EXECUTIVE DASHBOARD FOR HH EXECUTIVES 2018 AND FORWARD - BARBARA A MCCANN PRESIDENT AND CEO
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Executive Dashboard for HH Executives 2018 and Forward Barbara A McCann President and CEO

Home Health’s Challenges Going Forward
• The ‘bottom’: most physicians still do not know what home health does,
what is covered and for how long. The ‘failure’ of CMS’ F2F
- The most informed physicians are in ACOs or taking risk under an MA
• Too many HHAs limit their interpretation of what HH can do to a narrow
interpretation of the benefit. (e.g. plan of care, discipline and frequency,
hesitancy to use technology (telemonitoring) as not specifically paid for)
• Home health is consistently seen as fraudulent among federal agencies, on
the Hill. (Where are our compliance plans?)
• Home health promoted as needing management, by third parties
facilitating ‘middlemen’ – are they partners in quality?
chapinc.org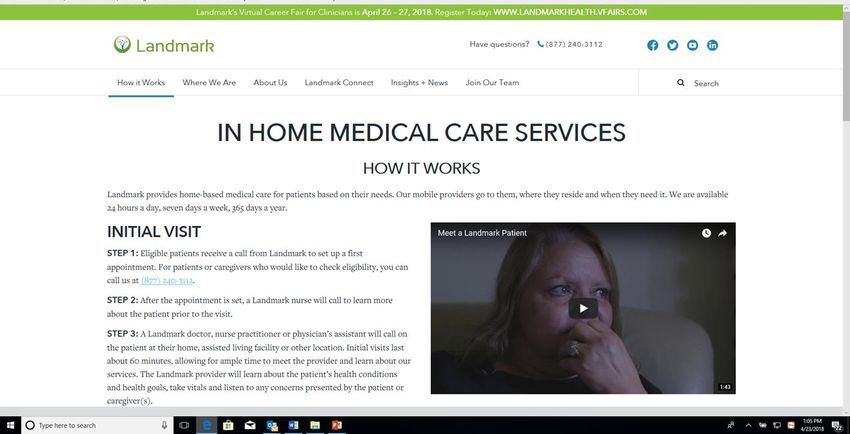
The HH Executive’s Balancing Act
CARE COMPLIANCE
COMPLIANCE
Value-based Manage
OUTCOMES
EFFICIENCY
CoPS Enough Utilization
STAFF
Billing Predictable
Regulations 2018 and
Consistent Identify
Competent Waste
Practice
Avoid
Improve and Adverse
Sustain Events
chapinc.org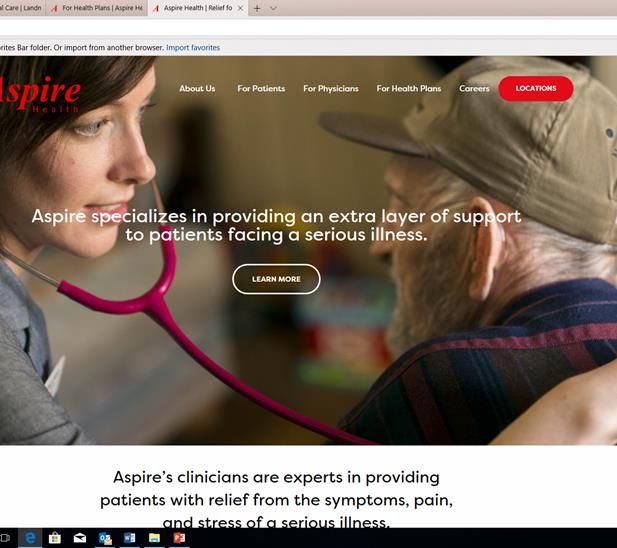
Compliance: Billing Regulation
• Do the right staff understand there are billing regulations and there are conditions of
participation, not the same ?
• Can you regularly see into the “whammies”, billing and now CoP implications:
- Unsigned plan of care or other orders – billing and CoPs (practice);
- Missed visits – billing, plan of care, now poor care coordination and patient at
risk:
- Number of patients without a visit in the past two weeks or more and not a
catheter patient and not discharged or transferred; and
- QAPI requirement – findings of fraud and waste are appropriately addressed……
• Federal billing oversight has no end in sight:
- Too many instances of fraud
- OIG cannot ‘see’ what HH or hospice does – ‘the black box’ has not gone away
chapinc.org
2018 HH CoPs – Survey Results & Insight
• Significantly expanded patient and family rights – many holes for
compliance citations:
- Policy done, new form available, sections left blank - financial
- Evidence that the patient and family received verbal explanation
- Selected representative, legal representative is identified and
information gets to them with evidence in 4 business days
- Transfer and Discharge policies, especially discharge for cause and
what is given to patient and family/representative
- Disciplines and frequency left in the home – and current
- Medication list in home is current and complete
Shhh! This could be a QAPI study!!
chapinc.org
2018 CoPs: Wholistic Patient Care
• Issues begin at the Plan of Care:
- Assessments that required a wholistic view of the patient – interdisciplinary team
- If PT or MSW eval done later, patient goals and outcomes needs to be consistent with
the plan of care (i.e. inability to reach goals or outcomes is a reason for discharge for
cause, meeting goal and outcomes means discharge)
- Software problems in allowing the clinicians to create individualized POCs
• What insight do you have into interdisciplinary practice and progress toward outcomes?
- Continue chart review, start now and read the first 2 weeks of notes – is there
evidence of team communication and progress toward outcomes and goals?
Shhh! This could be a another QAPI study!!
• How good are your Clinical Managers or the equivalent in responsibilities?
- The clinical manager role takes the ‘fall’ in the CoPs
chapinc.org
The Hidden ‘Gift’ in the CoPs
• The accountable role of the Clinical Manager should drive frequency, duration
and discipline to predictable outcomes and likely cost
- Similar to what the third party managers offer payers
• Effective clinical managers require introduction and use of:
- Data driven oversight – how well you move from referral to SOC,
interdisciplinary team involvement, and when is care done?
- Clinical practice or protocols that reduce risk for hospital admission and ER
used appropriately to risk level identified at admission
- Assessment of clinical competence, to support that you admit and meet the
needs of all patients referred without being at significant risk
o Common finding of complications associated with wound care
• What are the advantages of being a specialty agency vs. generalist HH in your
market? Have you thought through this strategically?
chapinc.org
Is Your Agency Big on Data?
It’s Time!!
Data Drives Accountability
• The multiple roles of accurate and timely documentation support:
- medical necessity and demonstration of need for billing
- assessment of effectiveness of intervention to better manage patient risk
- evidence of outcome achievement and sustainability
- Identification of variance in outcomes and cost of care by patient population,
and
- Demonstrated competence of staff
• What pieces of data do you need to do any one or all of the above? Do you have it
now? If so, do you have it when you need it?
• What do you have to showcase your agency?
- Can you tell me who you serve, their age, their most common diagnoses,
utilization of disciplines over what time period that appears to result in improve
or sustained outcomes? How well do you manage ER and hospitalization risk?
chapinc.org
A New, Important Acronym: HCC
• HCC: Hierarchical Condition Category risk score
• HCC is based on the patient health status and their
demographic characteristics.
• Used with MA plans to set reimbursement PMPM
• Hierarchies are used to characterize a patient’s illness level
within each disease process, while the effect of unrelated
disease processes increase predicted costs of care.
• Models for disease interaction
chapinc.orgWhat is Your Value Case Compared to Others: CMS ME Data
https://data.cms.gov/Medicare-Home-Health-Agency-HHA-/Medicare-Home-Health-Agency-HHA-Provider-Aggregate/5vaz-czzq/data CY 2015 Updated April 4, 2018 Maine
# Avg # Visits Avg # Nursing Avg # PT Avg Avg % % % % % Chronic
Episodes / Episode Visits/Episode Visits/Episode Age HCC CHF ALZ COPD Diabetes Kidney
Disease
257 14 4.7 5.2 78 1.95 44 31 43 48 51
1070 15 6.7 4.9 78 1.92 39 26 31 33 42
1186 18 8.5 4.8 80 1.9 37 26 31 33 41
1512 18 8.5 6.2 79 2.14 41 33 38 39 46
1559 18 4.9 7.4 80 2.05 42 37 33 38 43
2192 15 6.3 4.6 76 2.12 39 24 36 39 44
2267 16 7.7 5.4 77 1.94 38 24 30 37 43
3365 16 6.9 5.1 77 2.05 41 24 34 38 44
4227 18 9.5 3.7 76 1.93 34 22 39 38 42
chapinc.org27 Chronic Care Conditions Monitored by CMS, Potentially Disabling
*Based on Medicare FFS Claims; Beneficiary can be counted > 1X
Atrial Fibrillation Cataract Hip / Pelvic Fracture
Acquired Hypothyroidism
Acute Myocardial Infarction Chronic Kidney Disease Hyperlipidemia
Benign Prostatic Hyperplasia
Cancer, Colorectal Chronic Obstructive
Alzheimer's Disease Hypertension
Pulmonary Disease
Alzheimer's Disease,
Related Disorders, or Senile Cancer, Endometrial Depression Ischemic Heart Disease
Dementia
Anemia Cancer, Breast Diabetes Osteoporosis
Asthma Cancer, Lung Glaucoma Rheumatoid Arthritis /
Osteoarthritis
Cancer, Prostate Heart Failure Stroke / Transient Ischemic
Attack chapinc.orgShow Casing Your Agency by CCW Population:
Preparing for HHGMs and Medicare Advantage
• Over the past 12 months how many unique Medicare FFS beneficiaries did you care for in the
preceding unique diagnosis categories? What was their age distribution?
• What was the distribution of number of visits by episode; by discipline by episode; by visit and
discipline in first 30 days? Distribution of number episodes per beneficiary – (e.g. among those with >
1 episode what were the diagnoses, hospitalization history?
• What was your Medicare reimbursement per episode by diagnostic categories?
• Outcomes – remember, consider the % of your enrollees that are MA or that are Medicaid
- CAHPS: also an outcome, did the patient have the experiences that most often lead to quality
care
• Use state benchmarks wherever you can (e.g. PEPPER, PUF, etc.) External entities are using it!
• Consider yourself demonstrating why your HHA should be in a Network
• Long accepted belief: providers with more experience with a given condition/diagnosis are more likely
to achieve desired outcomes with a patient
chapinc.orgEmerging Alternative Payment Models to Save $
• The reality that people who died of a disease just 30 years ago are now living for decades in gradual
debilitation is now acknowledged in Washington circles, as well as the potential cost represented by
‘boomers’ long term chronic disease.
• Scope of coordination increases:
- PCP managing the primary disease – but other specialists must be involved,
o CoPs anticipate communication with all physicians involved in care…..
- Identification of the least costly site that can manage care and follow-up of the patient…but only
to a certain point
o Creation of guidelines for when settings are used, comorbidities are key as well as stay in the
setting and what outcomes for status moves the patient to the next setting
- Post discharge support as a service from ER or hospital, that includes medication management
and use of your own navigators
- Increased monitoring of the patient using technology when patient is ‘stable’,
chapinc.orgNow and Going Forward:
An Executive
Strategic Discussion27 Chronic Care Conditions Monitored by CMS, Potentially Disabling
*Based on Medicare FFS Claims; Beneficiary can be counted > 1X
Atrial Fibrillation Cataract Hip / Pelvic Fracture
Acquired Hypothyroidism
Acute Myocardial Infarction Chronic Kidney Disease Hyperlipidemia
Benign Prostatic Hyperplasia
Cancer, Colorectal Chronic Obstructive
Alzheimer's Disease Hypertension
Pulmonary Disease
Alzheimer's Disease,
Related Disorders, or Senile Cancer, Endometrial Depression Ischemic Heart Disease
Dementia
Anemia Cancer, Breast Diabetes Osteoporosis
Asthma Cancer, Lung Glaucoma Rheumatoid Arthritis /
Osteoarthritis
Cancer, Prostate Heart Failure Stroke / Transient Ischemic
AttackThe Emergence of
Serious Illness
Payment
• Which of the preceding
diagnoses would you say qualify
as long term serious illness?
• Two (2) demonstrations
approved, up and going to
demonstrate effective
management of the health of
individuals ‘pre-hospice’, who
have a ‘serious illness’
• Managing the cost of the
serious ill across time, at home
and in clinics.
Aspire Health: largest community-based palliative
care provider, 19 states and 42 cities.
chapinc.orgThe Serious Illness Provider
• An extra layer of support throughout the course of illness, ensuring that you
receive the care you want, in the location you want it, at the time you need it.
Aspire is here to help you and your family.
• Offering doctors, nurses, social workers and chaplains to provide:
• Symptom management
• Disease management
• Coordination with other medical professionals
• Communication with family members and other caregivers
• Coordination of in-home care and support services
• 24/7 support
chapinc.orgThe Home Care Company of the
New CMS Director of CMMI
chapinc.orgWhat This Home Care Offers:
• Ongoing Care: the Landmark provider sets a visit schedule based on the patient’s goals and
needs. Landmark collaborates closely with the patient’s Primary Care Provider (PCP) and other
specialists.
• Wellness visits: When patients join Landmark, they have access to an entire team working for
them. Beyond the Landmark provider, they will have a local nurse, pharmacist, social worker,
behavioral health specialist and dietitian.
• Urgent care: As needed, patients can receive urgent diagnosis and treatment in their homes,
including fluids, medications, prescriptions, labs and X-rays. No appointment is necessary and
drive time is avoided - long waits and germs at urgent care or the hospital…not to mention
expensive bills.
• Post-discharge care: Coming home from the hospital or SNF can be a challenge.
Unfortunately many patients are re-admitted within a few weeks. New diagnoses and
medications can be confusing. Patients and family members may have different recollections
of instructions. After discharge from the hospital or SNF, Landmark providers meet patients at
home, review medications and follow-up instructions, and put a plan in place to ensure that
they remain healthy at home.
• Care coordination: We work to ensure that PCPs, specialists, family and caregivers are aware
of our patients’ goals and needs, to have a full picture of health.
The words of Landmark
chapinc.orgWhat Do These Examples Tell Us?
• Know what you do best and at what cost, and what outcomes you can sustain
• Care coordination is emerging as a provider reimbursable intervention
• The inclusion of nurse practitioners and doctors delivering care at home, and acting
on behalf of the PCP, specialists or health plans is the scope of home-based care.
• Managing care from the home involves across settings and community resources –
becoming the trusted source over time.
• Post acute uniform reimbursement based on clinical classification of the patient -
not settings - the reason for the IMPACT act-likely to be considered by Congress
early 2020s.
• Expect increased steering and management by MA plans with increasing
enrollment.
This is a 5 year scenario, where do you want to be in 5 years?
What needs to be on your dashboard to get there?
chapinc.orgYou can also read