High rates of OCD symptom misidentification by mental health professionals
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ANNALS OF CLINICAL PSYCHIATRY
ANNALS OF CLINICAL PSYCHIATRY 2013;25(3):201-209 RESEARCH ARTICLE
High rates of OCD symptom misidentification
by mental health professionals
Kimberly Glazier, MA BACKGROUND: More than a decade may pass between the onset of obses-
Rachelle M. Calixte, BS
sive-compulsive disorder (OCD) symptoms and initiation of treatment.
Rachel Rothschild, BS
One explanation may be health care professionals’ limited awareness of
Ferkauf Graduate School of Psychology
OCD symptom presentations. We assessed mental health care providers’
Yeshiva University
Bronx, NY, USA ability to identify taboo thoughts as manifestations of OCD.
Anthony Pinto, PhD
Columbia University/New York State METHODS: A random sample of 2,550 American Psychological Association
Psychiatric Institute members were asked to give diagnostic impressions based on 1 of 5 OCD
New York, NY, USA
vignettes: 4 about taboo thoughts and 1 about contamination obsessions.
RESULTS: Three-hundred sixty (14.1%) providers completed the survey.
The overall misidentification rate across all vignettes was 38.9%. Rates of
incorrect (non-OCD) responses were significantly higher for the taboo
thoughts vignettes (obsessions about homosexuality, 77.0%; sexual obses-
sions about children, 42.9%; aggressive obsessions, 31.5%; and religious
obsessions, 28.8%) vs the contamination obsessions vignette (15.8%).
CONCLUSIONS: Mental health professionals commonly misidentify OCD
symptom presentations, particularly sexual obsessions, highlighting a
need for education and training.
KEYWORDS: obsessive-compulsive disorder, misidentification, taboo
CORRESPONDENCE
thoughts, symptom presentation
Kimberly Glazier, MA
Ferkauf Graduate School of Psychology
Yeshiva University
1165 Morris Park Avenue
Bronx, NY 10461 USA
E-MAIL
kimberlyglazier@gmail.com
AACP.com Annals of Clinical Psychiatry | Vol. 25 No. 3 | August 2013 201HIGH RATES OF OCD SYMPTOM MISIDENTIFICATION
I N T RO D U C T I O N rials for psychiatric clinicians, we decided to compare
participants’ ability to correctly identify taboo thoughts
The delay between the onset of obsessive-compulsive vignettes (covering aggressive, religious, and sexual
disorder (OCD) symptoms and the inception of treat- obsessions) vs a contamination vignette. We expected
ment typically is ≥10 years.1-3 This gap is of significant that vignettes about taboo thoughts would be more likely
concern because OCD can be a debilitating condition; to be misidentified, compared with vignettes about con-
for example, the World Health Organization reported that tamination obsessions.
OCD is the 11th leading cause of nonfatal burden in the
world.4 Because highly effective, empirically based treat-
ments exist,5 decreasing the time from onset of symp- METHODS
toms to treatment engagement may reduce the symptom
severity, distress, and impairment associated with OCD. Participants
One explanation for the delay between OCD symp- The APA online membership directory (http://memforms.
tom onset and treatment may be health care profession- apa.org/apa/cli/mbdirsearch/index.cfm) was used to
als’ lack of awareness regarding the broad range of OCD locate potential participants for this e-mail survey. Fifty
symptoms, which may result in misdiagnosis or nondi- APA members were randomly selected from each state and
agnosis of OCD. As many as 26% of individuals who meet the District of Columbia. When no e-mail address was pro-
OCD criteria are initially not correctly identified as having vided for a selected individual, the next member who pro-
OCD, with the most common impressions being general- vided his/her contact information was selected instead.
ized anxiety disorder, depression, family problems, and Results from a power analysis with a medium effect size
personality disorder.2 Misdiagnosis of OCD can result in (f = .25), α = .05, and 80% power supported a sample size
improper treatment, higher treatment-related costs, and of 200. Based on the response rate of a comparable online
poorer outcomes, including clinical worsening and treat- survey (14.8%), we predicted a response rate of 15%.19
ment dropout.2,6,7 Therefore, our assessment was that e-mailing 2,550 APA
OCD is a heterogeneous disorder with varying symp- members should result in approximately 380 completed
tom presentations both across and within individuals over surveys, well above the sample size estimated by our
time.8 Besides hoarding (now a distinct disorder in the power analysis.
DSM-59), factor analytic studies have reported the follow- Of the 2,550 APA members e-mailed, 360 (14.1%)
ing major OCD symptom dimensions: symmetry/order- completed the survey (57.5% female; mean age, 51.8
ing, doubt/checking, contamination/cleaning, and taboo years [SD = 12.6]). Most participants held a degree in
thoughts.10,11 Because no study to date has assessed mental clinical psychology, had a PhD, worked in a clinical set-
health professionals’ knowledge of OCD symptom presen- ting predominantly with adults, and reported cognitive-
tations, the impact of the heterogeneity of OCD symptom- behavioral therapy as their main theoretical orienta-
atology on misdiagnosis is not known. We hypothesize that tion. It should be noted that the participants’ training
the taboo thoughts dimension of OCD, including intrusive and experience in treating OCD was not assessed. This
thoughts about harming others, morality, incest, pedo- was done in attempt to keep the participants blind to the
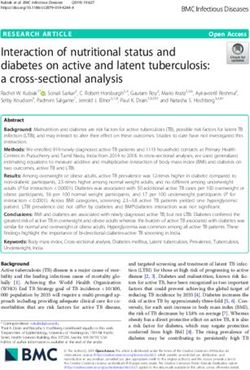
philia, sacrilege, sexuality, and violent images,12 is more study’s aim. See FIGURE 1 for response rates by vignette
likely to be misidentified because of limited awareness of type and TABLE 1 for sample demographics.
these presentations among clinicians. Taboo thoughts are
common, with reported prevalence rates ranging between Procedures
14% and 44% among individuals with OCD,13-15 but these Five vignettes were created to assess the ability of mental
obsessions are often overlooked in educational materials health professionals to accurately identify specific symp-
for psychiatric clinicians.16-18 tom presentations of OCD. A vignette about contamina-
We conducted a vignette-based survey study in a tion obsessions was selected as the study control because
random sample of mental health providers who were mental health professionals are more readily exposed to
members of the American Psychological Association this presentation through educational materials and the
(APA). Because the contamination-symptom presenta- media. The 4 experimental vignettes each focused on a
tion of OCD is commonly described in educational mate- common symptom presentation of taboo thoughts OCD:
202 August 2013 | Vol. 25 No. 3 | Annals of Clinical PsychiatryANNALS OF CLINICAL PSYCHIATRY
FIGURE 1
Response rates by vignette type
2,500 APA members randomly selected from online
directorya and e-mailed vignette-based survey
Obsessions about Sexual obsessions Aggressive Religious Contamination
homosexuality about children obsessions obsessions obsessions
510 members e-mailed 510 members e-mailed 510 members e-mailed 510 members e-mailed 510 members e-mailed
83 provided consent 91 provided consent 96 provided consent 83 provided consent 91 provided consent
74 (14.5%) 71 (13.9%) 73 (14.3%) 66 (12.9%) 76 (14.9%)
completed survey completed survey completed survey completed survey completed survey
50 US-based APA members per state and the District of Columbia.
a
APA: American Psychological Association.
aggressive obsessions, religious obsessions, obsessions through September 2011. The survey was piloted on 10
about homosexuality, and sexual obsessions about chil- individuals and the average completion time was 5 min-
dren. To reduce content bias, the demographic informa- utes, 37 seconds (SD = 59.7 seconds).
tion of the patient described remained constant across One of the 5 vignettes was randomly assigned to each
all 5 vignettes. Furthermore, in accordance with a review participant. To ensure equal distribution of vignettes, 10
article of clinical vignette–based studies that emphasized of each vignette were assigned per state. Participants were
that “clarity and brevity [of the vignettes] are impera- e-mailed a description of the study and a link to the sur-
tive,”20 the length of this study’s vignettes ranged from 4 to vey site. At least 2 weeks after the first e-mail, a follow-up
5 sentences (word count range, 64 to 80). According to the reminder e-mail was sent. The first page of the survey
Coleman-Liau Index, the vignettes were written at an aver- included consent information; participants who elected
age grade level of 10.80 (range, 9.80 to 12.10).21 Also, simi- not to provide informed consent were not permitted to
lar to previous vignette-based studies in which the content continue with the survey. Upon completion of the study,
of the vignettes was validated by specialists in the field,22-24 participants were invited to enter a raffle drawing for a
the content of the 5 vignettes was approved by 5 members $100 gift card.
of the Center for OCD and Related Disorders at the New Participants were asked whether they primar-
York State Psychiatric Institute, Columbia University. The ily work with children/adolescents or adults. Based on
OCD specialists who validated the vignettes consisted of a their response, they were presented with a vignette that
combination of researchers and clinicians, each of whom described “Jack, a teenaged boy” or “Jack, a middle-aged
had at least 5 years of experience working with OCD. The 5 man.” After the vignette, participants were asked to give
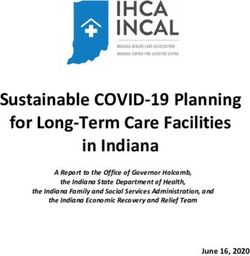
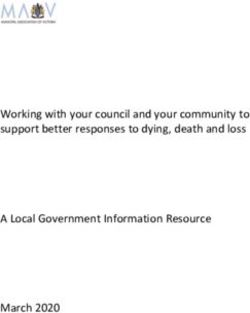
vignettes appear in FIGURE 2. their diagnostic impressions of “Jack” by selecting from a
The study was approved by the institutional review list of 36 psychiatric and nonclinical diagnoses (“Other”
board at Albert Einstein College of Medicine/Yeshiva was also an option) (FIGURE 3). If participants selected >1
University, and data collection took place from June 2011 condition, they were asked to rank the order of likelihood
AACP.com Annals of Clinical Psychiatry | Vol. 25 No. 3 | August 2013 203HIGH RATES OF OCD SYMPTOM MISIDENTIFICATION
TABLE 1
Description of total sample
Sample Sample
Characteristic (n = 360) Characteristic (n = 360)
Age, years (SD) 51.8 (12.6) Top 5 types of professional degree (%)
Gender Clinical psychology 72.0%
Female, % 57.5% Counseling psychology 8.6%
Ethnicity: Hispanic Child psychology 8.4%
Yes, % 3.9% School psychology 6.1%
Race a
Neuropsychology 5.3%
White 84.4% Top 5 specialty areas
African American 2.0% Anxiety disorders 45.3%
Asian 1.7% Mood disorders 44.4%
Other 1.5% Adjustment disorders 36.6%
Native American 1.2% Children/adolescents 35.5%
Years since highest degree awarded, mean (range) 20 (0 to 50) Family therapy 20.7%
Professional setting (%) a
Predominant patient population
Clinical 80.4% Adults 71.5%
Academic 26.0% Child/adolescents 28.5%
Research 14.5% Clients seen per day, mean (SD) 4.0 (3.1)
Other 5.4% New clients per month, mean, (SD) 6.4 (6.6)
Currently licensed (%) 81.3% Top 5 main theoretical orientations (%)
Top 5 degrees/licenses (%)a Cognitive-behavioral therapy 50.6%
PhD 67.6% Psychodynamic 17.0%
MA/MS 31.5% Eclectic/integrative 5.1%
PsyD 14.2% Humanistic 4.7%
EdD/EdS/EdM 6.8% Family relational 3.6%
MSW/LMSW 1.7% Primary location description (%)
Urban 43.6%
Suburban 32.4%
Rural 20.1%
a
More than one answer was permitted.
for each disorder chosen. Participants were considered ducted to compare rates of OCD misidentification for each
to have provided a correct response as long as OCD was vignette type vs the contamination obsessions vignette
selected as one of the possible conditions, regardless of (control condition). Frequencies were also calculated for
where OCD was listed on their ranking. the most prevalent non-OCD response for each vignette.
Point biserial correlations between OCD identifica-
Data analysis tion and each demographic variable were examined. To
SPSS (IBM) and SAS (SAS Institute) statistical software test for collinearity between demographic variables, point
were used for descriptive and logistic regression analyses. biserial correlations were conducted between those demo-
All analyses were 2 tailed, and statistical significance was graphic variables that had a significant correlation with
determined by α = .05. Rates of OCD misidentification OCD identification. It was decided a priori that if a pair of
were examined for each vignette. A Wald chi-square test demographic variables was correlated at ≥0.6, guidelines
within the context of a logistic regression analysis was con- for addressing multicollinearity would be followed.25
204 August 2013 | Vol. 25 No. 3 | Annals of Clinical PsychiatryANNALS OF CLINICAL PSYCHIATRY
A multivariate regression was conducted to deter- FIGURE 2
mine the best predictors of OCD identification among Study vignettesa
1) each of the demographic variables significantly corre- Contamination obsessions
lated with an OCD response, and 2) vignette type. Jack, a middle-aged man, constantly worries about dirt and germs.
These worries limit his range of daily activities, for Jack tries at all
costs to avoid touching objects he believes may be contaminated.
However, if Jack does come in contact with a “dirty” object, he
R E S U LT S immediately washes his hands to prevent himself from catching
a disease. These worries occur often and cause Jack significant
OCD misidentification by vignette type distress.
The response rate did not differ by vignette type (12.9% to Aggressive obsessions
14.9%; Wald χ2 [4] = 0.806; P = .938). Across all 5 vignettes, Jack, a middle-aged man, thought about pushing the lady next
38.9% of participants provided an incorrect (non-OCD) to him onto the subway tracks. He was distressed by the thought
and the fear that he might act on it, so he left the subway and
response. The contamination obsessions vignette walked home. However, Jack remained worried and found himself
resulted in the lowest misidentification rate, with 15.8% frequently visualizing the situation to make sure he did not actually
of participants providing a non-OCD response. In con- cause her any harm. This worry about harming others occurs often
and causes Jack significant distress.
trast, the 4 taboo thoughts vignettes were incorrectly
identified by 44.7% of mental health professionals (Wald Obsessions about homosexuality
χ2 [1] = 17.91; P < .001). APA members who reviewed one Jack, a middle-aged man, has been in a committed relationship
with his girlfriend for 2 years. While he loves his girlfriend and has
of the taboo thoughts vignettes were 99.7% less likely to never been sexually attracted to males, he finds himself wondering
identify OCD than those who reviewed the contamina- if he really is gay. Upon seeing males, Jack assesses his sexual
tion obsessions vignette. See TABLE 2 for rates of OCD arousal to determine if he is turned on. This doubt regarding his
sexuality occurs often and causes Jack significant distress.
misidentification for each vignette type and the odds
ratio of misidentification for each of the taboo thoughts Religious obsessions
vignettes vs the contamination obsessions vignette. Jack, a middle-aged, highly religious man, believes that he is
not allowed to say the Lord’s name in vain. Moreover, if he hears
When comparing specific taboo thoughts vignettes
someone else say anything remotely negative toward God, Jesus,
with the contamination vignette, OCD misidentification or the Virgin Mary, he feels significant distress, fearing for his and
was significantly higher for both the obsessions about the individual’s safety and well-being. Therefore, upon hearing
homosexuality and sexual obsessions about children such expressions, Jack prays repeatedly to himself until he feels
safe from harm. This can go on for hours.
vignettes.
The most common clinical impressions assigned Sexual obsessions about children
to “Jack” by participants who did not select OCD were Jack, a middle-aged man, used to love spending time with his
nieces and nephews and is their “favorite uncle.” Recently he had
as follows (listed by vignette type): sexual identity con- an image of touching one of the children inappropriately, which
fusion (65%; obsessions about homosexuality), pedo- upset him greatly. He was certain that he’d never harm them but
philia (37%; sexual obsessions about children), impulse the thoughts increased in frequency. He now tries to avoid contact
with the children and will not spend time alone with them. Jack’s
control disorder (38%; aggressive obsessions), strong fear of acting on these thoughts occurs often and causes him
religious values (30%; religious obsessions), and spe- significant distress.
cific phobia (63%; contamination obsessions).
aFor participants who work primarily with children/adolescents:
1. “Jack” was presented as a “teenaged boy” in each vignette.
Predictors of OCD identification 2. In the vignette on sexual obsessions about children, “uncle” and “nieces and
nephews” were changed to “cousin” and “cousins,” respectively.
Bivariate correlations and chi-square analyses identi-
fied the following variables as significantly associated
with an OCD response: cognitive-behavioral therapy
(CBT) theoretical orientation (r[348] = .121; P = .024), lowing demographic variables: licensed and clinical
licensure (r[343] = .129; P = .017), location of practice, psychology (r[344] = .298; P < .001), licensed and mood
ie, urban or suburban vs rural (χ2 [2] = 7.531; P = .023), disorder specialist (r[341] = .249; P < .001), clinical
clinical psychology degree (r[342] = .109; P = .044), psychology degree and mood disorder specialist
and mood disorder specialist (r[339] = .112; P = .039). (r[341] = .154; P < .004), clinical psychology degree and
Significant correlations were found between the fol- CBT orientation (r[344] = .125; P = .020), and licensed
AACP.com Annals of Clinical Psychiatry | Vol. 25 No. 3 | August 2013 205HIGH RATES OF OCD SYMPTOM MISIDENTIFICATION
FIGURE 3
Survey participants’ diagnostic impressions of patient in vignettea
Based on the vignette, which option most likely applies? If more than one, please mark all options that may apply:
____ Agoraphobia with panic disorder ____ Major depression
____ Agoraphobia without panic disorder ____ Marital problems
____ Anger management issues ____ Narcissistic personality disorder
____ Anorexia ____ Obsessive-compulsive disorder
____ Antisocial personality disorder ____ Obsessive-compulsive personality disorder
____ Attention-deficit/hyperactivity disorder ____ Organic disorder
____ Autism ____ Panic disorder
____ Avoidant personality disorder ____ Paranoid personality disorder
____ Bipolar I disorder ____ Posttraumatic stress disorder
____ Bipolar II disorder ____ Pedophilia
____ Borderline personality disorder ____ Psychosis
____ Bulimia ____ Sexual identity confusion
____ Delirium ____ Schizophrenia
____ Delusional disorder ____ Schizotypal personality disorder
____ Generalized anxiety disorder ____ Schizoid personality disorder
____ Histrionic personality disorder ____ Social phobia/social anxiety disorder
____ Impulse control disorder ____ Specific phobia
____ Intermittent explosive disorder ____ Strong religious values
____Other
If you marked more than one of the above, please rank your choices in order of likelihood:
aBased on a list of 36 psychiatric diagnoses and nonclinical symptom presentation and “Other.”
and CBT orientation (r[345] = .125; P = .020). Based to provide an OCD response, their rate of OCD misidenti-
on these correlations, there was no evidence of sig- fication was still 31.5%.
nificant multicollinearity among the demographic
variables.
When the 5 variables correlated with OCD identifi- DISCUSSION
cation were entered in a multivariate logistic regression
along with vignette type, only vignette type (Wald χ2 [4] The significant delay typically seen between onset
= 57.17; P < .001) and CBT orientation (Wald χ2 [1] = 3.92; of OCD symptoms and treatment initiation may be
P = .048) remained significant. However, even though impacted by limited awareness among mental health
CBT-oriented practitioners were significantly more likely professionals about the variety of OCD symptom pre-
206 August 2013 | Vol. 25 No. 3 | Annals of Clinical PsychiatryANNALS OF CLINICAL PSYCHIATRY TABLE 2 Comparison of rates of incorrect OCD identification between the contamination obsessions vignette and each of the taboo thoughts vignettes (n = 360) Vignette type Incorrect, % χ2 P Odds ratio Contamination obsessions 15.8% — — — Obsessions about homosexuality 77.0% 45.77
HIGH RATES OF OCD SYMPTOM MISIDENTIFICATION
the most commonly selected diagnosis by profession- vignettes on ordering/arranging, checking, and hoarding,
als who received the sexual obsessions about children in addition to the vignettes on contamination and taboo
vignette was pedophilia (identified as primary diagnosis thoughts. Furthermore, future research could include
by 37%). An incorrect “pedophile” label brings on intense non-OCD vignettes to provide a stronger control group. In
adverse societal reactions toward the individual as well addition, assessing the ability of primary care physicians
as detrimental psychological consequences. Individuals (PCPs) to correctly identify common OCD presentations
with OCD who have intrusive sexual thoughts about chil- is recommended. Research shows that from 20% to 62%
dren experience significant distress from the thoughts; of individuals first present their psychiatric symptoms
to have their worst fears of being a pedophile incorrectly to PCPs.28,29 A focus group study found the vast majority
confirmed by a mental health professional may induce of patients reported feeling more comfortable speaking
greater impairment in functioning and depression. A with their PCP regarding psychiatric issues as opposed
further complication is that in some states clinicians to a mental health professional.30 However, 38% of OCD
are mandated to report individuals who they believe patients who reported being misdiagnosed were given an
may harm an identifiable victim.27 Clinicians who are incorrect diagnosis by their general practitioner.2 Proper
not aware of intrusive aggressive and sexual thoughts OCD detection at the primary care stage facilitates appro-
as symptoms of OCD may incorrectly report individuals priate mental health referrals.
with these types of obsessions to the authorities. Intervention studies that focus on increasing aware-
To increase participation, the study was designed to ness of the various OCD symptom presentations may
take place over the Internet and to have an average com- help improve identification of the disorder and reduce
pletion time of approximately 5 minutes. Although all the health care costs. Targeting graduate and medical school
vignettes were validated as illustrating OCD, having to training programs may serve as an appropriate entry
decide on an individual’s condition based on 4 to 5 sen- point; increasing OCD education among individuals
tences has significant limitations. We attempted to miti- in training may have broad implications for increasing
gate the impact of this limitation by allowing participants awareness of OCD in clinical practice. ■
to select as many conditions as they deemed appropriate
and giving credit for OCD identification whether or not it DISCLOSURES: The authors report no financial relation-
was named as the primary disorder. Another study limita- ship with any company whose products are mentioned in
tion was that the study only included members of the APA, this article or with manufacturers of competing products.
resulting in an oversampling of clinicians with a PhD or
PsyD. Furthermore, the low response rate (14.1%) suggests ACKNOWLEDGMENTS: This study is supported by National
possible limitations to the representativeness of the find- Institute of Mental Health grant K23 MH080221 (Pinto).
ings to the sample population. In addition, the lower than We would like to thank Gary Winkel, PhD, for his help
expected response rate may be due to receiving the e-mail with the statistical analyses and members of the Center
solicitation from a graduate student, mental health profes- for OCD and Related Disorders at Columbia/New York
sionals’ busy schedules, and the low financial incentive. State Psychiatric Institute for approving the OCD con-
Future studies could assess mental health providers’ tent of the vignettes. We would also like to thank Shafou
ability to correctly identify OCD across a broader range Chen, MD, PhD, Jerome Wakefield, PhD, DSW, and Sonia
of OCD symptom presentations, for example, including Suchday, PhD, for their input and guidance.
REFERENCES
1. Cullen B, Samuels JF, Pinto A, et al. Demographic Global burden of obsessive-compulsive disorder in the health education issues. New York, NY: Nova Science
and clinical characteristics associated with treatment year 2000. http://www.who.int/healthinfo/statistics/ Publishers, Inc; 2008:198-205.
status in family members with obsessive-compulsive bod_obsessivecompulsive.pdf. Accessed January 14, 8. Pinto A, Grados MA, Simpson HB. Challenges in
disorder. Depress Anxiety. 2008;2:218-224. 2013. OCD research: overcoming heterogeneity. In: Simpson
2. Hollander E, Stein DJ, Kwon JH, et al. Psychosocial 5. American Psychiatric Association Practice HB, Neria Y, Lewis-Fernandez R, et al, eds. Anxiety
function and economic costs of obsessive-compulsive Guidelines. http://www.psychiatryonline.com/ disorders: theory, research, and clinical perspectives.
disorder. CNS Spectrum. 1998;3:48-58. pracGuide/pracGuideTopic_10.aspx. Accessed January Cambridge, UK: Cambridge University Press; 2010:69-79.
3. Pinto A, Mancebo MC, Eisen JL, et al. The Brown 14, 2013. 9. Diagnostic and statistical manual of mental dis-
Longitudinal Obsessive Compulsive Study: clinical 6. Gordon WM. Sexual obsessions and OCD. Sexual orders, 5th ed. Arlington, VA: American Psychiatric
features and symptoms of the sample at intake. J Clin and Relationship Therapy. 2002;17:343-354. Association; 2013.
Psychiatry. 2006;67:703-711. 7. Williams M. Homosexuality anxiety: a misunder- 10. Pinto A, Eisen JL, Mancebo MC, et al. Taboo
4. Ayuso-Mateos JL; World Health Organization. stood form of OCD. In: Sebeki LV, ed. Leading-edge thoughts and doubt/checking: a refinement of the factor
208 August 2013 | Vol. 25 No. 3 | Annals of Clinical PsychiatryANNALS OF CLINICAL PSYCHIATRY
structure for obsessive–compulsive disorder symptoms. 17. Morrison J. The first interview. 3rd ed. New York, Review. 1992;16:82-92.
Psychiatry Res. 2007;151:255-258. NY: Guildford Press; 2008. 25. Grewal R, Cote JA, Baumgartner H. Multicollinearity
11. Pinto A, Greenberg BD, Grados MA, et al. Further 18. Walker JI. Complete mental health: the go-to guide and measurement error in structural equation models:
development of YBOCS dimensions in the OCD for clinicians and patients. New York, NY: W.W. Norton implications for theory and testing. Marketing Science.
Collaborative Genetics study: symptoms vs categories. & Company; 2010. 2004;23:519-529.
Psychiatry Res. 2008;160:83-93. 19. Porter SR, Whitcomb ME. The impact of contact 26. Penzel F. How do I know I’m not really gay?
12. Goodman WK, Rasmussen SA, Price LH, et al. Yale- type on web survey response rates. Public Opinion International OCD Foundation. http://www.oc
Brown obsessive compulsive scale (Y-BOCS). http:// Quarterly. 2003;67:579-588. foundation.org/EO_HO.aspx. Accessed January 14, 2013.
www.stlocd.org/handouts/YBOC-Symptom-Checklist. 20. Veloski J, Tai S, Evans AS, Nash DB. Clinical vignette- 27. Tarasoff v Regents of the University of California. In:
pdf. Accessed January 14, 2013. based surveys: a tool for assessing physician practice Gostin LO, ed. Public health law and ethics: a reader.
13. Grant JE, Pinto A, Gunnip M, et al. Sexual obsessions variation. Am J Med Qual. 2005;20:151-157. Berkeley, CA: University of California Press. http://
and clinical correlates in adults with obsessive-compul- 21. Tests document readability: readability calculator. www.publichealthlaw.net/Reader/docs/Tarasoff.pdf.
sive disorder. Compr Psychiatry. 2006;47:325-329. http://www.online-utility.org/english/readability_test_ Accessed January 14, 2013.
14. Mataix-Cols D, Rauch SL, Manzo PA, et al. Use of and_improve.jsp. Accessed January 13, 2013. 28. Kessler RC, Zhao S, Katz SJ, et al. Past-year use of out-
factor-analyzed symptom dimensions to predict out- 22. Bruchmüller K, Margraf J, Schneider S. Is patient services for psychiatric problems in the National
come with serotonin reuptake inhibitors and placebo ADHD diagnosed in accord with diagnostic criteria? Comorbidity Survey. Am J Psychiatry. 1999;156:115-123.
in the treatment of obsessive-compulsive disorder. Am Overdiagnosis and influence of client gender on diagno- 29. Torres AR, Prince MJ, Bebbington PE, et al.
J Psychiatry. 1999;156:1409-1416. sis. J Consult Clin Psychol. 2012;80:128-138. Treatment seeking by individuals with obsessive-com-
15. Tek C, Ulug B. Religiosity and religious obses- 23. Gude T, Dammen T, Friis S. Clinical vignettes in pulsive disorder from the British psychiatric morbidity
sions in obsessive-compulsive disorder. Psychiatry Res. quality assurance: an instrument for evaluation thera- survey of 2000. Psychiatr Serv. 2007;58:977-982.
2001;104:99-108. pists’ diagnostic competence in personality disorders. 30. Lester H, Tritter JQ, Sorohan H. Patients’ and
16. Carlat DJ. Practical guides in psychiatry: the psychi- Nord J Psychiatry. 1997;51:207-212. health professionals’ views on primary care for people
atric interview. Philadelphia, PA: Lippincott Williams & 24. Lanza ML, Carifio J. Use of a panel of experts to with serious mental illness: focus group study. BMJ.
Wilkins; 2005. establish validity for patient assault vignettes. Evaluation 2005;330:1122.
PRESENTS
REGISTER NOW!
12 t h ANNUAL
ENDORSED BY:
UPDATE
Join us for this interactive, live symposium SATURDAY
where nationally renowned faculty will address: OCTOBER 26, 2013
CINCINNATI
Emerging Trends and Best
Practices in Pharmacotherapy
SYMPOSIUM DIRECTOR
EARN UP TO
Henry A. Nasrallah, MD 7.5 AMA PRA
CATEGORY 1
UNIVERSITY OF CINCINNATI COLLEGE OF MEDICINE
CREDITS™
FACULTY
James W. Jefferson, MD Anne Marie O’Melia, MS, MD, FAAP The University of Cincinnati is accredited by the
Accreditation Council for Continuing Medical
Roger S. McIntyre, MD Michael E. Thase, MD Education to provide continuing medical educa-
tion for physicians.
Robert K. McNamara, PhD Peter J. Weiden, MD The University of Cincinnati designates this live
activity for a maximum of 7.5 AMA PRA Category
1 Credits™. Physicians should claim only the cred-
its commensurate with the extent of their partici-
To register or for more information go to: www.PsychPharmUpdate.org pation in the activity.
AACP.com Annals of Clinical Psychiatry | Vol. 25 No. 3 | August 2013 209You can also read