Down Syndrome Disintegrative Disorder: A Clinical Regression Syndrome of Increasing Importance
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Down Syndrome Disintegrative
Disorder: A Clinical Regression
Syndrome of Increasing Importance
Mattia Rosso, MD,a Ellen Fremion, MD,b Stephanie L. Santoro, MD,c,d Nicolas M. Oreskovic, MD, MPH,c Tanuja Chitnis, MD,a
Brian G. Skotko, MD, MPP,c,d Jonathan D. Santoro, MDe,f
Downloaded from http://publications.aap.org/pediatrics/article-pdf/145/6/e20192939/1079455/peds_20192939.pdf by guest on 17 December 2021
Down syndrome disintegrative disorder (DSDD), a developmental regression abstract
in children with Down syndrome (DS), is a clinical entity that is characterized
by a loss of previously acquired adaptive, cognitive, and social functioning in
persons with DS usually in adolescence to early adulthood. Initially reported
in 1946 as “catatonic psychosis,” there has been an increasing interest among a
Ann Romney Center for Neurologic Diseases, Harvard
the DS community, primary care, and subspecialty providers in this clinical Medical School, Harvard University and Brigham and
area over the past decade. This condition has a subacute onset and can Women’s Hospital, Boston, Massachusetts; bInternal
Medicine-Pediatrics Program, Baylor College of Medicine,
include symptoms of mood lability, decreased participation in activities of Houston, Texas; cDivision of Medical Genetics and
daily living, new-onset insomnia, social withdrawal, autistic-like regression, Metabolism, Department of Pediatrics, Massachusetts
General Hospital, Boston, Massachusetts; dDepartment of
mutism, and catatonia. The acute phase is followed by a chronic phase in Pediatrics, Harvard Medical School, Harvard University,
which baseline functioning may not return. No strict criteria or definitive Boston, Massachusetts; eDepartment of Neurology,
Children’s Hospital Los Angeles, Los Angeles, California; and
testing is currently available to diagnose DSDD, although a comprehensive f
Keck School of Medicine, University of Southern California,
psychosocial and medical evaluation is warranted for individuals presenting Los Angeles, California
with such symptoms. The etiology of DSDD is unknown, but in several Drs Rosso and J.D. Santoro conceptualized and
hypotheses for regression in this population, psychological stress, primary designed the structure of the review, drafted the
psychiatric disease, and autoimmunity are proposed as potential causes of manuscript, and revised the manuscript; Drs
Fremion, S.L. Santoro, and Skotko drafted the
DSDD. Both psychiatric therapy and immunotherapies have been described as manuscript and revised the manuscript for
DSDD treatments, with both revealing potential benefit in limited cohorts. In intellectual content; Drs Oreskovic and Chitnis
this article, we review the current data regarding clinical phenotypes, critically reviewed and revised the manuscript for
important intellectual content; and all authors
differential diagnosis, neurodiagnostic workup, and potential therapeutic
approved the final manuscript as submitted and
options for this unique, most disturbing, and infrequently reported disorder. agree to be accountable for all aspects of the work.
DOI: https://doi.org/10.1542/peds.2019-2939
Accepted for publication Nov 13, 2019
Down syndrome (DS) is the most implications on both quality of life Address correspondence to Jonathan D. Santoro,
MD, Department of Neurology, Children’s Hospital Los
common cause of intellectual disability and the autonomy of persons with
Angeles, 4650 Sunset Blvd, Mail Stop 82, Los Angeles,
worldwide and occurs in ∼1 in 800 DS.4 It is, therefore, key for all CA 90027. E-mail: jdsantoro@chla.usc.edu
live births; it is most frequently caused providers to be aware of DSDD to PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online,
by trisomy of chromosome 21 due to evaluate and potentially treat this 1098-4275).
nondisjunction or translocation condition. The etiology, Copyright © 2020 by the American Academy of
events.1–3 In recent years, multiple pathophysiology, and therapeutic Pediatrics
centers have reported a specific options for DSDD are currently unclear, FINANCIAL DISCLOSURE: The authors have indicated
pattern of developmental regression although clinical data are rapidly they have no financial relationships relevant to this
in individuals with DS, wherein emerging. Our focus for this review is article to disclose.
patients lose language, behavioral, to summarize the current knowledge of FUNDING: No external funding.
and cognitive skills that they previously clinical features, potential etiologies,
acquired.4,5 This condition has been neurodiagnostic workup, and To cite: Rosso M, Fremion E, Santoro SL, et al.
more recently referred to as Down therapeutic options and to identify Down Syndrome Disintegrative Disorder: A
Clinical Regression Syndrome of Increasing
syndrome disintegrative disorder future areas of focus and research in
Importance. Pediatrics. 2019;145(6):e20192939
(DSDD). DSDD can be severe, with this field.
PEDIATRICS Volume 145, number 6, June 2019:e20192939 STATE-OF-THE-ART REVIEW ARTICLEHISTORICAL REPORTS TABLE 1 Characteristics of DSDD
6 Criterion Features
In 1946, Rollin described a cohort of
73 institutionalized adolescents and I Autistic regression
young adults with DS, 17 (23.3%) of II Cognitive decline resulting in a dementia-like state
III Older age at onset than at autistic regression
whom were diagnosed with
IV No other diagnosis that may explain the condition
“catatonic psychosis.” These
Adapted from Worley G, Crissman BG, Cadogan E, Milleson C, Adkins DW, Kishnani PS. Down syndrome disintegrative
individuals had an appropriate disorder: new-onset autistic regression, dementia, and insomnia in older children and adolescents with Down syndrome.
developmental period followed by J Child Neurol. 2015;30(9):1147–1152.
behavioral changes, including
agitation and harm directed toward
self and others, during early Statistical Manual of Mental Disorders also reported and include depression
Downloaded from http://publications.aap.org/pediatrics/article-pdf/145/6/e20192939/1079455/peds_20192939.pdf by guest on 17 December 2021
adolescence (ages 11–14) that led criteria of autism spectrum disorder (42%), social withdrawal (34%), and
their families to seek institutional to aid in standardization of anxiety (16%).5,12,13 In recent
care. Afterward, they experienced phenotypic description for the latter studies, catatonia was observed in
a deterioration phase marked by phenomenon.4,9 Diagnosis by using 47% of cases labeled as DSDD, which
incontinence, mutism, apathy, social these guidelines involves new-onset is higher than rates originally
withdrawal, occasional behavioral impairments in social interaction; reported by Rollin6 (38%).5,11,12
outbursts, and psychosis, eventually communication; stereotyped patterns New-onset insomnia was also
leading to catatonia. of movement, behavior, and thought; described in 43% of cases.4,5,7,11,12
and developmental delays.9 At Pooled estimates from 4 studies
In 2000, Kerbeshian and Burd7 baseline, autism can be present in revealed a 14% rate of psychotic
provided a clinical description of roughly 15% of children with DS; symptoms, including delusions and
autistic-like regression in a child with however, a previous diagnosis of hallucinations, in persons with
DS. In this study, the authors autism was not observed in any of the DSDD.4,5,11,12 Aggressive behavior
described an 8-year-old girl with DS studies reviewed in this report.10 was reported in 42% of
who experienced autistic regression DSDD is an entity that is believed to patients.2,5,11,13 As was highlighted by
(loss of social and communication be distinct and separate from autism Mircher et al,5 aggression in persons
skills), loss of cognitive functions, and spectrum disorder. with DSDD may be directed toward
a rapid-onset insomnia, referring to self (auto-aggression) or others
this condition as autistic-like Beyond regression, symptoms of (hetero-aggression). A minority of
regression.7 Subsequently, in 2015, DSDD can be heterogenous and are patients with DSDD (12%) also had
Worley et al4 presented similar case reported with variability (Table 2). In anorexia as part of their clinical
reports and characterized DSDD as 3 large studies, up to 87% of patients presentation.11,12
a subacute onset of “autistic with DSDD were diagnosed with
regression,” cognitive decline language regression, with symptoms Because there are no diagnostic
resulting in a dementia-like state, ranging in severity from dysfluency to criteria available, DSDD is best
occurring at an older age typical for mutism.5,11,12 Among patients in described as a clinical syndrome that
autistic regression, and no other whom severity of language regression should be considered in adolescents
established diagnosis to explain the was quantified, 38% had partial and young adults with DS and
condition (Table 1).8 language regression and 52% had subacute-onset behavioral
mutism.5,11,12 Mood symptoms are changes.13 It is also key to appreciate
CLINICAL MANIFESTATIONS
TABLE 2 Clinical Features Reported in DSDD
The demographic profile of DSDD Clinical Feature % (n/N)
includes a postpubertal onset and an
Language regression5,11,12 87 (42/48)
elevated female/male patient ratio of Partial 38 (18/48)
2:1.4,5 A defining feature of DSDD is Mutism 52 (25/48)
regression of previously attained Catatonia2,5,11,12 47 (25/53)
skills, notably in the domains of Mood symptoms2,5,12,13
language, communication, and social Depression 42 (21/50)
Social withdrawal 34 (15/44)
skills. No formal criteria exist within Anxiety 16 (8/50)
the diagnosis of DSDD to define either Insomnia4,5,11,12 43 (25/58)
regression or autistic-like behavioral Aggression2,5,11,13 42 (17/40)
regression; however, some groups Delusions or hallucinations4,5,11 14 (8/56)
have used the Diagnostic and Anorexia11,12 12 (5/43)
2 ROSSO et althat persons with DS may experience The imaging features of DSDD are a postpubertal onset and an elevated
adaptive, social, or cognitive heterogenous, and no defining female/male patient ratio of 2:1 in
regression for reasons other than characteristics have been identified. the 2 largest studies to date.4,5 This
DSDD, making a complete workup Across 5 studies, abnormal MRI finding has raised the suspicion that
critical in the assessment of these findings were found in 26% of inflammation may play a role in the
patients (see Evaluation and patients (n = 9 of 35).4,5,11,12 The etiology of DSDD because this
Differential Diagnosis). Compared imaging findings were described to be demographic is mirrored in other
with the typical onset of autistic dementia-like in 2 cohorts in which inflammatory disorders such as
regression in persons with DS, DSDD hippocampal atrophy was reported in multiple sclerosis and autoimmune
takes place when patients are older, 20% of patients (n = 4 of 20).5,12 In encephalitis.4,5,13,15 Additionally,
typically between the first and third other studies, there has been a failure recent research has revealed the
Downloaded from http://publications.aap.org/pediatrics/article-pdf/145/6/e20192939/1079455/peds_20192939.pdf by guest on 17 December 2021
decade.4,13 The acute regression to find any imaging findings presence of other autoantibodies,
appears to last for ∼6 months and is associated with DSDD, which may such as antinuclear antibodies, anti-
followed by a chronic phase in which reflect the significant heterogeneity of microsomal antibodies, striational
previous skills may not be the study cohorts.2,4,11 antibodies, thyroperoxidase
completely recovered (Table 3). In 2 antibodies, and anti-tissue
studies, it has been reported that transglutaminase antibodies, which
58% of persons with DSDD THEORIES ON ETIOLOGY have elevated levels in some
experience a partial or total recovery. Whereas the etiology of DSDD is not individuals with DSDD.11 These
Only 7.5% of patients experience fully understood, 2 possible causes findings may be understood as
additional worsening, whereas 35% that have been proposed are immune a consequence of DS, which is
of patients stabilize.4,5 However, in dysregulation and psychological generally associated with high serum
patients with stabilizing DSDD, stress triggering neuropsychiatric levels of proinflammatory cytokines,
a complete recovery to the presentations (analogous to Rollin’s6 high rates of complement protein
premorbid baseline condition original report). The demographic consumption, and various other
appears to be infrequent.2,4 profile of DSDD includes forms of immune dysregulation.16 As
TABLE 3 Studies of Patients With Clinical Phenotypes Similar to DSDD
Authors, Year Design Patient Population Summary of Results
6
Rollin, 1946 Case series 17 cases of DS with catatonic psychotic living in Description of a period of behavioral agitation followed by decompensation
an institution characterized by incontinence, mutism, apathy, social withdrawal,
occasional behavioral outbursts, and psychosis eventually leading to
catatonia
Kerbeshian and Case series 5 cases of DS and Tourette’s syndrome, 1 case Description of new-onset insomnia, autism, and loss of cognitive skills in
Burd,7 2000 of childhood disintegrative disorder and DS a patient with DS
Prasher,8 2002 Case series 357 patients with DS DSDD regression is severe and gradual, lasting 2 y and followed by
a chronic plateau; regression affected language, social, and cognitive
domains
Castillo et al,14 Case- 24 patients with DS and autism 50% (12 of 24) of patients with DS and autism lost previously acquired
2008 control language, social skills, and communicative abilities; language loss
study occurred later in DS with autistic regression than in isolated autistic
regression (62 vs 20 mo)
Akahoshi et al,12 Case series 13 young adults with DS with acute Patients with DS presented with depression, obsessive-compulsive
2012 neuropsychiatric symptoms behaviors, delusions, and hallucinations
Worley et al,4 2015 Case series 11 patients with DSDD Late mean age of onset of DSDD (mean = 11.4 y); autism was new in onset
in 8 of 11 patients and worsened in 3 of 11 patients; 91% (10 of 11)
patients had cognitive decline; s82% (9 of 11) patients had new-onset
insomnia
Ghaziuddin et al,2 Case series 4 patients with DS and regression Regression was accompanied by motor symptoms, including catatonia;
2015 recovery after a therapy with benzodiazepines and ECT
Jacobs et al,13 Case report Young adult male with DS 19-y-old patient presents with severe clinical deterioration; the patient
2016 presented with low mood, difficulty concentrating, anxiety, and motor
symptoms
Mircher et al,5 Case series 30 patients with DS and regression Regression was seen at all levels of cognitive functions; regression was
2017 characterized by partial or total loss of activities of daily living;
regression was associated with other psychiatric symptoms, which
included catatonia, depression, delusions, and stereotypical behaviors;
regression was preceded by severe emotional stress in all patients
PEDIATRICS Volume 145, number 6, June 2019 3the autoimmune etiology of several TABLE 4 Autoimmune Characteristics of DSDD
psychiatric syndromes becomes Authors, Year Patient Population Summary of Results
increasingly accepted, researchers Worley et al,4 11 patients with Anti-thyroperoxidase antibody levels were elevated in 91% of
speculate that some cases of DSDD 2015 DSDD patients with DSDD (10 of 11) vs 23% of patients with DS (5 of
may be driven by autoimmunity.17,18 21) (P , .001)
Jacobs et al,13 Young adult male Negative results on autoimmune panel
Elevated serum and cerebral spinal 2016 with DS
fluid levels of anti-thyroperoxidase Cardinale et al,11 4 patients with Anti-thyroperoxidase antibodies (n = 3 of 4), anti-TSH antibodies
antibodies found in some patients 2019 DSDD (n = 2 of 4), anti-microsomal antibodies (n = 2 of 4), anti-tTg
with DSDD have led some researchers antibodies (n = 1 of 4), antinuclear antigen antibodies (n = 1
of 4), anti-striational antibodies (n = 1 of 4)
to propose Hashimoto encephalopathy
anti-TSH, anti–thyroid-stimulating hormone antibodies; anti-tTg, anti-tissue transglutaminase.
(HE) as an underlying etiology. Across
Downloaded from http://publications.aap.org/pediatrics/article-pdf/145/6/e20192939/1079455/peds_20192939.pdf by guest on 17 December 2021
4 studies, 35% of persons with DSDD
(n = 16 of 46) had high titers of anti-
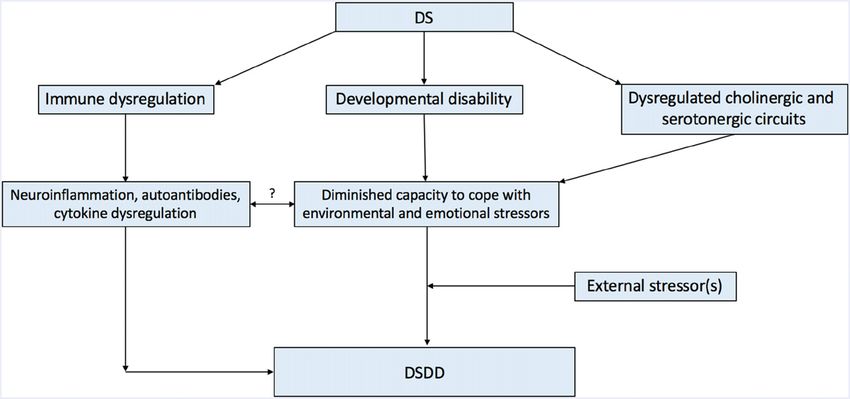
the largest study of 30 patients, An exact etiology of DSDD remains
thyroperoxidase antibodies, although
Mircher et al5 described a new school difficult to identify, although
the agreement between these studies
environment as the most common life components of immune
is considered poor because rates range
stressor preceding a diagnosis of dysregulation, psychiatric symptoms
from as low as 20% (Mircher et al,5
DSDD (51%).11,22 Other common in persons with intellectual disability,
n = 15 tested) to as high as 82%
stressors were awareness of disability and dysregulated cholinergic and
(Worley et al,4 n = 11 tested).11,13
triggered by the wedding or departure serotonergic circuits may be involved
Epidemiological studies have revealed
of a sibling (23%), assault (17%), (Fig 1). Although the role of
that thyroid disease has a greater
illness of a close one (13%), and inflammation in neuropsychiatric
prevalence in patients with DSDD than
overstimulation (10%).5 Although disease continues to evolve, the
in the general population.4 In addition,
notable, many children with DS combination of neuroinflammation,
the rates of thyroid disease increase
experience similar stressful triggers autoantibody generation, and/or
with time, as does the prevalence of
and do not have similar cytokine dysregulation could
thyroperoxidase antibodies, with rates
neuropsychiatric changes, rendering interface with existing psychological
up to 22% in asymptomatic patients.19
stress-related triggers an incomplete capacities to cope with external
The significance of anti-
explanation. Stein et al22 also reported stressors and the baseline circuity of
thyroperoxidase antibodies is unclear
on the role of environmental changes these responses. For this reason,
because steroid therapy, the gold
as potential triggers for regression in additional investigation into the cause
standard treatment of HE, has
DSDD. In their case study, the authors of this potentially polyfactorial
revealed no clinical benefit in DSDD.4
reported that a patient with DS phenomenon is needed.
HE also differs from DSDD because it
developed reactive depression after
presents with seizures, headaches,
moving to a new city and changing
hallucinations, and ataxia. Although EVALUATION AND DIFFERENTIAL
schools.23 The authors postulated that
HE can present as an isolated
the patient dealt with distress through DIAGNOSIS
psychiatric illness, this presentation is
complex behavioral and adaptive At this time, DSDD is best described
rare in children.20,21 Thus, additional
changes because she failed to express as a constellation of symptoms
studies are needed to fully elucidate
her distress with the usual verbal without a distinct etiology. Thus,
the pathologic role of anti-
channels.22 This description would clinicians should pursue
thyroperoxidase antibodies in patients
exist on the spectrum of an acute a comprehensive psychosocial and
with both DS and DSDD (Table 4).
stress reaction as opposed to medical evaluation of potential
An alternative hypothesis proposes a primary psychiatric disease and thus secondary causes of behavioral
that psychological stress may act as may explain the recovery noted in change and regression. In their
a trigger of regression in DSDD (Fig 1). patients over time. Mircher et al5 put article, Jacobs et al13 provide
In their studies, Stein et al22 and forth a hypothesis that explains the a suggested diagnostic workup for
Mircher et al5 postulated that such susceptibility in terms of widespread such cases organized in 5 different
behavioral changes may be a way for dysregulation of serotoninergic and tiers of testing (Table 5). The first 2
persons with DS to express distress in cholinergic circuits. If this were the tiers are common causes of a new
the context of their developmental case, DSDD may be amenable to onset of psychiatric symptoms in
delays. Across 3 studies, 86% of treatment with selective serotonin young adults with DS, which include
persons with DSDD (n = 30 of 35) reuptake inhibitors (SSRIs), which psychosocial stressors, depression,
reported identifiable life stressors have only been explored in a few electrolyte disturbances, infections,
preceding the onset of symptoms. In studies thus far.24,25 liver disease, thyroid disorders, and
4 ROSSO et alDownloaded from http://publications.aap.org/pediatrics/article-pdf/145/6/e20192939/1079455/peds_20192939.pdf by guest on 17 December 2021
FIGURE 1
Diagram of proposed DSDD pathophysiology.
immunologic disorders. Common adults. These syndromes are disorder, and anxiety disorders, may
co-occurring conditions associated characterized by an inability to have symptoms that mimic
with DS should also be considered process certain metabolites, including a regression.27 These disorders should
such as sleep apnea, acid reflux, celiac amino acids, fatty acids, or organic be evaluated thoroughly because they
disease, and constipation. Another acid. A final differential diagnosis to unify the presence of environmental
diagnosis in tier 2 is pediatric acute- be aware of is Lesch-Nyhan triggers and associated
onset neuropsychiatric syndrome, syndrome, the presentation of which neuropsychiatric disease, although
which displays some overlap with may closely resemble DSDD, except diagnosis can be challenging in
DSDD. Persons with pediatric acute- that onset is typically in infancy or persons with intellectual disability.28 A
onset neuropsychiatric syndrome early childhood. Patients with Lesch- key point to consider is that the
may present with a subacute onset of Nyhan syndrome present with presence of mild baseline psychiatric
abnormal motor movements, tics, and a combination of a regression of disease and exposure to stressful
obsessive-compulsive symptoms, intellectual skills, dystonic triggers may yield regression-like
although caution should be exercised movements, and compulsive self- symptoms, although this likely exists
before making this diagnosis, as well, mutilation because of a failure of along a complex spectrum. One final
given the heterogenous diagnostic purine metabolism.26 These genetic
important differential diagnosis to
and clinical criteria. conditions typically present in early
consider is early-onset Alzheimer
childhood rather than adolescence
Multiple genetic conditions can occur disease (AD), which continues to be an
and young adulthood like DSDD, but
in the same patient, and because DS is important differential for patients with
delayed diagnosis is plausible.
one of the most common genetic DSDD.11 Early-onset AD is common in
disorders, evaluation for other Finally, it is important to note that DS patients with DS owing to the 3 copies
genetic disorders should be is associated with several psychiatric of chromosome 21 (and thus 3 copies
considered. Two important diagnoses conditions. As previously mentioned, of amyloid precursor protein genes)
to evaluate for are Fragile X DSDD differs from other forms of carried by these patients. Early-onset
syndrome and Rett syndrome, which autistic regression in the later age at AD differs from DSDD because of the
are 2 important genetic causes of onset, high female/male patient ratio, later onset between the ages of 40
regression in early childhood. By the and presence of additional symptoms and 60 years and its steady and
same token, inborn errors of such as insomnia and catatonia.4,5 In irreversible decline, as opposed to
metabolism are possible causes of the presence of stressful triggers, the subacute and partially reversible
regression and behavioral primary psychiatric disorders, such as decline observed in DSDD.29 However,
abnormalities in children and young major depressive disorder, bipolar AD onset may occur earlier than age
PEDIATRICS Volume 145, number 6, June 2019 5TABLE 5 Proposed Diagnostic Workup for Regression in Patients With DS sertraline), and anticholinergic drugs
Tier Diagnosis Evaluation (eg, donepezil and rivastigmine) have
Tier Thyroid disorders: hypothyroidism, TSH, fT4, thyroperoxidase antibodies, thyroglobulin
been used to address many of the
1 hyperthyroidism, HE antibodies neuropsychiatric disturbances
Electrolyte disturbance, infections, Electrolytes, CBC, LFTs observed in DSDD.4 In 3 recent
liver disease studies, 25% of patients showed
Vitamin deficiency Folate, vitamin B12, 25-OH vitamin D a response to SSRIs, which seem to
Celiac disease Anti-tTg, total IgA
Obstructive sleep apnea Polysomnography improve mood symptoms, motor
Hearing loss Hearing test symptoms, and sleep
Vision loss (cataracts, ulcers, etc) Vision screen disturbance.12,31 Tamasaki et al31
Constipation Abdominal radiograph reported a case study of a 14-year-old
Downloaded from http://publications.aap.org/pediatrics/article-pdf/145/6/e20192939/1079455/peds_20192939.pdf by guest on 17 December 2021
Depression Depression screen
boy with DSDD symptoms who was
Stress and anxiety Screen for stressors
Other psychiatric disorders Psychiatric referral treated with donepezil, which led to
Other neurologic disorders Brain MRI a complete psychosocial recovery;
Tier Lyme disease Serological testing however, the efficacy of cholinergic
2 medications for cognitive impairment
PANDAS Antistreptolysin O
in individuals with DS is debatable,
Seizure disorder EEG
Other immunologic disorders Antinuclear antibodies, ESR, CRP and they are not US Food and Drug
Syphilis, HIV RPR, HIV serology Administration approved for children
Tier Fragile X syndrome Fragile X syndrome testing and adolescents.32,33 Another
3 therapeutic option for persons with
Rett syndrome Methyl CpG binding protein 2
DSDD is antipsychotic treatment.
Heavy metal toxicity Serum levels of lead, manganese, mercury, zinc, nickel,
thallium Across 4 studies, 70% of patients
NMDA receptor encephalitis Anti-NMDA receptor autoantibodies experienced at least some
Microdeletion or microduplication Chromosomal microarray improvement in motor symptoms,
syndrome sleep disturbance, and catatonia with
Tier Aminoacidopathies Plasma amino acids
antipsychotic therapy.2,12,13
4
Organic acidurias Urine organic acids, urine acylglycines
Fatty acid oxidation disorders Plasma acylcarnitines Ghaziuddin et al2 reported that high-
Mitochondrial disorders Pyruvate, lactates dose benzodiazepines, such as
Urea cycle disorders Ammonia lorazepam, could benefit patients
Ovarian teratoma (limbic encephalitis) Ovarian ultrasound with DSDD and catatonia. Across 4
Tier Lesch-Nyhan syndrome Hypoxanthine-guanine phosphoribosyl transferase
studies, 91% of patients with DSDD
5 gene mutation
Porphyria Aminolevulinic acid, porphobilinogen, and catatonia demonstrated at least
hydroxymethylbilane synthase gene mutation a partial response to
Congenital disorders of glycosylation Carbohydrate deficient transferrin benzodiazepines; however, catatonia
Peroxisomal storage disorders Very long chain fatty acids, phytanic acid, was unresponsive to benzodiazepines
plasmalogens
Lysosomal storage disorders Urine glycosaminoglycans, urine oligosaccharides,
in only 1 patient.2,11–13
urine sialic acid Electroconvulsive therapy (ECT) has
Other genetic disorders Whole exome sequencing also been shown as an effective
anti-tTg, anti-tissue transglutaminase; CBC, complete blood cell count; CRP, C-reactive protein; ESR, erythrocyte sedi- therapy for DSDD with catatonia that
mentation rate; fT4, free thyroxine; IgA, immunoglobulin A; LFT, liver function test; NMDA, N-methyl D-aspartate; PANDAS, warrants careful consideration by
pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections; RPR, rapid plasma regain;
clinicians.2 However, ECT can have
TSH, thyroid-stimulating hormone; 25-OH, 25-hydroxycholecalciferol.
several complications, including the
requirement of sedation, the potential
40 and may be exacerbated by factors also the need for choosing the most for memory impairment and
similar to those reported in DSDD.30 appropriate intervention. neurocognitive sequelae, and the
need for repeated ECT sessions to
Of note, the diagnosis of DSDD is maintain symptom remission; thus, it
based on clinical phenotype, and for THERAPEUTIC INTERVENTIONS FOR should be considered in conjunction
this reason, it is important to realize DSDD with specialists experienced with its
that this syndrome may be produced Several therapies have revealed some use in DS.34 In a recent case report,
by multiple causes. This is a necessary clinical benefit in patients with DSDD. administering high doses of the
consideration regarding not only the Symptomatically, antipsychotics (eg, antipsychotic clozapine was the only
need for a standardized workup but risperidone), SSRIs (eg, fluoxetine and effective treatment of catatonia and
6 ROSSO et alTABLE 6 Previously Reported Experimental Therapies in DSDD
Authors, Year Design Patient Population Summary of Results
Akahoshi et al,12 Case 13 young adults with DS with acute A total of 10 of 11 patients responded to pharmacotherapy, and marked improvements
2012 series neuropsychiatric symptoms were seen in 3 of 11; attempted pharmacotherapy included fluvoxamine, amantadine,
haloperidol, and benzodiazepines
Ghaziuddin Case 4 patients with DS and regression High-dose lorazepam and ECT were associated with the improvement of catatonia; SSRIs,
et al,2 2015 series mood stabilizers, antipsychotics, and antiepileptic drugs resulted in no change or
worsening of symptoms
Jacobs et al,13 Case Young adult male with DS Antipsychotics exacerbated the patient’s catatonia; trazodone and high-dose
2016 report benzodiazepines had no therapeutic benefit; the patient benefited from clozapine,
which brought him back to 85% of his baseline status (as reported by the patient’s
mother)
Downloaded from http://publications.aap.org/pediatrics/article-pdf/145/6/e20192939/1079455/peds_20192939.pdf by guest on 17 December 2021
Tamasaki et al,31 Case Male teenager with DS Initiated escitalopram after immune therapy with IV methylprednisolone and
2016 report anticatatonia therapies; improvement over 4-wk period, although continued autistic
features; initiated donepezil, with improvement in autistic features over an additional
4 wk
Cardinale et al,11 Case 4 patients with DSDD Immunotherapy improved catatonia, insomnia, autism severity, cognitive decline, and
2019 series psychosis in DSDD; regimens included IV and oral steroids, IV immunoglobulins,
mycophenolate, and rituximab
IV, intravenous.
was started after other treatment hypothesis of an immunologic classes of therapies have revealed
options were exhausted.13 It is crucial component in the pathophysiology of some clinical benefit (ie,
to consider that catatonia may be DSDD for individuals with positive benzodiazepines and ECT for catatonia
a symptom of DSDD because it may be autoantibody screening results, but in and SSRIs for mood symptoms), but
easily mistaken for schizophrenia or this study, a limited cohort was a standardized treatment guideline
another psychiatric disorder (Table 6).2 analyzed, and additional studies with should be developed. Future studies
larger cohorts are needed.4 However, will also be needed to elucidate the
Newer therapies have been proposed as noted above, the presumed role of immune dysregulation in DSDD
that target the hypothesized etiology may differ between cases; and the effectiveness of
autoimmunity etiology of DSDD. thus, the choice of therapeutic immunotherapies in larger cohorts.
Cardinale et al11 explored the use of intervention should mirror this
various immunotherapeutic regimens Molecular biomarkers and radiologic
because multiple causes could hallmarks also need to be identified
in 4 patients with DSDD who had produce the same clinical phenotype.
positive serum autoantibody that correlate with the clinical
screening results. Different regimens findings. Additionally, truly
separating the symptoms of DSDD
were attempted because of the side FUTURE DIRECTIONS
effects associated with many of these from chronic comorbidities
DSDD is a recently redefined associated with DS will be
treatments, which required treatment
constellation of symptoms, including a necessary component of future
discontinuation in many instances.
mood lability, socio-communicative analysis. Finally, prospective studies
The regimens included intravenous
regression, loss of activities of daily are needed to understand the long-
and/or oral steroids, mycophenolate
living, psychomotor changes, and term prognosis and the effectiveness
mofetil, intravenous
insomnia, which may permanently of therapies for this unique and
immunoglobulins, and rituximab. The
alter the adaptive and social functions troubling condition.
clinical benefit in the domains of
of persons with DS.4–6 Both patients
hallucinations, mood, autistic
and families are impacted by this
features, and insomnia was
condition. Additional research is ABBREVIATIONS
immediate in 3 of 4 patients, whereas
urgently needed with particular focus
1 patient showed a clinical AD: Alzheimer disease
on identification of the
improvement in ∼3 months.11 DS: Down syndrome
pathophysiology of the syndrome and
Catatonia was present in all patients DSDD: Down syndrome
the interplay between DSDD and
who responded completely to disintegrative disorder
other chronic comorbidities seen in
immunotherapy. Approximately 50% ECT: electroconvulsive therapy
patients with DS.
of patients experienced an HE: Hashimoto encephalopathy
improvement in sleep disturbance Prospective studies are needed to SSRI: selective serotonin reuptake
and autistic behaviors. These results identify the effective therapies for each inhibitor
may lend more credence to the of the symptoms in DSDD. Several
PEDIATRICS Volume 145, number 6, June 2019 7POTENTIAL CONFLICT OF INTEREST: Dr Skotko has received payment for expert witness testimony related to Down syndrome (but not Down syndrome disintegrative
disorder); the other authors have indicated they have no potential conflicts of interest to disclose.
REFERENCES
1. Stoll C, Alembik Y, Dott B, Roth MP. 11. Cardinale KM, Bocharnikov A, Hart SJ, think Hashimoto encephalopathy. Acta
Recent trends in the prevalence of et al. Immunotherapy in selected Paediatr. 2008;97(4):451–453
Down syndrome in north-eastern patients with Down syndrome
22. Stein DS, Munir KM, Karweck AJ,
France. Ann Genet. 1994;37(4):179–183 disintegrative disorder. Dev Med Child
Davidson EJ, Stein MT. Developmental
Neurol. 2019;61(7):847–851
2. Ghaziuddin N, Nassiri A, Miles JH. regression, depression, and
Downloaded from http://publications.aap.org/pediatrics/article-pdf/145/6/e20192939/1079455/peds_20192939.pdf by guest on 17 December 2021
Catatonia in Down syndrome; 12. Akahoshi K, Matsuda H, Funahashi M, psychosocial stress in an adolescent
a treatable cause of regression. Hanaoka T, Suzuki Y. Acute with Down syndrome. J Dev Behav
Neuropsychiatr Dis Treat. 2015;11: neuropsychiatric disorders in Pediatr. 2017;38(suppl 1):S26–S28
941–949 adolescents and young adults with
23. Watemberg N, Greenstein D, Levine A.
Down syndrome: Japanese case
3. de Graaf G, Buckley F, Skotko BG. Live Encephalopathy associated with
reports. Neuropsychiatr Dis Treat. 2012;
births, natural losses, and elective Hashimoto thyroiditis: pediatric
8:339–345
terminations with Down syndrome in perspective. J Child Neurol. 2006;21(1):
Massachusetts. Genet Med. 2016;18(5): 13. Jacobs J, Schwartz A, McDougle CJ, 1–5
459–466 Skotko BG. Rapid clinical deterioration
in an individual with Down syndrome. 24. Das D, Phillips C, Hsieh W, Sumanth K,
4. Worley G, Crissman BG, Cadogan E, Dang V, Salehi A. Neurotransmitter-
Am J Med Genet A. 2016;170(7):
Milleson C, Adkins DW, Kishnani PS. based strategies for the treatment of
1899–1902
Down syndrome disintegrative cognitive dysfunction in Down
disorder: new-onset autistic regression, 14. Castillo H, Patterson B, Hickey F, et al. syndrome. Prog
dementia, and insomnia in older Difference in age at regression in Neuropsychopharmacol Biol Psychiatry.
children and adolescents with Down children with autism with and without 2014;54:140–148
syndrome. J Child Neurol. 2015;30(9): Down syndrome. J Dev Behav Pediatr.
1147–1152 2008;29(2):89–93 25. Coppus AW, Fekkes D, Verhoeven WM,
Tuinier S, Egger JI, van Duijn CM.
5. Mircher C, Cieuta-Walti C, Marey I, et al. 15. Chitnis T, Pohl D. Pediatric Plasma amino acids and neopterin in
Acute regression in young people with demyelinating disorders. Neurology. healthy persons with Down’s syndrome.
Down syndrome. Brain Sci. 2017;7(6): 2016;87(9 suppl 2):S1–S3 J Neural Transm (Vienna). 2007;114(8):
E57 16. Sullivan KD, Evans D, Pandey A, et al. 1041–1045
6. Rollin HR. Personality in mongolism Trisomy 21 causes changes in the
26. Harris JC. Lesch-Nyhan syndrome and
with special reference to the incidence circulating proteome indicative of
its variants: examining the behavioral
of catatonic psychosis. Am J Ment Defic. chronic autoinflammation. Sci Rep.
and neurocognitive phenotype. Curr
1946;51(2):219–237 2017;7(1):14818
Opin Psychiatry. 2018;31(2):96–102
7. Kerbeshian J, Burd L. Comorbid Down’s 17. Al-Diwani AAJ, Pollak TA, Irani SR,
27. Palumbo ML, McDougle CJ.
syndrome, Tourette syndrome and Lennox BR. Psychosis: an autoimmune
Pharmacotherapy of Down syndrome.
intellectual disability: registry disease? Immunology. 2017;152(3):
Expert Opin Pharmacother. 2018;19(17):
prevalence and developmental course. 388–401
1875–1889
J Intellect Disabil Res. 2000;44(pt 1): 18. Kiecolt-Glaser JK, Derry HM, Fagundes
60–67 CP. Inflammation: depression fans the 28. Walker JC, Dosen A, Buitelaar JK,
flames and feasts on the heat. Am Janzing JG. Depression in Down
8. Prasher V. Disintegrative syndrome in syndrome: a review of the literature.
young adults. Ir J Psychol Med. 2002;19: J Psychiatry. 2015;172(11):1075–1091
Res Dev Disabil. 2011;32(5):1432–1440
101 19. Iughetti L, Predieri B, Bruzzi P, et al. Ten-
year longitudinal study of thyroid 29. Moran JA, Rafii MS, Keller SM, Singh BK,
9. American Psychiatric Association.
function in children with Down’s Janicki MP; American Academy of
Diagnostic and Statistical Manual of
syndrome. Horm Res Paediatr. 2014; Developmental Medicine and Dentistry;
Mental Disorders, 5th ed. Washington,
82(2):113–121 Rehabilitation Research and Training
DC: American Psychiatric Association;
Center on Aging With Developmental
2013 20. Mocellin R, Lubman DI, Lloyd J, Disabilities, University of Illinois at
10. Richards C, Jones C, Groves L, Moss J, Tomlinson EB, Velakoulis D. Reversible Chicago; American Association on
Oliver C. Prevalence of autism spectrum dementia with psychosis: Hashimoto’s Intellectual and Developmental
disorder phenomenology in genetic encephalopathy. Psychiatry Clin Disabilities. The National Task Group on
disorders: a systematic review and Neurosci. 2006;60(6):761–763 Intellectual Disabilities and Dementia
meta-analysis. Lancet Psychiatry. 2015; 21. Alink J, de Vries TW. Unexplained Practices consensus recommendations
2(10):909–916 seizures, confusion or hallucinations: for the evaluation and management of
8 ROSSO et aldementia in adults with intellectual during adolescence in Down syndrome. 33. Spiridigliozzi GA, Hart SJ, Heller JH,
disabilities. Mayo Clin Proc. 2013;88(8): Brain Dev. 2016;38(1):113–117 et al. Safety and efficacy of rivastigmine
831–840 in children with Down syndrome:
32. Kondoh T, Kanno A, Itoh H, et al.
30. Ballard C, Mobley W, Hardy J, Williams a double blind placebo controlled trial.
Donepezil significantly improves
G, Corbett A. Dementia in Down’s Am J Med Genet A. 2016;170(6):
abilities in daily lives of female Down
syndrome. Lancet Neurol. 2016;15(6): 1545–1555
syndrome patients with severe
622–636 cognitive impairment: a 24-week 34. Ingram A, Saling MM, Schweitzer I.
31. Tamasaki A, Saito Y, Ueda R, et al. randomized, double-blind, placebo- Cognitive side effects of brief pulse
Effects of donepezil and serotonin controlled trial. Int J Psychiatry Med. electroconvulsive therapy: a review.
reuptake inhibitor on acute regression 2011;41(1):71–89 J ECT. 2008;24(1):3–9
Downloaded from http://publications.aap.org/pediatrics/article-pdf/145/6/e20192939/1079455/peds_20192939.pdf by guest on 17 December 2021
PEDIATRICS Volume 145, number 6, June 2019 9You can also read

















































