Gynaecology & Obstetrics - Italian Journal of (SIGO) The Official Journal of the Società Italiana di Ginecologia e Ostetricia
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Italian Journal
of
Gynaecology
& Obstetrics
The Official Journal of the
Società Italiana di Ginecologia e Ostetricia
(SIGO)
March 2016 - Vol. 28 - N. 1 - Quarterly - ISSN 2385 - 0868
Quarterly
Partner-Graf 1
Italian Journal
of
Gynaecology
& Obstetrics
The Official Journal of the
Società Italiana di Ginecologia e Ostetricia
(SIGO)
Quarterly
Partner-Graf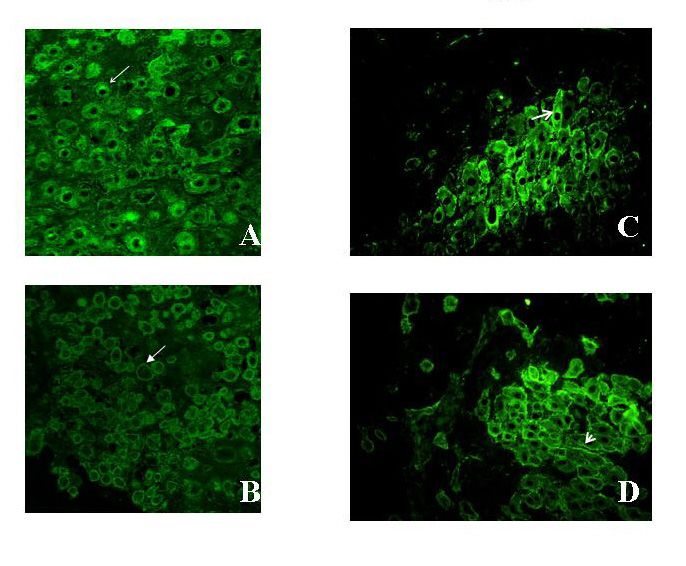
Editor in Chief Paolo Scollo, Catania Editors Herbert Valensise, Roma Enrico Vizza, Roma Editorial Board Cervigni Mauro, Roma Chiantera Vito, Napoli Costa Mauro, Genova De Stefano Cristofaro, Avellino De Vita Davide, Salerno La Sala Giovanni Battista, Reggio Emilia Locci Maria Vittoria, Napoli Marci Roberto, Roma Monni Giovanni, Cagliari Ragusa Antonio Franco, Milano Sirimarco Fabio, Napoli Trojano Vito, Bari Viora Elsa, Torino Editorial Staff Roberto Zerbinati Serena Zerbinati Management, Administrative office Partner-Graf Srl - Via F. Ferrucci, 73 - 59100 Prato Tel 0574 527949 - Fax 0574 636250 E-mail: info@partnergraf.it The Italian Journal of Gynaecology & Obstetrics is a digital magazine. You can download it freely from www.italianjournalofgynaecologyandobstetrics.com or www.italianjog.com

It. J. Gynaecol. Obstet.
2016, 28: N.1
Table of contents 5
Editorial.
Cancer and developing countries 7
Paolo Scollo
Medically Assisted Procreation: its risk in the maternal-fetal and neonatal
pathology 9
Marta Mancini, Valentina Latini, Roberta Licia Scala , Stefania Balzi, Maria Grazia Pellegrini, Mario
F. Segatore, Camilla Gizzi, Herbert Valensise
Autonomic dysfunction and flow-mediated dilation in polycystic ovary
syndrome (PCOS): a case-control study. Dysautonomia in polycistic ovary
syndrom 19
Alberto Zanella, Lucia Sarolo, Fabio Pomerri, Franca Bilora
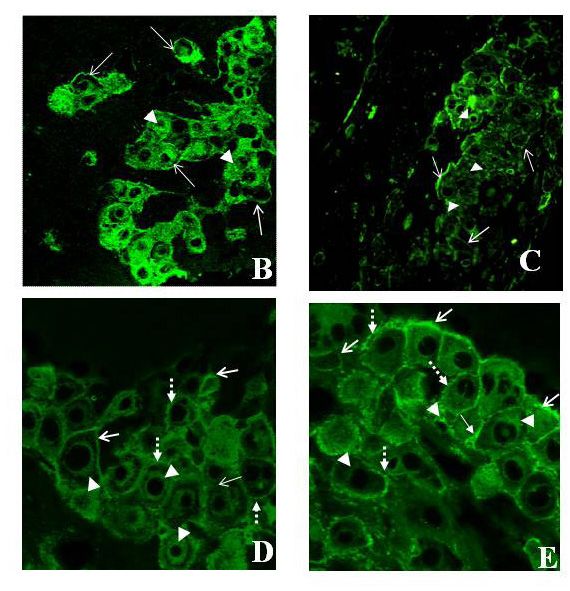
HLA-G intracellular expression in decidua trophoblasts in a normal term
placenta: a confocal and transmission electron microscopy study. 27
Barbara Chifenti, Maria T. Locci, Giuseppe Trojano, Paola Lenzi, Maria E. Filice, Pietro Bottone,
Maria G. Salerno, Lorella Battini
Knowledge and attitude of professional health workers toward human
papilloma virus (hpv) infection and vaccines. Attitude to HPV vaccine in Zaria 35
Oluwafumbi M Olajide, Abimbola O. Kolawole, Adekunle O. Oguntayo, Samuel A. Adewuyi
5

Editorial
Cancer and developing countries
Paolo Scollo
Cancer is a pressing challenge in global health that disproportionately affects developing countries:
60 per cent of the world’s total cases occur in Africa, Asia, and Central and South America, and these
regions account for about 70 per cent of the world’s cancer deaths, according to the International
Agency for Research on Cancer. Unless a shift in mindset occurs—with those committed to global health
investing more in cancer information, prevention, screening, and treatment—the number of new cancer
cases worldwide will grow from around 12 million today to 15 million in 2020, with much of that growth
occurring in developing nations. In low- and middle-income countries, the high incidence of malignant
tumors related to communicable diseases, such as the human papilloma virus (HPV), reflects a dearth
of reliable systems for disease control and screening services. By contrast, the increasing incidence of
lung, breast, and colorectal cancer is largely the result of demographic and lifestyle changes, including
longer life expectancy and accelerated urbanization, which in turn leads to reproductive patterns
(pregnancy at older ages, low prevalence of breastfeeding) and lifestyles (tobacco consumption, high
calorie intake, alcohol abuse) associated with several forms of cancer. The global health agenda remains
focused primarily on communicable diseases and the traditional identification of international health
with infectious disease control. We need, however, to adopt a more comprehensive view. According to
WHO, one-fifth of all cancers worldwide are caused by chronic infections produced by agents such as
HIV, HPV, hepatitis B virus, and Helicobacter pylori.
Cervical cancer is a consequence of a long-term infection with human papillomavirus (HPV), and
the majority of cervical cancer cases (>80%) occur in low- and middle-income countries. Cervical
cancer mortality rates have fallen in much of the developed world during the past 30 years, largely
due to screening and treatment programmes. During the same time, however, rates in most developing
countries have risen or remain unchanged, often due to limited access to health services, lack of
awareness and absence of screening and treatment programmes. Rural and poorer women living in
low- and middle-income countries, as well as poorer women living in high-income countries are at an
increased risk of invasive cervical cancer, because they often do not have access to crucial prevention,
screening and treatment services.
We have the technical knowledge to prevent hundreds of thousands of unnecessary deaths of women
worldwide. What is needed now is the strengthening of health systems to enable them to implement
what we know and give women and girls access to the services they need to stay alive.
Prof. Paolo Scollo
S.I.G.O. President
7
M E V
UT ICA
A C E O G IA
FARM INECOL
IN G LA NATURA CHE AIUTA
ClimaMEV
IncontinenzaMEV
VenaMEV
FARMACEUTICA MEV - Strada Cassia Sud, 175 - 53100 Siena (SI)
Tel. 0577 378091/ Fax 0577 379970 - www.farmaceutica-mev.itItalian Journal of
Gynaecology & Obstetrics
March 2016 - Vol. 28 - N. 1 - Quarterly - ISSN 2385 - 0868
Medically Assisted Procreation: its risk in the maternal-fetal and
neonatal pathology
Marta Mancini 1,4, Valentina Latini 1,2, Roberta Licia Scala 1, Stefania Balzi 1, Maria Grazia
Pellegrini 1, Mario F. Segatore 1, Camilla Gizzi 3, Herbert Valensise 1,4
1
Department of Obstetrics and Gynecology Ospedale Fatebenefratelli Isola Tiberina Rome Italy.
2
School of Emergency, Seconda Università degli Studi di Napoli, Italy.
3
Department of Neonatology Ospedale Fatebenefratelli Isola Tiberina Rome Italy.
4
Department of Biomedicina Section of Obstetrics and Gynecology Tor Vergata Univeristy Rome Italy.
ABSTRACT SOMMARIO
The increase of the Medically Assisted Procreation is due L’incremento delle procedure di Procreazione
to the effort that the research has made to improve the Medicalmente Assistita (PMA) è dovuto allo sforzo
techniques, but its effect on the maternal outcome and che la ricerca ha fatto per migliorarne le tecniche, pur
neonatal outcome has not been fully studied. Therefore, non valutandone gli effetti sull’outcome materno e
our study has focussed on a population of pregnant neonatale. A riguardo Il nostro studio ha preso in
women hospitalised in the obstetrical pathology unit esame una popolazione di donne gravide che sono
at the S. Giovanni Calibita Fatebenefratelli hospital in state ricoverate nel reparto di patologia ostetrica
Rome in the year 2013. dell’ospedale Fatebenefratelli S. Giovanni Calibita Isola
First of all, we have made a distinction between the Tiberina (Rm) nel corso dell’anno 2013.
women who have undergone an assisted reproductive Per prima cosa si è suddivisa la popolazione
technology (ART) and those in a spontaneous pregnancy rispettivamente in donne che si sono sottoposte a PMA e
and, successively, for each of them, we have evaluated donne che hanno concepito spontaneamente. In seguito,
the clinical history, the reason for admission, the course per ognuna, sono stati valutati i seguenti elementi: la
of the pregnancy, the outcome of childbirth and the storia clinica, il motivo del ricovero, il decorso della
clinical condition of the newborn. This work emphasises gravidanza, gli esiti del parto e le condizioni cliniche
the common profile of the woman who underwent del nascituro.
ART: multiple pregnancy, advanced maternal age, Lo studio ha messo in evidenza caratteristiche
chronic diseases such as hypertension, hospitalisation comuni e ricorrenti nelle donne che si sono sottoposte
for cervical incompetence and threats of preterm birth, a PMA: prevalenza di gravidanza gemellare, età
preterm birth, caesarean section, premature babies with materna avanzata, patologie croniche materne come
necessity of a recovery in intensive and sub intensive l’ipertensione, ricoveri per incompetenza cervicale e
care, increased hospitalisation of mother and infant. minacce di parto pretermine, bambini nati pretermine,
In the future it becomes necessary to regulate the ART taglio cesareo, neonati prematuri con necessità di
by using these results increasingly, both to select the ricoveri in terapia intensiva e sub-intensiva, aumento
patients and to choose the methods of prophylaxis and delle degenze della madre e del neonato. Pertanto
prevention of complications. in futuro risulta necessario regolamentare la PMA
utilizzando maggiormente questi risultati sia per
selezionare le pazienti sia per scegliere metodiche di
Keywords: medically assisted procreation; maternal profilassi e prevenzione delle complicanze.
outcome; neonatal outcome; assisted reproductive
technology; multiple pregnancy; advanced maternal age;
preterm birth; premature babies.
Correspondence to: man_marta@hotmail.it
Copyright 2015, Partner-Graf srl, Prato
DOI: 10.14660/2385-0868-31 9It. J. Gynaecol. Obstet. Medically Assisted Procreation: its risk in the maternal-fetal and neonatal pathology
2016, 28: N.1
INTRODUCTION derive a nosographic number of the patients, from
At all ages and in all societies infertility has which we have traced telematically their own
constituted a major health problem, mainly Personal Codes and, as a consequence, the clinical
related to the negative effects that longevity and records each of them had collected, reaching a total
environmental pollution have on the fertility of of about 549 folders consulted. Moreover, through
couples(1). As a result, the demand for medical the folder of the woman giving birth, we have
care is growing accordingly, as demonstrated traced the Personal Code and the medical record
by the wide variety of supporting treatments to of the newborn, from which we have derived data
alleviate infertility, such as an improvement of for a total of about 306 pediatric folders consulted,
the in vitro fertilization technique and a growing taking into account that for some children it
availability of oocyte donation techniques(2). The was possible to obtain information only from
medically assisted procreation has indeed become the “Born” paper Record books, stored in the
available to a wider population allowing for Neonatology hospital.
greater knowledge about both its techniques and The elaboration of the results was based upon
the problem of infertility itself. The increase of the separation of two classes of the population, 70
“artificial” pregnancies go on over time soliciting a of which have undergone the ART (19,83%) and
series of important repercussions from the clinical 283 have not undergone the ART (80,27%). Starting
point of view and for what concerns the healthcare from this division (Patients ART and Patients non
and the clinical expenses. The factors that can ART) the Neonatal Populations were derived: a
determine a favourable or unfavourable evolution total of 344 babies born alive, 94 of which born
of the gestation, independent from the technical from the Pts ART (27,32%) and 250 born from
ability of the biologists in the reproduction, are the Pts non ART (72,68%). For each population a
increased maternal age(3), the gestational ability of study was drafted taking into consideration the
a less elastic uterus(4), the frequency of multiple several variables that could be analysed. For what
pregnancies(5), the starting organic conditions of concerns the maternal population, the following
the mother are among. To this day, it is therefore data were taken into account: maternal age;
necessary to carefully observe the quality of the hypertensive diseases; threat of preterm birth;
pregnancies obtained via the assisted reproductive gestational age; type of pregnancy; number of
technology (ART) referring to the maternal-fetal hospitalisations for patient and total days of
and neonatal outcome. So we have conducted hospitalisation; mode of delivery. For the neonatal
a perspectival study during a calendar year population: neonatal anthropometric evaluation;
evaluating the effect of the ART recoveries against birth pathologies; internal transfers or transfers
non ART recoveries in the obstetrician pathology to other hospitals; days of hospitalisation of
division of the Fatebenefratelli hospital in Rome. infants. Each subgroup was then uniformed with
We have classified the patients progressively quantitative measures accurately calculated and
hospitalised for problems developed during their represented both by the absolute values and by
pregnancy, taking into consideration the main measures proportional to the total percentage of
diagnosis that had prompted their hospitalisation the reference populations and/or the percentage
and following the therapeutic process and of the total of each qualitative variable.
neonatal outcomes.
RESULTS
SUBJECTS AND METHODS From our study were derived results divided
The experimental study was conducted in the by maternal population, neonatal population and,
obstetrician pathology division of the S. Giovanni finally, public health considerations regarding
Calibita Fatebenefratelli hospital in Rome, in both populations.
agreement with the Tor Vergata University of Maternal population
Rome. In the period January-December 2013, 353 Maternal age was divided into intervals of five
women were selected after being hospitalised due years, except for the age groups of less than twenty
to a pathology arisen during their pregnancy. years. From this we have obtained the descriptive
Each woman has been hospitalised at least once statistics: those women who had chosen ART
during the time span. Patients have been followed have an average age of 38,68 and the modal class
longitudinally along pregnancy and their maternal between 35 and 39 years old (30%) is the one with
and neonatal outcome recorded for final analysis. a largest number of pregnant women. The non
Specifically, the Record book has allowed us to ART women, on the other hand, have an average
10Medically Assisted Procreation: its risk in the maternal-fetal and neonatal pathology M. Mancini et al.
of 33,38 years and the modal class in which the between 30 and 34 years old (36,04%).
highest number of pregnancies concentrates is
Table 1.
Division of the maternal age-by-age groups and the maternal
population into patients who have or not undergone ART.
By subdividing the pregnancy into single and
multiple, hence bigeminal and trigeminal, we
derive that 52,86% of the pregnancies of the Pts
ART are unique, while 47,14% are multiple (40%
bigeminal and 7,14% trigeminal). Among the
women who have not undergone ART, on the
contrary, the percentages vary considerably:
92,58% of the pregnancies are single, while
7,42% are multiple (7,07% bigeminal and 0,35%
trigeminal). If we observe the same data within the
total population of patients, there is an absolute
prevalence of the single pregnancy. In the Pts non
Figure 1. ART, that is 74,22% against the 10,48% of the Pts
Descriptive histogram of the maternal age groups in which the
highest distribution of the Pts ART is evidenced in the groups of
ART and a clear predominance of the multiple
more advanced age, mostly 35 years or older, compared with the pregnancy in the Pts ART, that is 9,35% (7,93% B;
Pts non ART that are distributed more around 34 years of age or 1,42% T), compared to the 5,95% (5,67% B; 0,28%
younger. T) in the Pts non ART.
Table 2.
Data collection per kind of pregnancy on the population of patients
who have undergone ART or not have.
Figure 2.
Distribution of each maternal population, which is Pts ART and Pts
non ART, within the subdivision of the pregnancy into single and
multiple, in turn bigeminal and trigeminal.
11It. J. Gynaecol. Obstet. Medically Assisted Procreation: its risk in the maternal-fetal and neonatal pathology
2016, 28: N.1
In this study we have observed the
pathological conditions occurred during these
pregnancies, more precisely we have focussed on
the hypertension, both chronic and gestational, in
the 20% of the Pts ART compared to the 10,6% of
the Pts non ART.
Figure 4.
Graphic representation of the results presented in the table. Notice
the high frequency of preterm birth threats both in the Pts ART
and in the non ART. On the other hand, cervical incompetence and
premature PROM are evidently more frequent among the Pts ART.
The gestational age was subdivided into
intervals, mainly respecting the concepts of
Figure 3. term pregnancy and pre-term pregnancy. The
In the evaluation of the pathological conditions of the mother we gestational age of the Pts ART was distributed
have taken into account the hypertensive disease. The results
are referred to the following pathologies: chronic and gestational among 62,5%, where we have it between the 32nd
hypertension, preeclampsia, eclampsia and HELLP. The distribution and 36th week +6 days and for a 23,21% over
of the hypertensive pathology evidences its higher impact in the the 37th week. Viceversa, the distribution of the
group of the Pts ART. gestational period in the Pts non ART: 53,95% of
them has a term pregnancy, while 29,82% has a
pregnancy between the 32nd and 36th week +6
In the same way, we have considered the cases days.
of threatened preterm delivery (TPT), of cervical
incompetence (CI) and of premature membranes Table 4.
rupture (PROM) and preterm PROM (pPROM). Subdivision of the gestational age of the patients, both ART and non
ART, in intervals that consider the term and pre-term pregnancy.
On the whole, we can see how the threatened
of preterm births is more frequent in the women
who have a spontaneous pregnancy (35,69% in
Pts non ART; 30% in Pts ART). But, if we consider
their highest number, among the Pts ART we find
a higher prevalence of CI and pPROM, that is
34,28% in the first and 10% in the latter, compared
to 16,96% in the first and 5,65% in the latter in the
case of the Pts non ART. On the other hand, among
the Pts non ART there is a higher prevalence of
PROM, that is 10,25% compared to 8,57% in the
Pts ART.
Table 3.
In the maternal population were collected data on those cases where
the pathology arises during the pregnancy. We have taken into
account, for both the Pts ART and non ART, threatened preterm
delivery (TPT), cervical incompetence (CI), premature membranes
rupture (PROM) and preterm PROM (pPROM).
Figure 5.
Representation of the distribution of the patients, ART and non
ART, in intervals of gestational age. The pregnancies in the Pts
ART are distributed mainly in 36 weeks +6 days, the pregnancies of
12 the Pts non ART go to term.Medically Assisted Procreation: its risk in the maternal-fetal and neonatal pathology M. Mancini et al.
Completed pregnancies were divided per type of Table 5.
delivery: spontaneous, operative and caesarean The relationship between gestational age and birth weight of the
infants allow us to distribute them into small for gestational
section. Overall, the caesarean prevails and it is age (SGA), appropriate for gestational age (AGA) and large for
configured in 85,96% of deliveries in the Pts ART gestational age (LGA). To do this we have made use of the new
and in 63,60% of the Pts non ART. Italian Neonatal Anthropometric Papers.
Figure 6.
Graphic distribution of the type of delivery, that is spontaneous
or vaginal operative, and caesarean section. Percentage values of
the type of delivery made by the patients and considered both with
respect to the total in each group, Pts ART or Pts non ART, and to
the total of the maternal population. In both populations, Pts ART
and Pts non ART, the caesarean prevails.
Figure 7.
The newborn appropriate for the gestational age represent the
majority of babies born from ART and non ART. The small newborn
Neonatal population for gestational age are of a higher number when born from ART. The
First of all, we have considered if a newborn is large newborn for gestational age are of a higher number when not
or not appropriate for the gestational age by using born from ART.
the new Italian Neonatal Anthropometric Papers,
realised with participation from 34 Neonatology
centres within the Italian Neonatal Study (INeS).
The consultation of the clinical records of the
The newborn have then been classified in small for
newborn babies has showed various pathological
gestational age (SGA), appropriate for gestational
cases, according to which the newborn have
age (AGA) or large for gestational age (LGA). The
been classified into healthy and sick, also taking
results have shown that the infants are mainly
into account the prematurity and the respiratory
distributed in the AGA class in both populations
distress syndrome. The children born ill from ART
(80,35% for those born from ART; 87,20% for those
represent the 75,53% of this population, 61,70% of
not born from ART), but there are differences in
which is premature and 29,79% has got RDS, while
the other two classes SGA and LGA. Those born
the healthy are just 24,47%. The children not born
from ART have a higher distribution within the
from ART present a higher percentage of health
SGA class (17,02% on a total of children born
than the previous ones, that is 52,80% and, among
from ART), compared to those not born from ART
the sick ones, not born from ART, the 31,20% is
(9,60% on a total of children not born from ART).
premature and the 19,20% has got RDS.
On the contrary, those not born from ART have
a higher distribution within the LGA class 3,20%
idem) compared to those born from ART (2,13%
idem).
13It. J. Gynaecol. Obstet. Medically Assisted Procreation: its risk in the maternal-fetal and neonatal pathology
2016, 28: N.1
Table 6. Table 7.
In the evaluation of the pathological conditions of the newborn Distribution of the ill children within the intensive therapy unit
we have taken into account eight subgroups: prematurity (Pm); (ITU), sub-intensive therapy unit (Sub-ITU), neonatal pathology
respiratory distress syndrome (RDS); malformations (M); jaundice unit (NPU) or other hospitals.
(J); anemia (A); hemorrahage (H); coagulopathy (C); infections (Inf).
Figure 8. Figure 9.
The graphical representation distributes the subgroups of the Those born from ART are distributed mostly in the intensive (ITU)
pathologies and highlights the predominance of sick infants, and sub-intensive therapy units (Sub-ITU). Those not born from
premature (Pm) and with respiratory distress syndrome (RDS), ART are mainly distributed in the neonatal pathology unit (NPU)
among those born from ART. or are transferred to another hospital.
Considerations of Public Health
Through the medical records, we were able
Moreover, the children born with problems to calculate the days of hospitalisation of both
during birth or during the pregnancy have been the mothers and the infants. The Pts ART have
moved into other divisions in the same hospital, a lower number of hospitalisation compared to
such as intensive and sub-intensive therapy, and the Pts non ART but, at the same time, the days
in other hospitals, due to saturation problems or of hospitalisation of the former are greater than
because of in need of paediatric surgery. Being the those of the other. The average of admissions and
total 344, 142 of them has required neonatologic days of hospitalisation in the Pts ART is 10,09,
assistance (41,28% of the total of the newborn compared to 9,54 in the Pts non ART, with a
babies) and of these 66 were born via ART (19,19% history of hospitalisation higher than 87 days in
on a total of the newborn), while 76 were not born the first group, compared to 69 days in the second
from ART (22,09% of the total of the newborn). group.
In particular, those born from ART are mainly
distributed in the II level functional units of the
Table 8.
hospital object of study (17,61% in Sub-TIN and
Collection of the hospitalisation’s number and of the total days
13,38% in TIN). While, those not born from ART of hospitalisation for the patients, both ART and non ART.
are mostly concentrated in the I level functional Resulting evaluation of the average number of days and number of
unit in the same hospital (26,06% in the neonatal hospitalisations.
pathology division) and another good part
were transferred to another hospital (14,08%).
14Medically Assisted Procreation: its risk in the maternal-fetal and neonatal pathology M. Mancini et al.
Figure 10. Figure 11.
Graphic representation of the tabulated values. As we can see, the Graphic representation of the tabulated values. We can see how,
Pts ART have a lower number of hospitalisations compared to the starting from the days of hospitalisation and the number of patients,
Pts non ART, but the hospitalisation per se has a duration in terms the children born from ART have on average a higher number of
of days higher than the patients who have not undergone ART. days of hospitalisation compared to those not born from ART.
In the population born from ART, constituted
DISCUSSION
by 94 components, we have 1541 days of recovery,
In Italy, from an ethical, legal and medical point
mainly collected by those born from multiple
of view, the Medically Assisted Procreation is a
pregnancies. Just think that there are 5/3 born in
topic more relevant that ever for the increase in the
this population and the days of hospitalisation
number of women who undergo the insemination
accumulated by them only is 149. Among those
techniques. This stems especially from the increase
born not from ART, 250 babies, we have 1933 days
in pregnancies for women over forty years of age
of recovery, mainly derived from the firstborn
in western countries, due to economic and social
(more numerous of the first population). The
reasons related to study and career choices.
description of the neonatal wards can be summed
In our research the women of advanced age
up in the following equations:
represent the majority of those who underwent
•71 NoP: 1541 days = 1 NoP: 21,27 days (no.1)
the medically assisted procreation, while women
•118 NoP :1933 days = 1 NoP: 16,38 days (no.2)
with spontaneous pregnancies slightly exceed the
In the equation no.1 is evidenced not only the
threshold of forty years of age. Given that the index
number of patients (NoP), born from ART, 71 of a
of fertility diminishes with the increasing age of
total of 94 children, but also that each one of them
the woman, the postponement of the pregnancy
has on average 21,27 days of hospitalisation.
has become a problem in the reproductive health
In the equation no.2 is on the contrary
and this could explain the consistent use of the
evidenced the number of patients, born not from
procreation in these age groups and, recently,
ART, that is 118 of a total of 250 children, and
this trend has been fostered by the development
each one of them has an average of 16,38 days of
of the egg donation techniques, that offer higher
hospitalisation.
chances of success for those women who carry
them out in menopausal and postmenopausal
periods. However, we should not create an axiom
Table 9. between the state of sub-fertility in a woman of
Collection of the total days of hospitalisation for children and their
number (NoP), both born from ART and not. Resulting evaluation advanced age and the use of the medically assisted
of the average days of hospitalisation and number of patients. procreation, because an increased maternal age can
also increase complications during pregnancy(6).
Procreation has mainly had, in the last few
years, an important role in increasing the incidence
of multiple pregnancies. The population observed
in the course of this study facilitates the emergence
of a high percentage of these, among the Pts ART, 15It. J. Gynaecol. Obstet. Medically Assisted Procreation: its risk in the maternal-fetal and neonatal pathology
2016, 28: N.1
in which the 50% is of a twin kind, and this result birth, RDS, malformations, bronchopulmonary
highlights the association between the number dysplasia, anemia, jaundice and infections. But
of twin pregnancies and the advanced age of the the advanced age affects the preterm births, also
patients. We, in fact, know that the age factor conditions at risk for women in this period of their
reduces the efficiency of the medically assisted life, such as NCDs (hypertension and diabetes)
procreative technique and, as a consequence, that, presenting themselves as threats during the
induces to a transfer of at least three embryos pregnancy, can induce women to choose between
in the uterus to guarantee its success(7). The the chance of an induced preterm birth or the
complications associated to multiple pregnancies possibility of an urgent delivery.
and their cost have caused a reshaping of this All this is exacerbated by the fact that the
trend through the concept of the transfer of a Pts ART, as we have seen, have with a higher
single embryo. frequency a multiple pregnancy and, as a
Yet, we shall not lose sight of the reasons for consequence, to sustain the growth of a uterus
the recovery in the obstetrician pathology that containing more foetuses reduces its chances
are often connected to very serious complications of growth compared to a single foetus and it
and are not made irrelevant by the choice of a induces earlier break of the membranes due to a
non-spontaneous pregnancy. We shall consider, mechanical stress of the wall because of a higher
for example, the chapter on the hypertensive distension of the uterus in a multiple pregnancy.
disease that is present not only in the 12,47% of The data regarding the high prevalence of
the population under study, but especially among premature babies born from ART explains their
the patients who have undergone an assisted higher hospitalisation and the need they have
procreation. The women belonging to this group of a more proper healthcare. These newborn are
are older than 35 years, however, as we have especially hospitalised in Sub-TIN and TIN, so
seen, they are more inclined to an increase of the there is an obvious difficulty in the neo family
risk factors, among which chronic diseases and that cannot go back home “with the baby in their
complications for the newborn, such as preterm arms”. This difficulty is even worse when the baby
birth (gestational ageMedically Assisted Procreation: its risk in the maternal-fetal and neonatal pathology M. Mancini et al.
It was relevant to note how it is the Pts ART estimate the days accumulated by each newborn
themselves that accumulate more days in hospital, baby, considering the fact that he/she is an only
while the Pts non ART accumulate a higher child or first-born, second-born and/or third-born
number of hospitalisations. These results expose in a multiple pregnancy, the third-born are those
a conduct that presents more certainty in knowing who accumulate more days.
the risks connected with pregnancies obtained In summary, the largest number of multiple
through ART, since most of the women who pregnancies among the women who have
undergo ART have risk factors already known, undergone ART (triplet deliveries in particular)
such as advanced age and multiple pregnancies. and the largest number of preterm births give
Moreover, if we consider that in the obstetrical account of the conspicuous duration of the
pathology divisions the number of beds is neonatal hospitalisation. The costs are high on this
limited, the 20% of Pts ART hospitalised at the front as well, not just considering the direct health
San Giovanni Calibita Fatebenefratelli hospital in expenses, but also for the healthcare commitment,
Rome becomes a conspicuous percentage if related both global and at a distance.
to their long-term care compared to a woman with It is therefore important to have a regulation of
spontaneous pregnancy in the same division. the Medically Assisted Procreation that can allow
It is easy to imagine how this affects the health for a selection of the patients to be subjected to this
expenditure and the availability of beds. treatment, taking into account the repercussions
The same can be said about the neonatal there can be upon the national healthcare system.
sphere, where notwithstanding the undeniable As a matter of fact, a methodology applied
progress made and the success achieved in the irrationally and with no selective criteria generates
maternal-neonatal area, the prevalence of the consequences on the cost of hospitalisation and on
preterm births does not show any sign towards a the health of both patients and newborn babies.
reduction of the time, also due to the emergence of In the future a greater use of these results will
the new gravid conditions described above. In our allow us to evaluate the efficacy in the selection of
job the number of preterm births and the number the patients, the possible methods of prophylaxis
of hospitalisations are higher than the pregnancies and the prevention of the complications.
due to medically assisted procreation. Is we
REFERENCES
1) Ehrlich S. Effect of fertility and infertility on longevity. 5) Scholten I, Chambers GM, van Loendersloot L, van der
American Society for Reproductive Medicine. Fertil Steril. Veen F, Repping S, Gianotten J, Hompes PG, Ledger W,
2015 May; 103 (5):1129-35. Mol BW. Impact of assisted reproductive technology on
2) Benagiano G, Filippi V, Sgargi S, Gianaroli L. Italian the incidence of multiple-gestation infants: a population
Constitutional Court removes the prohibition on gamete perspective. American Society for Reproductive Medicine,
donation in Italy. Reproductive Healthcare Ltd, 2014 Dec; 2015 Jan; 103(1):179-83.
29(6):662-4. 6) Laopaiboon M, Lumbiganon P, Intarut N, Mori R,
3) Sauer MV. Reproduction at an advanced maternal age Ganchimeg T, Vogel JP, Souza JP, Gülmezoglu AM;
and maternal health. American Society for Reproductive WHO Multicountry Survey on Maternal Newborn
Medicine. Fertil Steril. 2015 May; 103(5): 1136-43. Health Research Network. Advanced maternal age and
4) Elmes M, Szyszka A, Pauliat C, Clifford B, Daniel Z, pregnancy outcomes: a multicountry assessment. BJOG.
Cheng Z, Wathes C, McMullen S. Maternal age effects on 2014 Mar;121 Suppl 1:49-56. doi: 10.1111/1471-0528.12659.
myometrial expression of contractile proteins, uterine 7) Gleicher N, Kushnir VA, Barad D. Fertility Treatments
gene expression, and contractile activity during labor and Multiple Births in the United States. N engl j med 370;
in the rat. Physiological Reports published by Wiley 11 nejm.org march 13, 2014
Periodicals, 2015 Apr;3(4).
1718
Italian Journal of
Gynaecology & Obstetrics
March 2016 - Vol. 28 - N. 1 - Quarterly - ISSN 2385 - 0868
Autonomic dysfunction and flow-mediated dilation in polycystic ovary
syndrome (PCOS): a case-control study.
Dysautonomia in polycistic ovary syndrome
Alberto Zanella1, Lucia Sarolo1, Fabio Pomerri2, Franca Bilora1
1
Clinica Medica II - Università di Padova, Italy
2
Dipartimento di Medicina – DIMED, Università di Padova, Padova, Italy
ABSTRACT SOMMARIO
Aim: a case-control study was conducted on women Scopo: studio caso-controllo su donne affette da sindrome
with polycystic ovary syndrome (PCOS) with a view dell’ovaio policistico (PCOS) al fine di evidenziare
to identifying endothelial and autonomic nervous alterazioni endoteliali e/o autonomiche in grado di
system dysfunctions capable of explaining the higher spiegare l’alto rischio cardiovascolare riscontrato in
cardiovascular risk associated with PCOS. queste pazienti.
Material and methods: 35 women (mean age 26.51 ±3; Materiali e Metodi: sono state esaminate 35 donne (età
BMI 24.25 ±1.65) with documented PCOS and 35 controls media 26.51± 3 anni; BMI 24.25 ± 1.65) affette da PCOS
matched for age, BMI and cardiovascular risk factors were e 35 controlli appaiati per età, BMI e fattori di rischio
studied during a solar year. cardiovascolari durante un intero anno solare.
Endothelial dysfunction was assessed using flow-mediated La disfunzione endoteliale è stata valutata mediante la
dilation (FMD) and early atherosclerosis from the intima flow-mediated dilation (FMD) e l’arterioscleorosi precoce
media thickness (IMT) of the carotid district measured mediante lo studio dello dell’intima-media thickness
using eco-color Doppler. Autonomic dysfunction was (IMT) mediante eco-color-Doppler delle arterie carotidi.
assessed with the classic tests (tilt, lying-to-standing, deep La disfunzione autonomica (AD) è stata valutata mediante
breath, Valsalva, Stroop). i seguenti test: tilt, lying to standing, deep breath, Valsalva,
Results: by comparison with controls, patients with PCOS Stroop.
had an altered response in some of the autonomic tests, Risultati: nel confronto con i controlli, le pazienti con PCOS
i.e. lying-to-standing (mean values 3.25 ±4 mmHg vs -3.4 hanno presentato un’alterata risposta nei test autonomici
±2.04, pIt. J. Gynaecol. Obstet. Autonomic dysfunction and flow-mediated dilation in PCOS
2016, 28: N.1
INTRODUCTION AIM OF THE STUDY
Polycystic ovary syndrome (PCOS) is a To identify any endothelial dysfunction and
metabolic syndrome of uncertain etiology that autonomic variations in a sample of PCOS patients
affects young women. It is characterized by paired with healthy controls, and to see if this
anovulation, hyperandrogenism and insulin syndrome poses a cardiovascular risk per se, and
resistance, and is often associated with obesity, whether PCOS cardiovascular risk correlates with
hypertension, hypercholesterolemia, diabetes and the patient’s autonomic dysfunction.
metabolic syndrome (33-47%)(1). Women with
PCOS carry a higher risk of cardiovascular disease
than healthy controls. The question is whether SUBJECTS AND METHODS
PCOS represents a cardiovascular risk per se or Thirty-five women with PCOS according
whether this increased cardiovascular risk in to the Rotterdam criteria(18) referring to the
PCOS patients is associated with other factors. Endocrinology Clinic at Padua University were
Some authors have suggested that the greater paired with 35 controls (nnPCOS) recruited from
risk of cardiovascular disease in PCOS patients the II Medical Clinic at Padua University during
is unrelated to any obesity, hypertension or the course of a solar year 2012. Any women
diabetes(2), and another study found that this with cardiovascular, immunological, or other
higher risk (55% of increased risk) persisted after endocrinological disorders, neoplasms, liver
correcting results for age and obesity(3). Diastolic disease or pregnancy were ruled out.
dysfunction, ejection fraction abnormalities and The control group was paired for age, sex, BMI
inflammatory states are generally considered and cardiovascular risk factors (Table 1).
responsible for the extra cardiovascular risk. We considered women with a BMI >2530Autonomic dysfunction and flow-mediated dilation in PCOS A. Zanella et al.
AUTONOMIC ASSESSMENT “white” was written in grey, and so on). This test
Participants underwent cardiovascular is a mental stressor and blood pressure and heart
autonomic nerve function tests(20) in the following rate should rise in normal subjects at the end of
order: deep breath, Valsalva, isometric hand grip, the test(24).
lying-to-standing, tilt and Stroop.
The deep breath test measures vagal heart
rate control(21). The duration of the expiratory FLOW-MEDIATED DILATION AND
and inspiratory breaths was 5 seconds each, for a INTIMA MEDIA THICKNESS
total of 40 seconds (4 breathing cycles). The ratio Cases and controls meeting the inclusion/
of the longest to the shortest respiratory rate (RR) exclusion criteria underwent
interval was measured from the ECG for each ultrasound assessment of the arterial system
breathing cycle, and the mean of all four ratios (carotid and brachial arteries). The test was
was taken as the expiratory/inspiratory (E/I) performed with an Esaote Technos instrument
ratio. The RR was measured using a chronograph. (Tokyo, Japan) and a 7.5 MHZ probe for B-mode
The Valsalva test measures both echography, and a 6 MHz probe for pulsed
parasympathetic and sympathetic function. Doppler.
Participants blew into a manometer to maintain an The carotid arteries were assessed first, with
intrathoracic pressure of 40 mmHg for 15 seconds. patients lying on the couch with their neck rotated
The ratio between the shortest RR interval through 45°. The examiner sat by the patient’s
during the expiratory effort and the longest RR shoulder. All the arteries examined (common,
interval during the subsequent 20 seconds (the bifurcation, internal and external) were divided
Valsalva ratio) was calculated. The RR interval into three segments (inferior, medial and superior)
was measured on the ECG printout, while blood with an angle of incidence of 60°.
pressure was assessed using an automated The brachial artery was studied in the
sphygmomanometer identical to the one used at antecubital fossa.
our Critical Care Unit. An ultrasound technician completed the
In the isometric hand grip test, participants tests, which were all videotaped and reassessed
squeezed a dynamometer in their dominant hand by another ultrasound technician for validation
for 3 minutes using a force corresponding to 30% purposes. In cases of discrepancy, the videotapes
of their maximal squeezing force. Heart rate and were further examined blindly by a senior expert.
blood pressure were measured at rest, and again Atherosclerotic plaque was defined as a
before and after squeezing the dynamometer. protrusion into the vessel lumen of at least 2
In the lying-to-standing test, participants stood mm, as measured from the border between the
up suddenly after lying quietly in a supine position adventitial and medial layers(25). Stenosis due to
for 5 minutes. Heart rate and blood pressure were atherosclerotic plaque was classified according
measured at rest and then 1, 3, 5 and 7 minutes to the NASCET study(26) as follows: class 1 (an
after standing up(22). obstruction from 0 to 30%), class 2 (from 31 to
In the tilt test, participants lay supine on an 50%), class 3 (from 51 to 69%), class 4 (from 70
electric tilting table. A restraining strap across the to 99%) and class 5 (complete obstruction). IMT
upper abdomen secured them to the table during was measured at preset levels and expressed in
the test, applying a negligible pressure to the millimeters. The method for measuring IMT was
surface of the body. Blood pressure recordings and based on the principle of “two parallel echogenic
ECGs were obtained continuously throughout the lines”(27). Only images with the characteristic
test, which lasted 30 minutes and the result was double-line arterial pattern were transferred to the
judged to be positive for autonomic dysfunction computer by the sonographer.
only in the event of symptoms fully reproducing After digitalization to obtain 640 x 580 peak
the patient’s original pre-syncopal or syncopal cells with 256 gray levels, images were stored in
symptoms accompanied by arterial hypotension a memory mass system and analyzed off-line.
or bradycardia, or both(23). The highest of the values for each arterial system
In the Stroop test, the women were asked investigated (carotid and brachial) was recorded.
to read the name of 7 colors written on a sheet
of paper as fast as they could while lying on a
couch. The names of the colors were written using FLOW-MEDIATED DILATION
different colors from those they named (e.g. the We studied endothelial function by measuring
word “green” was written in yellow, the word independent endothelial vasodilation in the 21It. J. Gynaecol. Obstet. Autonomic dysfunction and flow-mediated dilation in PCOS
2016, 28: N.1
forearm; then we focused on the IMT of the carotid vasodilation. Longitudinal scans of the
district. brachial artery were taken continuously from
Endothelial dysfunction was assessed from 60 seconds before deflating the cuff until 120
brachial artery FMD measurements. We used seconds afterwards . After inducing the reactive
the procedures described in the Guidelines of hyperemia, arterial diameter was measured
the International Brachial Artery Reactivity Task between 45 and 60 seconds after deflating the
Force(27). We chose to test the brachial artery of the cuff, as this is considered the period of maximal
non-dominant arm at rest to avoid any influence of response(29). Fifteen minutes later, another resting
daily activity on the vessel’s diameter and capacity scan was obtained to confirm vessel recovery.
to dilate. Vascular reactivity is influenced by many The variation in vessel diameter due to shear
factors, such as temperature, food intake, drug stress was expressed as the percentage increase in
use and sympathetic stimuli. After fasting for 12 diameter over the vessel diameter measured at rest
hours, participants were assessed at rest in a quiet (%FMD). All patients completed the procedure
room at a controlled ambient temperature. Any without any complications; most of them reported
vasoactive medication was withheld for at least a sense of warmth and “pins and needles” in their
four half-lives, wherever possible. Participants lay hand and forearm after the sudden cuff deflation;
supine with their arms in a comfortable position all such symptoms disappeared within a few
for brachial artery imaging in the longitudinal minutes.
plane 3-5 cm above the antecubital fossa. We only STATISTICAL ANALYSIS
considered the images with a clear anterior and We examined the differences between PCOS
posterior intimal interface between the lumen and and nnPCOS patients as regard autonomic test
the vessel wall (near and far walls, respectively). results, IMT, and FMD. The PCOS patients who
The skin surface was marked and the arm was smoked or had hypercholesterolemia, diabetes
kept in the same position throughout the study. mellitus, or hypertension, were paired with
First, a sphygmomanometer cuff was placed controls with the same cardiovascular risk factors.
around the forearm distally to the target artery. The statistical analysis was performed using
A baseline image was acquired to assess brachial Student’s t-test. A p valueAutonomic dysfunction and flow-mediated dilation in PCOS A. Zanella et al.
In the light of these results, we tested whether The 3 women in the overweight PCOS group
common cardiovascular risk factors could had a BMI of 25.5.
influence the autonomic tests. We would have Table 3 shows the autonomic test results by
preferred to calculate the correlation coefficient BMI and confirms the autonomic changes, despite
probability, but the homogeneous samples (75% of the small size of the sample. The Valsalva and
the PCOS patients were 15-35 years old and 91% deep breath test results were significantly reduced
of the controls were 15-40 years old) and the few in normal-weight PCOS and overweight PCOS
cases with cardiovascular risk factors obliged us to patients. The variability emerging for the obese
opt for an exam of risk group. PCOS patients is due to the small size of the
We divided the samples into three groups by sample involved. The small sample size prevented
BMI: any useful conclusions from being drawn for the
-1. normal-weight (BMI30): 18% (6 PCOS and 6
controls).
Table 3.
Autonomic tests in participants grouped by BMI.
23It. J. Gynaecol. Obstet. Autonomic dysfunction and flow-mediated dilation in PCOS
2016, 28: N.1
As for the correlations between IMT and patients had a greater reduction than controls,
FMD in the cases and controls (Table 4), PCOS and PCOS seemed to influence FMD irrespective
coincided with an increased IMT and a reduced of age. About the correlation between IMT and
FMD by comparison with the controls, but with age the study pointed out that the older PCOS
no difference in brachial artery diameter at rest patients seemed to be protected from precocious
(3.17 mm vs 3.16 mm in cases and controls, atheroscleorisis, but this result is affected by the
respectively). two women over 45 years of age.
As regards FMD and BMI (Table 5), the
Table 4.
Endothelial function in cases and controls: intima media thickness
normal-weight and overweight PCOS patients had
(IMT) and flow-mediated dilation (FMD). a lower FMD than controls, while this was not true
of the obese patients. This finding is important
because other studies have reported that FMD
variations in PCOS depended on BMI (28), but in
our sample FMD was altered in normal-weight
PCOS patients too (Table 5a). IMT was greater in
the normal-weight PCOS patients than in controls,
but not in the overweight or obese patients (Table
5b). The small size of our sample prevents us
from drawing any conclusions concerning the
Concerning the risk factors,about FMD other cardiovascular risk factors such as type 2
variations in relation to age we evidenced that diabetes,hypertension or hyperlipidemia and
FMD declines with increasing age, but the PCOS FMD or IMT.
Table 5.
(a) Flow-mediated dilation (FMD) and (b) Intima media thickness (IMT) in cases (PCOS) and controls (nnPCOS) by BMI.
a) b)
DISCUSSION AND CONCLUSIONS
PCOS is a complex syndrome and women differences in FMD between obese PCOS patients
with this disorder are at greater cardiovascular and controls, which would confirm other reports
risk. In this study, we examined two aspects indicating that PCOS per se is also important in
of the syndrome: autonomic dysfunction and endothelial dysfunction (30). Further cohort studies
endothelial dysfunction. PCOS patients have are needed to assess the influence of obesity and
endothelial alterations irrespective of their age PCOS on cardiovascular risk factors. IMT was
or BMI, and other cardiovascular risk factors are found greater in normal-weight, young PCOS
probably likewise uninvolved. FMD was found patients than in controls, but this was not true
lower in PCOS patients than in controls, even after of the obese or older women with PCOS. These
excluding obese patients perhaps with a small findings confirm that PCOS is an independent
sample . While some studies on obese women with cardiovascular risk factor.
PCOS demonstrated a correlation between obesity As for autonomic dysfunction, our study
24 and a lower FMD in their patients(30), we found no identified a sympathetic hyperactivity. The testsAutonomic dysfunction and flow-mediated dilation in PCOS A. Zanella et al.
that we conducted are very simple and have a good PCOS and cardiovascular events is unclear from
reproducibility(4). The lying-to-standing, Valsalva the literature(34,35), but our data suggest a rule of
and deep breath tests revealed an increased endothelial dysfunction in the cardiac outcome
sympathetic activity in the patients’ cardiovascular of the polycystic disease. Other factors, such as
response, which can impair cardiac function. inflammation, may contribute to cardiovascular
These results confirm the findings of other studies disease in PCOS patients(34). The importance of
conducted using different methods(5,11) and may quantifying endothelial dysfunction in PCOS
contribute to explaining the cardiovascular risk stems from the fact that it is a simple method for
in PCOS patients. Hypersympathetic activity stratifying patients by cardiovascular risk and
is known to represent a cardiovascular risk, monitoring the efficacy of therapy.
particularly relating to sudden death(31), and We might be accused of failing to assess the
sympathoexcitation may be involved in the effect of insulin on all the functions examined in
pathogenesis of PCOS(31). While we can say nothing this study. In 2009 Pieracciante considered insulin
on the link between diabetes or hypertension as a possible explanation for the hyperactive
and autonomic dysfunction due to the small size sympathetic function seen in PCOS patients(36)
of our sample, we did find evidence of smoking and recently, Goodman stressed that insuline
and hypercholesterolemia exacerbating the PCOS resistance is belived to play an intrinsic role in
patients’ worse FMD and autonomic dysfunction. the pathogenesis of PCOS .It is implicated in the
FMD and IMT may be affected by cardiovascular ovulatory dysfunction of PCOS by distrupting
risk factors(31), but in our study - and particularly the hypothalamic-pituitary-ovarian axis(37). We
in the younger PCOS patients who were not obese restricted ourselves to assessing only the classic
- the influence of cardiovascular risk factors was risk factors because of the small size of our sample.
not important (confirming other reports of FMD Further studies will be necessary to ascertain the
being unassociated with BMI or other factors(32)). link between the autonomic system, PCOS, insulin
The same can be said of IMT(32). The link between and FMD.
REFERENCES
1) Zawadski JK, Dunaif A. Diagnostic criteria for 9) Giallauria F, Palomba S, Manguso F,et al. Abnormal
polycystic ovary syndrome: towards a rational approach. heart rate recovery after maximal cardiopulmonary
In: Dunaif A, Givens JR, Haseltine FP, Merriam GR, eds. exercise stress testing in young overweight women with
Polycystic Ovary Syndrome. Boston: Blackwell Scientific polycystic ovary syndrome. Clinical Endocrinology 2008;
Publications, 377–384,1992. 68:88–93
2) Sathyapalan T. and Atkin, S. L. Recent advances in 10) Tekin G, Tekin A, Kilicarslan EB,et al. Altered
cardiovascular aspects of polycystic ovary syndrome. autonomic neural control of the cardiovascular system
European Journal of Endocrinol 2012;166(4):575–583 in patients with polycystic ovary syndrome. International
3) Jovanovic VP, Carmina, E, Lobo RA. Not all women Journal of Cardiology 2009;130:49–55
diagnosed with PCOS share the same cardiovascular risk 11) Bergmann Sverrisdóttir Y, Mogren T, Kataoka J, Janson
profiles. Fertility and Sterility 2010;94:826–832 PO,et al. Is polycystic ovary syndrome associated with
4) Tekin G, Tekin A, Kilicarslan EB et al.Altered autonomic high sympathetic nerve activity and size at birth? Am J
neural control of the cardiovascular system in patients Physiol Endocrinol Meta,b 2008;294:576-581
with polycystic ovary syndrome. International Journal of 12) Keller J, Mandala M, Casson P,et al. Endothelial
Cardiology 2008;130:49–55 dysfunction in a rat model of PCOS. Evidence of increased
5) Yildirir A, Aybar F, Kabakci G. et al.Heart rate variability vasoconstrictor prostanoid activity. Endocrinology
in young women with polycystic ovary syndrome. Annals 2011;152:4927–4936
of Noninvasive Electrocardiology 2006;11:312-316 13) Moran LJ, Huthchinson SK, Meyer C, . A comprehensive
6) Heider U, Pedal I.e Spanel-Borowski, K. Increase in assessment of endothelial function in overweight women
nerve fibers and loss of mast cells in polycystic and with and without polycystic ovary syndrome. Clinical
postmenopausal ovaries. Fertility Sterility 2001; Science 2009;116: 761–770
75: 1141–1147 14) Mather KJ, Verma S, Corenblum B, AndersonTJ.
7) Dissen GA, Lara HE, Leyton V. et al. Intraovarian Normal endothelial function despite insulin resistance
excess of nerve growth factor increases androgen in healthy women with the polycystic ovary syndrome.
secretion and disrupts estrous cyclicity in the rat. Journal of Clinical Endocrinology and Metabolism 2000;
Endocrinology2000;141:1073–1082 85:1851–1856
8) Dissen GA, Garcia-Ruda C, Paredes A et al. Excessive 15) Paradisi G, Steinberg HO, Hempfling A, et al.
ovarian production of nerve growth factor facilitates Polycystic ovary syndrome is associated with endothelial
development of cystic ovarian morphology in mice and dysfunction. Circulation 2001;103: 1410–1415
is a feature of polycystic ovarian syndrome in humans. 16) Ketel IJ, Stehouwer CD, Henry RM et al. Greater
Endocrinology 2009; arterial stiffness in polycystic ovary syndrome PCOS is
150: 2906–2914 an obesity – but not a PCOS associated phenomenon.
25It. J. Gynaecol. Obstet. Autonomic dysfunction and flow-mediated dilation in PCOS
2016, 28: N.1
Journal of Clinical Endocrinology and Metabolism 2010;95: 27) Touboul PJ, Grobbee DE , den Ruijter H. Assessment
4566–4575 of subclinical atherosclerosis by carotid intima media
17) Cussons,AJ, Watts GF , Stuckey BG. Dissociation of thickness: technical issues. European Journal of Preventive
endothelial function and arterial stiffness in nonobese Cardiology 2012;19: suppl 18-24
women with polycystic ovary syndrome (PCOS). Clinical 28) Corretti MC, Anderson TJ, Benjamin EJ, et al.
Endocrinology 2009;71: 808–814 Guidelines for the ultrasound assessment of endothelial-
18) The Rotterdam ESHRE/ASRM-sponsored PCOS dependent flow-mediated vasodilatation of the brachial
Consensus Workshop Group Revised 2003 Consensus on artery: a report of the International Brachial Artery
diagnostic criteria and long-term health risks related to Reactivity Task Force. J Am Coll Cardiol 2002;39: 257-265
polycystic ovary syndrome (PCOS). Human Reproduction 29) Shroff R, Kerchner A, Maifeld M, et al. Young obese
2004;19: 41–47 women with polycystic ovary syndrome have evidence
19) Goodman NF,Cobin RH,Futterweit W,Glueck of early coronary atherosclerosis. Journal of Clinical
JS,Legro RS,Carmina E. American Association of Clinical Endocrinology and Metabolism 2007;92:4609-4614.
Endocrinologist,American College of Endocrinology and 30) Caroli R, Fatima J, Siddiqi Z, et al. Study of early
Androgen Excess and PCOS Society Disease state clinical atherosclerosis markers in women with polycystic ovary
review:guide to the best practices in the evaluation and syndrome. Indian J.of Endocrinol and Metab2012;
treatment of polycystic ovary syndrome-Part 1. Endocr 16: 1004-1008
Pract 2015;21:1291-300. 31) Barron HV, Lesh MD. Autonomic nervous system and
20) Bannister M, Mathias CJ, eds. Autonomic Failure: a sudden cardiac death. J Am Coll Cardiol.1996;28:1053-1060
Textbook of Clinical Disorders of the Autonomic Nervous 32) Lansdown A, Rees DA. The sympathetic nervous
System. 3rd ed. Oxford, UK: Oxford University Press; 1998 system in polycystic ovary syndrome: a novel therapeutic
21) Omerbegovic M. Analysis of heart rate variability and target? Clin Endocrinol 2012;77:791-801
clinical implications. Medicinski Archiv2009;63: 102-105 33) Orio F, Palomba S, Cascella T, et al. Early impairment
22) Task Force of the European Society of Cardiology of endothelial structure and function in young normal-
and the North American Society of Pacing and weight women with polycystic ovary syndrome. Clin
Electrophysiology. Heart rate variability: standards of Endocrinol Metab 2004;89:4588–4593
measurement, physiological interpretation and clinical 34) Diamanti-Kandarakis E, Alexandraki K, Piperi C.
use. Circulation 1996;93:1043-1065 Inflammation and endothelial markers in women
23) Sutton R, Bloomfield D. Indications, methodology and with polycystic ovary syndrome. Eur J Clin Inves
classification of results of tilt table testing. Am J Cardio 2006;36:691-697
1999;84: Q 10-9 35) Paterakis TS,Diamanti-Kandarakis E. Aspects of
24) Leite JR, Seabra M de Louredes, Sartori VA, et cardiometabolic Risk in Women with Polycystic Overy
al. The video-recorded Stroop color word test as Syndrome. Curr Obes Rep 2014;3:377-86.
a new model of experimentally induced anxiety. 36) Perciaccante A. Insulin resistance as link between
Progress in Neuro-Psychopharmacology and Biological polycystic ovary syndrome and cardiovascular
Psychiatry1999;25:809-822 autonomic dysfunction. International Journal of Cardiolog
25) Salonen JT, Salonen R. Ultrasound B-mode imaging 2009;135:e78-e79.
in observational studies of atherosclerotic progression. 37) Goodman NF, Cobin RH, Futterweit W, Glueck JS,
Circulation 1993;87:II-56-II-65 Legro RS, Carmina E. American Association of Clinical
26) Carpenter JP, Lexa FJ, Davis JT, et al. Determination Endocrinologist ,American College of Endocrinology and
of duplex Doppler ultrasound criteria appropriate to the Androgen Excess and PCOS Society Disease state clinical
North American Symptomatic Carotid Endoarteriectomy review:guide to the best practices in the evaluation and
Trial (NASCET). Stroke 1996;27,695-699. treatment of polycistic ovary syndorme - Part.2.
Endocr Pract 2015;21:1415-26
26You can also read