Confronting Psoriatic Disease: Putting New Tools to Work - Emerging Challenges in Primary Care: 2018 - Formatted_Birmingham
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Emerging
Challenges in
Primary Care:
2018
Confronting Psoriatic
Disease: Putting New Tools
to Work
Faculty
§ Adelaide A. Hebert, MD
The University of Texas
Professor, Department of Dermatology
Director, Pediatric Dermatology
Houston, TX
2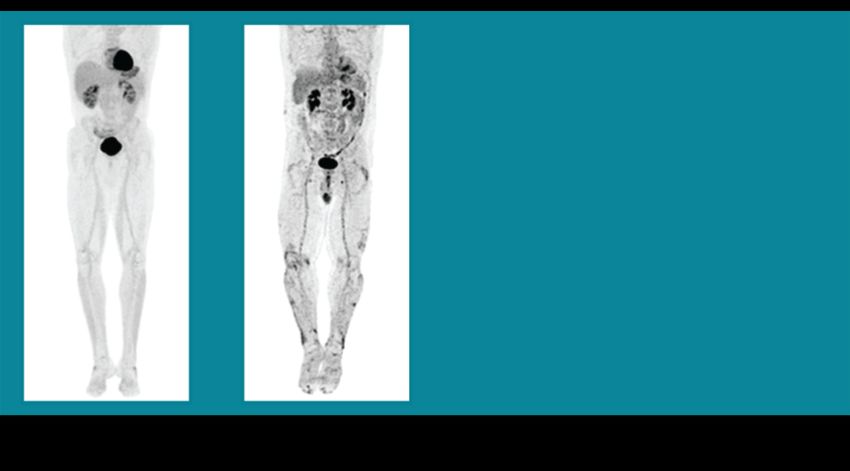
Disclosures
§ Adelaide A. Hebert, MD serves as a speaker for Pfizer,
Amgen, and Valeant. Dr. Hebert also serves on the research
grant team for Promins, GSK, Mayne, Sienna, Amgen,
Medimetriks, Galderma, and Celgene. Additionally, she serves
on the DSMB for GSK and Sanofi-Regeneron.
3 3
Learning Objectives
1. Identify and describe the clinical features of psoriatic skin
and joint disease
2. Review and discuss associated comorbidities and emerging
bio factors and their significance in the management of
psoriatic disease
3. Discuss the expanding and dynamically changing treatment
paradigm for psoriasis and its related disorders
4. Review and interpret up to date evidence-based clinical trial
data and the latest treatments available for the
management of psoriatic disease
4 4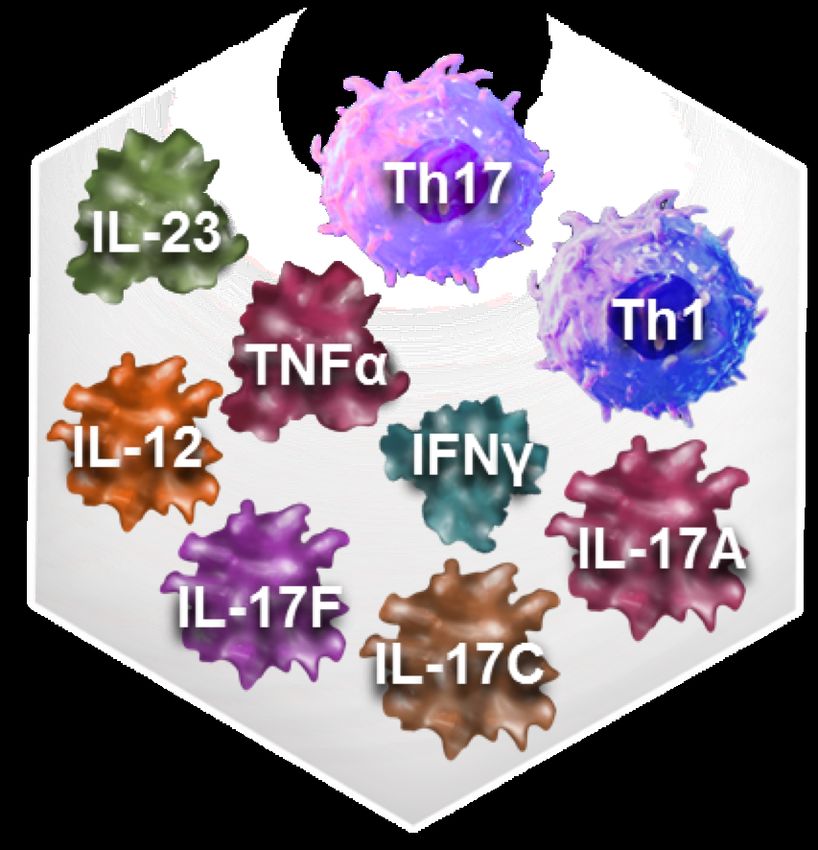
PRE-TEST QUESTIONS
5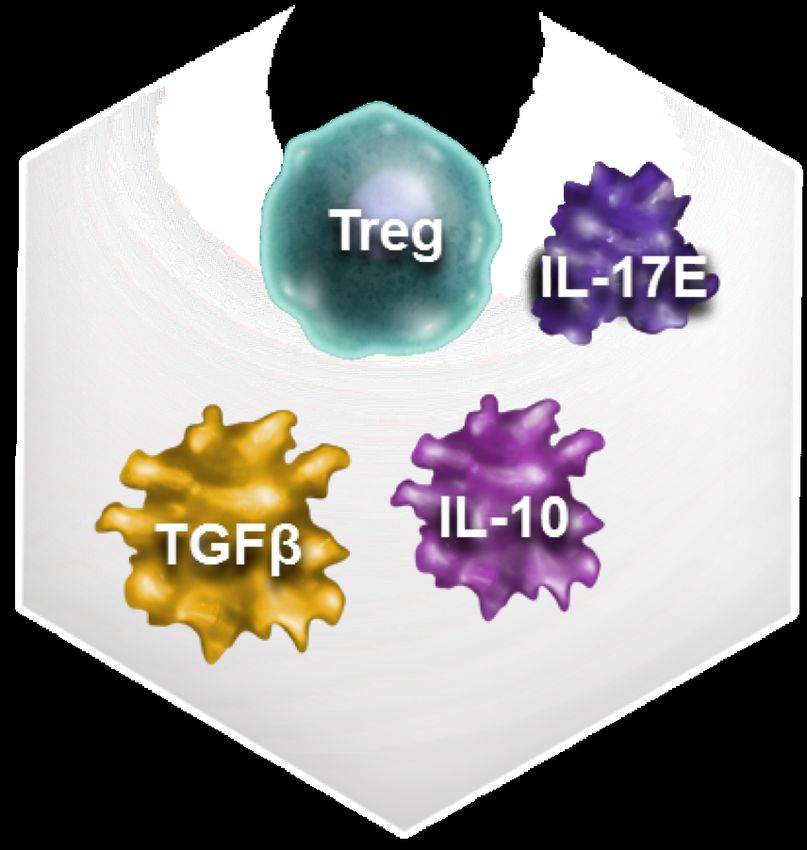
Pre-test ARS Question 1
Which of the following are among the most
common symptoms of psoriatic disease?
1. Enthesitis
2. Depressed mood
3. Pruritic skin lesions
4. Symmetric joint pain and swelling
6
Pre-test ARS Question 2
According to a population-based study, the relative
risk for myocardial infarction is highest in which of
the following patients with psoriatic disease?
1. Older patients with severe psoriasis
2. Older patients, regardless of severity
3. Younger patients with severe psoriasis
4. Younger patients with longer duration of
disease
7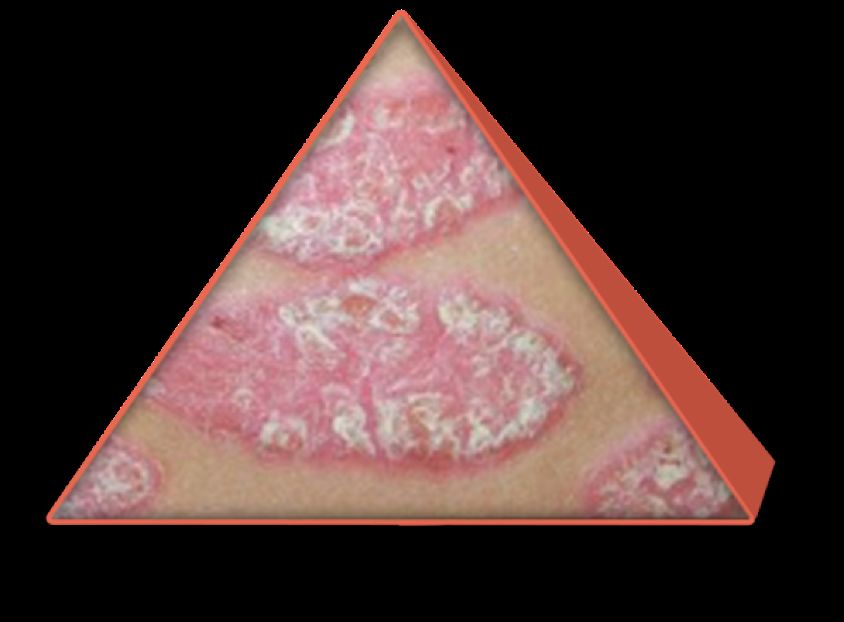
Post-test ARS Question 3
A 63-year-old obese man with a 12-year history of psoriasis and
2-year history of psoriatic arthritis presents reporting increased
disease activity (5% BSA, moderate joint disease activity).
Current medications include topical steroids and NSAIDs. He
recently underwent PCI for management of unstable angina.
Which of the following might be appropriate based on this
history?
1. Avoid methotrexate based on cardiovascular risk
2. Avoid TNF inhibitors based on cardiovascular risk
3. Consider biologic therapy or PDE4 inhibitor despite his
cardiovascular risk
4. Consider phototherapy and switch from NSAID to
acetaminophen
8
Pre-test ARS Question 4
How confident are you in your ability to
recognize co-morbidities associated with
psoriatic disease?
1. Not at all confident
2. Slightly confident
3. Moderately confident
4. Pretty much confident
5. Very confident
9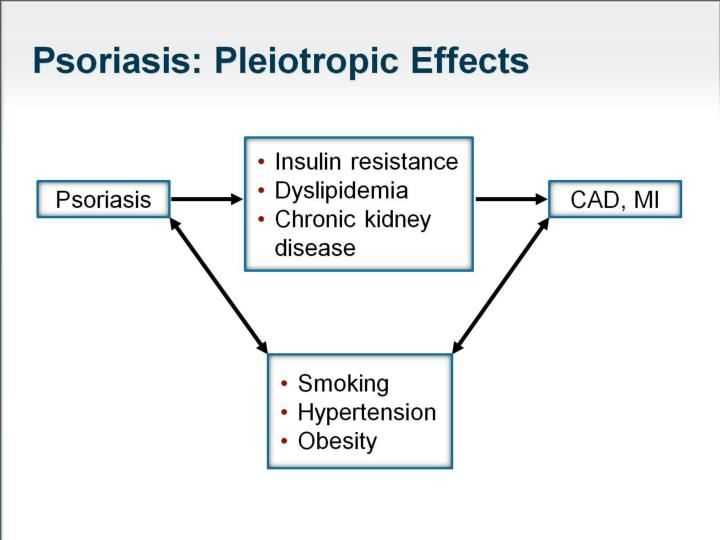
Pre-test ARS Question 5
How confident are you in your ability to
integrate the latest treatment data into the
management of patients with psoriatic disease?
1. Not at all confident
2. Slightly confident
3. Moderately confident
4. Pretty much confident
5. Very confident
10Psoriatic Skin Disease
Clinical Features Epidemiology
§ Chronic, relapsing, immune § Bimodal age of onset
dysregulatory inflammatory § 2nd-3rd decade of life and
disease
after 50 years of age
§ Erythema (redness)
§ OnsetAssessing Severity
of Psoriatic Skin Disease
§ Imagine 1 palm equal to 1% of your
body surface area.
§ Mild : 1-3%
§ Moderate: 3-10%
§ Severe: More than 10%
§ Location also determines severity
§ Scalp
§ Hands and feet
§ Groin and skin folds
12Plaque Psoriasis
§ Most common variant
§ 80% of all psoriasis cases
§ Other variants: guttate, inverse,
erythrodermic, scalp, nail, and
palmoplantar
§ Differential diagnosis
§ Eczema
§ Drug eruption
§ Tinea corporis
13Precipitating Factors
§ Stress
§ Infections
§ Group A beta-hemolytic
streptococcus ® guttate psoriasis
§ Physical trauma
(Koebnerization)
§ Drugs
§ Lithium
§ Beta-adenergic blockers
§ Systemic steroids (rebound)
§ Anti-malarials
§ NSAIDS
§ Interferon
§ Gold 14Psoriatic Arthritis
§ Estimated prevalence 6%-42% of patients with psoriasis
§ Most common between 30 and 50 years of age
§ Increases with disease severity and duration
§ Earlier onset associated with worse prognosis
§ Timing of onset:
§ Psoriasis precedes arthritis in 75% of cases
§ Arthritis onset ~10 years after skin lesions
§ Synchronous onset in 15% of cases
§ Arthritis precedes psoriasis in 10% of cases
§ Findings may include:
§ Asymmetric or symmetric inflammatory joint disease
§ Distal interphalangeal joints (DIP)
§ Spondylitis, enthesitis, dactylitis
15
Gottlieb A et al. J Am Acad Dermatol. 2008;58:851-864.Prevalence of rheumatologist-diagnosed psoriatic arthritis in
patients with psoriasis in European/North American
dermatology clinics
Philip J. Mease, MD, Dafna D. Gladman, MD Kim A. Papp, MD, PhD Majed M. Khraishi,
MD Diamant Thaçi, MD Frank Behrens, MD Robert Northington, PhD Joanne Fuiman, MS
Eustratios Bananis, PhD Robert Boggs, PhD Daniel Alvarez, MD
DOI: http://dx.doi.org/10.1016/j.jaad.2013.07.023
Background
Prompt identification and treatment of psoriatic arthritis (PsA) in patients with psoriasis is critical to reducing the risk of joint
damage, disability, and comorbidities.
Objective
We sought to estimate PsA prevalence in patients with plaque psoriasis in 34 dermatology centers in 7 European and North
American countries.
Methods
Consecutive patients were evaluated by dermatologists for plaque psoriasis and subsequently by rheumatologists for PsA.
PsA prevalence was estimated primarily based on rheumatologists' assessment of medical history, physical examination, and
laboratory tests.
Results
Of 949 patients evaluated, 285 (30%) had PsA (95% confidence interval 27-33) based on rheumatologists’
assessment. PsA diagnosis changed in 1.2% of patients when diagnostic laboratory tests were added to
medical history and physical examination. Of 285 patients given the diagnosis of PsA, 117 (41%) had not 16
been previously given the diagnosis.
https://www.ncbi.nlm.nih.gov/pubmed/23981683#Psoriasis Is Caused by Uncontrolled Inflammation1,2
Inflammatory response contributes to increased
keratinocyte turnover and joint disease
Proinflammatory Anti-inflammatory
IFN, interferon; IL, interleukin;
TGF, transforming growth factor;
Th, T-helper; TNF, tumor necrosis factor;
Treg, regulatory T-cell.
1. Goodman et al. Crit Rev Immunol. 2012;32:65-79.
2. Lowes et al. Annu Rev Immunol. 2014;32:227-255.Psoriasis is a Systemic Inflammatory
Disease
Increased signal indicative of
systemic inflammation1:
Knee and Ankle
Liver
Aorta and Femoral Arteries
Psoriatic Plaques
Chronic, widespread inflammation
may contribute to psoriasis-
associated comorbidities2
Person without Psoriasis Person with Psoriasis
Positron emission tomography (PET) scan
1. Mehta NN, et al. Arch Dermatol. 2011;147(9):1031-1039. 2. Gottlieb AB, et al. Am J Med.
2009;122(12):1150 e1151-1159. Psoriasis PET Scan Images Copyright © 2011 American Medical Association. 18
All rights reserved.Comorbidities
Established Emerging
§ Psoriatic arthritis § NAFLD (Non-Alcoholic Fatty
Liver Disease)
§ IBD § Lymphomas
§ Sleep apnea
§ Psychological and
§ COPD
psychiatric disorders
§ Osteoporosis
§ Metabolic syndrome § Parkinson´s disease
§ Celiac disease
§ Cardiovascular disease § Connective tissue disease
§ Erectile dysfunction
§ Uveitis
§ Aortic aneurysm
§ Fractures
19
Oliveira MF et al. Psoriasis: classical and emerging comorbidities. An Bras Dermatol. 2015;90(1):9-20.Metabolic Comorbidities
Obesity Diabetes
§ Doubles risk for § More common in
psoriasis psoriasis
§ BMI correlates with § Role of TNF-α in insulin
psoriasis severity resistance
§ Significant correlation of
blood resistin levels with
psoriasis activity
Hammings EA et al. Med Hypoth. 2006;67:76; Johnson A et al. Br J Dermatol. 2008; 159:342; Cohen A et 20
al. J Am Acad Dermatol. 2007;56:629.Risk of Myocardial Infarction in
Patients with Psoriasis
§ Incidences per 1000 pt-y for: Adjusted RR of MI in patients with
psoriasis based on patient age
§ Control 3.58 (95% CI, 3.52-
3.65)
§ Mild psoriasis: 4.04 (3.88–
4.21)
§ Severe psoriasis 5.13 )4.22-
6.17)
§ Conclusions:
§ Psoriasis may confer an
independent risk of MI
§ The RR was greatest in young
patients with severe psoriasis
21
Gelfand J et al. JAMA 2006;296:1735-41Comparing Comorbidities
§ Risk for diabetes higher in psoriasis than rheumatoid
arthritis (hazard ratio)
Psoriasis RA
Diabetes (all patients) 1.2 0.9
CV death (DMARD) 1.5 1.6
All-cause death (DMARD) 1.8 1.6
§ Severe psoriatic disease linked to higher rate of
atherosclerotic outcomes (hazard ratio)
Severity of Psoriatic Disease
Mild Moderate Severe
Atherosclerotic outcomes 1.14 1.39 1.81
DMARD – Disease-modifying antirheumatic drug
22
Dubreuil et al. Rhematology. 2014;53:346-352; Ogdie A et al. Ann Rheum Dis. 2014;73:149-153; Yeung H
et al. JAMA Derm. 2013;149:1173-1179.Risk of Lymphoma in Psoriasis
Lymphoma Adjusted relative risk (RR, 95% CI)
Mild Psoriasis Severe Psoriasis
All lymphoma 1.34 (1.16-1.54)† 1.59 (0.88-2.89)‡
Non-Hodgkin’s
1.15 (0.97-1.37)‡ 1.34 (1.16-1.54)§
lymphoma£
Hodgkin’s lymphoma 1.42 (1.00-2.02)** 3.18 (1.01-9.97)**
T-cell lymphoma 4.10 (2.70-6.23)† 10.75 (3.89-29.76)†
§ Population-based cohort study of UK General Practice Research Database
(1988-2002). 153,197 psoriasis patients and 765,950 controls.
§ Severity determined by use of systemic treatment for extensive disease
(3,994 yes, 149,203 no).
*RR = relative risk (confidence interval), adjusted for gender and age; †PPsoriasis Affects Employment
Adults with severe psoriasis Adults with severe psoriasis
reported that their health reported that they have lost a job
negatively impacted their work because of their health condition
Percentage of Subjects
Percentage of Subjects
50 50
40 PClinical and Psychological
Burden of Psoriasis
• Psoriasis patients are more likely to suffer from depression, to use
an SSRI, and have CV risk factors compared with control*
Increased likelihood (%)
n= 24,256
* After adjusting for age, gender, and Deyo-Charlson comorbiditiy.
Dabbous O, et al. AAD 2007: P2743.
25
Kimball, AB, et al. Am J Clin Dermatol. 2005;6(6):383-92.26
Hospitalized Moderate-Severe
Psoriasis Patients
Condition OR
Type 2 Diabetes 2.48
Hypertension 3.27
Hyperlipidemia 2.09
Coronary Heart Disease 1.95
Metabolic Syndrome 5.29
Smoking 2.96
Regular alcohol consumption 3.33
Heavy alcohol consumption 3.61
27
Sommer DM et al. Arch Dermato res. 2006; 298:321.Clinical Significance
§ Increased risks for MI, stroke, cardiovascular death,
diabetes, chronic kidney disease
§ 5 years of life lost
§ 10-year risk for major CV event attributable to psoriasis
= 6%
§ Risk for cardiovascular disease in patients with severe
psoriasis similar to risk conferred by diabetes
§ Patients treated for severe psoriasis are 30x more likely
to experience MACE (attributable to psoriasis) than
melanoma
(MACE = Major Adverse Cardiac Event)
28
Abuabara, K, et al. Br J Dermatol. 2010;163:586-592Screening Recommendations
§ Hypertension
§ Diabetes (fasting plasma glucose,
HbA1c, or oral glucose tolerance test)
§ Cardiovascular Risk Assessment
§ Annual skin cancer exam
29Talk With Your Patients About
Comorbidities
§ How does your disease affect you on a
daily basis?
§ Lifestyle modification recommended for
things you can control (weight, smoking,
alcohol consumption)
30Treating Psoriatic Disease:
A Focus on Systemic Therapy
§ Topical therapy
§ Moisturizers
§ Cortisone and steroid creams Mild
§ Calcipotriene
§ Vitamin A retinoids Psoriasis
§ Ultraviolet light/Lasers
§ UVB
§ PUVA
§ Excimer laser
§ Systemic Therapy Moderate
§ Methotrexate
§ Cyclosporine to
§ Acitretin (Soriatane)
§ Apremilast (Otezla) Severe
§ Biologics
§ Etanercept (Enbrel) Psoriasis
§ Infliximab (Remicade)
§ Adalimumab (Humira, Exemptia)
§ Ustekinumab (Stelara)
§ Golimumab* (Simponi)
§ Certolizumab* (Cimzia)
§ Secukinumab (Cosentyx)
§ Ixekizumab (Taltz)
§ Guselkumab (Tremfya)
§ Brodalumab (Siliq)
32
*FDA approved or psoriatic arthritis and not psoriasisAdverse Events Topical Steroids § Tachyphylaxis § Skin atrophy § Telangiectasias § Striae § Discoloration § HPA axis suppression 33
Conventional Oral Agents
Drug Adverse Effects Lab Tests Previous
Preg. Cat.
Methotrexate • Hepatotoxicity • LFTs X
• GI (nausea/vomiting) • CBC with platelets
• Malaise • Liver biopsy when
• Reactivation of phototoxic reactions 1.5 g methotrexate
• Ulcerative stomatitis reached
• Myelosuppression/anemia
• Pulmonary fibrosis
• Induction of lymphomas
Cyclosporine • Renal toxicity • Renal function tests C
• Hypertension • CBC with platelets
• GI (nausea/vomiting) • Magnesium
• Flu-like symptoms • Potassium
• Hypertrichosis • Blood pressure
• Gingival hypertrophy monitoring
• Skin malignancies
Acitretin • Teratogenicity • Pregnancy X
• Alopecia • Lipid panel
• Hepatotoxicity • LFTs
• Hyperlipidemia • CVC with platelets
• Mucocutaneous • Creatine
• Pseudotumor cerebri phosphokinase
• Hyperostosis
34TNF Inhibitors and Comorbidities
Drug PsO PsA Comorbidity Concerns
All TNF Untreated/latent TB,
inhibitors MS/demyelinating disease, Heart
Failure NYHA class III/IV,
active/chronic HBV or other active
infections
Adalimumab X X
Infliximab X X Also: infusion reactions, dose creep
Etanercept X X
Golimumab X
Certolizumab X
NYHA = New York Heart Association
Humira [prescribing information]. North Chicago, IL: Abbvie; 2017; Remicade [prescribing information]. Horsham, PA: 35
Janssen Biotech, Inc.; 2013; Enbrel [prescribing information]. Thousand Oaks, CA: Amgen; 2017; Simponi [prescribing
information]. Horsham, PA: Janssen Biotech, Inc.; 2011; Cimzia [prescribing information]. Smyrna, GA: UCB, Inc.; 2016.Non-TNF Agents and Comorbidities
Drug PsO PsA Comorbidity Concerns
IL-12/23 inhibitor
Ustekinumab X X Weight-based dosing and injection
frequency not optimized
IL-17 inhibitors
Secukinumab X X IBD, Candidiasis, neutropenia,
hypercholesterolemia
Ixekizumab X IBD, Candidiasis, injection site pain,
neutropenia
Brodalumab X IBD, depression/suicidal ideations
IL-23 inhibitor
Guselkumab X URI, Candidiasis, HSV
PDE-4 inhibitor
Apremilast X X Depression and suicide
36PASI Rates for Systemic Psoriasis
Therapies
PASI 75 PASI 90 PASI 100
Percent of patients achieving PASI
100 90
82 82
80 76
71 71
75/90/100
59 58 59
60 51
45 41
40 36 33
30 26
20 18
20 14
7
0
Methotrexate1 Etanercept2 Adalimumab3 Infliximab4 Ustekinumab 5 Secukinumab 6 Apremilast 7 Ixekizumab 8
(Week 16) (Week 24) (Week 16) (Week 24) (Week 12) (Week 12) (Week 16) (Week 12)
1. Saurat JH, et al. Br J Dermatol. 2008158:558-566; 2. Leonardi CL, et al. N Engl J Med. 2003;349:2014-2022;
3. Menter A, et al. J Am Acad Dermatol. 2008;58:106-115; 4. Reich K, et al. Lancet. 2005;366:1367-1374; 5.
Papp K, et al. Lancet. 2008;371:1675-1684; 6. Langley RG, et al. N Engl J Med. 2014;371:326-338; 7. Otezla
37
(apremilast) prescribing information. Celgene Corp. 2015; 8. UNCOVER-2 trial. Presented at the American
Academy of Dermatology annual meeting. 2016.PASI Rates for Systemic Psoriasis
Therapies in Development
1 2 3 4
(Week 12; 210 mg; Phase 3) (Week 16; 200 mg; Phase 2) (Week 16; 200 mg) (Week 12; Phase 2)
38
1. Lebwohl M, et al. N Engl J Med. 2015;373:1318-1328; 2. Gordon KB, et al. N Engl J Med. 2015;373:136-
144; 3. Papp K, et al. Br J Dermatol. 2015; 4. Papp K, et al. AAD 2015.Monitoring § Screen for TB before starting a biologic and on a yearly basis § Obtain CBC at baseline and yearly § Obtain complete metabolic panel at baseline and yearly § HBV and HCV screening at baseline and yearly § Optional HIV screen (high-risk patients/geographic areas) § While on therapy, use caution when the patient § Develops an infection § Plans to have major surgery § Plans to get a live vaccine (shingles, yellow fever, etc.) PDR.net. http://www.pdr.net/drug-information/enbrel?druglabelid=2228. Accessed March 6, 39 2015.
40
Final Thoughts
§ Detail the patient’s history…Listen and hear
their story
§ Focus on comorbidity AND lifestyle
management concurrently
§ Discuss goals of therapy
§ Choose treatment options that maximize benefit
and minimize risk
§ Spend 5 extra minutes! It may extend a psoriatic
patient’s life by 5 years
41POST-TEST QUESTIONS
42Post-test ARS Question 1
Which of the following are among the most
common symptoms of psoriatic disease?
1. Enthesitis
2. Depressed mood
3. Pruritic skin lesions
4. Symmetric joint pain and swelling
43Post-test ARS Question 2
According to a population-based study, the relative
risk for myocardial infarction is highest in which of
the following patients with psoriatic disease?
1. Older patients with severe psoriasis
2. Older patients, regardless of severity
3. Younger patients with severe psoriasis
4. Younger patients with longer duration of
disease
44Post-test ARS Question 3
63 y/o obese man, 12 yr hx psoriasis, 2 yr. hx of psoriatic
arthritis. Increased disease activity (5% BSA, mod. joint disease
activity)
Meds: topical steroids and NSAIDs. Recently underwent PCI for
unstable angina.
Which of the following might be appropriate based on this
history?
1. Avoid methotrexate based on cardiovascular risk
2. Avoid TNF inhibitors based on cardiovascular risk
3. Consider biologic therapy or PDE4 inhibitor despite his
cardiovascular risk
4. Consider phototherapy and switch from NSAID to
45
acetaminophenPost-test ARS Question 4
How confident are you in your ability to
recognize co-morbidities associated with
psoriatic disease?
1. Not at all confident
2. Slightly confident
3. Moderately confident
4. Pretty much confident
5. Very confident
46Post-test ARS Question 5
How confident are you in your ability to
integrate the latest treatment data into the
management of patients with psoriatic disease?
1. Not at all confident
2. Slightly confident
3. Moderately confident
4. Pretty much confident
5. Very confident
47You can also read

















































