Employee Benefits Guide - January 1, 2023 - December 31, 2023 - Goodwin University
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Employee Benefits Guide January 1, 2023 - December 31, 2023
2|Page
INTRODUCTION
Welcome to Benefit Enrollment! Our employee benefit plans are a valuable part of your overall compensation
package. The main goal of our benefit program is to help you build financial security for yourself and your family
through a benefit package that offers a broad range of coverage, at reasonable cost.
Complete details about the benefits that will be available to you and your eligible dependents are described in this
benefit guide.
Our Benefit Program Offers: NEW CARRIERS FOR THE 2023 OPEN ENROLLMENT!
Medical & Prescription Drug Coverage United Healthcare
Voluntary Dental Insurance United Healthcare
Voluntary Vision Insurance Ameritas
Basic Life and AD&D Insurance Lincoln Financial
Voluntary Life Insurance Lincoln Financial
Short-Term Disability Lincoln Financial
Long-Term Disability Lincoln Financial
Voluntary Accident Coverage United Healthcare
Voluntary Critical Illness Coverage United Healthcare
Voluntary Hospital Indemnity Coverage United Healthcare
NEW! Voluntary Pet Insurance Pet Benefit Solutions
Identity Theft Protection Norton Lifelock
Pre-Paid Legal Services MetLife
Flexible Spending Accounts (FSA) Progressive Benefit Solutions (PBS)
Benefit Enrollment is conducted online!
All benefit eligible employees are required to enroll in benefits through our online enrollment system, Employee
Navigator. Step-by-step instructions for new hire registration can be found on the next page. Current employees should
log in using their existing username and password – if you have forgotten your password, click on the reset password
link.
This document is intended to provide a brief summary of our benefit plans and is not a guarantee of coverage. For a complete description of plan
features, including eligibility and termination requirements, definitions, limitations and exclusions, please refer to your insurance booklet/certificate
and Summary Plan Description (SPD). The company reserves the right to change plan provisions in whole or in part as it deems necessary.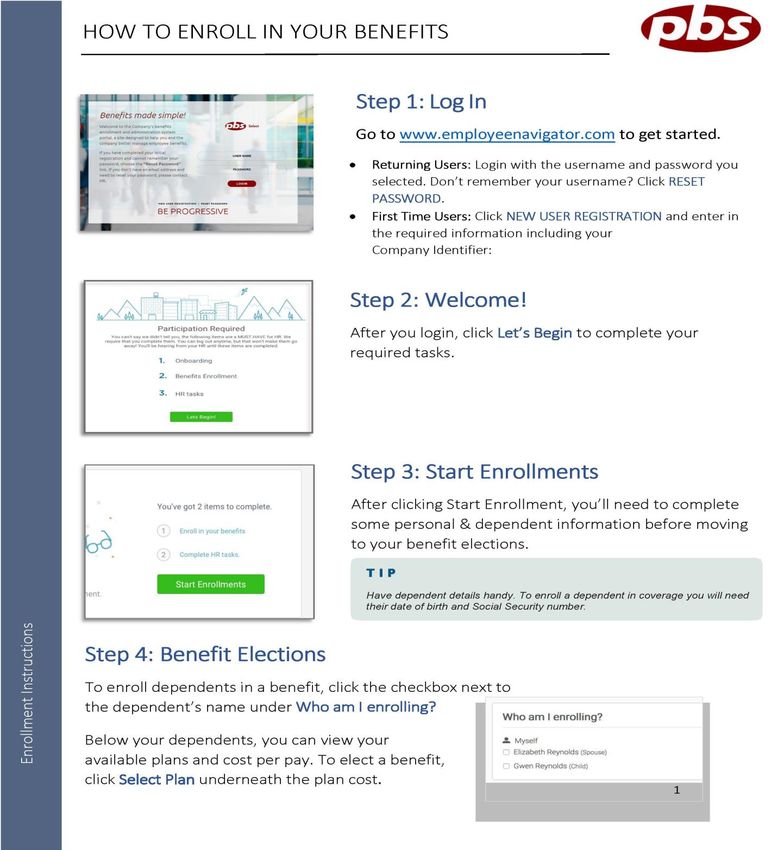
Page |3
goodwinuni
This document is intended to provide a brief summary of our benefit plans and is not a guarantee of coverage. For a complete description of plan
features, including eligibility and termination requirements, definitions, limitations and exclusions, please refer to your insurance booklet/certificate
and Summary Plan Description (SPD). The company reserves the right to change plan provisions in whole or in part as it deems necessary.
4|Page
If you need additional
assistance, email:
mmurphy1@goodwin.edu
tantoine@goodwin.edu
[Grab your reader’s attention with a great quote from the document or use cnyarady@bridgeport.edu
this space to emphasize a key point. To place this text box anywhere on
apisco@bridgeport.edu
the page, just drag it.]
This document is intended to provide a brief summary of our benefit plans and is not a guarantee of coverage. For a complete description of plan
features, including eligibility and termination requirements, definitions, limitations and exclusions, please refer to your insurance booklet/certificate
and Summary Plan Description (SPD). The company reserves the right to change plan provisions in whole or in part as it deems necessary.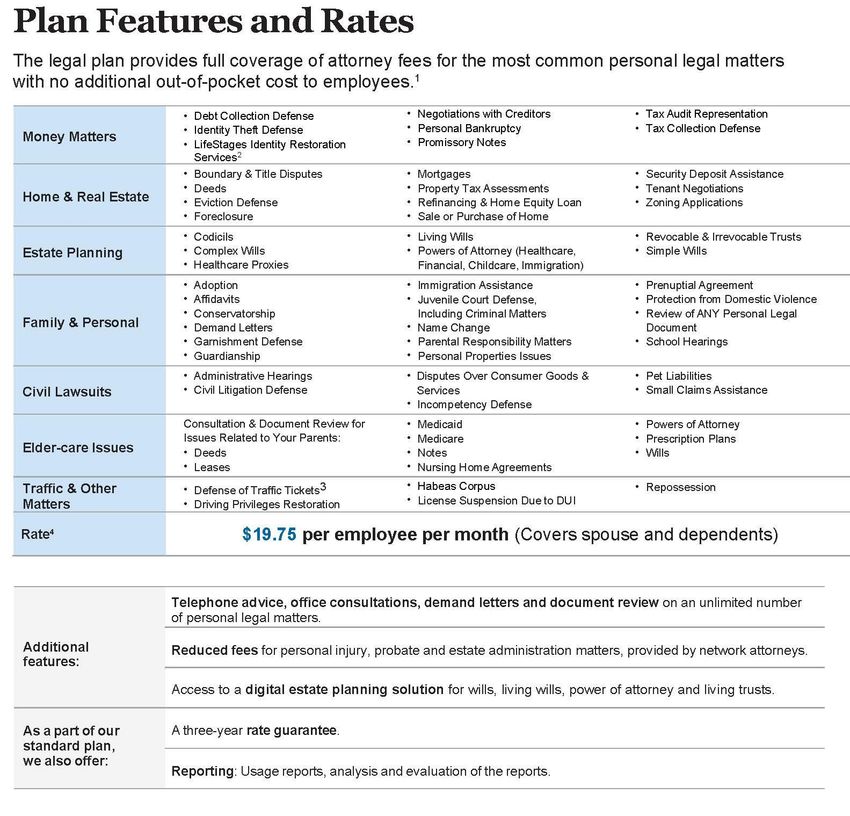
Page |5
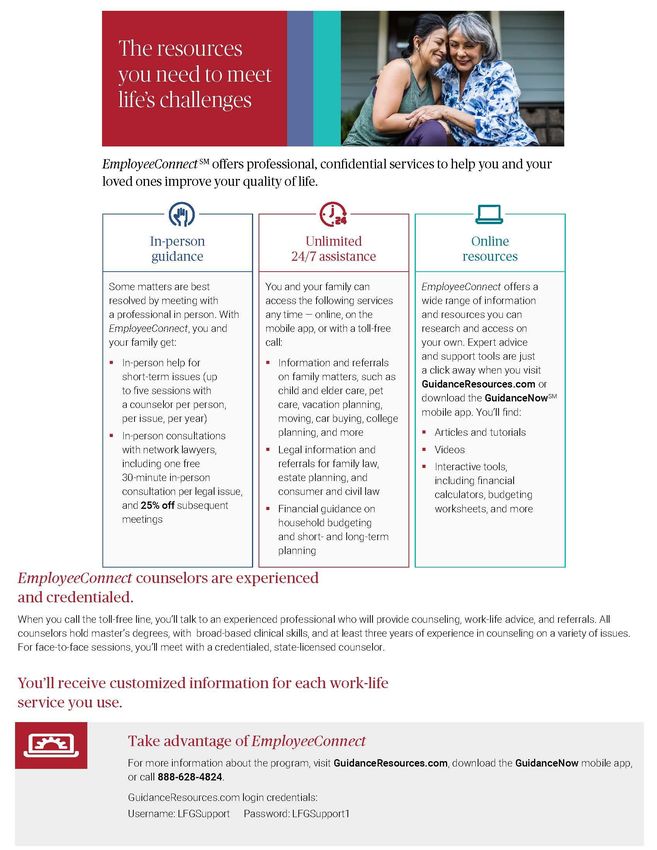
RESOURCES
When you have questions about your insurance coverage, or are experiencing problems with getting claims paid, you
have several resources:
Benefit Guide This guide is a summary of your insurance plans. It also contains benefit rates for all your insurance
plans. While it is a great tool, we recognize that you may need additional information to help you make the best
benefit decision. Therefore, this Benefit Guide contains all of the helpful phone numbers and websites. This benefit
guide highlights some of the main features of your benefit programs, but does not include all plan rules, features,
limitations or exclusions. The terms of your benefit plans are governed by legal documents, including insurance
contracts. Should there be any inconsistencies between this book and the legal plan documents, the plan documents
are the final authority.
Insurance Carrier Websites and Phone Numbers These websites are most helpful when you want to review a claim
that has been presented, order additional or replacement ID cards, and other administrative things. The websites are
also a valuable resource for locating in network providers. You can also contact the insurance carriers by phone with
any questions about your coverage. Their phone number(s) is located on your insurance identification care.
The Human Resource Team: can assist you with completing the enrollment process. We are also available to act as a
liaison in your dealings with insurance carriers. If you are having trouble getting claims paid or questions regarding
your coverage, we are here to help.
Goodwin University University of Bridgeport
Terry W. Antoine – Director, Human Resources Cheryl Nyarady – Director, Human Resources
Tantoine@goodwin.edu Cnyarady@bridgeport.edu
Phone: (860) 727-6938 Phone: (203) 576-4731
Meghan Murphy, HR Specialist Alexandra Pisco, HR Specialist
mmurphy1@goodwin.edu Apisco@bridgeport.edu
Phone: (860) 913-2259 Phone: (203) 576-4593
The HILB Group is our strategic partner in managing our benefit programs. They work closely with the HR team to
ensure that you have seamless benefits coverage. Andrews Benefits are also a great resource for discussing your 401(k)
retirement, and related questions and concerns.
Andrews Benefits / The HILB Group Contacts:
Erica Mitchell – SHRM-CP, Director of Operations Amanda Carlo – Group Account Manager
emitchell@hilbgroup.com acarlo@hilbgroup.com
Direct Line: 860-325-4671 Direct Line: 860-325-4448
Chris Andrews
candrews@hilbgroup.com
Direct Line: 860-325-4427
Phone: (860) 678-8888 Fax: (860) 678-0115
Certificates and Policies documents are required by Health Care Reform. You can find a copy of all Certificates and
Policies on Employee Navigator. If there is a discrepancy between the benefit guide and the Certificates and Policies,
the Certificates and Policies will prevail.
Summary of Benefits and Coverage (SBC) SBC’s is a document required by Health Care Reform. It is a summary of the
insurance plan design. The SBC for your Medical plan is available on Employee Navigator.
Insurance Carrier Websites
These websites are most helpful when you want to review a claim that has been presented, order additional or
replacement ID cards, and other things. They are also the resource for locating in network providers.
This document is intended to provide a brief summary of our benefit plans and is not a guarantee of coverage. For a complete description of plan
features, including eligibility and termination requirements, definitions, limitations and exclusions, please refer to your insurance booklet/certificate
and Summary Plan Description (SPD). The company reserves the right to change plan provisions in whole or in part as it deems necessary.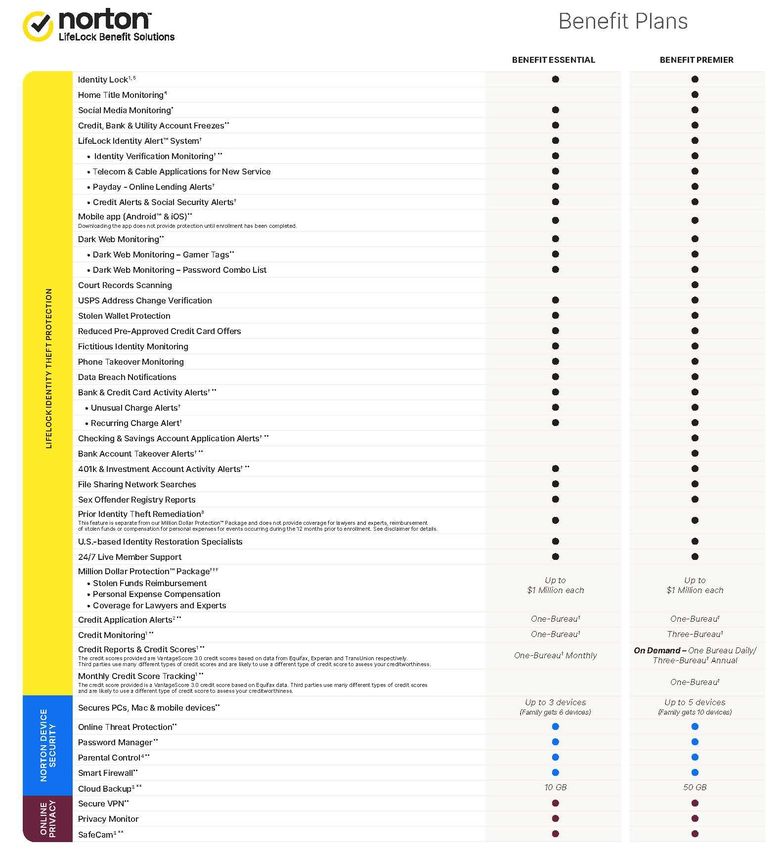
6|Page
CARRIER INFORMATION
United Healthcare: Member Services: 1-866-414-1959 / Online: www.myuhc.com Group # 930037
Medical Insurance Company/Employee Paid
Voluntary Dental Insurance Employee Paid
Ameritas: Member Services: 1-800-487-5553 / Online: www.ameritas.com Group # Pending
Voluntary Vision Employee Paid
Lincoln Financial Group (LFG): Member Services: 1-800-423-2765 Group # Pending
Online: www.lincolnfinancial.com
Basic Life and AD&D – 2x annual salary Company Paid
Voluntary Life – Coverage options for employee, spouse, and children Employee Paid
Short Term Disability – Coverage of 60% up to a max of $750 per week Company Paid
Long Term Disability – Coverage of 60% up to a max of $10,000 per month Company Paid
United Healthcare: Member Services: 1-800-444-6222 / Online: www.myuhc.com Group # Pending
Accidental Injury Insurance Employee Paid
Critical Illness Insurance Employee Paid
Hospital Indemnity Insurance Employee Paid
Wishbone: Member Services: 1-800-891-2565
Group # 6587
Online: https://wishboneinsurance.com/goodwinuniversity-universityofbridgeport
Voluntary Pet Insurance Employee Paid
Total Pet Plan: Member Services: 1-888-913-7387 / Online: www.petbenefits.com Group # 6587
Voluntary Pet Insurance Employee Paid
HSA Bank – Health Savings Account
You must open a Health Savings Account with HSA Bank in order to have money payroll deducted into the account. You can open an
account by completing the enrollment form on Employee Navigator or by enrolling online at www.hsabank.com.
Norton LifeLock: Member Services: 1-800-607-9174 / Online: www.nortonlifelock.com
Identity Theft Protection Employee Paid
MetLife Legal: Member Services: 1-800-821-6400 / Online: www.metlife.com
Pre-paid Legal Services Employee Paid
Progressive Benefit Solutions: Member Service: 1-888-333-3901 / Online:www.pbscard.com
Flexible Spending Accounts Employee Paid
COBRA Continuation Employee Paid
OPEN ENROLLMENT - PREVENTIVE CARE CAMPAIGN
Available to Employees & Spouses who enroll in Medical Coverage January 1, 2023:
The University is committed to the health and wellbeing our employees. We have redeveloped our wellness program where
employees and their spouses will receive a credit on their medical plan payroll deductions for taking the basic step of obtaining a
routine wellness exam. We feel that having this routine exam provides an opportunity for their personal physician to assess their
current health situation and create a plan to become their healthiest. This program is only applicable to employees and spouses
enrolled in our health plan; this program does not apply to children.
Employees that enroll in the health plan as of January 1, 2023 and submit their Physician Attestation Forms will be provided a $327
annual credit or a $654 annual credit for employee & spouse. If both employee and spouse are enrolled in the medical coverage,
both must provide the Physician Attestation Form as evidence of a current physical in order to receive the credit (partial credit will
NOT be provided). Those employees and spouses who choose not to submit the Attestation Form(s) will not be eligible for the
credit(s) and will pay a higher medical premium. The credit/surcharge will be provided as follows:
Coverage Level Bi-Weekly Credit
Employee Only $12.58
Employee + Spouse $25.15
Employee + Child(ren) $12.58
Employee + Family $25.15
We encourage all employees and applicable spouses to participate. The Physician Attestation Form must be submitted to Human
Resources no later than January 2, 2023.
This document is intended to provide a brief summary of our benefit plans and is not a guarantee of coverage. For a complete description of plan
features, including eligibility and termination requirements, definitions, limitations and exclusions, please refer to your insurance booklet/certificate
and Summary Plan Description (SPD). The company reserves the right to change plan provisions in whole or in part as it deems necessary.
Page |7
ELIGIBILITY
Open enrollment for eligible employees is the month of November, annually, with the new benefit plan
effective January 1, 2023
• You are eligible if you are a full-time employee, which is defined as:
▪ Faculty - regularly scheduled to work at least 35 hours a week.
▪ Staff – regularly scheduled to work at least 40 hours a week.
If you work an average of 30 hours a week, you are eligible to enroll in the medical insurance plan only.
• New employees are eligible for coverage on “The first of the month, 60 days after their date of
hire”.
• If new hires do not enroll for all benefits when first eligible, there could be late entrant penalties
and/or other plan limitations when enrolling later. Be sure to check each benefit’s enrollment rules
carefully.
• Open enrollment privileges apply to Medical, Dental, Vision, Accidental Injury, Critical Illness, and
Flexible Spending Accounts (FSA). Individuals may make changes or add dependents without having
to provide proof of insurability during the open enrollment period.
• The open enrollment period is the only time employees may enroll in the above medical or dental
coverage without the occurrence of a qualifying event (see definition below).
Legal Spouse eligibility:
• Employees may cover their spouse under medical, dental, vision, voluntary life, accidental injury, critical
illness plans, Lifelock and Legalease. An eligible spouse may be added to the employee’s medical, dental
and vision plan during the employee’s initial eligibility period, during open enrollment, or due to a
qualifying event. For more information regarding spouse eligibility please contact Human Resources.
Dependent Children eligibility:
• Medical and Dental Insurance – Dependents can be covered up to age 26 on the as long as they are not
covered under their own policy. Coverage will terminate at the end of the plan year following the
dependent’s 26th birthday.
• Vision Insurance – Dependent children are covered until the end of the month in which they turn 26.
• Voluntary Life Insurance – children ages 15 days to 26 years old are eligible for coverage. Coverage will
terminate at the end of the policy year following the dependents 26th birthday.
• Voluntary Benefits - Dependent children from newborns to age 26 are covered regardless of their martial
or student status. Coverage will terminate on the day the child is no longer eligible.
ENROLLMENT RULES
Special Enrollment Rules
You are eligible to enroll yourself and your eligible dependents in the plans when you meet the eligibility
requirements. Generally, the coverage you elect for yourself and your dependents may only be changed during
the next annual open enrollment period, unless you qualify to make a mid-year change in coverage due to a
qualifying event described under the Health Insurance Portability and Accountability Act of 1996 (HIPAA) and the
Internal Revenue Code § 125. Here is a partial list of qualifying events:
• A change in your employment status, or your spouse’s employment status that affects eligibility for
benefits;
• A change that causes your dependent children to become ineligible, such as age or student status;
• A change in your legal marital status (marriage, civil union, divorce);
• A change in the number of your dependents due to birth, adoption or death; and/or
• Loss of your coverage or your dependent’s coverage under your spouse’s plan due to loss of eligibility
under that plan.
If you wish to request a change in your coverage due to one of the qualifying events outlined above, or as
otherwise described under HIPAA you must submit a written request within 30 days of the date of the event. The
change you request must be consistent with, and on account of, the event listed above. Please contact Human
Resources if you wish to clarify your eligibility to make a mid-year change in your coverage.
This document is intended to provide a brief summary of our benefit plans and is not a guarantee of coverage. For a complete description of plan
features, including eligibility and termination requirements, definitions, limitations and exclusions, please refer to your insurance booklet/certificate
and Summary Plan Description (SPD). The company reserves the right to change plan provisions in whole or in part as it deems necessary.
8|Page
ENROLLMENT RULES
Should Your Employee Coverage Terminate
• Medical, Dental, and Vision coverage will expire the last day of the month in which your final
employment date occurs. You will be sent a COBRA Qualifying Event letter, offering you the
opportunity to continue your current coverage. COBRA coverage will be effective retro back to this
same date, should you elect it.
• Group Life and AD&D, Voluntary life, Short- and Long-Term Disability, and FSA coverages will
expire on the day you are no longer eligible.
• Accidental Injury, Critical Illness, and Hospital Indemnity coverage will terminate with
your last payroll deduction for the policy. Cigna will contact you directly with
continuation options.
• Group Life may offer Conversion and/or Portability options. You will have 30 days to make
contact with the carrier, if you are interested in either of these extensions.
COBRA CONTINUATION
Continuation Under COBRA
If you or your covered dependents lose health coverage under our group plan, you may be eligible for
continuation coverage under State COBRA regulations. In certain circumstances – death of a dependent, divorce,
or a dependent child ceasing to be eligible for coverage – it is your responsibility to notify the Human Resources
Department of the qualifying event within 60 days. You are also responsible to keep the Human Resources
Department informed of changes in your address, and your dependents’ address if that is different than yours. If
you would like more information about your rights and responsibilities under COBRA, please contact Human
Resources.
Per the Department of Labor (DOL): COBRA requires that continuation coverage extends from the date of the
qualifying event for a limited period of 18 or 26 months. The length of time depends on the type of qualifying
event that gave rise to the COBRA rights. A plan, however, may provide longer periods of coverage beyond the
maximum period by law. When the qualifying event is the end of employment or reduction of the employee’s
hours, qualified beneficiaries are entitled to 18 months of continuation coverage. When the qualifying even is the
end of employment or reduction in the employee’s hours, and the employee became entitled to Medicare less
than 18 months before the qualifying event, COBRA coverage for the employee’s spouse and dependents can last
until 36 months after the date the employee becomes entitled to Medicare.
Connecticut Continuation of Group Health Coverage Expanded to 30 Months
Employees/Group certificate holders under Connecticut fully insured plans who lose coverage due to a layoff,
reduction of hours, leave of absence, or termination of employment (except for gross misconduct) can elect
continuation of Medical coverage for up to 30 months.
COBRA Vendor
Progressive Benefit Solutions is our COBRA vendor. All correspondence and payments for COBRA continuation,
should you or a family member be eligible, will be directed to Progressive Benefit Solutions.
This document is intended to provide a brief summary of our benefit plans and is not a guarantee of coverage. For a complete description of plan
features, including eligibility and termination requirements, definitions, limitations and exclusions, please refer to your insurance booklet/certificate
and Summary Plan Description (SPD). The company reserves the right to change plan provisions in whole or in part as it deems necessary.
Page |9
NEW CARRIER! UNITED HEALTHCARE – MEDICAL INSURANCE
Plan 1 – Core Plan *Plan 2 – Buy Down Plan 3 – Buy Up 1
In-Network Balanced Choice Plus Choice EPO $30/$45 - Balanced Choice Plus
$30/$45 - $3,000/30% $3,000/30% $30/$45 - $2,500/20%
Deductible $3,000 Individual / $6,000 Family $3,000 Individual / $6,000 Family $2,500 Individual / $5,000 Family
Coinsurance 30% 30% 20%
Out-of-Pocket Maximum $5,000 Individual / $10,000 Family $5,000 Individual / $10,000 Family $5,000 Individual / $10,000 Family
Routine/Preventive Covered in Full Covered in Full Covered in Full
PCP Visit $30 $30 $30
Specialist Visit $45 $45 $45
General X-ray - Outpatient $0 $0 $0
Advanced Imaging - Outpatient $75 $75 $75
Laboratory - Outpatient $0 $0 $0
Urgent Care $75 $75 $75
Emergency Room $150 $150 $150
Ambulance Services 30% After Deductible 30% After Deductible 20% After Deductible
Hospital Inpatient 30% After Deductible 30% After Deductible 20% After Deductible
Outpatient Surgery 30% After Deductible 30% After Deductible 20% After Deductible
Prescription Drugs Plan 1 Plan 2 Plan 3
Tier 1 $5 $5 $5
Tier 2 $25 $25 $25
Tier 3 $40 $40 $40
Mail Order OptumRx Pharmacy OptumRx Pharmacy OptumRx Pharmacy
**Out-of-Network Plan 1 Plan 2 Plan 3
Deductible $5,000 Individual / $10,00 Family Not Available $5,000 Individual / $10,000 Family
Coinsurance 50% Not Available 40%
$10,000 Individual / $20,000 $10,000 Individual / $20,000
Out-of-Pocket Maximum Not Available
Family Family
Bi-Weekly Rates Plan 1 Plan 2 Plan 3
Employee Only $96.71 $79.38 $107.10
Employee & Spouse $306.05 $268.79 $328.40
Employee & Child(ren) $235.35 $204.16 $254.06
Employee & Family $401.38 $354.59 $429.45
Additional Information:
o Plans 1, 3, 4 & 5: **Out-of-Network Reimbursement – Out-of-Network reimbursement is based on the maximum
allowable amount. Members are responsible to pay any charges in excess of this amount. Please refer to your
employer’s health plan description for more information.
o All individual out-of-pocket maximum amounts will count toward the family out-of-pocket maximum, but an
individual will not have to pay more than the individual out-of-pocket maximum amount.
o Once you’ve met your deductible, you start sharing costs with your plan – coinsurance. You continue paying a
portion of the expense until you reach your out-of-pocket limit. From there, your plan pays 100% of allowed
amounts for the rest of the year.
This document is intended to provide a brief summary of our benefit plans and is not a guarantee of coverage. For a complete description of plan
features, including eligibility and termination requirements, definitions, limitations and exclusions, please refer to your insurance booklet/certificate
and Summary Plan Description (SPD). The company reserves the right to change plan provisions in whole or in part as it deems necessary.
10 | P a g e
NEW CARRIER! UNITED HEALTHCARE – MEDICAL INSURANCE
Plan 4 – Buy Up 2 Plan 5 –
In-Network Balanced Choice Plus Balanced Choice Plus
$20/$40 - $1,500/20% HSA $2,500/10%
$1,500 Individual / $3,000 Family $2,500 Individual / $5,000 Family
Deductible
Not Embedded
Coinsurance 20% 10%
$3,000 Individual / $6,000 Family $3,275 Individual / $6,550 Family
Out-of-Pocket Maximum
Embedded
Routine/Preventive Covered in Full Covered in Full
PCP Visit $20 10% After Deductible
Specialist Visit $40 10% After Deductible
General X-ray - Outpatient $0 10% After Deductible
Advanced Imaging - Outpatient $75 10% After Deductible
Laboratory - Outpatient $0 10% After Deductible
Urgent Care $75 10% After Deductible
Emergency Room $150 10% After Deductible
Ambulance Services 20% After Deductible 10% After Deductible
Hospital Inpatient 20% After Deductible 10% After Deductible
Outpatient Surgery 20% After Deductible 10% After Deductible
Prescription Drugs Plan 4 Plan 5
Tier 1 $5 $5 After Deductible
Tier 2 $25 $25 After Deductible
Tier 3 $40 $40 After Deductible
Mail Order OptumRx Pharmacy OptumRx Pharmacy
**Out-of-Network Plan 4 Plan 5
Deductible $2,000 Individual / $4,000 Family $2,500 Individual / $5,000 Family
Coinsurance 40% 30%
Out-of-Pocket Maximum $6,000 Individual / $12,000 Family $5,000 Individual / $10,000 Family
Bi-Weekly Rates Plan 4 Plan 5
Employee Only $131.04 $60.42
Employee & Spouse $379.87 $228.04
Employee & Child(ren) $297.15 $170.03
Employee & Family $494.08 $303.41
Additional Information:
o Plans 1, 3, 4 & 5: **Out-of-Network Reimbursement – Out-of-Network reimbursement is based on the maximum
allowable amount. Members are responsible to pay any charges in excess of this amount. Please refer to your
employer’s health plan description for more information.
o All individual out-of-pocket maximum amounts will count toward the family out-of-pocket maximum, but an
individual will not have to pay more than the individual out-of-pocket maximum amount.
o Plan 5: Once you’ve met your deductible, you start sharing costs with your plan – coinsurance. You continue paying
a portion of the expense until you reach your out-of-pocket limit. From there, your plan pays 100% of allowed
amounts for the rest of the year.
This document is intended to provide a brief summary of our benefit plans and is not a guarantee of coverage. For a complete description of plan
features, including eligibility and termination requirements, definitions, limitations and exclusions, please refer to your insurance booklet/certificate
and Summary Plan Description (SPD). The company reserves the right to change plan provisions in whole or in part as it deems necessary.P a g e | 11
NEW CARRIER! UNITED HEALTHCARE – MEDICAL INSURANCE
How to Look Up a Prescription:
1. Go to www.uhc.com
2. Click on “Member Resources” and then click “Pharmacy Benefits”
3. Click “Pharmacy Drug Lists” on the left-hand side
4. Scroll down and click “Connecticut Plans” and select “UHC Traditional Tier 3 Prescription Drug List (01/01/2023)”
For Medical ID Cards: You will receive two ID cards in the mail and they will list all of your enrolled dependents. You can
also access them online with the steps below or use the United Healthcare app to access your ID card.
To access ID cards, enrolled members can create a secure member account at myuhc.com using the following instructions.
1. Go to www.myuhc.com
2. For new members, select “Register”.
3. Enter your Name, Date of Birth, & your Member ID (this is not the same as SSN). If you do not know your Member
ID, then enter the last 4 digits of your SSN along with your zip code.
4. Create a username and password. Your access will then be complete and you will be free to navigate the site.
5. Once logged in, select “Print ID Card.” (If you do not see this option, click on the blue “select” button next to your
plan name.)
6. From the drop-down menu, select the person whose ID card you would like to print. Then click “Get ID Card.”
7. This generates a document with your ID card. Scroll to the bottom of this document where a toolbar will appear.
Click on the printer icon to print.
For the January 1, 2023 Open Enrollment: Current Cigna members that are taking a medication that requires step-therapy
or prior authorization have until February 1, 2023 to renew this with United Healthcare. You are allowed one fill of that
medication in the month of January, but you must call 1-866-314-0335 to override this requirement prior to your purchase.
This is a one-time exception for this Open Enrollment. Please do not call prior to January 1, 2023.
Mail Order is available through Optum Rx. For more info, call: 1-800-444-6222.
This document is intended to provide a brief summary of our benefit plans and is not a guarantee of coverage. For a complete description of plan
features, including eligibility and termination requirements, definitions, limitations and exclusions, please refer to your insurance booklet/certificate
and Summary Plan Description (SPD). The company reserves the right to change plan provisions in whole or in part as it deems necessary.12 | P a g e
HEALTH SAVINGS ACCOUNTS (HSA)
If you enroll in Plan 5– you may be eligible to open a Health Savings Account.
A Health Savings Account is a tax-advantaged medical savings account that is available to employees participating in the High
Deductible Health Plan (HDHP). The money you contribute to your HSA is tax-deductible and can be used to pay for qualified
expenses not only for yourself, but also for your spouse and tax dependents. Once you put money in your HSA, you can use it
to pay for qualified medical, dental and vision expenses now, or save and grow your balance to use later in life or in
retirement—all tax-free. Remember to contribute up to the maximum annual amount allowed by the IRS to maximize your
tax savings.
Annual Limits
Maximum Health Savings Account Contributions Per Year 2022 2023
Self-only coverage $3,650 $3,850
Family Coverage $7,300 $7,750
Catch Up (Age 55 & Older) $1,000 $1,000
You may not contribute to an HSA if you are covered by any other health plan, Including Medicare A & B.
HSA Deposits – The University will direct your HSA deposit to HSA Bank. You must open an account with HSA Bank online. Please see
Human Resources for more information. To open an account with HSA Bank please register on
https://secure.hsabank.com/group_enrollment/enrollment.aspx?id=943283324
Qualified medical expenses and your HSA Paying for qualified medical expenses such as doctor’s visits and prescription
medications is simple and tax-free. The money you contribute to your HSA is tax-deductible and can be used to pay for
qualified medical expenses not only for yourself, but also for your spouse and tax dependents.
HSA Eligibility Any individual who meets the following criteria is eligible for an HSA:
▪ Is covered by an HDHP;
▪ Is not covered by other health insurance;
▪ Is not enrolled in Medicare; and/or
▪ Can’t be claimed as a dependent on someone else’s tax return (children cannot establish their own HSAs).
Important reminders about qualified medical expenses Items that are merely beneficial to an individual’s general good
health, such as vitamins or dietary supplements, are not qualified medical expenses.
▪ Items that are merely beneficial to an individual’s general good health, such as vitamins or dietary supplements, are
not qualified medical expenses.
▪ Drugs must be purchased legally.
▪ Remember to save your receipts for OTC medicines for tax purposes.
▪ There may be situations when your doctor recommends a treatment that will be good for your health, but it still may
be considered ineligible, such as a vacation.
▪ As the HSA owner, you are ultimately responsible for determining whether a healthcare expense is eligible for
reimbursement from your HSA.
▪ If an HSA expenditure is not used for a qualified medical expense, you will be required to pay income tax and a 20
percent penalty on the amount used. (The 20 percent penalty tax does not apply to payments made after your death
or disability, or after you reach age 65).
How do I manage my HSA? Your Health Savings Account (HSA) is your account; the HSA dollars are your dollars. Since you are
the account holder or HSA beneficiary, you manage your HSA account. You may choose when to use your HSA dollars or when
not to use your HSA dollars. HSA dollars pay for any eligible expense. Most commonly, the HSA account holder will use HSA
dollars to pay the out-of-pocket expenses (i.e., deductible and coinsurance) associated with their high deductible health plan.
What expenses are eligible for reimbursement from my HSA? HSA dollars may be used for qualified medical expenses
incurred by the account holder and his or her spouse and dependents. Qualified medical expenses are outlined within IRS
Section 213(d). In summary the IRS Section 213(d) states that “the expense has to be primarily for the prevention or
alleviation of a physical or mental defect or illness.” In addition to qualified medical expenses, the following insurance
premiums may be reimbursed from an HSA:
▪ COBRA premiums
▪ Health insurance premiums while receiving unemployment benefits, Qualified long-term care premiums
▪ Qualified long-term care premiums
▪ Any health insurance premiums paid, other than for a Medicare supplemental policy, by individuals ages 65 and over
Are dental and vision care qualified medical expenses under an HSA? Yes, as long as these are deductible under the current
rules. For example, cosmetic procedures, like cosmetic dentistry, would not be considered qualified medical expenses.
This document is intended to provide a brief summary of our benefit plans and is not a guarantee of coverage. For a complete description of plan
features, including eligibility and termination requirements, definitions, limitations and exclusions, please refer to your insurance booklet/certificate
and Summary Plan Description (SPD). The company reserves the right to change plan provisions in whole or in part as it deems necessary.P a g e | 13
HEALTH SAVINGS ACCOUNTS (HSA)
Frequently Asked Questions about HSA Plan Usage
Can I use my HSA dollars for non-eligible expenses? Money withdrawn from an HSA account to reimburse non-eligible
medical expenses is taxable income to the account holder and is subject to a 20 percent tax penalty - unless over age 65,
disabled or upon death of the account holder.
What expenses are NOT eligible for reimbursement from my HSA? The following expenses may not be reimbursed:
▪ Premiums for Medicare supplemental policies
▪ Expenses covered by another insurance plan
▪ Expenses incurred prior to the date the HSA was established
What is a coverage gap? This is the gap between total out-of-pocket expenses associated with your high deductible health
plan and your HSA dollars. For example, assume that you have a $2,000 deductible, a $4,000 maximum out-of-pocket, and
either you or your employer has contributed $2,000 to your HSA account. If your medical costs incurred exceed $4,000 for
the year, then you are financially obligated to pay the difference between your total maximum out-of-pocket ($4,000) and
your HSA balance ($2,000) - ($4,000 - $2,000 = $2,000).
What happens when my HSA funds run out? You may be financially responsible for any eligible medical expenses that fall
within the coverage gap.
When can I start using my HSA dollars? You can use your HSA dollars immediately following your HSA account activation and
once contributions have been made.
When do I contribute to my HSA account, and how often can I? You, your employer or others can contribute to your HSA
account through payroll deductions or as a lump sum deposit. You can contribute as often as you like, provided your (and
your employer’s) total annual contributions do not exceed the annual limits.
How do I pay my physician or network facility at time of service with my HSA dollars? You may request that the network
provider submit your claim to your health plan. You should make sure that your provider has your most up-to-date insurance
information. Once the medical claim has been processed, if applicable, out-of-pocket expenses will be billed. At this time, you
may choose to use your HSA debit card or HSA check to pay for any out-of-pocket expenses, or you may choose to pay with
your own money and receive reimbursement at a later date. You should always ask that your medical claim be submitted to
the health plan before you seek reimbursement from your HSA. This procedure will ensure that provider discounts are
applied. Also, remember to keep all medical receipts and Explanation of Benefits (EOBs).
What if I have HSA dollars left in my account at year-end? The money is yours to keep. It will continue to earn interest and
will be available for you and your health care costs next year.
How do my remaining HSA dollars rollover at year-end? Any dollars left in your HSA account at year-end will automatically
roll over into next year’s HSA account.
What happens to my HSA dollars if I leave my employer? The funds are yours to keep. You may elect one of the following
options:
- Leave your funds in the current HSA account
- Transfer your funds to an HSA with your new employer
- Transfer your funds to another qualifying account within 60 days
Can my HSA dollars be used for retirement health care costs? Yes, only for expenses eligible for reimbursement.
Can I use the money in my account to pay for my dependents’ medical expenses? You can use the money in the account to
pay for medical expenses of yourself, your spouse or your dependent children. You can pay for expenses of your spouse and
dependent children even if they are not covered by your HDHP.
Can couples establish a “joint” account and both make contributions to the account, including “catch-up” contributions?
“Joint” HSA accounts are not permitted. Each spouse should consider establishing an account in their own name. This allows
you to both make catch-up contributions when each spouse is 55 or older.
My employer offers an FSA – can I have both an FSA and an HSA? You can have both types of accounts, but only under
certain circumstances. General Flexible Spending Accounts (FSAs) will probably make you ineligible for an HSA. If your
employer offers a “limited purpose” (limited to dental, vision or preventive care) or “post-deductible” (pay for medical
expenses after the plan deductible is met) FSA, then you can still be eligible for an HSA.
Can I shift my IRA funds to my HSA? Owners of individual retirement accounts that are enrolled in a high deductible health
plan can shift IRA funds to an HSA without facing a tax penalty. The IRS allows a one-time transfer that does not exceed your
maximum HSA contribution limit.
Can I borrow against the money in my HSA? No. You may not borrow against it or pledge the funds in it. For more
information on prohibited activities, see Section 4975 of the Internal Revenue Code.
Can the funds in an HSA be invested? Yes, you can invest the funds in your HSA. The same types of investments permitted
for IRAs are allowed for HSAs, including stocks, bonds, mutual funds, and certificates of deposit.
This document is intended to provide a brief summary of our benefit plans and is not a guarantee of coverage. For a complete description of plan
features, including eligibility and termination requirements, definitions, limitations and exclusions, please refer to your insurance booklet/certificate
and Summary Plan Description (SPD). The company reserves the right to change plan provisions in whole or in part as it deems necessary.14 | P a g e
Know Your Health Care FSA Eligible and Ineligible Expenses
Maximize the Value of Your Reimbursement Account | Effective January 1st, 2021
Your Health Care Flexible Spending Account (FSA) dollars can be used for a variety of out-of-pocket health care
expenses. The following is based on a list of eligible and ineligible expenses used by federal employees.
Eligible Expenses
BABY/CHILD TO AGE 13 MEDICAL EQUIPMENT/SUPPLIES MEDICATIONS
• Lactation Consultant* • Air Purification Equipment* • Insulin
• Lead-Based Paint Removal • Arches and Orthotic Inserts • Prescription Drugs
• Special Formula* • Contraceptive Devices
• Tuition: Special School/Teacher for • Crutches, Walkers, Wheel Chairs OBSTETRICS
Disability or Learning Disability* • Exercise Equipment* • Breast Pumps and Lactation Supplies
• Well Baby /Well Child Care • Hospital Beds* • Doulas*
• Mattresses* • Lamaze Class
DENTAL • Medic Alert Bracelet or Necklace • OB/GYN Exams
• Dental X-Rays • Nebulizers • OB/GYN Prepaid Maternity Fees
• Dentures and Bridges • Orthopedic Shoes* (reimbursable after date of birth)
• Exams and Teeth Cleaning • Oxygen* • Pre- and Postnatal Treatments
• Extractions and Fillings • Post-Mastectomy Clothing
• Oral Surgery • Prosthetics PRACTITIONERS
• Orthodontia • Syringes • Allergist
• Periodontal Services • Masks • Chiropractor
• Wigs* • Christian Science Practitioner
EYES • Dermatologist
• Eye Exams MEDICAL PROCEDURES/SERVICES • Homeopath
• Eyeglasses and Contact Lenses • Acupuncture • Naturopath*
• Laser Eye Surgeries • Alcohol and Drug/Substance Abuse • Optometrist
• Prescription Sunglasses (inpatient treatment and outpatient care) • Osteopath
• Radial Keratotomy • Ambulance • Physician
• Fertility Enhancement and Treatment • Psychiatrist or Psychologist
HEARING • Hair Loss Treatment*
• Hearing Aids and Batteries • Hospital Services THERAPY
• Hearing Exams • Immunization • Alcohol and Drug Addiction
• In Vitro Fertilization • Counseling (not marital or career)
LAB EXAMS/TESTS • Physical Examination (not employment-related) • Exercise Programs*
• Blood Tests and Metabolism Tests • Reconstructive Surgery (due to a congenital • Hypnosis
• Body Scans defect, accident, or medical treatment) • Massage*
• Cardiograms • Service Animals • Occupational
• Laboratory Fees • Sterilization/Sterilization Reversal • Physical
• X-Rays • Transplants (including organ donor) • Smoking Cessation Programs*
• Transportation* • Speech
• Weight Loss Programs*
Note: This list is not meant to be all-inclusive, as other expenses not specifically mentioned may also qualify. Also, expenses marked with an
asterisk (*) are “potentially eligible expenses” that require a Note of Medical Necessity from your health care provider to qualify for
reimbursement. For additional information, check your Summary Plan Document or contact your Plan Administrator.
This document is intended to provide a brief summary of our benefit plans and is not a guarantee of coverage. For a complete description of plan
features, including eligibility and termination requirements, definitions, limitations and exclusions, please refer to your insurance booklet/certificate
and Summary Plan Description (SPD). The company reserves the right to change plan provisions in whole or in part as it deems necessary.P a g e | 15
Eligible Over-the-Counter Medicines and Drugs
• Acid controllers • Cough, cold & flu • Medicated nasal sprays, drops,
• Acne medications • Denture pain relief & inhalers
• Allergy & sinus • Digestive aids • Medicated respiratory treatments
• Antibiotic products • Ear care & vapor products
• Antifungal (Foot) • Eye care • Motion sickness
• Antiparasitic treatments • Feminine antifungal & anti-itch • Oral remedies or treatments
• Antiseptics & wound cleansers • Fiber laxatives (bulk forming) • Pain relief (includes aspirin)
• Anti-diarrheals • First aid burn remedies • Skin treatments
• Anti-gas • Foot care treatment • Sleep aids & sedatives
• Anti-itch & insect bite • Hemorrhoidal preps • Smoking deterrents
• Baby rash ointments & creams • Homeopathic remedies • Stomach remedies
• Baby teething pain • Incontinence protection & treatment • Unmedicated nasal sprays,
drops & inhalers
• Cold sore remedies products
• Laxatives (non-fiber) • Unmedicated vapor products
• Contraceptives
• Menstrual Products
Eligible Over-the-Counter Items (Product categories are listed in bold face; common examples are listed in regular face.)
• Baby Electrolytes and Dehydration • Elastics/Athletic Treatments • Hearing Aid/Medical Batteries
• Pedialyte, Enfalyte • ACE, Futuro, elastic bandages, braces, • Home Health Care (limited segments)
• Contraceptives hot/cold therapy, orthopedic supports, • Ostomy, walking aids, decubitis/pressure
• Unmedicated condoms rib belts relief, enteral/parenteral feeding supplies,
• Denture Adhesives, Repair, and Cleansers • Eye Care patient lifting aids, orthopedic
• PoliGrip, Benzodent, Plate Weld, • Contact lens care braces/supports, splints & casts,
• Family Planning hydrocollators, nebulizers, electrotherapy
Efferdent
products, catheters, unmedicated wound
• Diabetes Testing and Aids • Pregnancy and ovulation kits
care, wheel chairs
• Ascencia, One Touch, Diabetic Tussin, • First Aid Dressings and Supplies
• Incontinence Products
insulin syringes; glucose products • Band Aid, 3M Nexcare, non-sport tapes
• Attends, Depend, GoodNites for
• Diagnostic Products • Foot Care Treatment
juvenile incontinence, Prevail
• Thermometers, blood pressure monitors, • Unmedicated corn and callus treatments
• Prenatal Vitamins
cholesterol testing (e.g., callus cushions), devices, therapeutic
• Stuart Prenatal, Nature's Bounty
• Ear Care insoles
Prenatal Vitamins
• Unmedicated ear drops, syringes, • Glucosamine &/or Chondroitin
• Reading Glasses and Maintenance
ear wax removal • Osteo-Bi-Flex, Cosamin D, Accessories
Flex-a-min Nutritional Supplements
• Hand Sanitizer & Hand Wipes
OTC items that are not medicines or drugs remain eligible for purchase with FSAs. You can use your
benefits card for these items.
Ineligible Expenses
• Contact Lens or Eyeglass Insurance • Insurance Premiums and Interest • Personal Trainers
• Cosmetic Surgery/Procedures (FSA Ineligible Only) • Sunscreen (spf less than 30)
• Electrolysis • Long Term Care Premiums • Swimming Lessons
(FSA Ineligible Only)
• Marriage or Career Counseling
Note: This list is not meant to be all-inclusive.
This document is intended to provide a brief summary of our benefit plans and is not a guarantee of coverage. For a complete description of plan
features, including eligibility and termination requirements, definitions, limitations and exclusions, please refer to your insurance booklet/certificate
and Summary Plan Description (SPD). The company reserves the right to change plan provisions in whole or in part as it deems necessary.16 | P a g e
This document is intended to provide a brief summary of our benefit plans and is not a guarantee of coverage. For a complete description of plan
features, including eligibility and termination requirements, definitions, limitations and exclusions, please refer to your insurance booklet/certificate
and Summary Plan Description (SPD). The company reserves the right to change plan provisions in whole or in part as it deems necessary.P a g e | 17
PROGRESSIVE BENEFITS SOLUTIONS (PBS) – FLEXIBLE SPENDING ACCOUNTS
Medical Reimbursement Account
What Is It? Tax sheltered account which allows you to use tax-free dollars to pay for medical,
dental, and vision expenses not covered by insurance.
Estimate your contributions carefully – excess contributions are subject to forfeiture.
Minimum Contribution $260 per plan year
Maximum Contribution $3,050 per plan year
Rollover – Medical Rollover Provision for 2022-2023: $570
Reimbursement Account
Rollover Provision for 2023-2024: $610
The rollover amount is not subject to the “use it or lose it” regulations and can be
added to your 2023 plan election (e.g. if you select $1,000 for your 2023 election and
have a rollover of $610 you can access $1,500 for that plan year).
Grace Period – Dependent
Care Account
Please note: you must elect to contribute at least $260 for the new plan year to be
eligible to access any and all Rollover Funds. If you do not contribute for the plan year you
forfeit any rollover funds available.
Additional Information If you are contributing to both an HSA and an FSA, the FSA will become limited use and
can only be used for dental, vision, or eligible over-the-counter expenses until your
HDHP deductible is met.
Dependent Care Account (DCA)
What Is It? Tax sheltered account which allows you to use tax-free dollars to pay for child and
elder care.
Estimate your contributions carefully – excess contributions are subject to forfeiture.
Minimum Contribution N/A
Maximum Contribution $5,000 per year ($2,500 per year if married and filing separately)
Rollover – Medical The grace period still applies, legislation allows employers who sponsor dependent
Reimbursement Account care FSA’s to add an extension of time at the end of the plan year during which
employees may incur eligible expenses and be reimbursed from their FSA funds. This
extension of time is called a grace period.
This means you have more time to spend your dependent care account (DCA) funds so
you will be less likely to forfeit any of your money.
Grace Period – Dependent
Care Account As a participant in a DCA you could normally submit claims incurred during the plan
year only. The effect of the grace period is that if you have unspent flex account dollars
at the end of November, you will still have until March15th to submit claims for the
previous plan year and the current plan year.
Additional Information Reimbursement for childcare is allowed for dependents up to age 13 only.
The first time you enroll in a reimbursement or dependent care account, you will receive TWO cards in the mail at home, along with
important information on using the Benny Cards. Your cards are valid for 5 years. Please use your cards until their expiration date or
from one plan year to another. You will not be sent new cards until your cards expire.
▪ ACTIVATE and SIGN your cards
▪ If your spouse or dependent will be using the second card, have them sign the back of the second card.
▪ The Benny Cards take 2 hours to become active from the time of activation.
Life insurance provides your loved ones with financial protection if you die. It can help pay your final expenses, or make mortgage,
or tuition payments. If you die as a result of an accident, AD&D will double your employer paid life insurance benefit. It will also
provide benefits for accidental: loss of eyesight, hearing or speech, loss of a limb, loss of limb due to paralysis, disfiguring third-
degree burns or coma.
This document is intended to provide a brief summary of our benefit plans and is not a guarantee of coverage. For a complete description of plan
features, including eligibility and termination requirements, definitions, limitations and exclusions, please refer to your insurance booklet/certificate
and Summary Plan Description (SPD). The company reserves the right to change plan provisions in whole or in part as it deems necessary.18 | P a g e
NEW CARRIER! UNITED HEALTHCARE –
VOLUNTARY DENTAL INSURANCE
PPO Low Plan PPO High Plan
In-Network Out-of-Network In-Network Out-of-Network
Deductible $50 Individual / $150 Family $50 Individual / $150 Family
Calendar Year Maximum $1,000 per covered person $2,000 per covered person
Preventive Services
Oral Exams Cleanings 100% (No Deductible) 100% (No Deductible)
Routine X-Rays
Basic Services
Fillings
80% After Deductible 80% After Deductible
Oral Surgery
Periodontics
Major Services
Crowns
50% After Deductible 50% After Deductible
Dentures
Bridges
Orthodontia 50% to $1,000 Lifetime Maximum* N/A
th
Reimbursement* N/A 90 Percentile N/A 90th Percentile
*Orthodontia – Coverage is for children up to age 19
Deductible is combined for Basic and Major services.
Bi-Weekly Rates: PPO Low Plan PPO High Plan
Employee $15.02 $22.33
Employee & Spouse $34.24 $44.42
Employee + Child(ren) $29.71 $44.18
Employee + Family $47.42 $70.40
Find a Dental Provider:
1. Visit www.myuhc.com and click “Find a Dentist”
2. Click “Employer and Individual Plans”
3. Enter your location to find a plan
4. Select your dental plan: “National Options PPO 30”
5. Search for providers and services or search by category
*Out-of-Network Reimbursement – Out-of-Network reimbursement is based on the maximum allowable
amount. Members are responsible to pay any charges in excess of this amount. Please refer to your employer’s
health plan description for more information.
*Please see your plan summaries and booklet certificates on Employee Navigator for the full and detailed coverages
and exclusions*
This document is intended to provide a brief summary of our benefit plans and is not a guarantee of coverage. For a complete description of plan
features, including eligibility and termination requirements, definitions, limitations and exclusions, please refer to your insurance booklet/certificate
and Summary Plan Description (SPD). The company reserves the right to change plan provisions in whole or in part as it deems necessary.P a g e | 19
NEW CARRIER! UNITED HEALTHCARE –
VOLUNTARY DENTAL INSURANCE
For Voluntary Dental ID cards: Dental ID cards are not sent out. You can access them online with the steps below or
use the United Healthcare app to access your ID card.
To access ID cards, enrolled members can create a secure member account at myuhc.com using the following instructions.
1. Go to www.myuhc.com
2. For new members, select “Register”.
3. Enter your Name, Date of Birth, & your Member ID (this is not the same as SSN). If you do not know your
Member ID, then enter the last 4 digits of your SSN along with your zip code.
4. Create a username and password. Your access will then be complete and you will be free to navigate the site.
5. Once logged in, select “Print ID Card.” (If you do not see this option, click on the blue “select” button next to
your plan name.)
6. From the drop-down menu, select the person whose ID card you would like to print. Then click “Get ID Card.”
7. This generates a document with your ID card. Scroll to the bottom of this document where a toolbar will
appear. Click on the printer icon to print.
Download the UnitedHealthcare App for Member ID cards, finding doctors, and more!
This document is intended to provide a brief summary of our benefit plans and is not a guarantee of coverage. For a complete description of plan
features, including eligibility and termination requirements, definitions, limitations and exclusions, please refer to your insurance booklet/certificate
and Summary Plan Description (SPD). The company reserves the right to change plan provisions in whole or in part as it deems necessary.20 | P a g e
NEW CARRIER! AMERITAS VOLUNTARY VISION INSURANCE
VSP Choice - Focus EyeMed Select - ViewPointe
In-Network Out-of-Network In-Network Out-of-Network
Deductibles $10 Exam
$10 Exam
$25 Eye Glass Lenses or No Deductible
$25 Eye Glass Lenses or Frames*
Frames*
Annual Eye Exam Covered in full Up to $45 Covered in full Up to $35
Lenses (per pair)
Single Covered in full Up to $30 Covered in full Up to $25
Bifocal Covered in full Up to $50 Covered in full Up to $40
Trifocal Covered in full Up to $65 Covered in full Up to $55
Lenticular Covered in full Up to $100 20% discount No benefit
Frames Up to $130 Up to $70 Up to $130 Up to $65
Frequencies
12/12/12 12/12/12
Exam/Lens/Frames
Contact Lenses Fit & Standard: Member cost up
Follow Up Member cost up to $60 No benefit to $40; Premium: 10% off No benefit
of retail
Elective Contacts Up to $130 Up to $105 Up to $130
Up to $104
Medically Necessary
Covered in full Up to $210 Covered in full Up to $200
Contacts
Sample In-Network More private providers and Costco, Cohens, & More national retailers - Lenscrafters, Target,
Locations Visionworks Pearle Vision, Sears, JCP
*Deductible applies to a complete pair of glasses or to frames, whichever is selected.
Additional lens options (including progressives can be found on the full benefit summary located in the Documents or
Resources tab in Employee Navigator. These can be accessed at any time). Plan discounts may not be combined with
any other discounts or promotional offers.
Bi-Weekly Costs –
VSP Choice - Focus EyeMed Select - Viewpointe
Employee $2.75 $2.75
Employee & Spouse $5.50 $5.50
Employee & Child(ren) $5.54 $5.54
Family $8.84 $8.84
ID CARDS – Are not needed however, Ameritas will send ID cards to members home address. Any participating
provider will be able to find coverage information using the employee’s SSN and date of birth. Dependents will not
receive their own ID card.
VSP Additional Information – Member Services: 1-800-877-7195
Register on the www.vsp.com to view policy information, claims, and to print out ID cards. You can also search for
providers using their Find a Provider search tool.
EyeMed Additional Information – Member Services: 1-866-289-0614
Register on the www.eyemed.com to view policy information, claims, and to print out ID cards. You can also search for
providers using their Find a Provider search tool.
This document is intended to provide a brief summary of our benefit plans and is not a guarantee of coverage. For a complete description of plan
features, including eligibility and termination requirements, definitions, limitations and exclusions, please refer to your insurance booklet/certificate
and Summary Plan Description (SPD). The company reserves the right to change plan provisions in whole or in part as it deems necessary.P a g e | 21
NEW CARRIER! LINCOLN FINANCIAL
BASIC LIFE & AD&D INSURANCE
100% Company Paid
Benefit
Coverage 2x of base salary up to a maximum of $200,000
50% at age 70
Reduction Schedule
Benefits terminate upon retirement
▪ Conversion options are available on Basic Life and AD&D coverage as long as you apply within 30
days of your loss of eligibility.
▪ Portability is available as long as the coverage was in-force at least 12 months prior to
termination of employment and the insured must not be disabled, on a leave of absence, or
retired. Please see Human Resources for more information.
This document is intended to provide a brief summary of our benefit plans and is not a guarantee of coverage. For a complete description of plan
features, including eligibility and termination requirements, definitions, limitations and exclusions, please refer to your insurance booklet/certificate
and Summary Plan Description (SPD). The company reserves the right to change plan provisions in whole or in part as it deems necessary.22 | P a g e
NEW CARRIER! LINCOLN FINANCIAL
VOLUNTARY LIFE INSURANCE
100% Employee Paid
GUARANTEE ISSUE AVAILABLE TO ALL EMPLOYEES DURING THE 01/01/2023 OPEN
ENROLLMENT
Employee Spouse Child(ren)
New Hire Guarantee Issue $300,000 $30,000 $10,000
Guarantee Issue during
Open Enrollment – as of Employees & Spouses can elect or increase coverage 2 benefit levels without underwriting approval.
01/01/2023
Increments of $10,000.
• 6 months to age 26 guaranteed
Not to exceed 5 times the
Increments of $5,000. Not to coverage amount = $10,000
employee’s annual salary.
exceed 50% of the employee’s • Live birth to 6 months guaranteed
Benefit Available Rounded to the next
benefit amount. Rounded to the coverage amount = $500
higher $10,000.
next higher $5,000. • Employee coverage is required to
Benefit Maximum =
elect child(ren) coverage.
$500,000
50% at age 70
Spouse rates are based on
50% at age 70 employee age. Coverage
Reduction Schedule N/A
Terminates at retirement terminates at Employee age 70 or
retirement; whichever occurs
first.
For this Open Enrollment only, Guarantee Issue applies to all eligible employees. If you have previously waived coverage, you
will have the opportunity to elect coverage, up to the Guarantee Issue amount without being subject to underwriting
approval. If you enrolled in benefits previously and it is above the guaranteed issue amount, this coverage will be
grandfathered by Lincoln, and you do not need to complete an evidence of insurability form to continue this coverage.
After the 01/01/2023 Open Enrollment:
• New Hire Guarantee Issue amounts are only available to new hires in their initial eligibility period. Any amounts over
the Guarantee Issue levels will require the completion and submission of an Evidence of Insurability form to be
reviewed by underwriting for approval.
• Current Employees: During open enrollment each year, you may elect to increase your current coverage amount by 2
benefit levels on a Guarantee Issue basis. This means that employees and/or spouses can increase coverage without
having to complete an Evidence of Insurability form, up to the maximum benefit amount as long as you or your spouse
have not been previously declined for coverage.
Additional Information:
• The maximum coverage for new employees that are 70 and over is $50,000
• Employee coverage is rounded to the next higher of $10,000 benefit and spouse coverage is rounded to
the next higher $5,000 benefit.
• Employee coverage is required for spouse and child(ren) to elect coverage
• Spousal rates are based on the employee’s age.
• Conversion options are available on Voluntary Life coverage as long as you apply within 30 days of your
loss of eligibility. Portability is available as long as the coverage was in-force at least 12 months prior to
termination of employment and the insured must not be disabled, on a leave of absence, or retired.
Please see Human Resources for more information.
• You must be actively at work on your effective date. If you are not actively at work on the day before
your scheduled effective date, your coverage will not become effective until the day after you complete
one full day of active work as an eligible employee.
Your personalized rates can be found on Employee Navigator.
This document is intended to provide a brief summary of our benefit plans and is not a guarantee of coverage. For a complete description of plan
features, including eligibility and termination requirements, definitions, limitations and exclusions, please refer to your insurance booklet/certificate
and Summary Plan Description (SPD). The company reserves the right to change plan provisions in whole or in part as it deems necessary.You can also read