DPP SYPHILIS SCREEN AND CONFIRM ASSAY - A UNIQUE POINT OF CARE, SINGLE USE RAPID DIAGNOSTIC - RAPID TESTS FOR EARLIER TREATMENT
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Rapid Tests for Rapid Tests for Earlier Treatment
Earlier Treatment
DPP SYPHILIS SCREEN and
®
Confirm Assay
A Unique Point of Care, Single Use Rapid Diagnostic
Rapid Tests for Earlier Treatment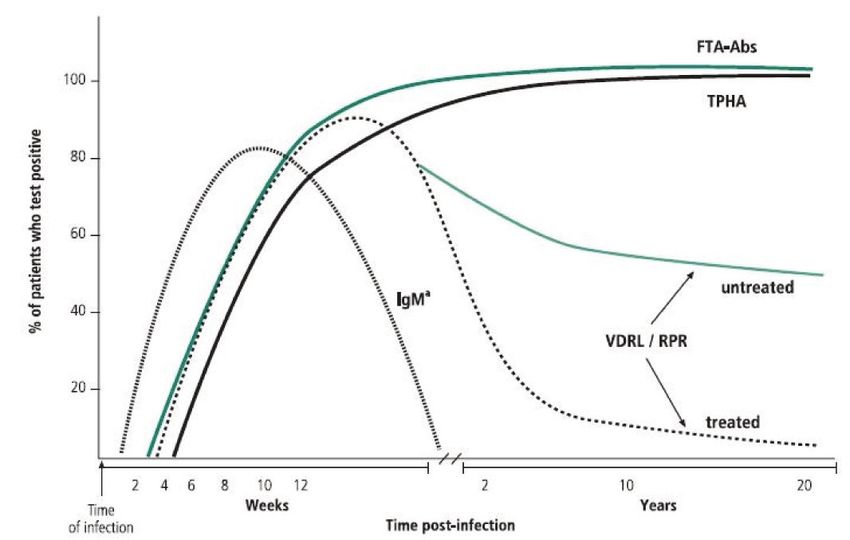
CHEMBIO DPP® SYPHILIS
SCREEN and CONFIRM
Background
T
he cause of Syphilis is Treponema pallidum, a Syphilis can be transmitted
spirochete. The Syphilis infection is limited to to the fetus through the
the human host and is generally transmitted by placenta during the first
sexual contact. The disease is spread widely throughout and second trimesters
the world. Low concentrations of penicillin can kill of gestation. As a result,
T. pallidum, and resistance to penicillin has not been some infected fetuses
demonstrated. can die and miscarry,
but some are stillborn
Approximately 70,000 new Syphilis cases are reported at birth, while others are
in the U.S. annually; however, the actual number of born live, but develop
infections is estimated at 500,000. congenital Syphilis or
other anomalies.
The disease manifests itself in infectious lesions on the
skin or mucous membranes of the genitalia. In almost Public health officials in
20% of the cases, the primary lesion is intrarectal, many countries are attempting to modify current
perianal or oral, suggesting that T.pallidum can control methods to better identify and treat Syphilis
penetrate the intact mucous membranes and skin. infected prostitutes, drug users, and their sexual
Later in the disease, the bacteria multiply at the site contacts based on a dramatic increase of Syphilis rates
of entry, spread to nearby lymph nodes, and reach the in many areas.
bloodstream. In 2 to 10 weeks, a papule develops at the
site of infection and breaks down to form an ulcer with
a clean, hard base (“hard chancre”). This primary lesion
Syphilis Serological Testing
always heals spontaneously, but 2 to 10 weeks later,
The recommended serological screening algorithm
the secondary lesions appear. Syphilitic meningitis,
for syphilis involves two types of serologic tests
chorioretinitis, hepatitis, nephritis (immune complex
(nontreponemal and treponemal).
type) or periostitis frequently occur in Syphilis. The
Syphilitic infection may remain subclinical and the
patient may pass through primary and secondary Non-Treponemal Tests
stages without symptoms and yet develop tertiary
lesions. About 30% of cases are cured, 30% remain Among the non-treponemal tests commonly used are
latent, and 40% progress to the tertiary stage, the Venereal Disease Research Lab (VDRL) and rapid
characterized by granulomatous lesions in skin, bones plasma reagin (RPR) tests. These tests are based on
and liver, degenerative changes in the central nervous the fact that particles of the lipid antigen (beef heart
system or cardiovascular lesions. However, tertiary cardiolipins) remain dispensed with normal serum, but
Syphilis is not usually infectious. form visible clumps when combined with reagin. The
Rapid Tests for Rapid Tests for Earlier Treatment
Earlier Treatment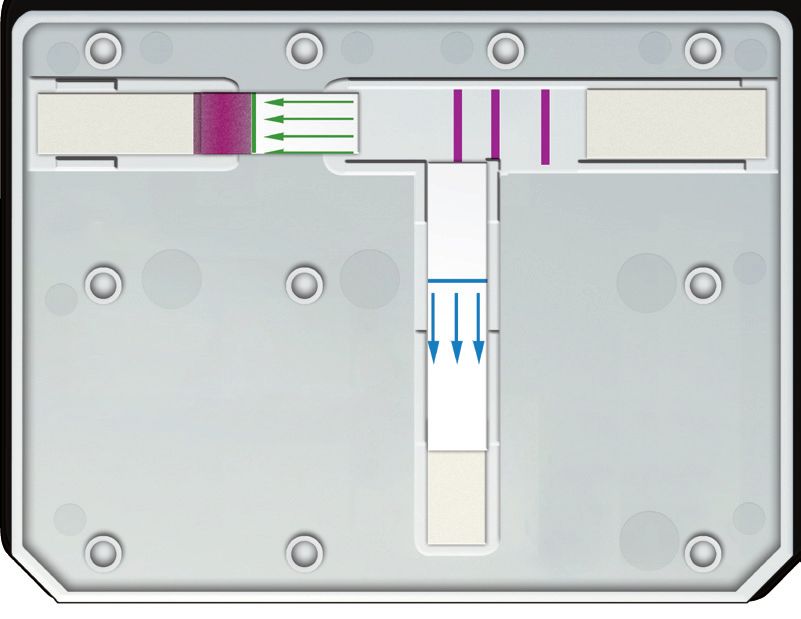
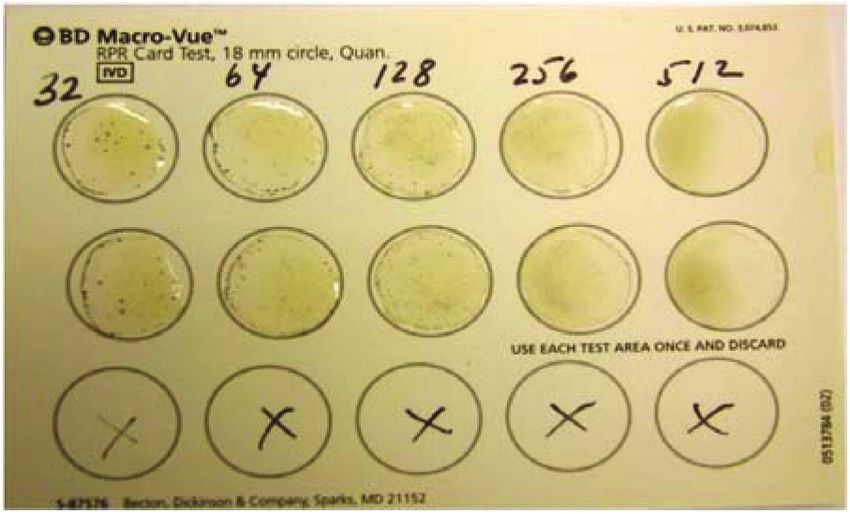
results are available in a few minutes and the tests are sensitivity for Syphilis antibodies. In the European
inexpensive, yet very labor intensive and technique Union (EU) the treponemal test is used as the first
dependent. screen for syphilis. This test, however, cannot be used
to judge the efficacy of Syphilis treatment. In addition,
the use of treponemal tests alone may also result
in overtreatment because they do not differentiate
between adequately treated and previous infections.
Treponemal tests have long been considered a
confirmatory test that have followed a positive non-
treponemal screening test. Positive screening tests are
then typically referred for a non-treponemal titer for
treatment surveillance and epidemiology purposes.
A Typical RPR Card Test
Algorithms
Positive VDRL and RPR tests revert to negative in 6 to We will consider three algorithms and their pluses
18 months after effective treatment. The VDRL can be and minuses: the Traditional Algorithm, The Alternate
performed on Cerebral Spinal Fluid (CSF). or Reverse Sequence Algorithm and the Rapid Point
of Care Algorithm. As mentioned earlier, traditional
Non-treponemal tests are subject to false positives algorithm, in the USA, has been a specimen received
(due to malaria, leprosy, measles, infectious mono-
nucleosis, vaccinations, SLE, rheumatoid arthritis Common patterns of serological reactivity in syphilis patients
and numerous other conditions), and false negative
in tertiary Syphilis. The use of a nontreponemal test
alone, such as the rapid plasma reagin (RPR) test, may
result in some overtreatment (treatment of uninfected
persons) owing to biological false-positive reactions.
Treponemal Tests
Among the most commonly performed treponemal
tests are Fluorescent Treponema Antibody Test (FTA-
ABS) and Treponema Pallidum Particle Agglutination the R Peeling et al WHO 2004
Test (TPPA). Newer enzyme immune assays (EIA) and
chemiluminescence immunoassay (CLIA) treponemal is screened with a non-treponemal assay, most
antibody tests have been introduced in both micro- commonly the RPR, with negatives reported out as
plate format, for large volume lab testing (blood bank) non-reactive. Reactive results reflex to a treponemal
as well as a rapid point of care test (POCT). confirmation, generally the TPPA or EIA.
The treponemal tests show excellent specificity and The advantages of the traditional algorithm is the
Rapid Tests for Rapid Tests for Earlier Treatment
Earlier Treatment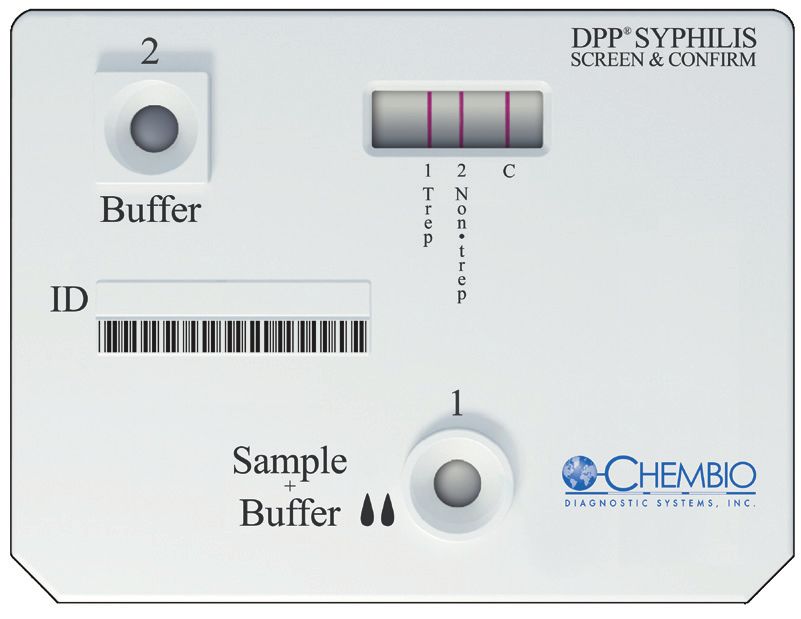
majority of tests are normally non-reactive and are life of a one time infected individual. Thus a positive
culled out with a relatively low cost assay in RPR. The treponemal test does not indicate an active infection,
disadvantages to the traditional algorithm are in the which can result in misdiagnosis if results are released
labor issues and the methodology issues including prior to, or in the absence of, a non-treponemal follow
specificity challenges. The RPR is a manual method up. This can result in over treatment of antibiotic and
that requires serum separation and heat inactivation, patient angst.
a technician to manually pipette and disburse sample
and add reagent, and after a mixing period, read a The newest arrival is a Rapid Point of Care (POC)
very subjective result. The RPR procedure should be Algorithm. With the approval of rapid point of care
run under very controlled environmental and lighting single use tests, a new paradigm must be considered.
conditions that can result in reproducibility issues, The current syphilis POC tests are simple lateral flow
technician performance variability, and reading errors. devices that utilize a treponemal component. The test
upside is that a sample can be run with the patient
An additional issue, most important to high volume present, in 15 to 30 minutes, allowing a physician
testing labs, is the labor issue. The RPR being so labor to determine if the patient has been infected with
intensive, requires a significant amount of trained syphilis. The downside of the test is that it does not
technician time as compared to a fully automated assay indicate that a positive test is an active infection and
procedure. There is a large problem with few qualified must be reflexed to a traditional nontreponemal assay
technicians choosing the laboratory field today as such as RPR. This would allow a screening of negatives
well as many current technicians retiring or moving and involves the traditional blood draw, lab submission
on to other fields. The result is finding technicians for and extended time for any positive result.
the lab (at higher labor cost) and the actual tech time
involved in RPR testing, has become more expensive Figure. CDC recommended algorithm for reverse sequence syphilis screening
(treponemal sets screening followed by nontreponemal test confirmation*
and in many cases outweighs the advantage of the less
expensive, lower cost RPR assay.
EIA or CIA
Recently in the USA an Alternate or Reverse Sequence
Screening algorithm is being reviewed by several
federal agencies and has been instituted in some labs. EIA / CIA EIA / CIA
As mentioned earlier, this is the preferred algorithm in + _Ɨ
the EU. This alternate algorithm involves performing
the Treponemal assay first then reflexing reactive Quantitative RPR
or other
specimens to a non-treponemal assay for confirmation, nontreponemal
test
thus sometimes referred to as the “reverse algorithm”.
RPR
The clear advantage of the reverse algorithm is the +
Syphilis
RPR
–
labor savings. The screening of the samples is done (past or present)5
with automated equipment eliminating the bulk of the
labor cost.
TP-PA
The drawback on the reverse assay is it determines
treponemal immunity status which can appear for the TP-PA
+ TP-PA
Syphilis –
(past or present)5 Syphilis unlikely1
Rapid Tests for Rapid Tests for Earlier Treatment
Earlier Treatment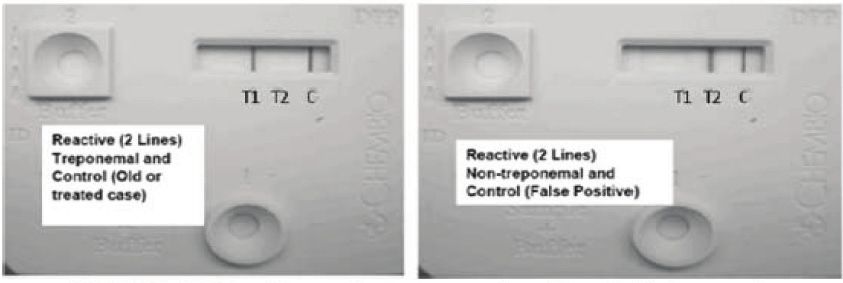
A B
Fig. 1. Structure of the Chembio dual POC test for syphilis showing the locations of the antigen lines.
A. Dissected view following testing of reactive serum; B, complete cassette following testing of reactive serum.
New DPP® Rapid Screen & Confirm Paradigm
A new point of care, rapid, single use syphilis test has assay will permit the clinician to initiate treatment
been developed by Chembio Diagnostic Systems and partner notification activities at the consultation
which employs both a Treponemal and Non- site. Statistics have shown that in outreach and clinical
treponemal component on their proprietary Dual Path settings as many as 40 to 50 percent of those testing for
Platform (DPP®). STDs never return for test results that traditionally have
taken from 24 to 48 hours to turn around. A rapid dual
The Chembio DPP® Syphilis Screen & Confirm Assay syphilis test could greatly improve efforts to control
IS NOT CURRENTLY CLEARED OR AVAILABLE FOR and eradicate syphilis.
CLINICAL USE IN THE US.
In addition to clinical and outreach use the DPP®
The Chembio DPP® Syphilis Screen & Confirm Assay IS Syphilis Screen and Confirm will be of utility in the lab
CE MARKED AND AVAILABLE FOR SALE AND CLINICAL setting as a follow up to a syphilis positive screening.
USE OUTSIDE THE US WHERE INDICATED. In either the traditional or alternate algorithm the
suggested next step is to run the complementary assay
The DPP® Syphilis Screen and Confirm Assay (DPPSC) to the Treponemal or non treponemal screen. The
provides a rapid (20 minutes), accurate visual reading at DPPSC will allow for that follow-up step and a repeat
room temperature allowing for the utilization of either of the screening result effectively and efficiently. This
the traditional algorithm or the reverse algorithm. The will be a welcome addition to most small, medium
treponemal marker (line) indicates a history of syphilis and large laboratories that currently only offer non
infection detecting IgG to T. palladium. The non- treponemal screens, or routinely send out specimens
treponemal marker was developed at the US Center for syphilis serology. In addition, the rapid and simple
for Disease Control and has been licensed for use in the performance characteristics of DPPSC outweigh
DPP® format by Chembio Diagnostic Systems. the cost and labor of running current or traditional
methods for Syphilis confirmation.
Considering the presence of both the treponemal
and nontreponemal markers on the dual syphilis POC The DPP® dual POC test exhibits remarkable
Rapid Tests for Rapid Tests for Earlier Treatment
Earlier Treatment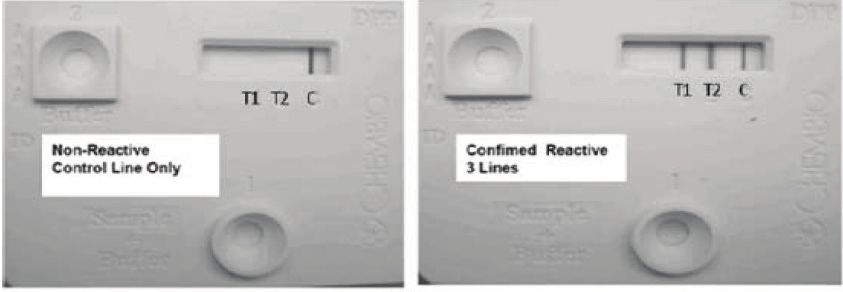
Fig. 2. Dual POC syphilis tests showing patterns of reactivity and their interpretations
performance characteristics compared to the standard RPR titers of 1:8, the dual POC test has, in preclinical
laboratory-based testing algorithm. When sera have studies, a sensitivity of 99.7%.
Table 1. Performance characteristics of the dual POC syphilis test (nontreponemal line) compared to the rapid plasma reagin (RPR) test.
Dual test Number of samples tested with RPR
Non-treponemal Line Positive Negative Total
Positive 739 11 750
Negative 95* 756 851
834 767 1601
Sensitivity 88.6%, Specificity 98.6%
*Of the 95 samples missed with the dual POC test had a RPR titer of 1:1 with RPR titer ≥ 1:2 the sensitivity was 98.7%
Table 2. Performance characteristics of the dual POC syphilis test (treponemal line) compared to the comparator Treponema pallidum
passive particle agglutination (TP-PA) test.
Dual test Number of samples tested with TP-PA
Treponemal Line Positive Negative Total
Positive 972 27 999
Negative 35 567 602
1007 594 1601
Sensitivity 96.5%, Specificity 95.5%
Table 3. Documented cases of syphilis tested with the dual DPP-POC test and the comparator rapid plasma reagin (RPR) and the
Treponema pallidum passive particle agglutination (TP-PA) tests.
Number of serum samples reactive (Sensitivity)
Dual rapid test Comparator
Syphilis category Total Non-Trepa Trepb RPR TP-PA
Primary untreated 7 7 (100%) 7 (100%) 7 7
Primary treated 14 9 (100%) 13 (100%) 9 13
Secondary untreated 6 6 (100%) 6 (100%) 6 6
Secondary treated 28 22 (84.6%) 28 (100%) 26 28
Latent untreated 5 3 (100%) 4 (80%) 3 5
Latent treated 45 35 (85.4%) 44 (97.8%) 41 45
Total 105 82 102 92 104
a
Non-Trep, Nontreponemal Line b
Treponemal Line
Rapid Tests for Rapid Tests for Earlier Treatment
Earlier Treatment
World Health Organization 2011 New Syphilis Cases Yearly Estimates
Access to syphilis diagnostics is limited in regions of high disease burden
REFERENCES
Blandford, J. M., T. L. Gift, S. Vasaikar, D. Mwesigwa-Kayongo, P. Dlali, and R. Nessa, K., A. Alam, F. A. Chawdhury, M. Huk, S. Nahar, G. Salauddin, S.
N. Bronzan. 2007. Cost-effectiveness of on-site antenatal screening to prevent Khursheed, S. Rahman, E. Gurley, R. F. Breiman, and M. Rahman. 2008. Field
congenital syphilis in rural eastern Cape Province, Republic of South Africa. Sex. evaluation of simple rapid tests in the diagnosis of syphilis. Int. J. STD AIDS
Transm. Dis. 34(7 Suppl.):S61–S66. 19:316–320.
Bronzan, R. N., D. C. Mwesigwa-Kayongo, D. Narkunas, G. P. Schmid, G. A. Peeling, R. W., and H. Ye. 2004. Diagnostic tools for preventing and managing
Neilsen, R. C. Ballard, P. Karuhije, J. Ddamba, E. Nombekela, G. Hoyi, P. Dlali, maternal and congenital syphilis: an overview. Bull. World Health Organ.
N. Makwedini, H. G. Fehler, J. M. Blandford, and C. Ryan. 2007. On-site rapid 82:439–446.
antenatal syphilis screening with an immunochromatographic strip improves
case detection and treatment in rural South African clinics. Sex. Transm. Dis. 34(7 Terris-Prestholt, F., D. Watson-Jones, K. Mugeye, L. Kumaranayake, L. Ndeki,
Suppl.):S55–S60. H. Weiss, J. Changalucha, J. Todd, F. Lisekie, B. Gumodoka, D.Mabey, and R.
Hayes. 2003. Is antenatal syphilis screening still cost effective in sub-Saharan
Castro A. R., J. Esfandiari, S.Kumar, M. Ashton, S.E. Kikkert, M.M. Park, Africa. Sex. Transm. Infect. 79:375–381.
and R.C. Ballard. 2010 Novel Point-of-Care Test for Simultaneous Detection of
Nontreponemal and Treponemal Antibodies in Patients with Syphilis. Jl. Clinical van Dommelen, L., A. Smismans, V. J. Goossens, J. Damoiseaux, C.
Micro Vol. 48, No. 12: 4615-4619 A.Bruggeman, F. H. Van Tiel, and C. J. Hoebe. 2008. Evaluation of a rapid one-
step immunochromatographic test and two Immuno-enzymatic assays for the
Deacon, W. E., and E. F. Hunter. 1962. Treponemal antigens as related to detection of anti-Treponema pallidum antibodies. Sex. Transm. Infect.84:292–296.
identification of syphilis serology. Proc. Soc. Exp. Biol. Med. 110:352–356.
Vickerman, P., R. W. Peeling, F. Terris-Prestholt, J. Changalucha, D. Mabey,D.
Goel, N., M. Sharma, N. Gupta, and R. Sehgal. 2005. Rapid Watson-Jones, and C. Watts. 2006. Modelling the cost-effectiveness of
immunochromatographic test for syphilis. Indian J. Med. Microbiol. 23:142–143. introducing rapid syphilis tests into an antenatal syphilis screening programme in
Mwanza, Tanzania. Sex. Transm. Infect. 82(Suppl. 5):v38–v43.
Harris, A., A. A. Rosenberg, and E. R. del Vecchio. 1948. The VDRL slide
flocculation test for syphilis; a supplementary report. J. Vener. Dis. Inf. 29:72–75. Watson-Jones, D., J. Changalucha, B. Gumodoka, H. Weiss, M. Rusizoka,
L.Ndeki, A. Whitehouse, R. Balira, J. Todd, D. Ngeleja, D. Ross, A. Buve´,
Hunter, E. F., W. E. Deacon, and P. E. Meyer. 1964. An improved FTA test for R.Hayes, and D. Mabey. 2002. Syphilis in pregnancy in Tanzania. I. Impact of
syphilis: the absorption procedure (FTA-ABS). Public Health Rep. 79:410–412. maternal syphilis on outcome of pregnancy. J. Infect. Dis. 186:940–947.
Hunter, E. F., R. M. McKenney, S. E. Madison, and D. D. Cruce. 1979.Double- Zarakolu, P., I. Buchanan, M. Tam, K. Smith, and E. W. Hook. 2002.Preliminary
staining procedure for the fluorescent treponemal antibody absorption (FTA-ABS) evaluation of an immunochromatographic strip test for specific Treponema
test. Br. J. Vener. Dis. 55:105–108. pallidum antibodies. J. Clin. Microbiol. 40:3064–3065.
Larsen, S. A., V. Pope, and R. E. Johnson. 1998. Manual of test for syphilis 9th
edition. American Public Health Association, Washington, DC.
Rapid Tests for Rapid Tests for Earlier Treatment
Earlier Treatment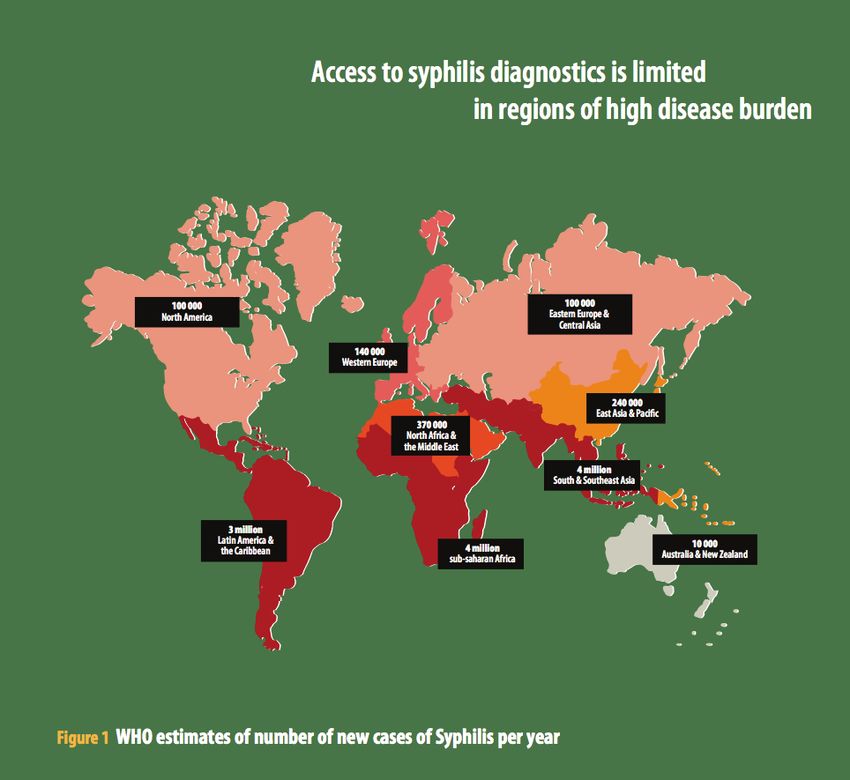
Rapid Tests for Rapid Tests for Earlier Treatment
Earlier Treatment
Chembio Diagnostic Systems, Inc.
3661 Horseblock Road
Medford, NY 11763 USA
info@chembio.com • www.chembio.comYou can also read

















































