or therapeutically can lead to ported in burn wound patients treated with silver sulfadiazine
manifestations of argyria and argyrosis with lysosomally bound normalized and were not associated with changes in long-term
deposits of silver sulfide or silver selenide occurring in liver, exposure.126,127
kidney, vascular tissues, and in connective tissues of the blood– Silver absorbed into soft tissues induces and binds the
brain barrier and skin. Silver ion exhibits a strong binding to cysteine-rich metallothioneins, which exibit a regulator and cy-
sulfhydryl (-SH) moieties in collagens of connective tissues and toprotective role.128,129 In the skin at least, metallothioneins play
basement membranes and has frequently been observed in the an instrumental role in the metabolism of silver in normal and
region of peripheral nerves (myelinated and nonmyelinated) but damaged tissues and possibly contribute to the action of silver
not within neurological tissues. in wound repair.130,131 Metallothioneins are present in all liv-
Considerable evidence points to the efficiency of the blood– ing cells and have a unique structure relating to their ability to
brain barriers in various parts of the central system in accu- sequester and bind metals like zinc and silver. Four isoforms
mulating silver, thereby mitigating whatever toxic influence the of metallothionein have been identified so far, including MT-I
metal might have on nervous tissue. This wider survey of silver and MT-II, which are expressed in a variety of tissues including
provides further evidence in support of Zheng’s hypothesis that the brain, MT-III, which is predominantly located in the brain,
silver should be classified alongside iron, zinc, and gold as a and MT-IV, which occurs in squamous epithelia like the tongue.
“sequestered choroid plexus toxicant,” namely, a metal that is Metallothioneins modulate three main processes in mammalian
sequestered by the tissue and not associated with pathological cells:
changes or pathophysiological consequences, including changes
1. Release of mediators (e.g., hydroxyl radical, nitric oxide).
in the blood–CSF barrier.29,33
2. Apoptosis.
Evidence that silver can penentrate the blood–brain barriers
3. Binding and exchange of heavy metals (zinc, cadmium, cop-
to cause transitory physiological change is provided largely by
per, silver, etc.).129,132
experimental studies in rodents dosed with high levels of ioniz-
able silver compound in drinking water or through intravenous Much remains to be learned regarding the primary function of
injection. Thus Rungby and Danscher have demonstrated silver MTs, including their regulatory role in tissue repair and re-
throughout the central nervous system but have failed to identify generation. They are present to a greater or lesser extent in
frank pathological changes.46,59,62 They based their observations all regions of the brain and spinal cord and have been impli-
entirely on autometallographic demonstration of silver in tis- cated in nerve regeneration and Alzheimer’s disease and other
sues. This technique employs histochemical methods in which neurological conditions.133 Experimental evidence suggests that
silver impregnation is used as an aid to identifying neuropatho- MT-III expression is altered in brain injury and that regen-
logical changes.124,125 It relies on reduction of silver residues in eration of peripheral nerves is advanced in MT-III knock-out
tissue sections by potassium cyanide and development of metal mice.134 Metallothioneins, notably MT-III, are predominantly
deposits using a developer containing silver as in photographic expressed in zinc-containing neurons of the hippocampus but ab-
processing. The validity of the method might be questioned, not sent from glial elements.133 Although silver displaces zinc fromNEUROTOXICITY OF SILVER 247
zinc–metallothionein complexes in the skin, it is unclear at the ACKNOWLEDGMENTS
moment whether it can displace zinc bound in MT-III com- I appreciate the constructive advice from Professor C.
plexes in the hippocampus or other regions of the brain leading Kennard, Deputy Principal, Imperial College Faculty of
to increased extracellular zinc as required for RNA and DNA Medicine, London, and express thanks to Professor A. Dayan,
synthetases and other essential enzymes. If, as suggested by ex- formerly director of DHSS Department of Toxicology, St.
perimental studies in the rat,46 silver does pass the blood–brain Bartholomew’s Hospital Medical School, London.
barrier to be sequestered by neurons and glial cells, it should
be assumed that it will induce MT synthesis in neural tissues REFERENCES
and initiate certain stress symptoms and pathophysiological pro- 1. Wan, A.T., Conyers, RAJ., Coombs, C.J., and Masterton, J.P.
cesses associated with excess zinc.93 At the moment, it is unclear (1991). Determination of silver in blood, urine and tissues of
whether silver induces MT-III or to what extent the protein acts volunteers and burn patients. Clin. Chem. 37:1683.
as a cytoprotectant in the central nervous system. 2. Lansdown, A.B.G. (1995). Physiological and toxicological
The observation of transient paralysis in the woman treated changes in the skin resulting from the action and interaction of
with silver-containing bone cement to anchor a Christianson metal ions. CRC Crit. Rev. Toxicol. 25:397.
3. Lansdown, A.B.G. (2002). Silver 2: Toxicity in mammals and
prosthesis is difficult to explain in terms of silver toxicity.18,19
how its products aid wound repair. J. Wound Care 11:173.
Despite the electrophysiological evidence of functional change, 4. White, R.J. (1999). A historical review of silver in wound man-
reduced conduction was not associated with silver deposits in agement. Br. J. Nurs.S3–S8.
nerves. The high concentrations of silver present in her hip joint 5. Klasen, H.J. (2000). A historical review of the history of silver in
fluid were probably strongly bound to proteins and hence in- burns. Burns 26:117.
ert. Silver deposition was reported in connective tissues around 6. Hambidge, A. (2001). Reviewing efficacy of alternative water
the hip joint and in the perineurium but the physiological im- treatment techniques. Health Estate 55:23.
plications of this are not known. Silver is not lipophilic and is 7. Lansdown, A.B.G., Williams, A., Chandler, S., and Benfield, S.
not known to penetrate myelin sheaths.29 Further neurophysi- (2005). Silver absorption and antibacterial efficacy of silver dress-
ological studies on the effects of extracellular silver on nerve ings. J. Wound Care 14/4:155.
conduction may shed some light on the clinical significance of 8. Humphreys, S.D.M., and Routledge, P.A. (1998). The toxicology
of silver nitrate. Adverse Drug React. Toxicol. Rev. 17:115.
this case.
9. Fung, M.C., and Bowen, D.L. (1996). Silver products for medical
The present review complements my earlier observations indications: risk-benefit assessment. Clin. Toxicol. 34:119.
that silver is without serious toxic risk to any organ system 10. Boosalis, M.G., McCall, J.T., Ahrenholtz, D.H. et al. (1982).
in the human body. However, recommendations for safe ref- Serum and urinary silver levels in thermal injury patients. Surgery
erence values are extremely difficult to make since silver de- 101:40.
posits will accumulate temporarily in most soft tissue, to be 11. Pariser, R.J. (1978). Generalised argyria: clinicopathologic fea-
eliminated eventually via the kidney or liver without toxic tures and histochemical studies. Arch. Dermatol. 114:373.
implications.1,12 Silver sulfide/selanide deposits in the skin and 12. Coombs, C.J., Wan, A.T., Masterton, J.P., et al. (1992). Do burn
eye may be long-lasting but have not been associated with patients have a silver lining? Burns 18:179.
toxicity or ill health.13,105 Silver deposits in the eye may ob- 13. Lansdown, A.B.G., and Williams, A. (2004). How safe is silver
scure night vision, but this has not been associated with neu- in wound care? J. Wound Care 13:131.
14. Bleehan, S.S., Gold, D.J., Harrington, C.I., et al. (1981). Occupa-
rological changes.80,81 A small number of people experience
tional argyria: Light and electron microscopic studies and X-ray
delayed hypersensitivity to silver, and they should avoid sil- microanalysis. Br. J. Dermatol. 104:19.
ver ingestion, inhalation, and use of silver-containing medical 15. Deitl, H.W., Anzil, A.P., and Mehraein, P. (1984). Brain involve-
devices. ment in generalised argyria. Clin. Neuropathol. 3:32.
Permissible exposure limits and threshold limit values set 16. Landas, S., Bonsib, S.M., Ellerbroek, R., and Fischer, J. (1986).
by the American Conference of Governmental Industrial Hy- Argyria: Microanalytic-morphologic correlation using paraffin
gienists (ACGIH),135,136 the National Institute for Occupational embedded tissue. Ultrastruct. Pathol. 10:129.
Safety and Health (NIOSH), and the European Commission 17. Mirsattari, S.M., Hammond, A.R., Sharpe, M.D., et al. (2004).
recommended threshold limit values (TLV) of 0.01 mg/m3 Myoclonic status epilepticus following repeated injection of col-
for metallic silver (including nanoparticulate forms) and sil- loidal silver. Neurology 62:1408.
ver compounds. According to Drake and Hazelwood the AG- 18. Vik, H., Andersen, K.J., Juhlshamn, K., and Todnem, K. (1985).
Neuropathy caused by silver absorption from arthroplasty cement.
CIH recognized the different outcomes from exposure to solu-
Lancet I:872.
ble and/or insoluble silver compounds, rationalizing that solu- 19. Sudmann, E., Vik, H., Rait, M., et al. (1994). Systemic and lo-
ble compounds are more likely to cause argyria and associated cal silver accumulation after total hip replacement using silver-
effects than does the “dust or fume of metallic silver.”135,136 impregnated bone cement. Med. Prog. Technol. 20:179–184.
As such the recommended TLV for metallic silver exposure is 20. Roper, W.L. (1990). Toxicological profile for silver. Agency
set at 0.01 mg/m3 and that for soluble silver compounds is 0.1 for Toxic Substances and Disease Registry, U.S. Public Health
mg/m3 .136 Service, Atlanta, GA.You can also read