Lifelong Care for Children with Chronic Conditions: A discussion series Re-imagining the Package of Care for Children Subgroup - Child ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Lifelong Care for Children with
Chronic Conditions:
A discussion series
Re-imagining the Package of Care for Children Subgroup
May 14, 2021
Child Health Task Force Today
from
1500+ members 50+ countries 300+ organizations
Working together in 10 subgroups
Focused on 5 themes of work
Series objectives • Share and get feedback on UNICEF’s working “Integrated Chronic Lifelong Care for Children and Adolescents” framework • Present case studies on specific chronic conditions • Draw lessons for broader programming and implementation

Nande Putta Bistra Zheleva Dr. Sreehari Nair
Program Specialist VP Global Strategy and HQ State Nodal Officer Child
Child Survival Advocacy, Children’s Health, National Health Mission.
UNICEF HeartLink Department of Health, Kerala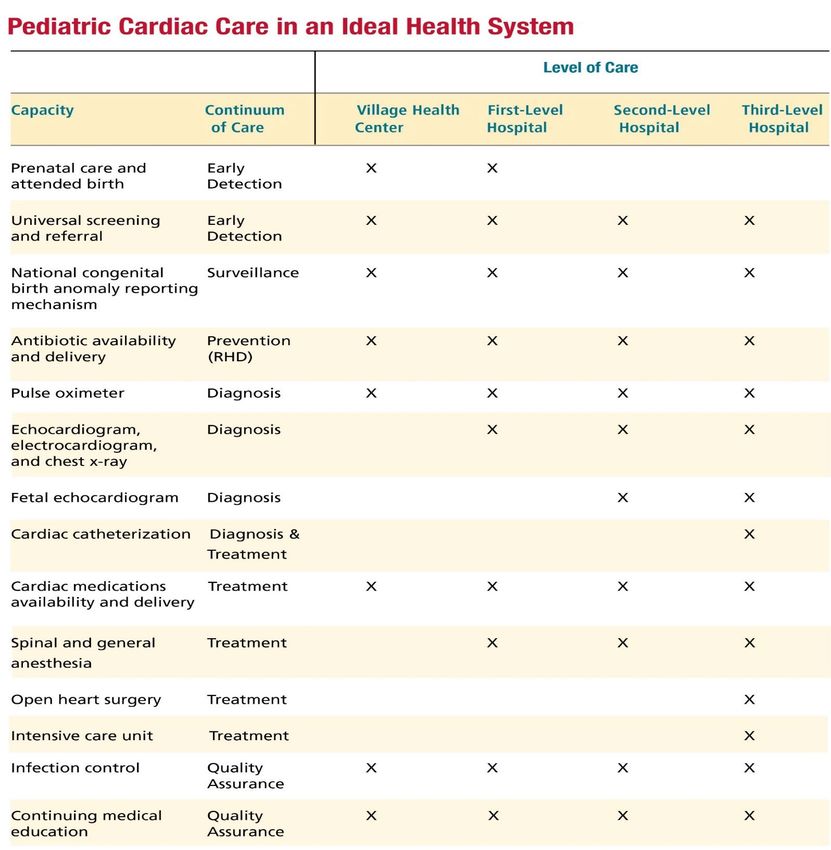
May 2021
Integrating Chronic Lifelong Care for
Children and Adolescents in Primary Health
Care
Dr. Nande Putta
© UNICEF/Lister
Presentation Outline
Rationale Framing in the broader Conceptual Graphic of Ongoing processes
context of Child Health the Chronic Care Model towards guidance
Epidemiology and PHC (CCM) for Children and development
Adolescents
Rationale • Chronic Conditions affecting Children and Adolescents: HIV, Diabetes, Rheumatic Heart Disease, Asthma, Disabilities, Sickle Cell Disease, Cancers, Hep B, Syphillis • In contrast with high-income countries, Chronic Care for children and adolescents is a less-developed area in low-and-middle-income countries • These countries have typically focused on “episodic” management of common childhood illnesses that significantly contribute to child mortality • With shifting epidemiologies, in part due to improving economies and gains in child mortality; and with UNICEFs focus on a thrive and transform agenda over and above survival; chronic conditions come more into focus.
DALY’s by NCDs, Injuries, and communicable/nutritional
disorders in the 1st two decades of life
Burden of
diseases/disorders
and NCDIs varies by
economic income
Embedding Chronic Lifelong Care Models for Children &
Adolescents in PHC
Well Child and Adolescent
Acutely sick or afflicted Child and Adolescent
Chronically sick or afflicted Child and Adolescent
Early Middle
Infancy Adolescence
LIFECOURSE Pregnancy Birth
(0-1 yrs)
Childhood Childhood
(10-19)
(1-4yrs) (5-9)
Routine entry points ANC Immunization Immunization, well and sick
baby clinics, nutrition services School & health services
Community, Civil Society & Multi-Sectoral engagement
Community Health literacy (awareness raising, prevention messaging) for chronic diseases
level Early detection of risk and referral
Peer and treatment support
PRIMARY CARE
Primary health Screening in pregnancy Early screening, detection and diagnosis Transition of care
(HIV, SCD, CHD, CS) Early interventions Adherence risk
facility level
Newborn screening for genetic (Asthma, CHD, Childhood cancer, Congenital management
Syphilis, Developmental Delays & Disabilities, Adolescent friendly
metabolic conditions
HIV, RHD, T1 & T2 diabetes) services
Developmental monitoring, treatment monitoring & longitudinal tracking
Specialized Care Specialized care e.g. surgery, chemo/radiotherapy
Management of complicated cases, treatment failuresEarly Middle
Infancy Adolescence
LIFECOURSE Pregnancy Birth
(0-1 yrs)
Childhood Childhood
(10-19)
(1-4yrs) (5-9)
Routine entry points ANC Immunization Immunization, well and sick
Health
Supply Chain School & health services
Management baby clinics, nutrition services
Workforce
Health Systems Strengthening
PRIMARY CARE
Quality of National and sub-
Care national financing
Developmental monitoring, treatment monitoring & longitudinal tracking
Data and Digital District HSS and
Specialized Care Health Governance and decentralized
Partnerships (CSO, management
Pvt. Sector)Overview of process underway
External Expert Group
Evidence review
Partnership building
Internal Reference Group Webinar series
Resource mobilization
Stakeholder consultation
Thank You!
Early country level work across
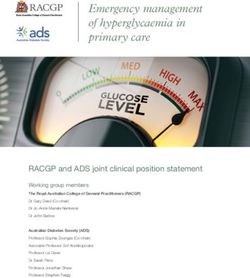
diverse countriesCONGENITAL HEART DISEASE –
A CASE FOR POPULATION HEALTH
APPROACH
Bistra Zheleva
Children’s HeartLink
May 2021Children’s HeartLink
Vision: Children around the world have access to high-quality heart care
Mission: We save children’s lives by transforming pediatric heart
care in underserved parts of the world
Advocacy Hospital Capacity Patient Care Pathways
14
@bzheleva2030 Targets:
①End preventable childhood deaths
• NM, 12 per 1,000 live births
• U5M 25 per 1,000 live births
②Reduce by 1/3 premature mortality from NCDs
③Achieve UHC, including financial risk protection
④Substantially increase health workforce in LMICs
15
@bzheleva16
17 A Case for the Invisible Child @bzheleva http://theinvisiblechild.childrensheartlink.org/
Causes of death in children >1 year, 2019 (by death rate per 100 000)
18
*GBDcompare tool, 2019 data
@bzhelevaTHE GLOBAL BURDEN OF CONGENITAL HEART
DISEASE
217,000
deaths from CHD globally
13.3 million
prevalence
18.6 million
DALYs
96%
deaths in LMICs
70% (150,000)
deaths were in infants
19
@bzheleva GBDcompare tool, 2019 dataIndia CHD deaths, 2019
Total: 38,152NCD mortality beyond SDG target 3.4
WHO 25×25 target & SDG 3.4 → deaths from NCDs 30-70 age
2016
▲ 12.5 million deaths (30-70)
▲ 1.7 million deaths inRHD and CHD: Global YLDs and YLLs by Age, 2017
Aggregate Data
YLDs
- RHD: 1,900,974
- CHD: 589,479
YLLs
- RHD: 7,492,586
- CHD: 21,634,418
22
@bzheleva Zimmerman et al. Lancet CAH, 20207% world population has access to cardiac surgery
90% no CHD treatment or suboptimal care
23
Hoffman CVJ Africa 24:141;2013
@bzheleva26
Zheleva, Int. J. Neonatal Screen. 6, 49; 2020
@bzheleva2016
POPULATION
HEALTH APPROACH
TO CHD
Improving timely
screening, diagnosis
and referral, increase
access to tertiary care
27
@bzhelevaKerala Malaysia
SDG3: Reduce child mortality
2/3 by 2020 and 50% by 2030
7 to 5 by 2020 Build pediatric cardiac
NMR
to 3 by 2030 surgery in the public sector
12 to 8 by 2020
Reduce reliance on private
IMR and semi-private providers
to 6 by 2030
Regionalize pediatric
U5M 14 to 9 by 2020 cardiac surgery
R to 7 by 2030
CATALYST: RBSK, national 0-18 screening and
80
intervention program for diseases,
IMR per 1,000
60
live births
40 defects at birth & disabilities India
20 (Rashtriya Bal Swasthya Karyakram) Kerala
0 Malaysia
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
28
@bzheleva29
IMR Trend
India has registered a significant decline in Infant
Mortality Rate (IMR) in the last two decades.
As per SRS 2019 , IMR of India has declined to 32 per
1000 live births.
Kerala Scenario
Kerala's IMR was stagnant around 12 over a
decade.
As per SRS 2019, IMR Kerala is now down to 7 per
1,000 live births.
• This reduction in IMR in Kerala is a result of efforts in bringing
down anaemia among pregnant women, crucial interventions
in the treatment of infectious disease among Newborn &
infants, improved breast-feeding practises, better sanitation
& hygiene, etc.• CAUSES OF INFANT MORTALITY IN KERALA 2013
Why CHD has been given
importance under IMR reduction
strategy
Maternal
Others
4%
12%
IMR in Kerala while examined in detail Infection / Prematurity
revealed that Prematurity & Birth sepsis 35%
Asphyxia followed by Congenital 12%
Anomalies are the leading cause.
Low birth
weight
Among the congenital anomalies 4% Congenital
Congenital Heart Disease is the major Birth anomalies
contributor. asphyxia 28%
5%
• IAP study 201333 MILLION POPULATION, 14 ADMIN. UNITS (DISTRICTS)
0.5 MILLION EST. CHILDREN BORN/YEAR
12 INFANT MORTALITY RATE, PER 1,000 LIVE BIRTHS
6,000 EST. INFANT DEATHS/YEAR
8 PER 1,000 EST. CHD INCIDENCE
4,000 EST. NEW CHD/YEAR
1,000-1,200 EST. NEW CRITICAL CHD/YEAR (25-30% OF ALL NEW CHD)
650-750 EST. INFANT DEATHS FROM CHD/YEAR
ANNUAL KERALA-BORN INFANT CHD SURGERIES
500 EST.
PERFORMED
42-50 % EST. ESTIMATED INFANT SURGICAL TREATMENT COVERAGE
EXISTING PEDIATRIC CHD SURGERY CENTERS, 2
7
2016 PUBLIC AND 5 PRIVATE
Private Pediatric
Cardiac Program 12 PEDIATRIC CARDIOLOGISTS
Public Pediatric
Cardiac Program
10 PEDIATRIC CARDIAC SURGEONSMILE STONES..
Metabolic Screening VBD screening as part of RBSK ROP Screening for High Risk Preterm
Started as a special As part of rolling out RBSK, Screening for Retinopathy of Prematurity
initiative in selected documenting Newborn Birth defect started in 7 Tertiary Care Special Newborn
delivery points screening in delivery points were Care Units
initiated
2012 2014 2016 2018 2018
Hearing (OAE) Screening Pulse Oximetry Screening
OAE Screening program started with Started in selected 54 delivery points
the support of KSSM, Presently, (with more than 100 delivery per
extended to all Delivery points with month) for early detection of cCHD
more than 50 delivery per monthFUNCTIONAL BIRTH DEFECT SCREENING
Pulse Oximetry screening for Congenital Heart Disease at all 98 Public Delivery points
Pulse Oximetry Screening PO Results to Hridyam Combined with Physical
for CHD portal Examination Pulse Oximetry linked to
HRIDYAM
Machine while connected to
local computer. with Internet All failed cases by send to
PO Screening at 24 -48 Pediatrician for Failed cases will be alerted to
Hours after birth & the set Connectivity PO results against specifically looking for DEIC who will arrange for
algorithm in machine detects each child get updated in any confirmatory ECHO. The
PO passed/failed Hridyam & VBD portal case will get registered in
HEART MURMUR
& LOW Vol FEMORAL Hridyam and case followed
PULSE up.
Insert Your Image Insert Your Image Insert Your Image Insert Your Image
Hridyam PortalRegistration
DEIC/Public
Case Registration from
Public (Web/Android app) / DEIC
Follow up
DEIC
DEIC
will
coordin
Add more Information Verify and
ate transfer to Pediatric cardiologist for
expert Opinion/Suggestion of Category
Treatment
cardiologist
Advise Review If No If Yes
Pediatric
for further
examination
with a PC Information checked for Suggest Category &
adequacy to Categorize
Treatment plan
Advise
All Cases
Hospitals
Investigations like
Public
ECHO, CT/MRI, Cath Cases of cat 1a & Cases of
Procedure at PH/EH
Public Hospital Cat 1 a, b, c from Districts
other than Tvm, Klm,Ptt, Allot to
Investigation Ktym Public/Empaneled
Completed If Yes Hospital
Hridyam
Case refer to
Admin
If No
Empaneled
Consent Treatment hospitals
plan within Treatment
Empanelled
tentative date
Hospitals
Allot to Forwarded to Empaneled. plan within
Public/Empaneled Hospital tentative date
Hospital ConsentSURGERY DONE 2018 &19
Focus is on Infant Cases/ Neonates with complex diseases as a life saving program.
Sl.
No. INSTITUTIONS 2020 2019 2018 2017
1 SCTIMST 148 330 439 171
2 MCH KOTTAYAM 23 86 108 1 10%
3 MCH KOZHIKKODE 4 13 -- --
4 AIMS Cochin 357 298 225 16
20%
5 Aster Medicity, Ernakulam 3 3 0 0
6 Lissie Hospital 234 85 49 13
70%
7 Aster MIMS, Kozhikode 199 127 22 0
Believers Church Medical
8 College 42 49 42 7
SAT Cases Registered & Operated in 2017, 2018 & 2019
THIRUVANANTHAPURAM
9 (Only interventions) 11 40 45 0
Total 1021 1031 930 208Follow up of Hridyam Cases in Community
Case Registered in Hridyam portal
Post-Surgical Case
Pre-Surgical Case
Cases redistributed as per their local Case followed up as per pre-defined protocol.
area, So that the community Nurse can First visit after 72 hours post discharge, 7th day,
see the case in their login 14 days, 1 month, 3 months and 6 months or as
recommended by treating team
Case is followed up as per
predefined schedules, at
least once in every month
Action initiated as per the need of the case.
Will document the findings as per
the designed format digitally real-
time
Response initiated by treating team in case of
emergencies through Hridyam portalCHARACTARISTIC • The Main Success Factors are :
• Uniqueness, Importance & Focus
• First of this kind - comprehensive • Thrust given to early Diagnosis -
• All surgical slots in Kerala made
approach to Children with Congenital
various means Ante natal Fetal Heart
Heart Disease (CHD).
into a single pool & available for
Screening, Pulse Oximetry combined
• Cashless Treatment children registered under Hridyam
with physical examination.
in Private empanelled Hospitals. • Waiting period became finite
• Capacity building - Technical and
• Web based Single registry Those registered knows there
Infrastructure
For children with CHD – Case, pre tentative surgery dates
is also taken up as a
surgical and post surgical follow up
comprehensive program
40hridyam.in https://www.facebook.com/ hridyamkerala/ https://twitter.com/@Hridyam_kerala THANK YOU www.hridyam.kerala.gov.in
Lifelong Care for Children with Chronic Conditions Discussion Series
Series Dates & Case Study Discussions:
Engage with the co-chairs:
• Cara Endyke Doran - May 14th: Congenital heart disease
cendykedoran@globalcommunities.org June 11th: HIV, type 1 diabetes & sickle cell disease
July 9th: Integrated NCD package of services
• Raoul Bermejo - rbermejo@unicef.org
Time: 9 - 10:30am EDT [GMT-4]
Check out the Child Health Task Force Website for important resources!
Subgroup information, recordings and presentations from previous webinars are available on the Photo credit: Liberia, Kate Holt/MCSP
subgroup page of the Child Health Task Force website:
www.childhealthtaskforce.org/subgroups/expansion
Become a member of the subgroup: www.childhealthtaskforce.org/subscribeYou can also read