Hepatitis C Therapeutika - Opinion-Leader-Meeting: Therapeutische Innovationen und neue Industrie-Akademia Kooperationsmodelle - DGIM
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Hepatitis C Therapeutika
Opinion-Leader-Meeting: Therapeutische Innovationen und neue
Industrie-Akademia Kooperationsmodelle
Schloss Löwenstein, Kleinheubach, 24.-25. Januar 2020
Univ.-Prof. Dr. Stefan Zeuzem
Universitätsklinikum Frankfurt a.M.
Disclosures • Advisory boards: AbbVie, Allergan, Bristol-Myers Squibb, Gilead Sciences, Intercept, Janssen, Merck Sharp & Dohme/MSD • Speaker: AbbVie, Gilead Sciences, Merck Sharp & Dohme/MSD

Epidemiology and Natural Course of Disease
Global burden of HCV
• Estimated that 80 million people are living with chronic HCV worldwide
Viraemic prevalence
0.00–
HCV Disease Progression
Spontaneously
Acute Hepatitis
Cured
Chronic Hepatitis – Chronic Hepatitis – Chronic Hepatitis – Chronic Hepatitis – Compensated
F0 F1 F2 F3 Cirrhosis
Hepatocellular Decompensated
Carcinoma Cirrhosis
Liver Related Liver
Death Transplantation
Razavi H, Waked I, Sarrazin C, et al. The present and future disease burden of hepatitis C virus (HCV) infection with today's treatment paradigm. J Viral Hepat 2014;
21 Suppl 1: 34-59.
Extrahepatic Manifestations of Chronic HCV
Infection
Neuropsychiatric Thyroid dysfunction
manifestations
Ocular manifestations Pulmonary fibrosis
Hematological disorders/ Cardiovascular/
malignancies metabolic diseases
Mixed cryoglobulinemia
Renal impairment
Skin
manifestations Reduced fertility
Peripheral neuropathy
Musculoskeletal and
connective tissue
disorders
Extrahepatic disease can be present in up to 74% of individuals with chronic HCV
Cacoub P, et al. Dig Liver Dis 2014; 46(Suppl 5):S165–S173; Negro F, et al. Gastroenterology 2015; 149:1345–1360;
Englert Y, et al. Fertil Steril 2007; 88:607–11.
Impact of SVR on the Course
of the Disease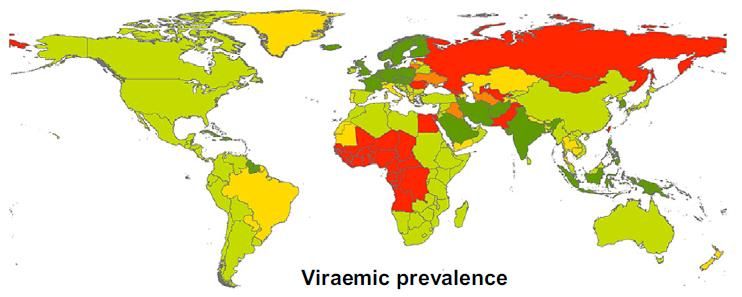
SVR and Mortality Among Patients With
Chronic Hepatitis C and Advanced Fibrosis
30
SVR
non-SVR
Liver Failure (%)
20
p
SVR and Mortality Among Patients With
Chronic Hepatitis C and Advanced Fibrosis
30
SVR
non-SVR
20
HCC (%)
p
HCV Cure Decreases Mortality from Both
Hepatic and Non-hepatic Diseases
23,820 adults in Taiwan; 1095 anti-HCV positive,
69.4% with detectable HCV RNA
HCV seropositive, HCV RNA detectable
HCV seropositive, HCV RNA undetectable
HCV seronegative
Hepatic diseases Extrahepatic diseases
20 20 19.8%
18 pSVR is associated with a reduced
mortality, HCC and transplant
Meta-analysis of 129 studies of IFN-based therapy in 34,563 HCV patients
• Achieving SVR was associated with:
• 62–84% reduction in all-cause mortality
• 68–79% reduction in risk of HCC
• 90% reduction in risk of liver transplant
SVR No SVR
5-year risk of death (all cause) 5-year risk of HCC 5-year risk of liver transplant
13,9
14 14 14
12 11,3 12
10,5 10 12 10
Patients (%)
10 10 9,3 10
8 7,3
8 8
6 6 5,3 6
4,5
3,6
4 4 2,9 4 2,2 2,7
2 1,3 2 0,9 2 0,6
0 0,2
0 0 0
General Cirrhotic HIV/HCV General Cirrhotic HIV/HCV General Cirrhotic HIV/HCV
Saleem J, et al. AASLD 2014; Poster # 44SVR – Patient-relevant End Point ?
• According to the German IQWiG Institute
• SVR is surrogate end-point
• SVR is not a validated patient-relevant end-point
• After major critisms of scientific associations (DGVS, DGIM)
at the G-BA: some non-quantifiable benefit, reduction of
HCC risk possibleLimitations of Evidence-based Medicine Objectives: To determine whether parachutes are effective in preventing major trauma related to gravitational challenge. Design: Systematic review of randomised controlled trials. Both authors without any COI. The study not funded by industry. Data sources: Medline, Web of Science, Embase, and the Cochrane Library databases; appropriate internet sites and citation lists. Study selection: Studies showing the effects of using a parachute during free fall. Smith GC, Pell JP., BMJ 2003;327(7429):1459-61
Limitations of Evidence-based Medicine
Main outcome measure:
Death or major trauma.
Results: We were unable to
identify any randomised
controlled trials of parachute
intervention.
Conclusions: As with many interventions intended to prevent ill
health, the effectiveness of parachutes has not been subjected to
rigorous evaluation by using randomised controlled trials.
Advocates of evidence based medicine have criticised the adoption
of interventions evaluated by using only observational data. We
think that everyone might benefit if the most radical protagonists of
evidence based medicine organised and participated in a double
blind, randomised, placebo controlled, crossover trial of the
parachute.
Smith GC, Pell JP., BMJ 2003;327(7429):1459-61Treatment of Hepatitis C
Treatment of chronic hepatitis C
´90 IFNa 3x3 MU x 24 wks
Davis et al., NEJM 1989
54-63% ´96 IFNa 3x3 MU x 48 wks
60 Poynard et al., NEJM 1995
Poynard et al., Hepatology 1996
50 40% 39% ´98 IFNa + Ribavirin
McHutchison et al., NEJM 1998
40 Poynard et al., Lancet 1998
´00 PEG-IFNa2a
30 Zeuzem et al., NEJM 2000
16%
20 ´01 PEG-IFNa2b + RBV
Manns et al., Lancet 2001
6% ´01 PEG-IFNa2a + RBV
10
Fried et al., NEJM 2002
0 ´02 PEG-IFNa2a + RBV
1990 1996 1998 2000 2001 Hadzyannis et al., Ann Intern Med 2004Treatment of chronic hepatitis C
´90 IFNa 3x3 MU x 24 wks
Davis et al., NEJM 1989
54-63% ´96 IFNa 3x3 MU x 48 wks
60 Poynard et al., NEJM 1995
Poynard et al., Hepatology 1996
50 40% 39% ´98 IFNa + Ribavirin
McHutchison et al., NEJM 1998
40 Poynard et al., Lancet 1998
´00 PEG-IFNa2a
30 Zeuzem et al., NEJM 2000
16%
20 ´01 PEG-IFNa2b + RBV
Manns et al., Lancet 2001
6% ´01 PEG-IFNa2a + RBV
10
Fried et al., NEJM 2002
0 ´02 PEG-IFNa2a + RBV
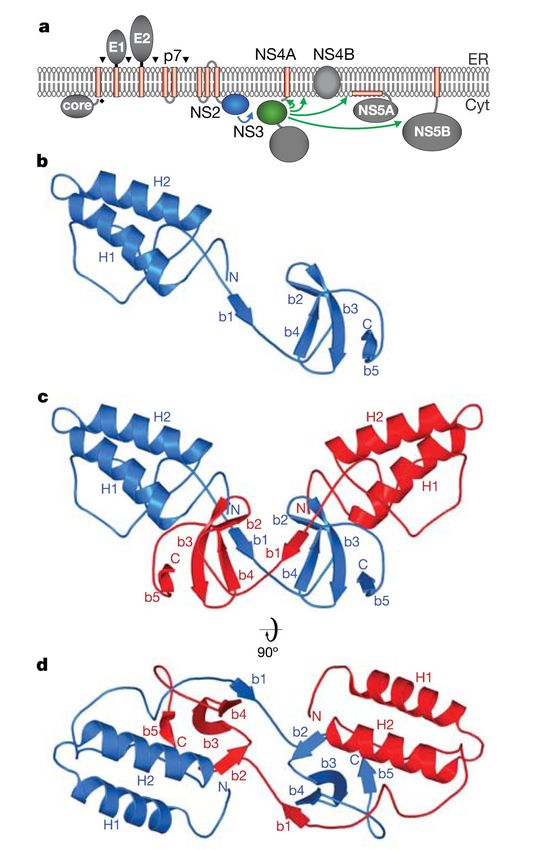
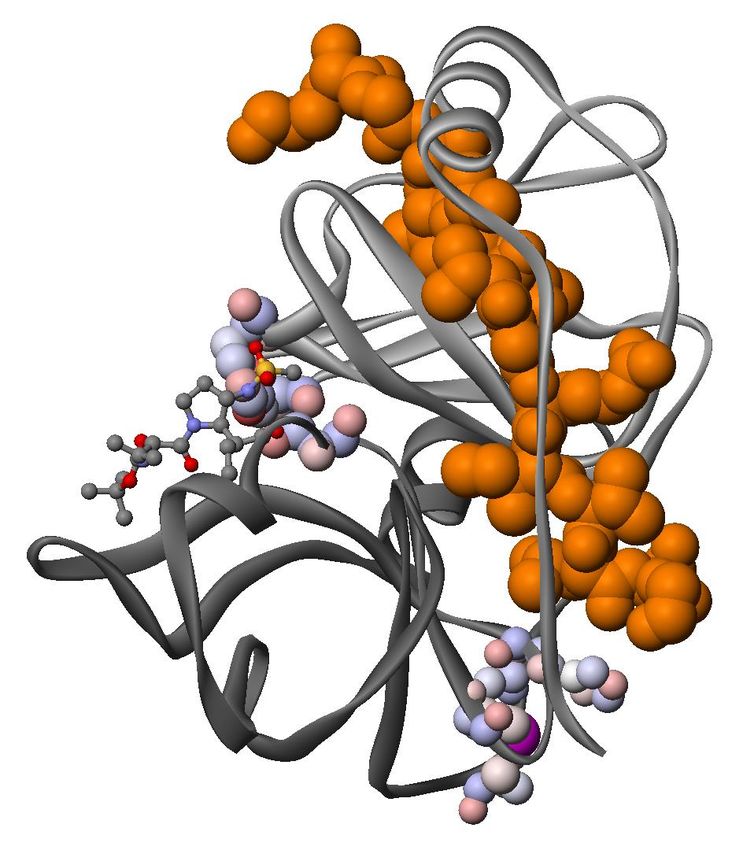
1990 1996 1998 2000 2001 Hadzyannis et al., Ann Intern Med 2004NS3 protease structure and function
Structure and function
active site
“catalytic triad”
NS4A
STRUCTURE and FUNCTION
▪ NS3 protease domain (aa 1-181)
▪ serine protease
▪ chymotrypsine-like fold
▪ polyprotein processing
▪ active site “catalytic triad”
subdomain (His57, Asp81, Ser139)
boundary
▪ oxyanion hole (Gly137)
▪ zinc-finger (Cys97, Cys99, Cys145)
zinc-finger ▪ NS4A is a cofactor that directs the
Lorenz et al., Nature 2006
localization of NS3 and modulates
Kronenberger et al., Clin Liver Dis 2008 its enzymatic activities
Shimakami et al. Gastroenterology 2011Virologic response rates in treatment naive
patients (no head-to-head data)
ADVANCE (TVR) SPRINT-2 (BOC)
PR + TVR PR PR + BOC PR
RVR (wk 4) 66-68% 9% - -
Wk 8 (LI + 4 wk) - - Not reported Not reported
eEVR1 57-58% 8% 44% N/A
EoT 81-87% 63% 71-76% 53%
Relapse 9% 28% 9% 22%
SVR (all) 69-75% 44% 63-66% 38%
RVR, rapid virologic response; LI, lead-in; eRVR, extended RVR;
EoT, end of treatment; SVR, sustained virologic response
Jacobson et al., NEJM 2011
1 Different definitions of eEVR in ADVANCE and SPRINT-2 Reddy et al., APASL 2011
Poordad et al., NEJM 2011Telaprevir and Boceprevir - Safety
(no head-to-head data)
ADVANCE (TVR) SPRINT-2 (BOC)
TVR12/PR PR BOC RGT PR
Discontinuation due 10% 7% 12% 16%
to AEs
Discontinuation due 7% 1%
to rash
Anemia 36% / 9% 14% / 2% 45% / 5% 26% / 4%
(TVR-associated rash during triple therapy
Pilot study with all oral anti-HCV treatment
BMS-790052 + BMS-650032 BMS-790052 + BMS-650032 + PR
7 7
6 6
Log10 HCV RNA
Log10 HCV RNA
5 5
4 4
LOQ 25 IU/mL
3 3 LODAll-oral Hepatitis C Therapy:
a Fast and Competitive Race
Zeuzem S., Nat Rev Gastroenterol Hepatol. 2014;11:644-5.Replikationszyklus des Hepatitis C Virus und
Angriffspunkte der antiviralen Medikamente
Rezeptorbindung
und Endozytose
Transport und Freisetzung
Fusion NS5A-Inhibitoren
(….asvir)
NS3/4A- Protease- (+) RNA
Inhibitoren Zusammensetzung
der Virionen
(….previr)
RNA Replikation
Translation und Poly-
protein Prozessierung
NS5B-Polymerase
Inhibitoren
(….buvir)
Zeuzem, Dtsch Ärztebl Int 2017;114:11-20Genotypische antivirale Aktivität
HCV-1 HCV-2 HCV-3 HCV-4 HCV-5 HCV-6
Sofosbuvir + RBV (x)24 wks x (x)24 wks (x)24 wks (x)24 wks (x)24 wks
Sofosbuvir + PEG-IFN + RBV x x x x x x
Sofosbuvir + Ledipasvir x x x x
Sofosbuvir + Velpatasvir x x x x x x
Sofosbuvir + Daclatasvir x x x x x x
Sofosbuvir + Simeprevir x x x x x
Paritaprevir/r + Ombitasvir x x
± Dasabuvir ± RBV
Grazoprevir + Elbasvir x x (x)
Glecaprevir + Pibrentasvir x x x x x x
Tripel-Therapien x x x x x xWirksamkeit und Verträglichkeit dualer
antiviraler Kombinationen
SVR Nebenwirkungen Laborwert-
veränderungen
Sofosbuvir + Ledipasvir > 95% Kopfschmerzen, Amylase, CK
Erschöpfung
Sofosbuvir + Velpatasvir > 95% Kopfschmerzen, Amylase, CK
Erschöpfung, Übelkeit
Grazoprevir + Elbasvir > 95% Verminderter Appetit, Bilirubin, GPT
Schlaflosigkeit, Angst,
Depression, Schwindel,
Kopfschmerzen, Übelkeit,
Diarrhö, u.a., Pruritus,
Arthralgie, Ermüdung,
Asthenie, Reizbarkeit
Glecaprevir + Pibrentasvir > 95% Kopfschmerzen, Durchfall, Bilirubin, GPT
Übelkeit, FatigueWichtige Medikamenteninteraktionen* (DDI)
dualer antiviraler Kombinationen
DDI
Sofosbuvir + Ledipasvir Amiodaron, Antikonvulsiva, Antacida, PPI (hohe Dosis),
Rifampicin, Johanniskraut, Statine
Sofosbuvir + Velpatasvir Amiodaron, Antikonvulsiva, Antacida, PPI (hohe Dosis),
Rifampicin, Efavirenz, Johanniskraut, Statine
Grazoprevir + Elbasvir Dabigatran, Antikonvulsiva, Antimykotika, Bosentan,
Johannniskraut, Atazanavir, Darunavir, Lopinavir, u.a.,
Efavirenz, Statine, Ciclosporin, Modafinil
Glecaprevir + Pibrentasvir Dabigatran, Antikonvulsiva, Rifampicin, Ethinylestradiol,
Johanniskraut, Atazanavir, Darunavir, Efavirenz, Statine,
Ciclosporin, Omeprazol
*HEP Drug Interactions, University of Liverpool: http://www.hep-druginteractions.org
*HEP Mobile Apps (Apple, Android)Posologie dualer antiviraler Kombinationen
Dosis pro Tablette Tablettenzahl Nahrungseffekt
Sofosbuvir + Ledipasvir 400 mg / 90 mg 1 Tablette / Tag mit oder ohne
Sofosbuvir + Velpatasvir 400 mg / 100 mg 1 Tablette / Tag mit oder ohne
Grazoprevir + Elbasvir 100 mg / 50 mg 1 Tablette / Tag mit oder ohne
Glecaprevir + Pibrentasvir 100 mg / 40 mg 3 Tabletten / Tag mit Nahrung
Charakteristika dualer antiviraler Kombinationen
Genotypische CKD-4,5 decompensierte
Aktivität Zirrhose
Sofosbuvir + Ledipasvir nicht GT-2 & GT-3 Nein Ja
Sofosbuvir + Velpatasvir pangenotypisch Nein Ja
Grazoprevir + Elbasvir nur GT-1 & GT-4 Ja Nein
Glecaprevir + Pibrentasvir pangenotypisch Ja NeinProfil: Sofosbuvir + Velpatasvir (Epclusa®)
Empfohlene Behandlung und Dauer für alle HCV-Genotypen
Patientengruppea Behandlung und Dauer
Patienten ohne Zirrhose und Epclusa für 12 Wochen
Patienten mit kompensierter Die Zugabe von Ribavirin kann bei
Zirrhose Patienten mit einer Infektion vom
Genotyp 3 und kompensierter Zirrhose
erwogen werden
Patienten mit dekompensierter Epclusa + Ribavirinb für 12 Wochen
Zirrhose
a Einschließlich Patienten mit Koinfektion mit HIV und Patienten mit rezidivierender
HCV-Infektion nach Lebertransplantation
b RBV 1000-1200 mg/Tag bei CPT B vor LTx;
RBV 600 mg/Tag bei CPT C vor LTx und CPT B oder C nach LTx
Fachinformation Epclusa, September 2019Profil: Glecaprevir + Pibrentasvir (Maviret®)
(1) Empfohlene Behandlungsdauer für (2) Empfohlene Behandlungsdauer
Maviret bei therapienaiven Patienten für Maviret bei Patienten, bei denen
eine Vorbehandlung mit peg-IFN +
Ribavirin +/- Sofosbuvir oder mit
Sofosbuvir + Ribavirin versagt hat
Empfohlene Empfohlene
Genotyp Behandlungsdauer Genotyp Behandlungsdauer
Ohne Mit Ohne Mit
Zirrhose Zirrhose Zirrhose Zirrhose
GT 1, 2, 4-6 8 Wochen 8 Wochen GT 1, 2, 4-6 8 Wochen 12 Wochen
GT 3 8 Wochen 12 Wochen GT 3 16 Wochen 16 Wochen
Fachinformation Maviret, September 2019Vergleich der pan-genotypischen Kombinationen
Sofosbuvir + Velpatasvir Glecaprevir + Pibrentasvir
✓Therapiedauer bei nicht-vorbe-
handelten Patienten 8 Wochen
✓Therapiedauer 12 Wochen (12 Wo. bei GT3 mit Zirrhose)
✓Dekompensierte Zirrhose ✓Behandlung auch bei Nieren-
✓CrCl > 30 ml/min insuffizienz möglich, nicht aber
✓RBV bei GT3 Patienten mit bei Patienten mit
Zirrhose und allen Patienten dekompensierter Zirrhose
mit dekompensierter Zirrhose ✓Therapiedauer bei vorbe-
handelten Patienten zwischen
8 Wo. (ohne Zirrhose), 12 Wo.
(mit Zirrhose) und 16 Wochen
(GT3 mit/ohne Zirrhose)
✓Kein RBV bei GT3-Patienten mit
ZirrhoseSpezielle klinische Konstellationen • Akute Hepatitis C • Limitierte Studiendaten zu Kindern und Jugendlichen • Zeitpunkt der antiviralen Therapie bei Patienten auf Transplantationslisten (“point-of-no-return”, Allokation HCV-positiver Organe) • Zeitpunkt einer antiviralen Therapie bei Patienten mit chronischer Hepatitis C und einem in kurativer Intention behandelten HCC • Therapie einer Hepatitis C bei Patienten mit einem nicht kurativ behandelbaren HCC • Tripeltherapien für Patienten mit virologischem Relapse nach DAA Therapie
SOF/VEL/VOX for 12 weeks as a salvage regimen in
NS5A inhibitor-experienced G1–6 patients
(i) Overall SVR12 (ITT) (ii) SVR by genotype
96
100 97 96 100 100 95 91 100 100
100
80
80
SVR12, %
SVR12, %
60 6 relapses 60
1 on-tx failure
40
2 withdrew consent 40 146
97/ 45/ 5/ 74/ 20/ 1/
1 LTFU 6/
20 /
101 45 5 78 22 1 6
20 150
253/263
0
G1 G1a G1b G2 G3 G4 G5 G6
0
(iii) SVR by cirrhosis (iv) SVR by NS5A RASs
99 93 100 98 96 100 94 97
100
80 80
SVR12, %
SVR12, %
60 60
1 withdrew consent 6 relapses
1 LTFU 1 on-tx failure
40 1 withdrew consent 40
20 20 42/ 199/ 9/ 120/ 70/
140/142 113/121 43 208 9 127 72
0 0
No Any NS3 NS5A NS3 +
No Cirrhosis Cirrhosis RASs RASs only only NS5A
Bourlière M, et al., NEJM 2017Global targets achieved if viral hepatitis
is controlled by 2030
90% reduction in 80% of treatment 65% reduction in
new cases of chronic eligible people with chronic hepatitis B and C
hepatitis B and C hepatitis B and C treated deaths
100
80
60
Percent
40
20
0
New cases of chronic Treatment eligible Hepatitis B and C
hepatitis B and C people with chronic deaths
hepatitis B and C
World Health Organization. Draft global health sector strategies. Viral Hepatitis, 2016–2021. Available at:
http://apps.who.int/gb/ebwha/pdf_files/WHA69/A69_32-en.pdf?ua=1 (accessed September 2016)Global timing of hepatitis C virus elimination:
Estimating the year countries will achieve the
World Health Organization elimination targets
Year of HCV elimination by country or territory
Iceland Belgium New Zealand
Spain Canada Norway
France Chile Oman
Australia Cyprus Poland
Japan Czechia Portugal
Italy Denmark Qatar
Switzerland Estonia Singapore
UK Finland Slovakia
South Korea Greece Slovenia
Austria Hong Kong Sweden
Germany Hungary Taiwan
Malta Israel United Arab Emirates
Saudi Arabia Kuwait United States
Ireland Latvia
Netherlands Lithuania
Bahrain Luxembourg
Year of elimination
80% (36/45) of high-income countries/territories are not on track to
meet the WHO 2030 HCV elimination targets
67% (30/45) are off-track by ≥20 years
Razavi H, et al. EASL 2019, Vienna, Austria. #SAT-260Zusammenfassung • Eine Therapieindikation besteht für alle Patienten mit Hepatitis C, Screening ! • SOF/VEL und GLE/PIB sind pan-genotypische Kombinationen • Andere Kombinationen haben in Deutschland nur eine Bedeutung bei der Optimierung der Behandlungskosten • Protease-Inhibitoren sind bei Patienten mit einer dekompensierten Zirrhose kontraindiziert • SOF ist bei Patienten mit schwerer Niereninsuffizienz nicht zugelassen • SOF/VEL/VOX zugelassen für DAA-Nonresponder • WHO-Ziele werden in vielen Ländern nicht erreicht werden
Treatment cascade simplification from 10 to only 4 steps ?
Treatment/Monitoring phase
(doctor visits required)
4
10
Pre-treatment Phase
9
8 SVR 12 CURE
Primary
Care 7 Week 12 if
6
3 Cirrhotic
Week 8
Diagnostic Phase 5 Week 4
4 Treatment
Fibrosis choice
3
Evaluation
2 Genotype
1 HCV treater
Confirmed (see a
Viral Load specialist)
Screen (anti
HCV)
For 80% For 80% Phone Phone
subjects subjects Call Call
4 8 12
APRI EXPEDITION-8
Key
Barriers Low Limited
• Low disease • Low patient • Sick funds • Reflex RNA
Along priority linkage to
awareness motivation control system testing
Patient among care
capacity
Journey PCPsA meta-analysis of the risk of HCC occurrence
following SVR to IFN or DAAs
IFN DAA
1.14 (0.86–1.52) 2.96 (1.76–4.96)
HCC occurrence rate (/100 PY) HCC occurrence rate (/100 PY)
Meta regression of HCC occurrence
Unadjusted RR Adjusted RR 95% CI P-value
Average follow-up 0.88 0.75 0.56–0.99 0.04
Average age 1.11 1.06 0.99–1.14 0.12
DAA treatment 2.77 0.68 0.18–2.55 0.56
Waziry R, et al. J Hepatol 2017;67:1204–12 RR: risk ratioA meta-analysis of the risk of HCC
recurrence following SVR to IFN or DAAs
IFN DAA
12.16 (5.00–29.58)
9.21 (7.18–11.81) HCC recurrence rate (/100 person-years)
HCC recurrence rate (/100 PY)
Meta regression of HCC reccurrence
Unadjusted RR Adjusted RR 95% CI P-value
Average follow-up 0.86 0.79 0.55–1.15 0.19
Average age 1.11 1.11 0.96–1.27 0.14
DAA treatment 1.36 0.62 0.11–3.45 0.56
Waziry R, et al. J Hepatol 2017;67:1204–12You can also read