DON'T FAIL ME NOW: HORMONAL CONTRACEPTIVES - COURTNEY KAIN, PHARMD, BCPPS EMILY RODMAN, PHARMD, BCPPS - TEXAS CHILDREN'S HOSPITAL
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Don’t Fail Me Now: Hormonal Contraceptives Courtney Kain, PharmD, BCPPS Emily Rodman, PharmD, BCPPS DEPARTMENT NAME
DISCLOSURES • The presenters have no financial conflicts of interest to disclose DEPARTMENT NAME

OBJECTIVES • Classify routes of administration for hormonal contraceptives • Identify common adverse effects and contraindications related to hormonal contraception • Evaluate literature regarding safety and efficacy of certain types of hormonal contraceptives DEPARTMENT NAME
TEEN BIRTH RATE BY ETHNICITY
Birth Rates per 1,000 Females Aged 15-19 Years by Race,
100 2000-2015
90
80
70
60
50
40
30
20
10
0
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Year
White Black American Indian/Alaska Natives Asian/Pacific Islander Hispanics
DEPARTMENT NAME
Hamilton. Continued Declines in Teen Births in the United States, 2015. NCHS Data Brief. 2016;No.259:Figure 1.
Hamilton. Births: Final data for 2014. National Vital Statistics Reports. 2015;64(12):Table 4.
TEEN BIRTH RATE* BY COUNTRY
Switzerland
Japan
Netherlands
Sweden
Denmark
Italy
Countries
Finland
Norway
Germany
France
Greece
Spain
Canada (2009)
Portugal
Australia
United Kingdom
United States (2012)
0 5 10 15 20 25 30 35
Rate* (per 1,000 females age 15-19)
DEPARTMENT NAME
*All rates are from 2013 unless otherwise stated
United Nations Statistical Division. Demographic Yearbook 2014. New York: United Nations.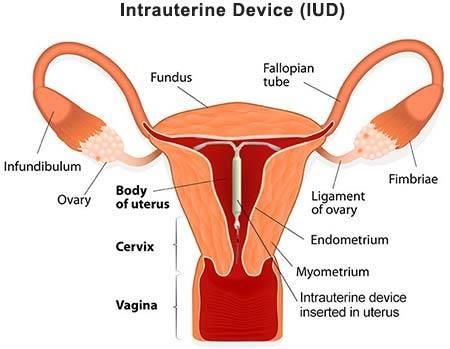
TEEN PREGNANCY RATE BY STATE
DEPARTMENT NAME
Ventura. National and State Patterns of Teen Births in the United States, 1940-2013. National Vital Statistics Reports. 2014;63(4):Figure 11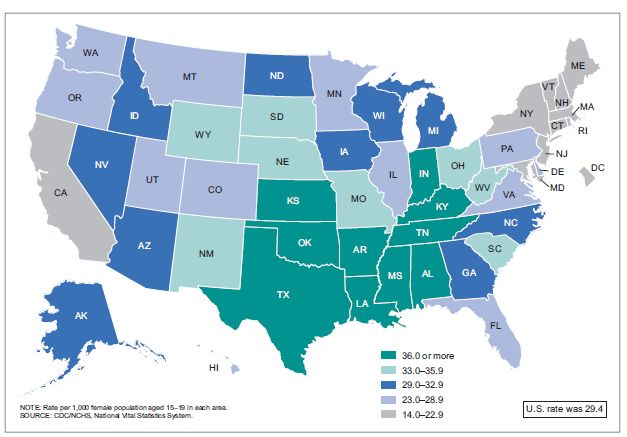
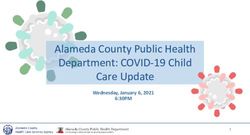
IMPACT OF CONTRACEPTION ON TEENS
• 1 in 5 women will give birth before the age of 20
• 80% of teen pregnancies are unintended
• 46% of teen pregnancies due to non-use of
contraception
• 54% of teen pregnancies due to contraceptive failure
related to:
• Use of moderately or less effective methods
• Incorrect or inconsistent use
DEPARTMENT NAME
Committee on Adolescence. Contraception for adolescents. Pediatrics. 2014 Oct;134(4):e1244-56.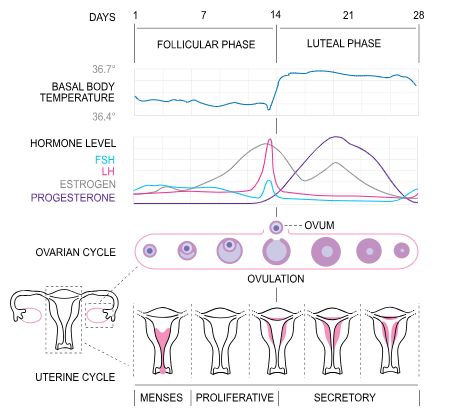
BACKGROUND Physiology of Hormonal Contraception DEPARTMENT NAME
INDICATIONS FOR HORMONAL CONTRACEPTION
• Pregnancy prevention • Premenstrual syndrome
(PMS)
• Dysmenorrhea
• Premenstrual dysphoric
• Endometriosis disorder (PMDD)
• Polycystic ovarian • Treatment of
syndrome (PCOS) androgenisation
symptoms
• Fertility preservation • Acne
during chemotherapy • Hirsutism
• Menstrual migraines • Alopecia
DEPARTMENT NAME
Schindler AE. Int J Endocrinol Metab. 2013 Winter. 11(1): 41-7.MENSTRUAL CYCLE PHYSIOLOGY
• Length of menstrual cycle varies
• Regular: < 8 days between longest & shortest cycles
• Moderately irregular cycle: variations between 8-20 days
• Very irregular cycle: variations > 21 days
• Average cycle lasts 28 days
• Hormone production in hypothalamus, pituitary gland, ovaries and
uterus
• Three phases
• Follicular
• Ovulation
• Luteal
DEPARTMENT NAMEDEPARTMENT NAME
By Isometrik - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=8703107ESTROGEN & PROGESTERONE’S ROLE IN
CONTRACEPTION
Hypothalamus
GnRH
Inhibitory
Pituitary
Effect
LH FSH
Inhibitory
Effect Ovaries
Estradiol Progesterone
DEPARTMENT NAMEAdverse Effect More Likely Less Likely
Acne Progestin-only methods COC, vaginal ring
Amenorrhea Progesterone IUD, depot, continuous cycle
COC, progestin-only pills
COC, continuous use ring
Breakthrough bleeding Low-dose COC, extended cycle regimens High-dose COC, progesterone IUD,
(with levonorgestrel), progestin-only pills, extended cycle regimens (with
implant norethindrone), ring, patch
Breast tenderness Low estrogen COC, >18 months COC use,
Patch
ring
Decreased libido Very low-dose COC (35
Headache (menses-associated) -- Extended cycle COC
Heavy menses Implant, depot COC, patch, ring, progesterone IUD
Hirsutism Progestin-only methods COC
Increased vaginal discharge Ring All other methods
Irregular menses Emergency contraceptives, depot, implant Patch
Nausea Patch, COC for emergency contraceptive Ring, no difference between COCs
Oily skin Progestin-only methods COC
WeightDEPARTMENT
gain NAME Depot COC, patch, ring, progestin-only pills, IUD
Adapted from Grossman N, et al. Am Fam Physician. 2010 Dec 15;82(12):1499-1506.
COC = combined oral contraceptive, IUD = intrauterine device, depot = depot medroxyprogesterone acetate
patch = estrogen/progestin topical patch, ring = estrogen/progestin vaginal ring, implant = progestin subdermal implantTYPES OF HORMONAL CONTRACEPTION
Progestin-only contraceptives
• Oral pill
• Depot injection
• Subdermal implant
Combined hormonal contraceptives
• Oral pill (COC)
• Ring
• Patch
Intrauterine devices
Emergency contraceptives
DEPARTMENT NAME
COC = Combined oral contraceptiveORAL CONTRACEPTIVES DEPARTMENT NAME
ORAL CONTRACEPTIVE AGENTS
• Progestin-only pill (POP)
• Thicken cervical mucus
• Thin uterine lining
• Prevents release of ovary from follicle
• Combined oral contraceptives (COC)
• Estrogen + progestin
• Decreases breakthrough bleeding, less bleeding in general
• Reduces menstrual cramping
DEPARTMENT NAME
Dhont M. Euro J Contracept Reprod Health Care. 2010 Dec; 15(S2): S12-18.HISTORY OF COCS
• First Generation
• High estrogen component (≥ 50mcg)
• High progesterone component
• Lynestrenol, norethisterone, ethynodoil diacetate
• Weak androgenic activity → weight gain/water retention, hirsutism, voice changes/hoarseness
• Increased risk of thromboembolism (serum estrogen)
• Second Generation
• Reduction of estrogen dose (15mcg, 20mcg, 25mcg, 30mcg)
• Less breast tenderness, nausea & bloating
• Retained same low level of breakthrough bleeding
• New progesterone derivatives (no anti-mineralcorticoid activity)
• Levonorgestrel, norgestrel/norgestimate
• Anti-androgenic activity
• Some mineralcorticoid activity → weight/water gain, increased BP
DEPARTMENT NAME
Dhont M. Euro J Contracept Reprod Health Care. 2010 Dec; 15(S2): S12-18.HISTORY OF COCS
• Third Generation
• Retained lower estrogen dose (20mcg or 30mcg)
• New progestins
• Gestodene, desogestrel
• Lower androgenic activity than 2nd generation (acne, hirsutism, weight gain)
• Reported increase risk of VTE with this generation
• Fourth Generation
• New progestins
• Drospirenone, dienogest, cyproterone acetate, chlormadinone acetate
• Stronger anti-androgenic and anti-mineralcorticoid effects
• Less effect on blood pressure 2/2 less water retention
DEPARTMENT NAME
Gallo MF, Nanda K, Grimes DA, Lopez LM, Schulz K. Cochrane Database of Systematic Reviews. 2013, Issue 8
Bachmann G, Kopacz S. Patient Prefer Adherence. 2009; 3:259-64.
Dhont M. Euro J Contracept Reprod Health Care. 2010 Dec; 15(S2): S12-18.COMBINED ORAL CONTRACEPTIVES
Monophasic Constant dose of estrogen and progestin provided in the active pills per cycle
Biphasic, triphasic, Dose of estrogen and progestin vary in active pills
and four-phasic
21/7 regimen 21 days of active tablets, followed by 7 days of inactive tablets; provides monthly
withdrawal bleeding
24/4 regimen 24 days of active tablets, followed by 4 days of inactive tablets; provides monthly
withdrawal bleeding with decreased duration and lighter blood flow as compared
to 21/7 regimens
24/2/2 and 21/2/5 Decreases hormone-free interval from 7 to 2 days by providing a lower,
regimen noncontraceptive dose of ethinyl estradiol (0.01 mg) in place of placebo tablets.
Provides monthly withdrawal bleeding with decreased duration and lighter blood
flow as compared to 21/7 regimens
84/7 regimen Extended-cycle contraceptive. Consists of 84 days of active tablets, followed by 7
days of inactive tablets. Decreases withdrawal bleeding to 4 times/year.
DEPARTMENT NAME
Adapted from Lexicomp Online, Pediatric and Neonatal Lexi-Drugs Online, Hudson,
Ohio: Wolters Kluwer Clinical Drug Information, Inc.; 2019; Dec 17, 2019.SAFETY & EFFICACY OF ORAL CONTRACEPTIVES
• Pearl Index (PI)
• Rate of unwanted pregnancies per 100 women-years
• POP: 0.48
• COC: 0.3
• Safety
• Increased venous thromboembolism (VTE) rates
• Incidence of certain hormone-regulated cancers
DEPARTMENT NAME
Oedingen C, Scholz S, Razum O. Thrombosis Research. 2018; 165:68-75.RISK OF VTE AND COCS
• VTE incidence in non-users: 1.9-3.7 per 10,000 women
• Age 30-34: 2.5 per 10,000
• Age 60-64: 9.3 per 10,000
• Annual incidence in COC users: 7-12 per 10,000
• Cochrane Review
Relative Risk (RR) vs Non-User RR vs First-Gen
Non-user --- ---
1st Gen 3.2 (2.0 – 5.1) ---
2nd Gen 2.8 (2.0 – 4.1) 0.9 (0.6 – 1.4)
3rd Gen 3.8 (2.7 – 5.4) 1.4 (1.0 – 1.8)
DEPARTMENT NAME
Oedingen C, Scholz S, Razum O. Thrombosis Research. 2018; 165:68-75.ORAL CONTRACEPTIVES AND CANCERS
Increased Incidence Decreased Incidence
• Cervical cancer • Endometrial cancer
• Breast cancer • Ovarian cancer
• Melanoma (conflicting • Colorectal cancer
evidence)
DEPARTMENT NAME
Donley GM, Liu WT, Pfeiffer RM, et al. British J Cancer. 2019; 120:754-60.
Cervenka I, RahmounMA, Mahamat-Saleh Y, et al. Int J Cancer. 2019.CERVICAL CANCER & ORAL CONTRACEPTIVES
• Fourth most common cancer among women
• European Prospective Investigations into Cancer and
Nutrition (EPIC) study
• Recruited from 1992 to 2000
• Number women evaluated: 308,036
• Follow-up average: 9 years (7.5-10.8 years)
• Endpoints
• Cases of cervical intraepithelial neoplasia, grade 3 (CIN3)
• Cases of invasive cervical cancer (ICC)
DEPARTMENT NAME
Roura E, Travier N, Waterboer T, et al. PLOS One; 2016 Jan.CERVICAL CANCER & ORAL CONTRACEPTIVES
CIN3 ICC
Non-cases/ Hazard Ratio Non-cases/ Hazard Ratio
Cases (95% CI) Cases (95% CI)
Oral Contraceptive (OC) Use
Never 121,117/169 1.0 (ref) 121,286/76 1.0
Ever 176,993/548 1.1 (0.9-1.3) 177,541/165 1.6 (1.1-2.3)
Past 152,658/411 1.0 (0.9-1.3) 153,069/134 1.6 (1.1-2.2)
Current 17,384/127 1.8 (1.4-2.4) 17,511/22 2.2 (1.3-4.0)
Duration of OC Use
≤ 1 year 31,867/78 1.0 (0.8-1.3) 31,945/27 1.5 (0.9-2.4)
2-4 years 40,168/127 1.1 (0.8-1.4) 40,295/27 1.3 (0.8-2.0)
5-9 years 38,816/136 1.1 (0.9-1.4) 38,952/41 2.0 (1.3-3.0)
10-14 years 26,969/90 1.2 (0.9-1.6) 27,059/26 1.6 (1.0-2.6)
≥ 15 years 23,395/82 1.6 (1.2-2.2) 23,477/28 1.8 (1.1-2.9)
DEPARTMENT NAME
Roura E, Travier N, Waterboer T, et al. PLOS One; 2016 Jan.
Loopik DL, IntHout J, Melchers WJG, et al. Euro J Cancer. 2020; 124:102-9.BREAST CANCER AND ORAL CONTRACEPTIVES
General consensus
• Higher doses of estrogen increase risk of ER + BC
• Longer use of OC’s increases risk
• Risk negated once discontinue OC for > 1 year
• Age of first use may be independent risk factor
• No difference in BC mortality of OC users compared
to non-users
DEPARTMENT NAME
Ji L, Jing C, Zhuang S, Pan W, Hu Z. Medicine. 2019; 98;36(e15719)
Beaber EF, Buist DSM., Barlow WE, Molone KE, Reed SD, Li CI. Cancer Res. 2014 Aug; 74(15): 4078-89.
Nur U, Reda DE, Hashim D, Weiderpass E. BMC Cancer. 2019;19:807.BREAST CANCER AND ORAL CONTRACEPTIVES
• 2014 study of U.S. women 20-49 years
• January 1990 to October 2009
• Data retrieved from health records, pharmacy records
• Rate of ER+/ER- breast cancer (BC) in OC and non-OC users
• Correlation of amount of estrogen component and BC diagnosis
• Correlation of type of progestin component and BC diagnosis
• Participants: 23,054
• Non-BC controls: 21,952
• BC cases: 1,102
DEPARTMENT NAME
Beaber EF, Buist DSM., Barlow WE, Molone KE, Reed SD, Li CI. Cancer Res. 2014 Aug; 74(15): 4078-89BREAST CANCER AND ORAL CONTRACEPTIVES
Controls/Cases OR (95% CI) ER+ OR (95% CI) ER- OR (95% CI)
Recent Oral Contraceptive (OC) Use and Breast Cancer (BC) Risk
Never 19,953/957 Ref Ref Ref
OC 1,999/145 1.8 (1.5-2.3) 2.0 (1.5-2.6) 1.4 (0.8-2.2)
Concentration of Estrogen
Low (20mcg) 228/11 1.0 (0.6-1.9) 1.4 (0.7-2.6) ----
Moderate (30-35mcg) 734/45 1.3 (1.0-1.8)* 2.1 (1.5-2.8)* ----
High (50mcg) 47/6 2.7 (1.1-6.2) 3.9 (1.6-9.4) ----
Progesterone Types
Norethindrone 403/39 2.1 (1.5-2.9)* 2.1 (1.4-3.2)* ----
Norgestimate 76/6 1.7 (0.7-3.9) 1.7 (0.6-4.9) ----
Levonorgestrel 211/11 1.1 (0.6-2.1) 1.1 (0.5-2.3) ----
*p = < 0.001
DEPARTMENT NAME
Beaber EF, Buist DSM., Barlow WE, Molone KE, Reed SD, Li CI. Cancer Res. 2014 Aug; 74(15): 4078-89WHICH ORAL CONTRACEPTIVE IS “BEST”?
• Progestin-only pill
• Patient cannot take estrogen due to medical conditions
• Breastfeeding or < 30 days postpartum
• Comorbidities with high risk of VTE (HTN, migraines with aura, clot history)
• Adverse effects from estrogen (breast tenderness, nausea, bloating)
• Combination pill
• Experience heavier menstrual bleeding
• Severe menstrual cramping
• Hormone-related comorbidities (acne, menstrual migraines, PMS)
Caution with patients on phenobarbital, phenytoin, carbamazepine,
rifampin & St. John’s Wort
DEPARTMENT NAMEHORMONAL PATCHES AND INJECTABLES DEPARTMENT NAME
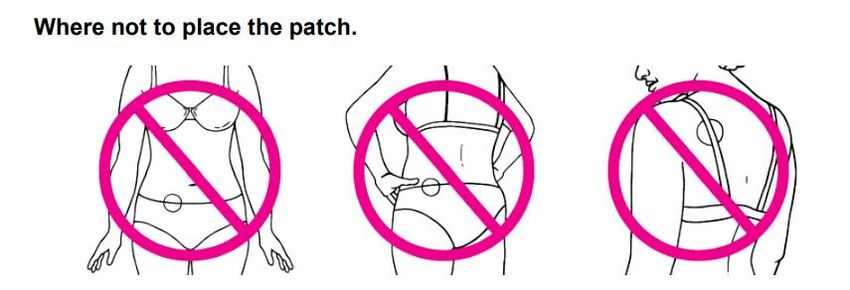
HORMONAL PATCH
• Ortho Evra™, Evra™, Xulane®
• Ethinyl estradiol 20mcg + norelgestromin 150mcg/day
• Women > 90kg show decreased contraceptive efficacy
• Improved adherence compared to COC
• Less fluctuation in serum estrogen levels
• Dosing
• One patch each week for 3 weeks (21 days)
• Follow with one week (7 days) patch-free
• Use additional form of contraception for 7 days if patch not
applied on first day of menstruation
DEPARTMENT NAME
Lexicomp Online, Pediatric and Neonatal Lexi -Drugs Online, Hudson, Ohio: Wolters Kluwer Clinical Drug Information, Inc.; 2020;
Feb 11, 2020.
Galzote RM, Rafie S, Teal R, Mody SK. Intl J Woman’s Health.2017;9:315-21.HORMONAL PATCH
Estrogen Concentration Estrogen Exposure
(mcg) Variability (AUC0-21)
Combined OC 30 +++ ----
Patch 20 + 4.5x less than COC
NuvaRing® 15 + 1.6x less than COC
• Transitioning from another contraceptive agent
• Apply patch on day next pill cycle starts, new ring insertion
or injection due
• If patch applied 7 days after previous contraceptive agent
stopped, cover with additional contraceptive agent for first
7 days of patch
DEPARTMENT NAME
Lexicomp Online, Pediatric and Neonatal Lexi-Drugs Online, Hudson, Ohio: Wolters Kluwer Clinical Drug Information, Inc.; 2020; Feb 11, 2020.
Van del Heuvel MW, et al. Contraception. 2005;72(3):168-74.
Galzote RM, Rafie S, Teal R, Mody SK. Intl J Woman’s Health.2017;9:315-21.HORMONAL PATCH
• Twirla® (FDA approved 2/14/20)
• Ethinyl estradiol 30mcg + levonorgestrel 120 mcg/day
• 7 day patch for women with BMI < 30kg/m 2
• BMI < 25kg/m2: PI score 3.5 (95% CI, 1.8-5.2)
• BMI 25-30kg/m2: PI score 5.7 (3.0-8.4)
• BMI ≥ 30kg/m2: PI score 8.6 (5.8-11.5)
• Dosing similar to other contraceptive patch
DEPARTMENT NAME
Twirla [package insert]. Grand Rapids, MI: Agile Therapeutics Inc ;2020.INJECTABLE CONTRACEPTIVES
• Depot medroxyprogesterone acetate (DMPA)
• Brand: Depo-Provera® (IM), Depo-SubQ Provera 104™
• Strengths: 150mg/mL (IM), 104mg/0.65mL (SubQ syringe)
• Dosing (contraception)
• No weight/BMI limitations
• First dose administered during first 5 days of period
• Backup contraception not indicated if within 7 days of menstruation
onset, immediately after abortion or postpartum
• Menstruation onset > 7 days, cover with additional agent for 7 days
• Depo-Provera® 150mg IM every 13 weeks/3 months
• Depo-SubQ Provera 104™ SubQ every 3 months/12-14 weeks
DEPARTMENT NAME
Lexicomp Online, Pediatric and Neonatal Lexi -Drugs Online, Hudson, Ohio: Wolters Kluwer Clinical Drug Information, Inc.; 2020;
Feb 11, 2020.INJECTABLE CONTRACEPTIVES
• Administration
• Shake vigorously prior to administration
• Injection area
• SubQ: anterior thigh or abdomen
• IM: gluteal or deltoid muscle (deep IM)
• Rotate administration site with each injection
• Transitioning from another contraceptive agent
• Depo-SubQ Provera™: administer within 7 days of discontinuing
contraceptive agent
• Depo-Provera® (IM): administer day after last active tablet, final inactive
tablet or discontinue alternative agents 7 days after IM administration
• IM to SubQ formulation: give SubQ dose 13 weeks after IM dose
DEPARTMENT NAME
Lexicomp Online, Pediatric and Neonatal Lexi -Drugs Online, Hudson, Ohio: Wolters Kluwer Clinical Drug Information, Inc.; 2020;
Feb 11, 2020.IMPLANTED SYSTEMS DEPARTMENT NAME
IMPLANTED DEVICES
• Nexplanon®
• Etonogestrel 68mg (progestin only)
• 4cm x 2mm (dia) non-biodegradable, latex-free rod
• Replace every 3 years subdermally
• Administration
• Trained healthcare professional
• Insert Day 1 to 5 of menstrual cycle – no backup required
• Use backup contraception for 7D if inserted any other time
DEPARTMENT NAME
Lexicomp Online, Pediatric and Neonatal Lexi -Drugs Online, Hudson, Ohio: Wolters Kluwer Clinical Drug Information, Inc.;
2020; Feb 11, 2020.
Image from: https://www.getthefacts.health.wa.gov.au/fun-stuff/lets-talk/everything-you-need-to-know-about-implanonIMPLANTED DEVICES: EFFICACY AND SAFETY
Population Intervention Outcome Measures Results
- Integrated ENG Implant - Cumulative Pearl - No pregnancies reported while
analysis of 11 in all subjects Index in women implant in place, 6 occurred
randomized ≤ 35 years within 14 days after removal
trials - Bleeding profiles - Including these 6 pregnancies,
- Total of 942 - Adverse event Pearl Index: 0.38
women age incidence - Infrequent bleeding (33.3%)
18-40 years amenorrhea (21.4%), prolonged
bleeding (16.9%), frequent
bleeding (6.1%)
- Discontinuation for SE:
emotional liability (2.3%), weight
gain (2.3%), headache (1.6%),
acne (1.3%), depression (1%)
DEPARTMENT NAME
Darney P, et al. Fertil Steril. 2009 May;91(5):1646-53.INTRAUTERINE SYSTEMS DEPARTMENT NAME
DEPARTMENT NAME
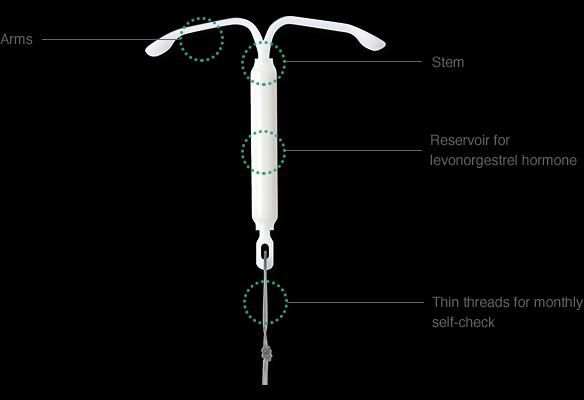
INTRAUTERINE SYSTEMS
Duration of Use Levonorgestrel dose Levonorgestrel dose
IUS Size (mm)
(years) (total mg) (mcg/day)
Skyla® 3 13.5 6 28 x 30
Kyleena® 5 19.5 9 28 x 30
Liletta® 6 52 14.3 32 x 32
Mirena® 5 52 20 32 x 32
Paragard® 10 None None 32 x 36
DEPARTMENT NAME
IUS = Intrauterine system
Lexicomp Online, Pediatric and Neonatal Lexi -Drugs Online, Hudson, Ohio:
Wolters Kluwer Clinical Drug Information, Inc.; 2019; Dec 17, 2019.IUS: EFFICACY
• Pregnancy rate 0.5 per 100 users
• Levonorgestrel IUDs found to have comparable efficacy to
copper IUDs
• Can be used in nulliparous, postpartum, or post-
abortion patients
• Nulliparous users are not at increased risk for infection or
infertility compared to multiparous users
• Safety and acceptability of levonorgestrel IUDs found
to be equivalent to oral contraceptives
DEPARTMENT NAME
Backman T, et al. Am J Obstet Gynecol. 2004 Jan;190(1):50-4.
French R, et al. Cochrane Database Syst Rev. 2004;(3):CD001776. Review.
Prager S, et al. Contraception. 2007 Jun;75(6 Suppl):S12-5. Epub 2007 Apr 3. Review.
Suhonen S, et al. Contraception. 2004 May;69(5):407-12.IUS: ADVERSE EFFECTS • Headache • Acne • Breast tenderness • Irregular bleeding • Mood changes • Cramping or pelvic pain • Expulsion DEPARTMENT NAME
IUS VS. COC
Population Intervention Outcome Measures Results
- 200 women LNG-IUS Group: - Discontinuation rates - Discontinuation 20% in
- Age 18-25 - 94 subjects - Reasons leading to LNG vs. 27% in COC
years COC Group: discontinuation (p=0.28)
- 99 subjects - Adverse event - Pain was the most
incidence common
- Menstrual discontinuation reason
questionnaires in LNG group
- Subjective well-being - Hormonal SE most
and sexual behavior common
discontinuation reason
in COC group
DEPARTMENT NAME
Suhonen S, et al. Contraception. 2004 May;69(5):407-12.
LNG-IUS = levonorgestrel intrauterine system, COC = combined oral contraceptiveIUS: CANCER RISK
Breast cancer
Increased
Incidence
Decreased Cervical cancer
Incidence
Ovarian cancer
Endometrial cancer
DEPARTMENT NAME
Lassise DL, et al. Int J Epidemiol. 1991 Dec;20(4):865-70.
CortessisVK, et al. Obstet Gynecol. 2017 Dec;130(6):1226-1236.
Wheeler LJ, et al. Obstet Gynecol. 2019 Oct;134(4):791-800.
Hormonal Contraception and Risk of Breast Cancer. American College of Obstetrics and
Gynecology Practice Advisory. 2018 Jan.LONG ACTING REVERSIBLE CONTRACEPTION (LARC) DEPARTMENT NAME
DEPARTMENT NAME
Adapted from https://www.your-life.com/en/contraception-methods/long-acting-contraception/RECOMMENDATION FOR ADOLESCENTS
“Expanding access to LARC for young
IOM women has been declared a national
priority”
ACOG “Should be considered as first-line
choices for both nulliparous and
2007
parous adolescents”
AAP “LARC methods should be considered
first-line contraceptive choices for
2014
adolescents”
DEPARTMENT NAME
Finer, Fertil Steril. 2012 Oct;98(4):893-7
Committee on Adolescence. American Academy of Pediatrics. 2014 Oct;134(4)e1244-e1256.ADOLESCENT USE OF LARC
Population Intervention Outcome Measures Results
- 12 studies - IUD or - 12-month - 74% continuation of IUD
- 4886 women implant continuation - 84% continuation of implant
< 25 years rates
- Young women have a high 12-month continuation of
LARC
- Intrauterine devices and implants should be
considered first-line in adolescents
DEPARTMENT NAME
DiedrichJT, et al. Am J Obstet Gynecol. 2017 Apr;216(4):364.e1-364.e12.BARRIERS TO LARC
• Concern about safety
• Risk of STIs
• Providers not trained in IUD insertion
• IUDs not available at site
• Reimbursement challenges
• Knowledge
• 80% of adolescents surveyed had not heard of IUD
• Opportunity – CHOICE Project in St. Louis, MO
• Educated about LARC
• Provided all methods without cost
• 62% of adolescents (15-19 years) chose LARC
DEPARTMENT NAME
Tyler, Obstet Gynecol. 2012;119(4):762-71
Madden, Contraception. 2010;81(2):112.-6
Holland, Womens Health Issues. 2015;25(4):355-8
Whitaker, Contraception 2008;78:211.
Mestad, Contraception 2011;84:493.AAP RECOMMENDATIONS ON COUNSELING
• Confidentiality and consent
• Best practice guidelines: confidentiality around sexuality
and STIs and minor consent for contraception
• Sexual history taking
• 5 P’s: partners, prevention of pregnancy, protection from
STIs, sexual practices, and past history of STIs and
pregnancy
• Counseling about abstinence and contraceptives
• Follow-up
DEPARTMENT NAME
Committee on Adolescence. Contraception for adolescents. Pediatrics. 2014 Oct;134(4):e1244-56.
STI: sexually transmitted infectionDEPARTMENT NAME
CLINICAL PEARLS
• Patient preference and expected compliance should guide
therapy choice
• Implantable and IUDs are associated with less unexpected
pregnancies
• More stable hormonal serum levels throughout day
• Decreased compliance issues
• Certain contraceptive agents have BMI/weight limitations
• Small increased risk of breast cancer & cervical cancer
with COC
DEPARTMENT NAMEDon’t Fail Me Now: Hormonal Contraceptives Courtney Kain, PharmD, BCPPS Emily Rodman, PharmD, BCPPS DEPARTMENT NAME
You can also read