Enrollmen Ki 2022-23 Academi Yea - Squarespace
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
2022-23 Academic Year Enrollment Kit

A message from our Head of School... Welcome to The Vanguard School. Vanguard is a community of teachers, residential faculty, administrators, and staff all dedicated to the mission of preparing students for higher educational opportunities and independent life. We function as a close and committed community of students, families, faculty, residential faculty, and staff. Please complete this Enrollment Kit as we try to help set expectations and safety procedures for our students. We value your dedication to our mission and commitment to hard work, and we encourage open, direct, and respectful communication. It is in this spirit that this Enrollment Kit has been assembled. Working together, we strive to create an exceptional residential educational experience for our students and a rewarding and invigorating environment to grow as individuals. Our families entrust their most precious assets - your children - to us. We take this trust seriously and strive to meet and then exceed our community's high expectations. The Mission and Vision of Vanguard School are at the heart of everything we do. No matter what the employee’s role at the school, their work is essential to achieving our high goals, and to providing an exceptional experience for students. Please take the time to become familiar with the packet and complete the Kit. Great care has been taken to put into one document all the necessary forms and to clearly outline the paperwork. Though we have tried to consider all aspects of the student experience at Vanguard School, please know that if at any point you have questions or concerns regarding policies and forms that follow or anything else in your role as a parent, I encourage you to ask our Admissions Team Susi Vacek or Aubrie Brooks for guidance or assistance. Thank you for being part of our tight-knit Vanguard Community - and for taking this role in your child’s education by giving them a Vanguard experience where students learn to build confidence to feel comfortable academically, socially, and emotionally to reach their potential. Sincerely, L. Shannon Graves Head of School

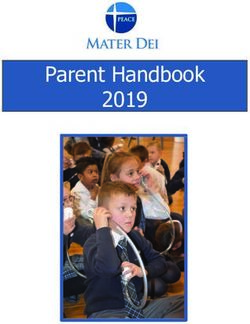
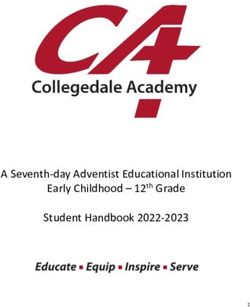
AUG 16 Res Staff Return JAN 8-9 Boarding Students Return /New
SEMESTER 2
17 All Employee Return/Training Students Begin
SEMESTER 1
21 Boarding Student Registration 9-10 Orientation
22 Day Student Registration 11 Term 3 Begins (Semester 2)
22-24 Orientation 16 Martin Luther King, Jr. Day /
25 Term 1 Begins Community Service
SEP 5 Labor Day FEB 20 President's Day (School is In-Session)
OCT 21 Term 1 Ends MAR 10 Term 3 Ends
24 Term 2 Begins 11 Travel Day
NOV 24-27 Fall Break 11-18 Spring Break
DEC 13-16 Semester 1 Exams 19 Travel Day
16 Term 2 Ends 19 Graduation
MAY
17 Travel Day 22-24 Semester 2 Exams
18 - 1/9 Winter Break 25-26 Faculty Work Days
AUGUST SEPTEMBER OCTOBER
MO TU WE TH FR SA SU MO TU WE TH FR SA SU MO TU WE TH FR SA SU
1 2 3 4 5 6 7 1 2 3 4 1 2
8 9 10 11 12 13 14 5 6 7 8 9 10 11 3 4 5 6 7 8 9
15 16 17 18 19 20 21 12 13 14 15 16 17 18 10 11 12 13 14 15 16
22 23 24 25 26 27 28 19 20 21 22 23 24 25 17 18 19 20 21 22 23
29 30 31 26 27 28 29 30 24 25 26 27 28 29 30
31
NOVEMBER DECEMBER JANUARY
MO TU WE TH FR SA SU MO TU WE TH FR SA SU MO TU WE TH FR SA SU
1 2 3 4 5 6 1 2 3 4 1
7 8 9 10 11 12 13 5 6 7 8 9 10 11 2 3 4 5 6 7 8
14 15 16 17 18 19 20 12 13 14 15 16 17 18 9 10 11 12 13 14 15
21 22 23 24 25 26 27 19 20 21 22 23 24 25 16 17 18 19 20 21 22
28 29 30 26 27 28 29 30 23 24 25 26 27 28 29
30 31
FEBRUARY MARCH APRIL
MO TU WE TH FR SA SU MO TU WE TH FR SA SU MO TU WE TH FR SA SU
1 2 3 4 5 1 2 3 4 5 1 2
6 7 8 9 10 11 12 6 7 8 9 10 11 12 3 4 5 6 7 8 9
13 14 15 16 17 18 19 13 14 15 16 17 18 19 10 11 12 13 14 15 16
20 21 22 23 24 25 26 20 21 22 23 24 25 26 17 18 19 20 21 22 23
27 28 27 28 29 30 31 24 25 26 27 28 29 30
MAY
MO TU WE TH FR SA SU
A C A D E M I C
1 2 3 4 5 6 7
C A L E N D A R
8 9 10 11 12 13 14
15 16 17 18 19 20 21
22
29
23
30
24
31
25 26 27 28
2022-2023
The Vanguard School
2022-23 Bell Schedule
7:40 - 8:20 Breakfast
8:30 - 8:45 Mentor Period
8:50 - 9:35 Period 1
9:40 - 10:25 Period 2
10:25 - 10:35 Break
10:35 - 11:20 Period 3
11:25 - 12:05 Period 4
12:05 - 12:50 Lunch
12:50 - 1:35 Period 5
1:40 - 2:25 Period 6
2:25 - 2:40 Break
2:40 - 3:25 Period 7
3:30 - 4:15 Study Hall
THE VANGUARD SCHOOL
RESIDENTIAL STUDENT PACKING LIST
This list is a recommendation to assist your child pack for school.
Please identify your child’s clothing items with the student’s name or initial labels or sewn-in
name tags. Stickers will not survive the laundering process.
Students are encouraged to personalize their rooms, as this is their “home away from home”.
All students are responsible for the care and maintenance of their personal space, as the
responsibility of all personal items will be reflected in room checks by residential staff. We
recommend the rule of thumb that all student items should fit in one carload. Items may be
mailed/delivered to The Vanguard School ahead of registration with name of student listed.
All Students:
1 laundry mesh or canvas bag (labeled with name) 10 1 pair each: shower shoes, gym shoes,
day (min.) supply of undergarments including socks 1 casual shoes, and rain shoes/boots
large beach towel Clothing hangers
2 options of appropriate swimwear 1 Raincoat/jacket/poncho
4-5 pairs of blue jeans Belts (optional)
OR Mix/Match Shower/Hygiene items
4-8 pairs of casual/dress shorts or casual pants (solid 4 bath towels and 4 washcloths
khaki, black, grey, navy, or blue jeans) 1 shower caddy
Bedspread/comforter/sleeping bag
2 sets Twin XL sheets with pillowcases, Masks - optional with appropriate
2-4 Sleepwear sets images or logo
1 study lamp
Alarm clock or equivalent 2 athletic supporters (Students in
athletics)
VANGUARD UNIFORM DRESS CODE ITEMS - Mandatory
1-2 hoodies/sweatshirts (Purchased through Vanguard)
5 Vanguard polo shirts (option of 4 Vanguard polo shirts
and 1 Vanguard T-shirt only for Fridays)
Formal Meal Dress Options - Mandatory
Oxford dress shirts with a tie, jacket, dress pants, dress
shoes, dress, blouse, or skirt
OPTIONAL ITEMS:
42 inch TV or smaller
Air purifying fan
Bicycle/skateboard/rollerblades/skates
(Helmet for students under 16 years unless signed
permission from parent/guardian)
Section1: Medical The Vanguard School 2022 - 23 Enrollment Kit

The Vanguard School
2022-23 Academic Year
Medical Management Information
Student Name_____________________________________________
DOB_________________________
Please indicate the choice applicable to your student:
_____ My child is a boarding student who will take medications at school this year.
_____ My child is a day student who will take medications at home this
year.
_____ My child is a day student who will take medications at school this year.
_____ My child is not currently taking any medications.
Please indicate your current or preferred pharmacy for your child’s prescriptions:
_____ CVS Pharmacy
_____ Publix Pharmacy
_____ Walgreens Pharmacy
_____ Other:____________________________________________
For medical distribution, we are recommending the use of pill-pack services from your
preferred pharmacy when it is available for student medications. This increases the accuracy
of medical distribution as all, or most, student medications are sent to the school with the
student’s name, medication name, dosage, and time for distribution. Many pharmacies now
offer this service. There may be exceptions to this option, but we do ask parents to inquire if it is
an option for any ongoing medication prescriptions. Be aware that supplements, vitamins,
over-the-counter, or dietary substances must be turned in to our MedTeam for monitored
intake.
_________ ________All prescriptions will be strictly followed as indicated by the prescribing doctor. Any adjustments or cessation of medications must come from the physician. _________ ________Medications are packaged and travel with students over the breaks or any extended periods returning home. Medication Name / Dosage Time 1_______________________________________________________________________ 2_______________________________________________________________________ 3_______________________________________________________________________ 4_______________________________________________________________________ 5_______________________________________________________________________ Allergies Please list all known student allergies: 1______________________________________ _____Epipen 2______________________________________ _____Epipen 3______________________________________ _____Epipen 4______________________________________ _____Epipen 5______________________________________ _____Epipen Student Name___________________________________________________________________

Insurance Company___________________________________________________
Policy Number_________________________________
Group Number_________________________________
Primary Insurance Holder Name_________________________________________
DOB___________________________
Primary Insurance Holder’s SSN____________________________________
The Vanguard School must receive a copy of the insurance card. All students are
required to have individual health insurance or be covered on a family policy.
International Students Options:
iNext https://www.inext.com/plans/travel-to-usa/academic
ISI https://www.internationalstudentinsurance.com/student-health-insurance/
If you have any questions, please contact Jae Allen jae.allen@vanguardschool.org, or our
Medical Services medteam@vanguardschool.org.
Child’s Primary Physician____________________________________________________
Location_______________________________________________________
Phone_________________________________________________________
Child’s Primary Psychiatrist__________________________________________________
Location_______________________________________________________
Phone_________________________________________________________
Child’s Primary Psychologist/Counselor______________________________________
Location_______________________________________________________
Phone_________________________________________________________
Student Name___________________________________________________________________
History Please indicate if your child has a history of any of the following: _____Cardiac or circulatory issues _____Respiratory problems including asthma _____Kidney, bladder, or urinary problems including bedwetting _____Back, neck, or spinal problems _____Musculoskeletal problems (ex. shoulders, legs, feet, etc) _____Vision or auditory issues _____Gastrointestinal problems, including constipation or diarrhea _____Skin issues _____Diabetes _____Head injuries or brain issues (ex. seizures, migraines, chronic headaches) _____Psychological issues or treatments _____Substance use or abuse _____Major surgery or hospitalization _____Dietary Restrictions or eating disorders _____Exercise or physical restrictions _____Motion Sickness _____Physical, mental, or psychological condition requiring social restrictions, considerations, or limits to your child participation in specific activities For any indication above, please explain: _____________________________________________________________________________ _____________________________________________________________________________ _____________________________________________________________________________ Student Name___________________________________________________________________
Standing Orders FEVER: Acetaminophen (Tylenol) 325-1000 mg by mouth every 4 hours or Ibuprofen (Advil) 200-400 mg every 6 hours for fever over 101.0 F. DIARRHEA: Clear liquids – soup, clear juice, non-caffeinated soda, Gatorade until stools significantly slow or stop, then may increase the diet to BRAT (bananas, rice, applesauce, and toast/tea) or bland diet – No Milk. If not resolved in one day, may give Imodium as directed on the bottle. EARACHE: Tylenol or Advil and Sudafed as directed above. Observe ear for discharge. Consult MD if pain persists, there is discharge from the ear, or if the student has a fever. NAUSEA: If mild, Tums 2 tabs every 4 hours or Pepto Bismol 30 cc’s (2 tbsp.) every 4 hours. If severe, sips of clear liquids or NPO (Nothing by mouth) until symptoms subside. VOMITING: NPO (Nothing by mouth) until no vomiting for 2+ hours then may try sips of clear liquids. If severe, and continuous, consult MD. CONSTIPATION: Increase bulk/fiber and fluids, especially apple or prune juice. If not resolved, may give Milk of Magnesia as directed on the bottle. COUGH: Robitussin DM 10 cc’s (2 tsp) every 4 hours or 2-3 cough drops. INDIGESTION: See “NAUSEA” above. May also use antacid. Maalox as directed on the bottle. PAIN: (Headache & Muscle/Joint): Tylenol or Ibuprofen – see “FEVER” above for dosing. MILD/MODERATE ALLERGIC REACTION: Benadryl 25 mg by mouth, consult MD, or send to the hospital immediately if symptoms increase. SEVERE ALLERGIC REACTION: Epi-pen as directed if available. Send to hospital for evaluation. MINOR CUTS AND ABRASIONS: Cleanse wound(s) with mild soap and water, dry well. Apply triple antibiotic ointment and dry sterile dressing. May soak in betadine (Iodine) if irritated and the student is not allergic. NOSEBLEEDS: Apply direct pressure to the nose for 5 minutes. If bleeding does not subside, consult MD. May use Vaseline to protect mucous membranes. SKIN IRRITATION: (Sunburn, mild contact dermatitis, etc.): Apply soothing topical anesthetic lotion or spray (Bactine, Aloe Vera, Solarcaine, Cortaid, Lanacaine, Lotion, etc.) or ½ %-1% hydrocortisone cream. May also apply calamine lotion or cream. MUSCLE ACHES: See “PAIN” above. INSECT BITES: Apply ice to the area for at least 15-20 minutes upon initial sting. Wash area with mild soap and water, dry well. Apply ½ % - 1% hydrocortisone cream. Observe the student for allergic reactions.
SORE THROAT: Chloraseptic spray or lozenges every 2 hours. Consult MD if no relief in one day or if presents with fever or exudate on the throat. JOCK ITCH: Antifungal powder or cream to the affected area (after washing with soap and water and drying well) in the morning and at night as well as before and after athletic activities. ATHLETE’S FOOT: Clean feet well with soap and water, dry well. Apply Desenex spray or powder to the affected area morning and night, pay attention to space between toes. Instruct the student to wear well-ventilated shoes and change shoes and socks at least once per day. CANKER/COLD SORES: Salt Water rinses, use Blistex or a topical anesthetic (Orabase or Anbesol) to the area as needed. Instruct the student not to share drinking glasses or food utensils until lesions are gone. FOOD SUPPLEMENTS: Multivitamins as per request from parents or ordered by MD. MOTION SICKNESS: Dramamine as directed on the bottle. MINOR JOINT/BONE PAIN: If no injury or minor injury with no deformity or severe swelling, give pain med as instructed above, put ice on the area for 15-20 minutes. If not better, consult MD, or send to the hospital. These orders have been reviewed and approved by: Dr. Donald Eason, MD Please select one of the following: _____ I agree with the above-mentioned orders as written above and reviewed/approved by a physician for my child. I understand that generic forms of medications listed may be administered under the same instructions. _____No medications of any kind may be administered without my consent. _______________________________________ _______________________________________ K-Health is a Telehealth provider which offers 24/7 opportunity to medical care by a lisenced medical provider. The Vanguard School will be accessing this program for staff and students. The cost of this program is monthly or annual for all members of a family and can be accessed at https://www.khealth.com/ for more information. _______ I authorize the Vanguard School medical staff to administer the Influenza Immunization during the fall semester. I understand this is NOT a live virus, and will not be given to anyone who is allergic to eggs. _______ I do not authorize the Vanguard School medical staff to administer the Influenza Immunization during the fall semester. I understand this is NOT a live virus, and will not be given to anyone who is allergic to eggs. Student Name___________________________________________________________________
The Vanguard School
2022-23 Academic Year
MEDICAL AND HOSPITAL AUTHORIZATION
Student Name (Last, First)_________________________________________________
Date of Birth____________________________
Address_______________________________________________________________
I hereby authorize The Vanguard School to make necessary medical examinations. This may
include physical examinations, x-rays, laboratory studies, and obtain medical results, records
and any other pertinent medical information, including psychiatric evaluation, follow-up care,
and am giving consent for recommended prescriber medications and care, regarding the
student’s health and medical treatment. Daily assessment, and recommendation of testing, as
well as notification in the event of any positive testing, are also authorized.
I also authorize the School to institute preventive medical and dental measures that the School
or its physician may feel are indicated. I authorize the School to administer any medication the
School and/or its physician may feel indicated for the improvement of health and comfort.
In the event of an acute condition or illness, I request and authorize the School to seek
whatever medical care may be indicated. Hospitalization, surgical treatment, and anesthesia
may be authorized by any member of the School’s medical and administrative staff and any
necessary consent executed thereto.
I request and authorize (Student Name) __________________________________________ to
participate in all School activities including athletics, swimming, and special trips away from
School when the staff feels these are indicated for education or enjoyment.
______________________________________________________________________________ Parent or Guardian Signature
The foregoing instrument was acknowledged before me this _______ day of __________________, 20____,
By ______________________________ who is personally known to me,
or who produced ___________________________________ as identification.
______________________________________________________
Notary Public Signature Commission ExpiresSection 2: Financial The Vanguard School 2022-2023 Enrollment Kit
The Vanguard School
2022-23 Parent Financial Updates
Registration Payments
● Signed Contract (Payment Schedule determined in FACTS Financial Account)
● Tuition Insurance Indication and Payment (4% of Tailored Tuition amount)
● Student Account Payment (Boarding Students owe $2,000; Day Students owe $500)
● All Florida State Scholarship letters must be turned in before 8/1 to receive first
payment for the 2022-23 academic year.
Tuition Payments Payment in the 2022-23 academic year can be made through the secure
FACTS Financial Account for each family. Families will select their payment schedule, and will
have access to view the payment information and applied payments at any time by logging
into this account. Payments include any external scholarships including Florida School Choice
options. For questions, please contact Tamika Smith, tamika.smith@vanguardschool.org.
Allowance The Vanguard School strongly recommends that families research and utilize a
student debit card or pre-paid debit card for their student. These cards offer families the
opportunity to determine allowance, track spending, and real-life experience in money
management for students. Gift cards are available for use in the Student Center store only.
Credit Card Authorization Form Parents are encouraged to complete and submit a
credit/debit authorization form for the Business Office to have on file in the event of
incidentals.
Updated Tailored Tuition and Florida State Scholarship Policy
The Vanguard School’s Tailored Tuition opportunity is designed to assist families who qualify
through the generosity of school donors. Each year we are seeing a growing need for
increases to Tailored Tuition based on financial need. In order to keep this program available
for families, we are updating our year-end credit balance policy.
If, at the end of the school year, you have a credit balance and you received both Vanguard
Tailored Tuition and Florida Scholarships, no credit or refund will be issued or carried forward.
Your account will be brought to a zero balance and Vanguard will offset the credit against
the amount of Tailored Tuition received.
I understand the above stated items, and agree to these updates.
________________________________________ ______________________________________
Student Name ___________________________________________________________________________The Vanguard School
22000 Hwy 27
Lake Wales, FL 33859
(863) 676-6091
Credit/Debit Card Payment Authorization Form
Please complete and sign this form to authorize The Vanguard School to make debits to your credit/debit card
listed below.
By signing this form you give us permission to debit your account for the amounts approved by you over the
phone, through email, or as indicated below. This is permission to maintain your credit card information on file for
approved usage. There is an additional 3% charge on all credit/debit card payments.
________________________________________________________________________________
Please Complete the Information Below:
I, _____________________________, authorize The Vanguard School to charge my
credit/debit card in the amount of $____________, plus 3%, $ __________
Total Amount $_____________
On the ____ day of ___________, 20____.
This transaction is to pay for: __________________________________________
Student’s Name: ___________________________________________________
Card Billing Address: ________________________________________________
City, State, Zip: ____________________________________________________
Country: ____________________________ Phone: _______________________
Email: ____________________________________________________________
Card Type: ____Visa _____MasterCard ____Discover ____American Express
Cardholder’s Name: ________________________________________________
Account Number: __________________________________________________
Expiration Date: _______________________ CCV Code: ____________
Signature: ___________________________________________ Date: _____________
Staff’s Name: ______________________ Signature: ___________________________
I authorize the above named business to charge the credit/debit card indicated in this authorization form according
to the terms outlined above. I certify that I am an authorized user of this credit/debit card and that I will not dispute
the payment with my credit/debit card company; so long as the transaction corresponds to the terms indicated in
this form.Section 3: Program Requirements The Vanguard School 2022-2023 Enrollment Kit
The Vanguard School
2022-2023 Dress Code
We consider the academic portion of our program as being each student’s profession
and they should dress accordingly. To help reduce distractibility, provide consistency,
and build an community culture at The Vanguard School, students are expected to
follow the school dress code as outlined below. Students found not meeting the dress
code will be addressed on an individual basis and required to change into appropriate
clothing. All pants/shorts must be worn above the hip bone, and any violation of this
policy will result in the student being required to wear a belt at all times.
Students have the option to have one or more masks with them. They may be in a
situation on or off-campus that requests their use of a mask. We will follow the
state/local Health Department or legal requirements of health and safety measures.
Masks or clothing with inappropriate images, words, or implications will not be allowed
on-campus, or during any school-related activity. Parents will be notified if an issue
arises. No torn, ripped or cut clothing will be allowed to meet dress code expectations.
Dress Code/School Uniform
Pants
● Cotton or twill, and denim is acceptable in solid color grey, navy, black, or khaki
(no other colors are allowed)
● Joggers are NOT allowed during the academic day
Shorts/Skorts (please note skirts are not allowed)
● Shorts/Skorts must be in solid color grey, navy, black or khaki, or regular fit denim
● Shorts/Skorts hemlines must be fingertip length
● Violations may result in the student wearing pants
Shirts
● Must be the official Vanguard polo shirt (must be purchased through
Vanguard) Monday through Thursday in academic settings
● Other official Vanguard shirts may be worn on Fridays only
Jackets/Hoodies/Sweatshirts
● Must be official Vanguard merchandise for academic day use
Shoes
● Closed toe and heel are preferred to prevent injuries
● No flip flops slides, nor slippers may be worn
Belts
● Are not required unless the student violates the above policy regarding proper
wearing of pants/shorts
Hair
● Must be clean, neat, and demonstrate appropriate hygieneOptional Apparel
● Appropriate hats and sunglasses may only be worn outside of school hours, on
fieldtrips, or during outdoor activities.
● Non-Vanguard jackets with hoods or hats may only be worn outside of school hours,
on evening and weekend fieldtrips, or during outside activities in cold weather.
● No hoods, hats, or sunglasses may be worn inside of the classroom buildings with the
exception of official Vanguard beanies or hats.
● Pajama bottoms may not be worn outside of the dorm.
● Rain boots may be worn on rainy days.
● Any clothing depicting gang activity, drugs, alcohol or other objectionable or illegal
material is not to be worn.
Special Activities
● Professional Dress is required for all special activities such as formal lunches and
dinners, award programs, graduation, dances and other special events.
● Formal Meal dress expectations include dress shirt, jacket, dress pants, dress shoes,
dress socks, skirt, or dress as applicable and appropriate.
Cultural Dress
● Students who come from other cultures may wear appropriate cultural
clothing.
Dorm Dress
● In the dorms, resident students may wear clothes of their choosing, provided they are
appropriate and are not obscene or objectionable to staff and other students.
● Please select one of the following:
_______ I give permission for my child to bike, skate, or rollerblade without the use of a
helmet.
_______ I do not give permission for my child to bike, skate, or rollerblade without the
use of a helmet.
Dress Code Consequences
● Dress Code Violations: Change to appropriate clothing and discussion of
self-advocacy and planning strategies. Parents may be contacted.
● Repetitive Offenders: Change to appropriate clothing, and a Parent Conference will
be held. Disciplinary action may include, but is not limited to, purchasing of additional
uniform items, additional community service chores, and/or loss of weekend privileges,
etc.
The undersigned student and parent(s) acknowledge receipt of the
above-mentioned policies and understand and agree to the terms thereof.
Student Name (please print)_____________________________________________
Student Signature __________________________________________________
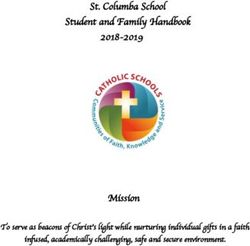
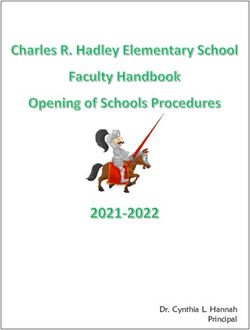
Parent Signature ___________________________________________________2022-23 Uniform Bundles
Bundles 1 - 4* Include the Dress Code Essentials for Students!
Refresh the Essentials with Bundles 1-4*, or add new
Rec and Weekend pieces with Bundles 5-7*.
White Polos are going out-of-stock at $10 while supplies last!
*You can substitute a zipper hoodie for $5 in Bundles 1,2, 5, or 7.
4 Poly-Cotton Polos Pullover Hoodie*
Bundle #1 Bundle #5
Pullover Hoodie* Tshirt
$150.00 Tshirt $55.00 Athletic Shorts
4 Dri-Fit Polos Jacket
Bundle #2 Bundle #6
Pullover Hoodie* Tshirt
$150.00 Tshirt $55.00 Beanie
4 Poly-Cotton Polos
Bundle #3 Bundle #7 Hoodie
Tshirt Tshirt
$110.00 $75.00 Athletic Shorts
4 Dri-Fit Polos
Bundle #4
Tshirt White Polos $10
$110.00
while supplies last
*Zipper Hoodie can be substituted for any Pullover Hoodie at $5 additional cost.2022-23 Uniform Order
Please select your preferred Bundle(s), and
complete the size and color selections.
Student Name:_________________________________Date: / /
Payment Choice: ___ Card ___Check ___ Student Account
Payment Total:_________________ (Please add $5.00 for Zipper Hoodies)
___ White Polos Unisex___ Ladies___ Size:____ Number Requested____
$10.00 While supplies last - Limited availability
___ Bundle #1 $140.00
4 Polos Unisex___ Ladies___ Size:_____ Navy____ Grey____
Hoodie Reg.____ Zipper____ Size:_____ Navy____ Grey___
Tshirt Unisex___ Ladies___ Size:_____ Navy____ Grey____
___ Bundle #2 $140.00
4 Polos Unisex___ Ladies___ Size:_____ Navy____ Grey____
Hoodie Reg.____ Zipper____ Size:_____ Navy____ Grey___
Tshirt Unisex___ Ladies___ Size:_____ Navy____ Grey____
___ Bundle #3 $110.00
4 Polos Unisex___ Ladies___ Size:_____ Navy____ Grey____
Tshirt Unisex___ Ladies___ Size:_____ Navy____ Grey____
___ Bundle #4 $110.00
4 Polos Unisex___ Ladies___ Size:_____ Navy____ Grey____
Tshirt Unisex___ Ladies___ Size:_____ Navy____ Grey____
___ Bundle #5 $55.00
Hoodie Reg.____ Zipper____ Size:_____ Navy____ Grey___
Tshirt Unisex___ Ladies___ Size:_____ Navy____ Grey___
Shorts Unisex___ Ladies___ Size:_____. Navy Only
___ Bundle #6 $55.00
Jacket Size:_____ Navy Only
Tshirt Unisex___ Ladies___ Size:_____ Navy____ Grey___
Beanie Navy Only
___ Bundle #7 $75.00
Hoodie Size:_____ Grey Only
Tshirt Unisex___ Ladies___ Size:_____ Navy____ Grey___
Shorts Unisex___ Ladies___ Size:_____ Navy OnlyThe Vanguard School
Drugs, Alcohol, Tobacco, and Medication Policy
Sale, Distribution, or Possession with Intent to Sell or Distribute
The Vanguard School is a drug-free, tobacco-free, and smoke-free campus. A student
who sells or distributes attempts or conspires with someone else to sell or distribute, or
possesses with intent to sell or distribute an intoxicating or controlled beverage,
narcotic, any mood modifying prescription, over-the-counter, or other drug is guilty of a
very serious breach of conduct. Parents are obligated to pay for all services stated in
their contract. Discipline and an investigation will be handles on an individualized basis.
All Vanguard students are subject to random drug testing and searches without
provocation. Campus and residential searches can and will be executed via residential
and/or administrative staff following respectful handling of student and staff person and
property. In the event of a positive test or search result, students and staff are subject to
disciplinary action.
The Vanguard staff may search a student’s room, car, and person when use or
distribution is suspected.
Upon determination of inappropriate use or possession of inappropriate materials
students are subject to suspension and/or being sent home or expulsion, at the parent’s
expense. Additional screenings will be completed to monitor continued to desist of use.
While at home, students are responsible for assigned academic task completion. Upon
return to Vanguard, the student will be tested randomly at the parent’s expense, and
may need to complete a drug abuse program. Parents are obligated to pay for all
services stated in their contract and counseling, and may incur the loss of in-house
Tailored Tuition.Tobacco/Smoking/Vaping It is the goal of the Vanguard School to be “tobacco-free”; staff, students, and parents are to refrain from using, distributing, purchasing, and sharing any form of tobacco (including chewing tobacco and electronic cigarettes) while on campus. Students who are in possession of, purchase, and/or use tobacco products (including electronic cigarettes) will be subject to the following consequences: Parent notification, suspension, or expulsion at parent’s expense and/ or sent home, reduction in privileges, or increased community service chores. The student’s overall behavior will be considered in this determination. In the event of suspected purchase or distribution to minors, students may be expelled from the program. Over-the-Counter Medication Students should not have over-the-counter medication in their dorm rooms, or on their person unless approved by the Administration or School Medical Team. (Examples include Tylenol, cold or allergy medicines, anabolic steroids, vitamins, supplements, etc.) Prescription Medication: All prescription medications must be kept and dispensed by the Medical Team. All prescriptions are recommended to be filled through a “pill pack” method and will be dispensed to the student by the School as directed by the prescribing physician. Any changes to medication orders and directions must be received by the pharmacy and the School in writing from the prescribing physician’s office. No changes to medications or to their dosage and instructions will be made unless written orders have been received by the prescribing physician. The undersigned student and parent(s) acknowledge receipt of the above-mentioned policies and understand and agree to the terms thereof. Student’s Name: _________________________________________________________ Student’s Signature: _______________________________________________________ Parent/Guardian Signature: _______________________________________________
The Vanguard School
2022-23 Student Counseling and Support Services
Student’s Name:______________________________ Birthdate:_______________
Parent/Guardian(s) Name(s):___________________________________________
Address:_______________________________________________________________
The services that are checked below will assist us in planning appropriate educational
services or support for your child. Please indicate any and all services that you would like
your child to participate in.
Please indicate all that apply.
_______ I want you to recommend a local counselor for my child ot receive individual
counseling
_______ I wish for my child to continue individual counseling with the following:
Name:______________________________________Phone:__________________________
_____ Focus Group sessions: (i.e. Anxiety/Depression, Family Dynamics, Health &
Nutrition, Healthy Relationships)
_____ Other Services:(Please indicate)_________________________________________________
Please INITIAL the space in front of ONE of the following:
_____ I do give permission for my child to receive the services or interventions requested
above.,
_____ I do not wish my child to receive the services or interventions mentioned above at
this time, but please contact me with any concerns or recommendations.
Parent/GuardianSignature:_____________________________________
Exceptions to Confidentiality include: Suicidal ideation/intent/plan, Child abuse/neglect/sexual abuseThe Vanguard School
Student Counseling and Support Services
The Vanguard School is committed to providing quality care to our students. We
provide every effort to ensure every student is treated with dignity, privacy, and
respect. In an effort to achieve this goal, parents/guardians or school staff may
refer students to counseling, or students may request counseling. The focus of
the counseling program is to help students better understand the world they live
in and themselves, develop coping skills, and make better choices on and
off-campus. There are several methods that a student can receive counseling
services as a Vanguard student. For brief solution-focused and crisis
management situations on campus, the school’s counselor is on call to provide
care for our students. School counseling services are aimed at providing
education and socialization to the student within the school community. These
services are not intended as a substitute for psychological counseling, diagnosis,
or medication.
Benefits and Risks
There are numerous benefits of counseling, which can include emotional
growth, gained insight, increased coping skills, communication skills, and peer
relationship skills can be improved.
Limited risks are also associated with counseling participation. Students may
experience feelings of an unpleasant aspect of their life such as sadness, guilt,
anger, frustration, loneliness, or helplessness.
The student and counselor sessions are confidential. There are exceptions to
confidentiality that relate to the health and safety of the student.
Exceptions include:
● Suicidal ideation/intent/plan: Harm to self or others
● Child abuse/neglect/sexual abuse
● Elderly/disabled persons being abused or neglected
● Any other reporting required by State or Federal LawThe counselor working with the student will help the student share with his/her/their parents or guardians if something arises in therapy that should be shared that is in the best interest of the student. Overview of Support Services Counseling at The Vanguard School is designed to assist our students in their educational experiences. As a school, we are concerned about each student’s emotional well-being, academic progress, personal, and social development. This information is intended to provide you information about counseling integration, counseling relationships, and counseling services. Feel free to contact Ana Pizarro (ana.pizarro@vanguardschool.org) with any questions you have regarding this matter. Role of the School Counselor The School Counselor, in cooperation with nursing, faculty, staff, and administration at The Vanguard School, is responsible for providing a comprehensive school counseling program for students enrolled in grades 6th through 12th. We work with our local community to provide services for our students on and off-campus. On-campus, we provide services to educate and support students with mental health care needs. Responsive Services Involve both direct and indirect services to students. The methods of services include individual and/or group counseling, consultation, referrals, crisis response, and peer facilitation. Group Counseling or Focus Groups Direct and short-term service to respond proactively or reactively to student needs. This format offers experiences based on relevant and developmentally appropriate topics and skills such as study skills, social skills, grief, and other topics. Consultation An indirect service involving collaboration with parents, administrators, faculty, staff, and other counseling professionals to address student issues or concerns. The goal is to inform curriculum planning, address academic or behavioral interventions, provide training for faculty and staff, contribute to policy planning, and support mental health coordination. Referrals The School Counselor may enlist the services of other mental health professionals to assist students in handling complex issues with the knowledge of parents/guardians. Students may be referred to on-campus psychologists or therapists, psychiatrists, or other professionals. Information is considered confidential that is shared between mental health professionals.
Individual counseling These sessions involve offering direct service to students to address both proactive and reactive needs for an unspecified period of time. This service is provided only by an off-campus psychologist or therapist at the parents’/guardians’ expense. Some providers may be able to arrange these sessions on-campus in-person or through tele-mental health, and coordinated through the School Counselor. Crisis Response This involves immediate and critical intervention in an acute situation. The goal is an intervention to diffuse a situation, serve the school and community members affected by the situation, and promote a healing process. Peer Facilitation A mechanism to cultivate leadership skills in students. This direct peer-to-peer opportunity focuses on interpersonal skills in leadership to empower group members to integrate the core values of Vanguard.
Section 4: Athletics The Vanguard School 2022-2023 Enrollment Kit
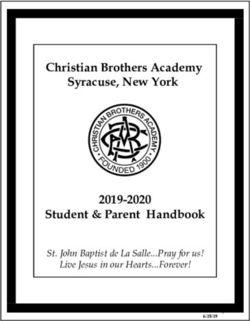
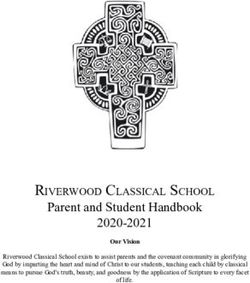
EL2
Florida High School Athletic Association Revised 03/16
Preparticipation Physical Evaluation (Page 1 of 3)
This completed form must be kept on file by the school. This form is valid for 365 calendar days from the date of the evaluation as written on page 2.
This form is non-transferable; a change of schools during the validity period of this form will require page 1 of this form to be re-submitted.
Part 1. Student Information (to be completed by student or parent)
Student’s Name: ________________________________________________________________________ Sex: _____ Age: _____ Date of Birth: _____/ _____/ _____
School: ____________________________________________________ Grade in School: _____ Sport(s): ________________________________________________
Home Address: _______________________________________________________________________________________ Home Phone: ( _____) _______________
Name of Parent/Guardian: _______________________________________________________________ E-mail: ___________________________________________
Person to Contact in Case of Emergency: _____________________________________________________________________________________________________
Relationship to Student: _______________________ Home Phone: ( _____) ______________ Work Phone: ( _____) _____________ Cell Phone: ( _____) _____________
Personal/Family Physician: ___________________________________________City/State: ___________________________ Office Phone: ( _____) _____________
Part 2. Medical History (to be completed by student or parent). Explain “yes” answers below. Circle questions you don’t know answers to.
Yes No Yes No
1.
Have you had a medical illness or injury since your last ____ ____ 26. Have you ever become ill from exercising in the heat? ____ ____
check up or sports physical? 27. Do you cough, wheeze or have trouble breathing during or after ____ ____
2. Do you have an ongoing chronic illness? ____ ____ activity?
3. Have you ever been hospitalized overnight? ____ ____ 28. Do you have asthma? ____ ____
4. Have you ever had surgery? ____ ____ 29. Do you have seasonal allergies that require medical treatment? ____ ____
5. Are you currently taking any prescription or non- ____ ____ 30. Do you use any special protective or corrective equipment or ____ ____
prescription (over-the-counter) medications or pills or medical devices that aren’t usually used for your sport or position
using an inhaler? (for example, knee brace, special neck roll, foot orthotics, shunt,
6. Have you ever taken any supplements or vitamins to ____ ____ retainer on your teeth or hearing aid)?
help you gain or lose weight or improve your 31. Have you had any problems with your eyes or vision? ____ ____
performance? 32. Do you wear glasses, contacts or protective eyewear? ____ ____
7. Do you have any allergies (for example, pollen, latex, ____ ____ 33. Have you ever had a sprain, strain or swelling after injury? ____ ____
medicine, food or stinging insects)? 34. Have you broken or fractured any bones or dislocated any joints? ____ ____
8. Have you ever had a rash or hives develop during or ____ ____ 35. Have you had any other problems with pain or swelling in muscles, ____ ____
after exercise? tendons, bones or joints?
9. Have you ever passed out during or after exercise? ____ ____ If yes, check appropriate blank and explain below:
10. Have you ever been dizzy during or after exercise? ____ ____ ___ Head ___ Elbow ___ Hip
11. Have you ever had chest pain during or after exercise? ____ ____ ___ Neck ___ Forearm ___ Thigh
12. Do you get tired more quickly than your friends do ____ ____ ___ Back ___ Wrist ___ Knee
during exercise? ___ Chest ___ Hand ___ Shin/Calf
13. Have you ever had racing of your heart or skipped ____ ____ ___ Shoulder ___ Finger ___ Ankle
heartbeats? ___ Upper Arm ___ Foot
14. Have you had high blood pressure or high cholesterol? ____ ____ 36. Do you want to weigh more or less than you do now? ____ ____
15. Have you ever been told you have a heart murmur? ____ ____ 37. Do you lose weight regularly to meet weight requirements for your ____ ____
16. Has any family member or relative died of heart ____ ____ sport?
problems or sudden death before age 50? 38. Do you feel stressed out? ____ ____
17. Have you had a severe viral infection (for example, ____ ____ 39. Have you ever been diagnosed with sickle cell anemia? ____ ____
myocarditis or mononucleosis) within the last month?
40. Have you ever been diagnosed with having the sickle cell trait? ____ ____
18. Has a physician ever denied or restricted your ____ ____
41. Record the dates of your most recent immunizations (shots) for:
participation in sports for any heart problems?
Tetanus: _______________ Measles: _______________
19. Do you have any current skin problems (for example, ____ ____
Hepatitus B: ____________ Chickenpox: ____________
itching, rashes, acne, warts, fungus, blisters or pressure sores)?
20. Have you ever had a head injury or concussion? ____ ____
FEMALES ONLY (optional)
21. Have you ever been knocked out, become unconscious ____ ____
or lost your memory? 42. When was your first menstrual period?________________________
22. Have you ever had a seizure? ____ ____ 43. When was your most recent menstrual period?__________________
23. Do you have frequent or severe headaches? ____ ____ 44. How much time do you usually have from the start of one period to
the start of another?________________________________________
24. Have you ever had numbness or tingling in your arms, ____ ____
hands, legs or feet? 45. How many periods have you had in the last year?________________
25. Have you ever had a stinger, burner or pinched nerve? ____ ____ 46. What was the longest time between periods in the last year?_________
Explain “Yes” answers here:________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________________________
We hereby state, to the best of our knowledge, that our answers to the above questions are complete and correct. In addition to the routine medical evaluation required by s.1006.20, Florida
Statutes, and FHSAA Bylaw 9.7, we understand and acknowledge that we are hereby advised that the student should undergo a cardiovascular assessment, which may include such diagnostic
tests as electrocardiogram (EKG), echocardiogram (ECG) and/or cardio stress test.
Signature of Student: _____________________________________ Date: ____/ ____/ ____ Signature of Parent/Guardian: __________________________________ Date: ____/ ____/ ____
–1–EL2
Florida High School Athletic Association Revised 03/16
Preparticipation Physical Evaluation (Page 2 of 3)
This completed form must be kept on file by the school. This form is valid for 365 calendar days from the date of the evaluation as written on page 2.
This form is non-transferable; a change of schools during the validity period of this form will require page 1 of this form to be re-submitted.
Part 3. Physical Examination (to be completed by licensed physician, licensed osteopathic physician, licensed chiropractic physi-
cian, licensed physician assistant or certified advanced registered nurse practitioner).
Student’s Name: _____________________________________________________________________________________________ Date of Birth: _____/_____/_____
Height: _____________ Weight: _____________ % Body Fat (optional): ____________ Pulse: _________ Blood Pressure: ____ / ____ ( ____/____ , ____ /____ )
Temperature: _____________ Hearing: right: P ______ F _____ left: P _____ F _____
Visual Acuity: Right 20/_______ Left 20/_______ Corrected: Yes No Pupils: Equal _________ Unequal _________
FINDINGS NORMAL ABNORMAL FINDINGS INITIALS*
MEDICAL
1. Appearance ________ ________________________________________________________________________ ____________
2. Eyes/Ears/Nose/Throat ________ ________________________________________________________________________ ____________
3. Lymph Nodes ________ ________________________________________________________________________ ____________
4. Heart ________ ________________________________________________________________________ ____________
5. Pulses ________ ________________________________________________________________________ ____________
6. Lungs ________ ________________________________________________________________________ ____________
7. Abdomen ________ ________________________________________________________________________ ____________
8. Genitalia (males only) ________ ________________________________________________________________________ ____________
9. Skin ________ ________________________________________________________________________ ____________
MUSCULOSKELETAL
10. Neck ________ ________________________________________________________________________ ____________
11. Back ________ ________________________________________________________________________ ____________
12. Shoulder/Arm ________ ________________________________________________________________________ ____________
13. Elbow/Forearm ________ ________________________________________________________________________ ____________
14. Wrist/Hand ________ ________________________________________________________________________ ____________
15. Hip/Thigh ________ ________________________________________________________________________ ____________
16. Knee ________ ________________________________________________________________________ ____________
17. Leg/Ankle ________ ________________________________________________________________________ ____________
18. Foot ________ ________________________________________________________________________ ____________
* – station-based examination only
ASSESSMENT OF EXAMINING PHYSICIAN/PHYSICIAN ASSISTANT/NURSE PRACTITIONER
I hereby certify that each examination listed above was performed by myself or an individual under my direct supervision with the following conclusion(s):
____ Cleared without limitation
____ Disability: _____________________________________________________ Diagnosis:____________________________________________________________
_______________________________________________________________________________________________________________________________________
____ Precautions: _________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________________
____ Not cleared for: __________________________________________________________________________ Reason: ____________________________________
_______________________________________________________________________________________________________________________________________
____ Cleared after completing evaluation/rehabilitation for: _______________________________________________________________________________________
____ Referred to ______________________________________________________________________________ For: _______________________________________
_______________________________________________________________________________________________________________________________________
Recommendations: ________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________________
Name of Physician/Physician Assistant/Nurse Practitioner (print): __________________________________________________________ Date: _____/_____/_______
Address: ________________________________________________________________________________________________________________________________
Signature of Physician/Physician Assistant/Nurse Practitioner: ____________________________________________________________________________________
–2–EL2
Florida High School Athletic Association Revised 03/16
Preparticipation Physical Evaluation (Page 3 of 3)
This completed form must be kept on file by the school. This form is valid for 365 calendar days from the date of the evaluation as written on page 2.
This form is non-transferable; a change of schools during the validity period of this form will require page 1 of this form to be re-submitted.
Student’s Name: _____________________________________________________________________________________________
ASSESSMENT OF PHYSICIAN TO WHOM REFERRED (if applicable)
I hereby certify that the examination(s) for which referred was/were performed by myself or an individual under my direct supervision with the following conclusion(s):
____ Cleared without limitation
____ Disability: _____________________________________________________ Diagnosis: ___________________________________________________________
_______________________________________________________________________________________________________________________________________
____ Precautions: _________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________________
____ Not cleared for: __________________________________________________________________________ Reason: ____________________________________
____ Cleared after completing evaluation/rehabilitation for: _______________________________________________________________________________________
Recommendations: ________________________________________________________________________________________________________________________
Name of Physician (print): ___________________________________________________________________________________________ Date: ____/____/_______
Address: ________________________________________________________________________________________________________________________________
Signature of Physician: ___________________________________________________________________________________________________________________
Based on recommendations developed by the American Academy of Family Physicians, American Academy of Pediatrics, American Medical Society for Sports Medicine, American Orthopae-
dic Society for Sports Medicine and American Osteopathic Academy for Sports Medicine.
–3–EL3
Florida High School Athletic Association Revised 06/21
Consent and Release from Liability Certificate (Page 1 of 4)
This completed form must be kept on file by the school. This form is valid for 365 calendar days from the date of the most recent signature.
This form is non-transferable; a change of schools during the validity period of this form will require this form to be re-submitted.
School: __________________________________________ School District (if applicable): __________________________
Part 1. Student Acknowledgement and Release (to be signed by student at the bottom)
I have read the (condensed) FHSAA Eligibility Rules printed on Page 4 of this “Consent and Release Certificate” and know of no reason why I am not eligible to represent
my school in interscholastic athletic competition. If accepted as a representative, I agree to follow the rules of my school and FHSAA and to abide by their decisions. I
know that athletic participation is a privilege. I know of the risks involved in athletic participation, understand that serious injury, including the potential for a concus-
sion, and even death, is possible in such participation, and choose to accept such risks. I voluntarily accept any and all responsibility for my own safety and welfare while
participating in athletics, with full understanding of the risks involved. Should I be 18 years of age or older, or should I be emancipated from my parent(s)/guardian(s), I
hereby release and hold harmless my school, the schools against which it competes, the school district, the contest officials and FHSAA of any and all responsibility and
liability for any injury or claim resulting from such athletic participation and agree to take no legal action against FHSAA because of any accident or mishap involving my
athletic participation. I hereby authorize the use or disclosure of my individually identifiable health information should treatment for illness or injury become necessary.
I hereby grant to FHSAA the right to review all records relevant to my athletic eligibility including, but not limited to, my records relating to enrollment and attendance,
academic standing, age, discipline, finances, residence and physical fitness. I hereby grant the released parties the right to photograph and/or videotape me and further to
use my name, face, likeness, voice and appearance in connection with exhibitions, publicity, advertising, promotional and commercial materials without reservation or
limitation. The released parties, however, are under no obligation to exercise said rights herein. I understand that the authorizations and rights granted herein are voluntary
and that I may revoke any or all of them at any time by submitting said revocation in writing to my school. By doing so, however, I understand that I will no longer be
eligible for participation in interscholastic athletics.
Part 2. Parental/Guardian Consent, Acknowledgement and Release (to be completed and signed by a parent(s)/guardian(s) at the bot-
tom; where divorced or separated, parent/guardian with legal custody must sign.)
A. I hereby give consent for my child/ward to participate in any FHSAA recognized or sanctioned sport EXCEPT for the following sport(s):
__________________________________________________________________________________________________________________________________
List sport(s) exceptions here
B. I understand that participation may necessitate an early dismissal from classes.
C. I know of, and acknowledge that my child/ward knows of, the risks involved in interscholastic athletic participation, understand that serious injury, and even death,
is possible in such participation and choose to accept any and all responsibility for his/her safety and welfare while participating in athletics. With full understanding of
the risks involved, I release and hold harmless my child’s/ward’s school, the schools against which it competes, the school district, the contest officials and FHSAA of
any and all responsibility and liability for any injury or claim resulting from such athletic participation and agree to take no legal action against the FHSAA because of
any accident or mishap involving the athletic participation of my child/ward. As required by F.S. 1014.06(1), I specifically authorize healthcare services to be provided for
my child/ward by a healthcare practitioner, as defined in F.S. 456.001, or someone under the direct supervision of a healthcare practitioner, should the need arise for such
treatment, while my child/ward is under the supervision of the school. I further hereby authorize the use or disclosure of my child’s/ward’s individually identifiable health
information should treatment for illness or injury become necessary. I consent to the disclosure to the FHSAA, upon its request, of all records relevant to my child/ward’s
athletic eligibility including, but not limited to, records relating to enrollment and attendance, academic standing, age, discipline, finances, residence and physical fitness.
I grant the released parties the right to photograph and/or videotape my child/ward and further to use said child’s/ward’s name, face, likeness, voice and appearance in
connection with exhibitions, publicity, advertising, promotional and commercial materials without reservation or limitation. The released parties, however, are under no
obligation to exercise said rights herein.
D. I am aware of the potential danger of concussions and/or head and neck injuries in interscholastic athletics. I also have knowledge about the risk of continuing to
participate once such an injury is sustained without proper medical clearance.
READ THIS FORM COMPLETELY AND CAREFULLY. YOU ARE AGREEING TO LET YOUR MINOR CHILD ENGAGE
IN A POTENTIALLY DANGEROUS ACTIVITY. YOU ARE AGREEING THAT, EVEN IF MY CHILD’S/WARD’S SCHOOL,
THE SCHOOLS AGAINST WHICH IT COMPETES, THE SCHOOL DISTRICT, THE CONTEST OFFICIALS AND FHSAA
USES REASONABLE CARE IN PROVIDING THIS ACTIVITY, THERE IS A CHANCE YOUR CHILD MAY BE SERI-
OUSLY INJURED OR KILLED BY PARTICIPATING IN THIS ACTIVITY BECAUSE THERE ARE CERTAIN DANGERS
INHERENT IN THE ACTIVITY WHICH CANNOT BE AVOIDED OR ELIMINATED. BY SIGNING THIS FORM YOU ARE
GIVING UP YOUR CHILD’S RIGHT AND YOUR RIGHT TO RECOVER FROM MY CHILD’S/WARD’S SCHOOL, THE
SCHOOLS AGAINST WHICH IT COMPETES, THE SCHOOL DISTRICT, THE CONTEST OFFICIALS AND FHSAA IN
A LAWSUIT FOR ANY PERSONAL INJURY, INCLUDING DEATH, TO YOUR CHILD OR ANY PROPERTY DAMAGE
THAT RESULTS FROM THE RISKS THAT ARE A NATURAL PART OF THE ACTIVITY. YOU HAVE THE RIGHT TO RE-
FUSE TO SIGN THIS FORM, AND MY CHILD’S/WARD’S SCHOOL, THE SCHOOLS AGAINST WHICH IT COMPETES,
THE SCHOOL DISTRICT, THE CONTEST OFFICIALS AND FHSAA HAS THE RIGHT TO REFUSE TO LET YOUR
CHILD PARTICIPATE IF YOU DO NOT SIGN THIS FORM.
E. I agree that in the event we/I pursue litigation seeking injunctive relief or other legal action impacting my child (individually) or my child’s team participa-
tion in FHSAA state series contests, such action shall be filed in the Alachua County, Florida, Circuit Court.
F. I understand that the authorizations and rights granted herein are voluntary and that I may revoke any or all of them at any time by submitting said revocation in
writing to my school. By doing so, however, I understand that my child/ward will no longer be eligible for participation in interscholastic athletics.
G. Please check the appropriate box(es):
____ My child/ward is covered under our family health insurance plan, which has limits of not less than $25,000.
Company: ____________________________________________________________ Policy Number: ________________________________
____ My child/ward is covered by his/her school’s activities medical base insurance plan.
____ I have purchased supplemental football insurance through my child’s/ward’s school.
I HAVE READ THIS CAREFULLY AND KNOW IT CONTAINS A RELEASE (Only one parent/guardian signature is required)
__________________________________________________ ____________________________________________________ _______/_______/____________
Name of Parent/Guardian (printed) Signature of Parent/Guardian Date
__________________________________________________ ____________________________________________________ _______/_______/____________
Name of Parent/Guardian (printed) Signature of Parent/Guardian Date
I HAVE READ THIS CAREFULLY AND KNOW IT CONTAINS A RELEASE (student must sign)
__________________________________________________ ____________________________________________________ _______/_______/____________
Name of Student (printed) Signature of Student Date
–1–You can also read