Food allergy in Primary Care Overview & update 2019 - Dr Heidi Northover Consultant Paediatrician
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Food allergy in Primary Care
Overview & update 2019
Dr Heidi Northover
Consultant Paediatrician
Intended learning outcomes
To gain a better understanding of;
Food allergy in children, including nut & egg allergy.
Risk of allergy, death due to allergy
Most recent guidance on prescribing and use of adrenaline
auto-injectors
The use and abuse of allergy tests, when should siblings
be tested?

The extent of the problem
UK is in top three countries in the world for the
highest incidence of allergy
In the last decade, the cases of food allergies have doubled
Number of hospitalisations caused by severe allergic
reactions has increased 7-fold (EAACI, 2015)
Nearly 20% of the UK adults consider themselves to have a
food allergy or intolerance:
•
Childhood allergy in context
How common are allergies?
How common is death from allergy?
What is responsible for most childhood
anaphylaxis?
Most childhood deaths are associated with which
allergen?
Who is at highest risk of death due to allergy?
Toddlers or teenagers?
Childhood allergy in context
Allergies are common; 1:10 ‐15
Death from allergies are rare; 1:10 million
~20% of adults believe they have a food allergy;
only 2‐5% truly do
10% children have raised IgE to peanut but only
1% children have a clinical reaction when exposed
to peanut
Food accounts for 90% childhood anaphylaxis
Anaphylaxis &
deaths due to food allergy
Majority of deaths associated with nuts, especially
peanuts
Combined mortality results from UK, USA &
Sweden over 14 year period;
46 deaths in children; 34 due to peanuts or tree
nuts
3/46 in children < 5 years of age, 1 to milk, 1 to egg
43/46 > 5 years
Deaths due to food allergy
Risk to all food allergic people:
Risk of death is 1.81 micromorts
100+ times more likely to die in RTC than from food
anaphylaxis
Those < 19 years of age; higher risk group
Risk is 3.25 micromorts
Still more likely to be murdered!
Higher risk individuals;
Asthma, teenagers, previous history of anaphylaxis
Responsible foods
In the UK, 9 foods are responsible for 90% of allergic
reactions to food.
Together, peanuts and tree nuts allergens account for 70-90%
of reported fatal food-induced anaphylaxis.
Around 2% of children are allergic to eggs and 2%-3% to cow's
milk.
After peanuts and tree nuts, milk is the third most common
food allergen to cause life-threatening anaphylaxis.
Approximately 40% of infants and young children with eczema
suffer from food allergy.
Natural history of food allergy varies with the food; is it
transient or lifelong?
Prevalence varies with exposure; sesame seed & birds’nests.
Allergenicity varies with degree of cooking & processing of
food.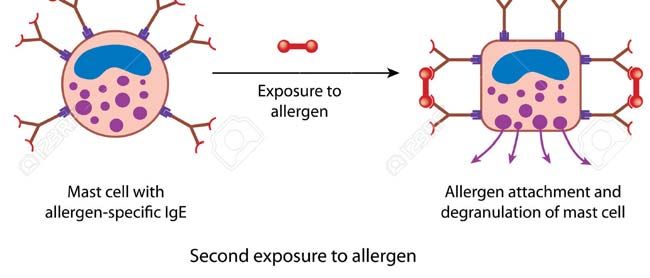
Top 9 food allergens in UK; responsible for 90% allergic reactions 1. Peanuts Lifelong (>80%) 2. Tree nuts Lifelong 3. Milk Transient 4. Egg Transient 5. Soya Transient 6. Wheat Transient 7. Finfish Lifelong 8. Shellfish Lifelong 9. Sesame Lifelong (>80%)
Egg allergy
Prevalence approximately 2% in children & 0.1% in adults
First presentation usually in infancy; typically present within
minutes of first apparent exposure to egg white:
Urticaria and/or angio-oedema
Vomiting
Wheeze with rapid onset
70% will out grow by 5 years of age
Most reactions are mild, with facial urticaria only.
More severe reactions with significant respiratory symptoms are
less common
75% of children with an egg allergy can eat plain cakes & biscuits
containing egg
History of more severe reaction to egg more likely to have
persistent disease
Should be referred to a specialist serviceVaccinations and egg allergy
Cultured on derivatives of hens egg
MMR
Yellow fever
Influenza
Skin prick testing; poor predictive value as a screening tool
Serum IgE testing
Egg ladder; Introduction of well-cooked egg can help to induce
immune tolerance
https://www.bsaci.org/Guidelines/egg-allergy
https://www.bsaci.org/Guidelines/MMREggRecommendations.pdfThe egg ladder https://www.thh.nhs.uk/documents/_Patients/PatientLeaf lets/paediatrics/allergies/PI414_Egg-Ladder-1.pdf
Nut allergy
Tree nuts Peanut relatives = legumes Brazil Peas Hazel Beans Almond Soya (edamame) Cashew Lentils Pistachio Carob Walnut Liquorice Macadamia
Peanut allergy (Ground nuts, monkey nuts, arachis)
Common (1:100 people)
Most common cause of fatal & non fatal
anaphylaxis to food
Most allergies to peanut are lifelong
Typically cause acute, IgE mediated reactions
(Type 1 hypersensitivity)
Other names for peanuts; BEWARE!Management of food allergy
Allergen avoidance
Emergency treatment/action plans including
antihistamine for all
Cetirizine or desloratidine; non sedating,
long acting
Piriton; sedating, short acting
Adrenaline auto injector pens; Epipen ®
JEXT® Emerade®Adrenaline auto-injectors (AAI) New BSACI guidance October 2016 AAP update on use of adrenaline in anaphylaxis 2017 Primary care guidelines
BSACI Joint statement;
key recommendations
Prescribe an AAIP as soon as possible after a suspected anaphylactic
reaction
Give training on how and when to use an AAIP
Aim is to start treatment early, without waiting for help.
Refer to an allergy specialist for a comprehensive risk assessment & a
personal care plan, including the practical steps to minimise potential
risks in everyday life.
Sample action plans available on BSACI website
Number of AAIPs
BSACI has not made a blanket recommendation on the number of auto-injectors
anyone should carry as this should be based on a risk assessment.
Every patient should have a personally tailored management plan, which
should determine whether one, two (or no) auto-injectors should be
prescribed.BSACI guideline:
Ewan et al Clinical and Experimental Allergy;
Volume 46, Issue 10 October 2016
American Academy of Pediatrics guidance (2017)
Adrenaline/epinephrine is the first-line treatment for anaphylaxis.
Use in patients with significant airway involvement or hypotension,
occurring as part of an anaphylactic reaction.
All other medications, including antihistamines and
bronchodilators such as salbutamol, provide adjunctive treatment
but do not replace adrenaline.
Do not hesitate to use adrenaline for possible anaphylaxis, even in
the absence of proof that patients' symptoms are the result of an
allergic reaction.
Delays in using adrenaline may lead to more severe and treatment
resistant anaphylaxis.
Adrenaline in appropriate doses is safe, there are no absolute
contraindications to its use in anaphylaxis.
Adrenaline auto-injectors;
who should have one?
Those patients who should be considered for adrenaline auto-injectors
include;
Severe systemic reactions, where the allergen cannot be easily
avoided
Allergic to high-risk allergens, for example nuts with other risk
factors (such as asthma), even if the reaction was relatively mild
Who had a reaction in response to trace amounts of allergen/trigger
Who cannot easily avoid the allergen
With continuing risk of anaphylaxis (e.g. food-dependent exercise-
induced)
With idiopathic anaphylaxis or exercise induced anaphylaxis
Strongly positive skin prick tests
With significant co-factors e.g. asthma requiring brown inhalers
Teenagers (high risk group)
(Parents insist)How much should be used?
JEXT/Epipen Junior = 150 ug
JEXT/Epipen = 300 ug
In a healthcare setting; up to 500 ug in a teenager/adult
Adrenaline should be given in the muscle of the mid-
outer thigh because that helps achieve peak efficacy
and is safer than injecting a bolus intravenously.
Emerade
https://www.sps.nhs.uk/wp-content/uploads/2018/09/Summary-of-the-key-
differences-between-3-presentations-of-adrenaline-prefilled-syringes-
final.pdfEmerade
In the UK, BNF/NICE recommend 500 mcg in adults and
children over 12 years for self-administration
UK Resuscitation guidelines for healthcare providers
recommend 500 mcg for most patients above 12 years.
Emerade is available in a 150, 300 and 500 mcg dose (5-10
ug/kg)
Longer needle
Longer shelf life of 30 months
No upper temperature limits
Remove needle cap and inject
Keep in place for 5 seconds
Rub area
Call 999
Lie down unless difficulty breathing The prescriber must take responsibility for training
Training videos
https://www.emerade-bausch.co.uk/patient/how-to-use-emerade
http://www.epipen.co.uk/ hcp/supporting-patients/
https://hcp.jext.co.uk/about-jext/video-demonstrations/Management of anaphylaxis Call for help Lie patient flat Raise legs Oxygen Adrenaline im Then fluid bolus Chlorphenamine Hydrocortisone iv
Lily aged 2 years
Mother made home made
brownies containing hazelnuts and
Nutella (hazelnut spread)
Eaten Ferrero Rocher chocolates
before without problems
Ate a brownie for breakfast, went
to school
Gave her Piriton – little effect
Came home and felt ‘hot’ – mum
Repeated Piriton – little effect
took her uniform off – covered in
red itchy blotchy rash Went to bed- rash improved
overnight
No complaints from school
Ate another brownie the next
morning – rash returned
Referred ? Hazelnut allergy
History – what was unusual?What was unusual? Eaten hazelnuts before? Was able to go to school? Rash appeared over a period of hours? Felt hot when she came home? Piriton had little effect? Rash improved overnight? She ate another brownie the next morning?
Allergy testing
Can I have some allergy tests doctor?
Jack has peanut allergy. Can his baby sister
be tested too?Allergy testing Reminder 10% children have raised IgE to peanut but only 1% children have a clinical reaction when exposed to peanut SPT to egg: poor predictive value as a screening tool
Using and interpreting allergy tests Allergy tests provide supportive evidence Should only be used if there is evidence from the history to suggest the responsible allergen They should not be used as a screening test Used incorrectly there is a significant risk of misinterpretation of the results/misdiagnosis SPT and SSIgE give a prediction of likelihood of reaction not severity
Using allergy tests with a clinical history
Likelihood of clinical allergy from specific IgE
Likelihood of clinical Low (15 Ku/L)
allergy from history 15 Ku/L)
High, eg urticaria & Possible allergy Probable allergy ALLERGY
wheeze on more than
one exposure
Intermediate eg urticaria Possible allergy Possible allergy Probable allergy
on one exposure
Low eg non IgE No allergy Possible allergy Possible allergy
symptomsNICE recommendations
Do not carry out allergy testing without first taking
an allergy focused clinical history.
Based on the results of the allergy-focused clinical
history, if IgE mediated allergy is suspected:
Offer a skin prick test and/or blood tests for specific
IgE antibodies to the suspected foods and likely co-
allergens.
Interpret the results of tests in the context of
information from the allergy-focused clinical history.
Do not use atopy patch testing or oral food
challenges to diagnose IgE-mediated food allergy in
primary care or community settings
Do not use allergy testing ‘to screen’ for allergy.Allergy tests; which are valid in the diagnosis of food allergy? Skin prick tests Oral food challenge Hair analysis VEGA testing Serum specific IgE IgG4 York test Patch testing
Allergy tests; which are valid in the diagnosis of food allergy? Skin prick tests Oral food challenge Hair analysis VEGA testing Serum specific IgE (RAST, Immunocap) IgG4 York test Patch testing
Evidence based allergy tests
Skin prick tests; cheap, instant results, almost any food
can be tested (prick- prick)
Serum specific IgE; “RAST” or Immunocap; one blood test,
risk free, more expensive, delayed results
Gold standard: Oral food challenge; but labour intensive
and slow
Avoid antihistamines for 5 days before
Pin-head size amount
Pea size amount
Double every 15 min until normal portion tolerated
Observe for 2 hrs after food has been eaten
Patch testing; only useful for contact dermatitisCost of allergy tests per person
(8 allergens)
Skin prick test* Blood test**
Test cost £1.70 £96.00
Staff cost £44.49 £30.97
Consumables £1.08
Total cost £47.27 £126.97Molecular allergy or component
resolved diagnosis (MA or CRD)
Maps the allergen sensitization of a patient at a molecular level;
increased accuracy in allergy diagnosis & prognosis.
Currently more than 130 allergenic molecules commercially available
for in vitro testing.
Enables three key aspects of allergy diagnosis:
Resolves genuine versus cross-reactive sensitization in poly-sensitized
patients, thereby improving the understanding of triggering allergens.
Assessment of, in selected cases, the risk of severe, systemic versus mild,
local reactions in food allergy, thereby reducing unnecessary anxiety for
the patient and the need for food challenge testing.
Identifies patients and triggering allergens for specific immunotherapy
(SIT).Use of Ara h1, 2 & 3 in peanut allergy Component resolved specific IgE testing for peanut allergy more accurately identifies patients with peanut allergy than the routine use of peanut extract–specific IgE serology or skin prick testing. Among the peanut component proteins, IgE antibodies to Ara h2, and to a much lesser extent Ara h1, Ara h3, Ara h6, and Ara h9, have been identified as the major driver of clinically relevant allergy. Sensitization to Ara h2 is found in up to 90% of patients with clinical peanut allergy. Ara h2 in particular, is considered a risk marker for severe allergic reactions. In a patient with positive IgE test to peanut, prognosis can be very different depending on whether the sensitization is linked to a Bet v 1- like protein (major allergen component of white birch pollen), a seed storage protein (Ara h2), or an lipid-transfer protein (LTP).
Peanut FC & IgE tests RAST – specific peanut IgE Positive IgE to team The team is dangerous The team is a threat 13 players or components to the threat Is one more dangerous & significant than the others?
Component resolved diagnosis
RAST/SSIgE
13 players or components to
the threat
Is one more dangerous &
significant than the others?
Component resolved diagnosis tells us that ….
Only 4 players are a real threat
The others may look like a threat (perhaps one is the twin
brother of a star player in another team?) or be
insignificant/harmlessSan Antonio – testing the siblings
of food allergic children
Conclusions:
False-positive results could lead to food avoidance, which
can increase the risk of developing an allergy down the
road.* LEAP
Many children are sensitized to a food, so they will have a
positive test result, but that does not mean they have a
true food allergy (peanuts)
The presence of sIgE reflects allergic sensitization
and not necessarily clinical allergy.Chicago Family Cohort food allergy study
478 children with confirmed food allergy, and 642 of their siblings.
Caregivers completed detailed screening histories for both the
allergic child and the siblings.
Skin prick testing (SPT) & serum specific IgE (sIgE) on siblings
Cow’s milk, egg white, soybean, wheat, peanut, walnut, sesame
seed, fish mix, and shellfish mix.
Results
34% of the siblings had no sensitization to foods and no clinical
symptoms
53% had sensitization to food (potential for false positive in > 50%)
13% had an actual food allergyLEAP study- Gideon Lack et al
Introduction of peanut-containing foods into the diets of
high-risk infants (early onset atopic disease eg egg allergy or
severe eczema) aged between 4 and 11 months.
Found
Early, sustained consumption of peanut products was
associated with a substantial & significant decrease in the
development of peanut allergy in high-risk infants.
Conversely, peanut avoidance was associated with a greater
frequency of clinical peanut allergy than was peanut
consumption.
Delaying introduction can be associated with an increased
risk for peanut allergy.Lily– what was unusual?
Had eaten hazelnuts before without problems
Rash appeared over hours – not typical of type 1 reactions
Piriton didn’t seem to help
So what next?
SPT to hazelnut (positive is >3mm greater than control)
Negative control 0 mm, positive control 8 mm
Hazelnut 0 mm
Serum specific IgE – total = 780 Ku/L
Hazelnut, brazil, cashew, walnut, pistachio < 0.35
(negativePhysical signs of allergic disease
Physical signs of allergic disease
Dermatographism;
Form of physical urticaria to touch & pressure.
Unknown cause
Allergic shiners
Dennie Morgan folds
Lick eczema
Allergic mannerisms
Allergic salute
Side swipeAny questions?
You can also read