FMC Sleep and Respiration Rounds June 13, 2018 - Andrea Loewen - Alberta Health Services
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

FMC Sleep and
Respiration Rounds
June 13, 2018
Andrea Loewen
The Pharmacology of Sleep
Andrea Loewen MD, FRCPC, DABIM
Respiratory and Sleep Medicine
Peter Lougheed Centre
Wednesday, June 13, 2018
O1500
O’Brien Centre (Health Sciences Centre)
Agenda
Lunch: 11:30 am
(Served in room 1500, O’Brien Centre)
Presentation: 12:00-1:00
(Room 1500, O’Brien Centre)
The Sleep and Respiration Rounds in the division of Respiratory Medicine at the University of Calgary is a
self-approved group learning activity (Section 1) as defined by the Maintenance of Certification Program of
the Royal College of Physicians and Surgeons of Canada.
Supported by an unrestricted educational grant
from RANA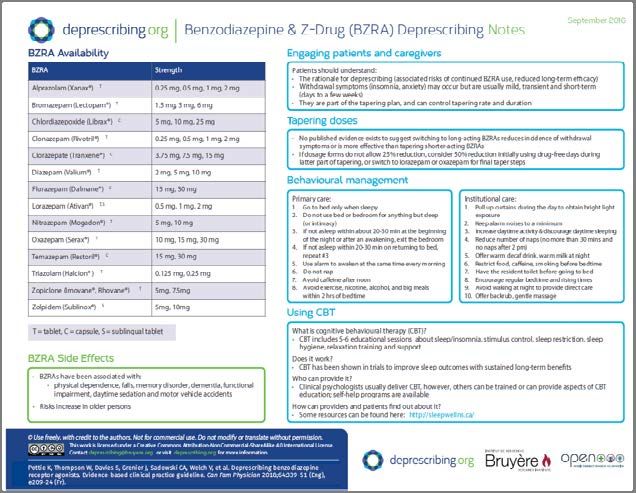
Pharmacology of Sleep
Dr Andrea Loewen
June 13, 2018
Faculty Presenter Disclosure
• Faculty: Dr. A. Loewen
• Relationships with commercial interest:
– None
1
Copyright
• I have taken the appropriate steps to ensure that the use of third
party material in this presentation falls under fair dealing or the
educational exceptions in the Copyright Act.
(http://library.ucalgary.ca/copyright/permitted‐uses)
• I have properly cited third party material in one of the ways outlined below.
– I can also provide citations for all of my material at the end of the lecture.
Order an Ankle X‐ray if:
• Bone tenderness at A
• Bone tenderness at B
• Inability to bear weight
both immediately and in
ED
© Ottawa Health Research
Institute, 1053 Carling Avenue,
Ottawa, Ontario, Canada, K1Y
Copyright Unknown http://lindsay.ucalgary.ca
4E9
Objectives
• Definitions • Pharmacology of
common drugs: alcohol,
• Neurophysiology of sleep hypnotic, narcotics,
• Pharmacology of cannabinoids
anaesthetics
2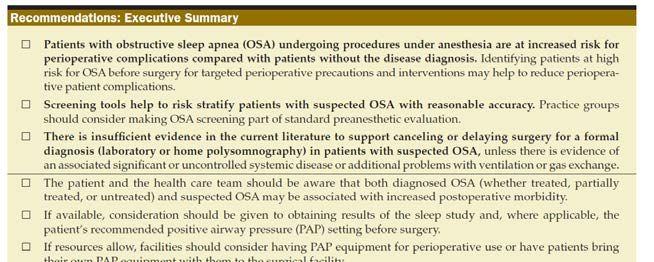
phar∙ma∙col∙o∙gy
ˌfärməˈkäləjē/
noun
the branch of medicine concerned with the uses, effects, and modes of action of drugs.
Definition: Pharmacology
• Pharmacodynamics – the effects of a drug on
biological systems
• Pharmacokinetics – the effects of biological
systems on drugs
– Absorption
– Distribution
– Metabolism (Phase I, II, III)
– Excretion
3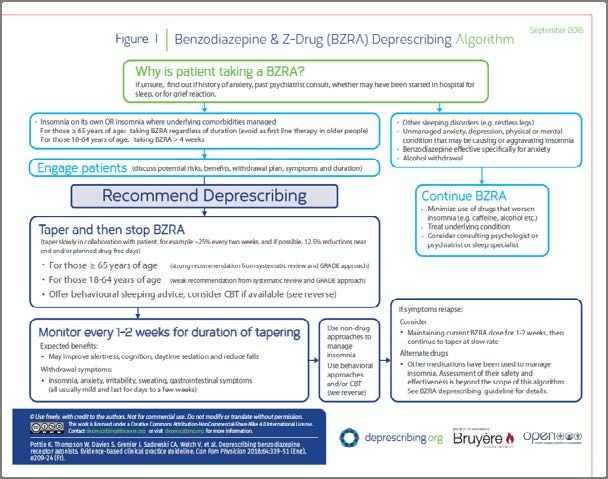
First pass metabolism
• Usually significantly
reduces the activity of
drugs through
metabolism in the liver
first
llustration from Anatomy & Physiology, Connexions Web
site. http://cnx.org/content/col11496/1.6/, Jun 19, 2013
Definition: SLEEP
• 3 behavioural states
– Wakefulness
– NREM sleep Glutamate
– REM sleep Acetylcholine
• Complex interaction of GABA
neurotransmitters Norepineprine
Dopamine
• Dysregulation and Serotonin
medications can lead to Histamine
– Sleep‐wake disorders Hypocretin
– Changes in functional Melanin concentration hormone
state Adenosine
Melatonin
4
Neurochemistry of sleep
Holst S Sleep Clin Med 2018
ANAESTHETIC AGENTS
5
Anaesthesia
• Anesthesia produces EEG changes analagous to
NREM sleep (spindles, delta waves)*
• Molecular target of many anesthetics is GABA(A)
receptor (propofol, volatile agents)
• GABA(ergic) inhibitory projections to wake‐active
regions of brain may be the convergence
between anesthesia and natural sleep
• Other pathways: glutamate antagonism (ketamine)
Franks NP Can J Anesth 2011
Propofol (Diprivan)
• Pharmacodynamics‐ presumed GABAa agonist
(possible glutaminergic activity). Rapidly induces
sleep, ↓BP, ↓ dal volume
• Pharmacokinetics
• Absorption – lipophilic, IV. Onset 9‐50 seconds
• Distribution – LARGE volume of distribution (up
to 60L/kg after 10days. Half life elimination 50
min acutely, but after 10 days can be 1‐3 days)
• Metabolism – hepatic
• Excretion ‐ renal
www.mjworld.net
6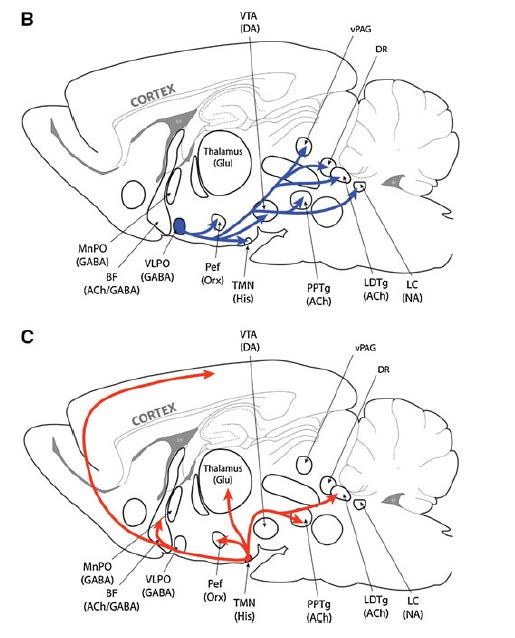
PHARMACOLOGY OF COMMON
SEDATIVES AND HYPNOTICS
Insomnia
• Telephone sample n=2000
• 13% prevalence of insomnia in Canada
• Patient‐reported treatment
– 10% prescription sedative, 9% natural remedy, 6%
OTC remedy, 5% alcohol
Morin CM Can J Psychiatry 2011
7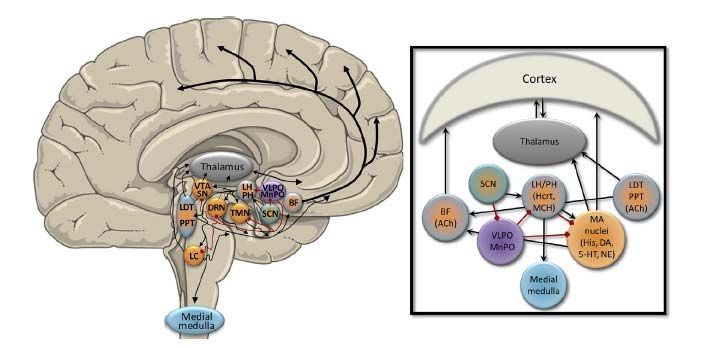
Diphenhydramine (eg. Benadryl)
• Pharmacodynamics – competes for histamine H1
receptor sites in GI tract, respiratory, blood
vessels. AcH effects. Also causes drowsiness via
H1 antagonism in CNS
• Pharmacokinetics
– Absorption – peak in 2hr. Bioavailablility ~60%
– Distribution ‐
– Metabolism – hepatic. Elimination half life adults 9 hr
(7‐12), elderly 14 hr, children 5 hr
– Excretion ‐ renal
8Dimenhydrinate (eg. Gravol)
• Salt of 2 drugs , almost 50:50 ratio
• diphenhydramine : 8‐chlorotheophylline
• Pharmacodynamics: competes for H1
receptors on GI, resp tract and blood vessels,
AcH effects. Nausea. 8‐chlorotheophylline
exerts a stimulant effect to counteract
drowsiness
• Pharmacokinetics: onset 30 minutes, effect 5‐
6 hrs.
Doxepine (Silenor)
• Pharmacodynamics
– Inhib reuptake of 5‐HT and NE in CNS antidepressant
– Antagonist of H1 drowsiness
• Pharmacokinetics
– Absorption delayed with high fat meal >3hr
– Distribution ‐ Vd 20L/kg
– Metabolism ‐ hepatic CYP2C19, 2D6 active metabolite
– Elimination half life 15 hours (30 hr for the metabolite)
– Excretion ‐ renal
• Dosing
– Antidepressant start 25‐50mg (max 300mg)
– Insomnia 3‐6 mg (max 6mg)
9Mirtazepine (Remeron)
• Pharmacodynamics – tetracyclic antidepressant,
cenrtral presynaptic alpha2 adrenergic
antagonistincreasing NE and 5HT release. Blocks H1
and 5HT2 and 3 receptors
• Pharmacokinetics
– Absorption – rapid, bioavail 50%, peak 2hr
– Distribution – low (highly protein bound)
– Metabolism – hepatic. Elimination half life 20‐40 hr
– Excretion – renal
• Sedating antidepressant. 50% of people experience
sedation with the drug. Start 15mg 45mg nightly as
tolerated.
Z‐drugs ‐ Pharmacodynamics
• Similar to benzodiazepines – enhance
inhibitory GABA
• Reduce sleep latency, increases sleep time
10Zopiclone ‐ Pharmacokinetics
• Absorption – oral; bioavailability 77%
• Distribution – 92‐105 L, 45% protein binding
• Metabolism – hepatic (CYP3A4 ‐ YES and CYP2C8)
– Time to peak 2 hr
– Half life elimination 5 hr (elderly 7hr, hepatic
impairment 12 hours)
• Excretion – renal75% (5% unchanged drug)
**cirrhosis – metabolism is decreased 77%**
Zolpidem ‐ Pharmacokinetics
• Absorption – rapid sublingual absorption
• Distribution – 30‐50 L, 93% protein binding
• Metabolism – hepatic (CYP3A4 ‐ limited, CYP2C9,
CYP1A2)
– Time to peak 1.6 hr (2.2 with food)
– Half life elimination 1‐4 (average 2.2) hr (elderly,
hepatic impairment ≥ 10 hr)
• Excretion – renal 58%
**cirrhosis – metabolism is decreased**
11What’s so important about CYP3A4?
• CYP3A4 is responsible for the metabolism of more than 50% of
medicines. It is the most abundant of the dominant CYP3A family.
• CYP3A4 activity is absent in new‐borns but reaches adult levels at
around one year of age.
• The liver and small intestine have the highest CYP3A4 activity.
• Some important CYP3A4 interactions are due to intestinal rather than
hepatic enzyme inhibition (eg, grapefruit).
• There is considerable variability in CYP3A4 activity in the population.
• Women have higher CYP3A4 activity than men.
• Potent inhibitors of CYP3A4 include clarithromycin, erythromycin,
diltiazem, itraconazole, ketoconazole, ritonavir, verapamil, goldenseal
and grapefruit.
• Inducers of CYP3A4 include phenobarbital, phenytoin, rifampicin, St.
John’s Wort and glucocorticoids.
http://www.medsafe.govt.nz/profs/PUArticles/Marc
h2014DrugMetabolismCytochromeP4503A4.htm
Copyrights apply
12Benzodiazepines
• Clonazepam, lorazepam, temazepam,
midazolam
• Pharmcodynamics – enhance GABA
© 2018 UpToDate, Inc.
Copyrights apply
13Rationale for deprescribing BDZ
• Efficacy can wane after as little as 4 weeks
– Amnes c effects can persist longer even as effect on sleep latency ↓
• BDZ associated with risk
– Falls
– MVC
– Cognition/memory
– Daytime sedation
• Deprescribing has been associated with only mild side effects
– Insomnia
– Restlessness
– Anxiety
• Choosing Wisely recommendation
Holbrook CMAJ 2000; Rosenberg Neurosci Biobehav
Rev 1985; choosingwiselycanada.org
14• Try 25% reduction at each step
• If dose does not allow 25% reduction, use 50%
reduction, with alternating days
15PHARMACOLOGY OF OTHER
SEDATING MEDICATIONS
Alcohol (Ethanol)
• Pharmacodynamics – psychoactive substance,
increases GABA inhibitory neurotransmitter.
Also affects glutamate, glycine, Ach, 5‐HT
• Pharmacokinetics –
– Absorption – peak at 30‐90 min if fasting
– Distribution – no protein binding
– Metabolism – alcohol dehydrogenase, liver
– Excretion
16Effects of alcohol on sleep architecture
• Decrease sleep latency
• Increases SWS, decreases REM
• Can cause increased arousal/alpha activity
• Diuresis/ nocturia
• Worsens OSA, sleep‐disordered breathing
• Rebound insomnia
17Opiates
• In the 1990s in the US “pain” was referred to as
“the fifth vital sign”
• Increasing prescriptions of narcotics (ARCOS)
– 1990 2.2million grams morphine, 3273 g fentanyl
– 1996 morphine ↑ by 59%, fentanyl ↑ by 1168%
• preBotzinger complex and
retrotrapezoid/parafacial respiratory nucleus
general normal respiratory rhythm
• Central and peripheral chemoreceptors modulate
this rhythm
Yue, H Med Clin N Am 2010
Opiates ‐ Pharmacodynamics
• Opioids bind opioid receptors
• Four classes of receptors
• preBotzinger sensitive to opioids
• Low doses: ↓ dal volume
• Higher doses: ↓ rate and rhythm genera on AND
blunted hypoxic respiratory drive
• ALSO upper airway obstruction,
glottic/supraglottic obstruction
(fentanyl/sufentail in particular)
Yue, H Med Clin N Am 2010
18Effects of opioids on sleep and
breathing
• Increased central apnea (periodic)
– Longterm methadone CAI > 5 is 30%
• Increased ataxic breathing (Biot)
– 70% longterm opiate users have some, compared
to 5% controls
• OSA – no clear consensus
• Hypoventilation
Wang D Chest 2005;128(3):1348‐56
Farney Chest 2003; 123(2):632‐9
Walker J Clin Sleep Med 2007; 3(5):455‐61
Effects of narcotics on sleep
architecture
• Acute administration of
morphine to healthy
adults
• Decreased SWS, REM
• Increased N2
• No effect on sleep
efficiency, WASO, or
total sleep time
Shaw IR Sleep 2005;28(6):677‐82
Dimsdale JE J Clin Sleep Med 2007;3(1):33‐6
19Opiates – pharmacokinetics
(morphine)
• Absorption – iv, im, oral, transdermal. Onset
5min‐30min. Oral bioavailabilty limited by first
pass metabolism
• Distribution ‐1‐6 L/kg
• Metabolism – hepatic CYP2D6
– Codeine metabolized to morphine. Ultrarapid codeine
metabolizers at risk of respiratory depression, toxic
amounts of morphine accumulate quickly
• Excretion ‐ renal
20Cannabis Sativa
Cannabis
• >100 cannabinoids in cannabis plant (C. sativa, C.
indicus)
• 2 main receptors (CBD1, CBD2)
• 2 extensively researched cannabinoids
– CBD – via CBD 2 analgeisa, anti‐inflammatory
– Delta ‐ 9 THC – via CBD1 euphoria, hallucinations, anxiety,
tachycardia
• In 2016 9% of grade 8 students, 36% of grade 12
students reported using marijuana (US)
• Bidirectional effect on sleep in adolescents.
Johnston LD survey Institute for Social
Research, University of Michigan; Ann
Arbor MI 2017
21Cannabis – Pharmacokinetics
• Absorption/ Bioavailability
– Smoked/ vaped – THC 15‐30%, CBD 11‐45%
– Oral – THC 5‐10%, CBD 5%
• Distribution – Vd is small (protein binding). THC
lipophilic thus higher Vd
• Metabolism – hepatic
– THC is metabolized to 11‐hydroxy‐THC which is more
highly lipophilic and more potent than the original
THC
• Excretion ‐ renal
Effects of cannabis on sleep
architecture
• Attenuates circadian rhythms (changes in body
temperature)
• Acute CBD may↑ TST.
– Anxiolytic dose 300mg CBD did not alter PSG in RCT
(Linares Front Pharmacol 9(13); doi 103389/fphar;2018.00315)
• Acute THC ↓ sleep latency ↓ REM
– Chronic use also ↓SWS
– Withdrawal associated with poor sleep (reported in
40‐70%) and REM rebound
– Adverse effects on working memory longterm
(Tervo‐Clemmens B Neuroimag 2017;169:496‐509)
Furer T Med Sci 2018;6(11); doi;10.3309/medsci
22Treating sleep symptoms of cannabis
withdrawal in chronic users
• BDZ, Z‐drugs
• Gabapentin, N‐acetylcysteine, naltrexone
• Behavioural interventions (CBTI for insomnia)
Furer T Med Sci 2018;6(11); doi;10.3309/medsci6010011
Synthetic Cannabinoids
• Synthetic THC (dronabinol, nabilone)
• Synthetic CBD
• Synthetic Nabiximols (1:1 THC/CBD
combination)
23Dronabinol
• May improve
respiratory stability
through peripheral
serotonergic
antagonism
• PACE II RCT
Prasad B Front Psychiatry 2013;4(1)
Carley DW Sleep 2018;41(1)
Conclusions
• Sleep is modulated by numerous
neurotransmitters and neuromodulators
• Dysregulation of these systems leads to sleep –
wake disorders
• Pharmacological treament is often symptomatic
• Pharmacologic responses are subject to
individual variation – the future may lie in further
research in pharmacogenomics to help tailor
individual therapy
24Copyrights apply
25Caffeine
• Pharmacodynamics – adenosine receptor
antagonist; increases cyclic AMP
(phosphodiesterase inhibitor).
– Promotes wakefulness
– Increases sensitivity to CO2.
– Increases skeletal muscle contraction.
• Pharmacokinetics
– Absorption – oral time to peak 30min‐2hr
– Distribution – Vd 0.6 L/kg
– Metabolism – hepatic CYP1A2
– Excretion – urine, as metabolites
200‐300mg a day is safe and well –tolerated
Modafinil
26Methylphenidate (Ritalin)
Blocks reuptake of NE, DA
Onset
RitaIin Immediate release – 20‐60min
Concerta Extended release – 20‐60 min
Ritalin SR Sustained release – 60‐180min
Duration
3‐5 hr, 8‐12 hr, 2‐8 hr, respectively
Dextroamphetamine (Dexedrine)
• Sympathomimetic amine that promotes
release of DA and NE
• Onset IR 4‐6hr, ER ~8hr
• Peak IR 3hr, ER >8hr
• Elimination half life 10‐12 hr
27Lisdexamfetamine
• Prodrug that is metabolized to
dexamphetamine
• Rapid onset, peak in 1 hr, duration 8‐14 hr
• RBCs hydrolyze the prodrug, the active
metabolite (dexamphetamine) is hepatically
metabolized
28Deprescribing benzodiazepines
• Should be offered to all patients >65 on BDZ
• Should be offered to anyone 18‐65 who has
been on >4wk BDZ
• Should be offered for both primary and
secondary insomnia
• Does NOT apply to patients with insomnia
related to psychiatric condition (depression,
anxiety, other physical/mental health
condition perpetuating insomnia)
Pottie Can Fam Physician May 2018
Neurophysiology of Sleep
Franks NP Can J Anesth 2011
29Chung F et al Anaesthesia and Analgesia August 2016; 123(2)
30You can also read